
Abstract
The treatment of inflammatory arthritis has been revolutionised by the introduction of biologic treatments. Many biologic agents are currently licensed for use in both paediatric and adult patients with inflammatory arthritis and contribute to improved disease outcomes compared with the pre-biologic era. However, immunogenicity to biologic agents, characterised by an immune reaction leading to the production of anti-drug antibodies (ADAs), can negatively impact the therapeutic efficacy of biologic drugs and induce side effects to treatment. This review explores for the first time the impact of immunogenicity against all licensed biologic treatments currently used in inflammatory arthritis across age, and will examine any significant differences between ADA prevalence, titres and timing of development, as well as ADA impact on therapeutic drug levels, clinical efficacy and side effects between paediatric and adult patients. In addition, we will investigate factors associated with differences in immunogenicity across biologic agents used in inflammatory arthritis, and their potential therapeutic implications.
Introduction
The discovery and clinical use of biologic treatments in the management of inflammatory arthritis in children and adults has been associated with significant clinical benefits, as well as advances in understanding the pathogenesis of different types of inflammatory arthritis. Immunogenicity to biologic treatments is an unwanted immune reaction against a therapeutic antigen. This immune reaction generates anti-drug-antibodies (ADAs), which could counteract the therapeutic effects of the biologic treatment and, in rare cases, induce adverse reactions.1,2
It has become increasingly recognised that biologic treatment duration, mode, rate and route of administration, and more specifically, the type of biologic therapeutic [e.g. monoclonal antibodies (mAbs) versus recombinant fusion proteins] are all factors that influence the risk of immunogenicity. 3 In addition, individual patient factors, such as genetic background, 4 disease type, 5 and concomitant use of disease modifying anti-rheumatic drugs (DMARDs), 6 all contribute differentially to the formation of ADAs. Recent research has been focused on highlighting the genetic risk for developing ADAs: e.g. HLA-DRB1*15 was associated with increased the risk for developing high ADA levels to interferon (IFN)β-1a treatment in multiple sclerosis, while HLA-DQA1*05 decreased this risk, 7 and HLA-DQA1*05 was associated with increased ADA prevalence across various biologics and autoimmune diseases. 8 Other factors such as smoking and infections are also associated with increased risk,8,9 whereas concomitant use of antibiotics and immunosuppressant medication are associated with decreased immunogenicity risk. 8 In addition, the manufacturing process of various biologic agents, in particular, their contamination with low-level host proteins, is a major contributor to immunogenicity. 10
Therapeutic drug monitoring and immunogenicity testing comprise measurement of trough drug levels and ADAs. The most widely used ADA detection methods are bridging enzyme-linked immunosorbent assay (ELISA; which use labelled therapeutic mAbs) and radioimmunoassay (RIA), while other new methods such as competitive displacement and tandem mass spectrometry have also been proposed. 11 Currently, most mAbs on the market are humanised or fully human; however, they still carry immunogenic risk. This could be attributed to anti-idiotype reactivity, which is a common reaction of the immune system to the appearance of any novel antibody. 12
The molecular mechanisms leading to generation of ADA are not completely elucidated and a detailed discussion of immune mechanisms is beyond the scope of this review (for a recent review see 13 ). One basis for ADA generation involves the capacity of the human immune system to recognise ‘non-self’. Since the first therapeutic mAbs of murine origin were developed, further efforts have now been made to improve their performance and decrease their immunogenicity. The continuous advancement in recombinant deoxyribonucleic acid (DNA) technologies has led to the development of chimeric (fused human–murine mAbs) and humanised mAbs. Chimeric antibodies were developed by replacing the constant region of murine mAbs with human components and the humanised mAbs are constituted entirely of human sequences, with the exception of the complementarity determining regions of the variable regions which are of mouse-sequence origin. Subsequently, the advanced antibody engineering achieved the production of fully human antibodies where antigen specificity has been selected either in vivo in genetically modified mice or by antibody engineering processes combined with screening. 14 Many factors contribute to differences in immunogenicity, from biopharmaceutical properties related to downstream processing and drug formulation 15 to patient individual characteristics, including the antigen burden which correlates with their disease activity. 16
Both ELISAs and RIAs detect only free circulating ADAs; therefore, they can be associated with false negative results in the context of presence of ADA-immune complexes which are detectable only if they exceed in concentration the circulating drug levels.17,18 In one study, ELISA was more sensitive in detecting ADA when present in high titres than RIA, while in patients with ADA detected by RIA but not by enzyme-linked immunosorbent assay, only the drug levels were significantly associated with treatment response to adalimumab. 19 Interestingly, measuring drug levels and drug clearance alone is also shown to be a reliable predictor for ADA in RA and juvenile idiopathic arthritis (JIA) patients.20,21 Several studies concluded that although ADAs were not independently associated with treatment response, they may be helpful in determining the cause of low drug levels and guide therapeutic decisions.22,23
The presence of ADAs may be associated with reduced clinical efficacy through two main mechanisms. ADAs that compete with the cytokine binding site (the Fab fragment of the therapeutic agent) have neutralising properties as they block the pharmacological function of the drug. ADAs directed against the Fc fragment (more frequently targeting the junction between Fc and Fab) lead to formation of immune complexes associated with enhanced drug clearance that may also influence the clinical response to biologic treatment through leading to sub-optimal (sub-therapeutic) drug levels. 24 Therefore, based on their specificity ADA can be grouped as neutralising (when they target the antigen binding sites of the therapeutic drug) or non-neutralising (when they recognise epitopes away from the drug-binding site, therefore not directly impairing the efficacy of the drug). 3
Here, we review the evidence of impact of ADAs against various biologic therapeutics used for treatment of inflammatory arthritis in adults and children, as there are no previous reports investigating immunogenicity across age. This review focuses on depicting differences between ADA prevalence, titres and timing of development, as well as impact on therapeutic drug levels, clinical efficacy and side effects in children compared with adults with inflammatory arthritis. Where data are available, we will also investigate the clinical predictors for ADA development, as well as the influence of additional DMARD therapy on ADA development and biologic drug retention.
Neutralising ADAs against mAbs targeting TNF-α were more prevalent than ADA against fusion proteins (etanercept and biosimilars) while the kinetic of ADA generation varied across anti-TNF-α agents in adult and paediatric inflammatory arthritis studies
Many studies have reported the presence of ADAs against anti-tumour-necrosis-factor-alpha (anti-TNF-α) inhibitors used to treat different types of inflammatory arthritis, including etanercept [fusion protein of the extracellular ligand-binding portion of the human 75KD p75 TNF receptor (TNFR) linked to the Fc portion of human immunoglobulin G1 (IgG1)], adalimumab (fully human mAb), certolizumab (humanised antibody Fab’ fragment), golimumab (human IgG1κ monoclonal antibody) or infliximab (a chimeric mAb; Table 1). The general observation is that ADAs against etanercept have a lower prevalence compared with ADAs against adalimumab or infliximab. 25 Furthermore, comparative studies show that ADAs to human/humanised (adalimumab, certolizumab, golimumab) and chimeric (infliximab) anti-TNF-α therapeutic mAbs are largely neutralising, 26 while the ADAs against etanercept are predominantly non-neutralising. 27
Impact of ADAs on disease outcomes in children and adults with inflammatory arthritis treated with anti TNF-α agents.

ve, positive; −ve, negative; ADA, anti-drug antibody; AS, ankylosing spondylitis; AZA, azathioprine; CI, confidence interval; CRP, C-reactive protein; DMARD, disease-modifying antirheumatic drug; ERA, enthesitis-related arthritis; ESR, erythrocyte sedimentation rate; EULAR, European League Against Rheumatism; HAQ-DI, Health Assessment Questionnaire Disease Index; IJD, inflammatory joint disease; JIA, juvenile idiopathic arthritis; JPsA, juvenile psoriatic arthritis; MMF, mycophenolate mofetil; MTX, methotrexate; n, number of patients treated with a certain biologic included in the study/systematic review; PsA, psoriatic arthritis; RA, rheumatoid arthritis; RCT, randomised control trial; SD, standard deviation.
In adults, the rates of ADA formation against infliximab range from 8% to 62% in rheumatoid arthritis (RA), 15% to 33% for psoriatic arthritis (PsA) and 6.1% to 69% for ankylosing spondylitis (AS; 28 Table 1). ADAs against infliximab are also shown to be associated with lower serum biologic drug concentrations in adult inflammatory arthritis patients.27,28,31,32,44–48 There is a paucity of studies investigating the timing of development of ADA against various anti-TNF-α agents: evidence suggests that longer exposure to infliximab increases immunogenicity; for example, ADAs against infliximab in adults with RA occurred after the first 10 infusions (23.4 ± 2.4 weeks), while ADAs were detected in 25% of JIA patients after 52 weeks and in 37% at 204 weeks.35,36,49 The dose of biologic agent, as well as patients’ age, could influence immunogenicity: a higher incidence of ADAs was observed in patients treated with infliximab 3 mg/kg (38%), compared with 6 mg/kg (12%), 36 while a significantly higher prevalence of ADAs was found in younger children (ADA-positive mean age 7.01 years versus ADA negative 9.88 years, p = 0.003). 29
The prevalence of ADAs against adalimumab has high variability across different types of autoimmune diseases in adults25,28,31,50–52 and children with JIA 35 (Table 1). The timing of adalimumab ADA development is controversial: in some adult studies ADA prevalence did not increase with treatment duration,53,54 while in other studies there was a significant increase, with ADA developing between 4.5 months and 12 months of treatment.9,34,44,50,52,55 Similarly, studies in JIA showed both trends: a significant increase of ADA with time 35 or no correlation with treatment duration, 30 suggesting that ongoing monitoring to establish their clinical relevance and impact on management is required.
Etanercept treatment was associated with a lower ADA rate than infliximab and adalimumab 25 (Table 1), with the vast majority of adult studies reporting no detectable ADA25,27,28,31,32,50,52,55 This pinpoints that the chemical structure of the anti-TNF-α therapeutic agent (fusion protein versus mAb) is likely to be a key factor in inducing drug immunogenicity. When detected, ADAs against etanercept were found to be non-neutralising in both adult and paediatric studies.28,35 ADA prevalence increased with treatment duration with a corresponding decrease in etanercept drug levels over time in JIA.37,38
A highly sensitive ELISA test detected ADA against golimumab in 31.7% of patients with RA, PsA and AS in comparison with standard ELISA which detected ADA only in 4.1%, 40 while their prevalence varied across adult studies (Table 1). The impact of ADA on serum golimumab concentrations was consistent in JIA and RA studies, whereby higher ADA titres were associated with lower drug concentrations.28,39,41,56 This was generally shown at ADA titres >1:1000 in JIA, 39 and in adults, median peak titres ⩾100 were associated with undetectable or very low drug levels. 57 Interestingly, in another study in PsA, which used a standard assay, the golimumab dose (50 mg versus 100 mg) did not appear to affect the ADA rates, which remained low for the whole duration of the study through to week 52 (4.9%). 58
There are fewer studies investigating the presence of ADAs against certolizumab,42,43 although in both studies, ADAs were associated with lower drug levels (Table 2). A more recent study, however, reported that there was no significant correlation between ADA and certolizumab drug levels (r = −0.471, p = 0.122). There is evidence that ADAs were still detected at higher certolizumab concentrations of >10 mg/l. 59 The majority of patients with ADA had detectable titres from week 16 onwards, and 65% remained ADA positive after 1 year of follow up. 59 There are no studies in paediatric populations.
Impact of ADAs on disease outcomes in children and adults with inflammatory arthritis treated with other biologic agents.

ve, positive; −ve, negative; ADA, anti-drug antibody; ARDS, autoimmune rheumatic diseases; AS, ankylosing spondylitis; AZA, azathioprine; DMARD, disease-modifying antirheumatic drug; F, female; INF, infliximab; IL, interleukin; IQR, interquartile range; IV, intravenous; JIA, juvenile idiopathic arthritis; M, male; MTX, methotrexate; PsA, psoriatic arthritis; pSS, primary Sjögren syndrome; RA, rheumatoid arthritis; RCT, randomised control trial; RTX, rituximab; SC, subcutaneous; SD, standard deviation; SLE, systemic lupus erythematosus; TCZ, tocilizumab.
When anti-TNF-α agents have been studied comparatively in adults, there was evidence of increased prevalence of ADAs against infliximab compared with adalimumab (25.3% versus 14.1% respectively), as well as between adalimumab and golimumab (14.1% versus 3.8%). 25 A similar trend was found in a meta-analysis of biologic agents in JIA, where the pooled prevalence of ADAs against infliximab was 36.6% compared with 21.8% for ADAs against adalimumab. 35 As mentioned above, the prevalence of ADAs against golimumab seems to be higher in children (46.8%) but based on limited evidence. 39
Variable impact of ADAs directed against anti-TNF-α treatments on clinical efficacy: loss of efficacy to adalimumab and infliximab was consistently found in children and adults who developed ADAs
Various studies in RA, PsA and AS provided evidence for an association between the presence of ADA against adalimumab and loss of clinical efficacy or diminished clinical response,23,28,31,50 while other studies found no association53,54 (Table 1). The impact of ADAs on the trend of inflammatory markers is not clear; some studies found higher erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) in patients who had detectable ADAs,27,31 whereas other studies found no such association. 53 In addition, the presence of both ADA and low adalimumab concentration at 3 months were together significant predictors of poor response at 12 months.50,52 However, the risk of flares following various adalimumab tapering strategies in RA did not seem to be influenced by the adalimumab serum levels or ADA prevalence. 84
A higher proportion of ADA-positive JIA patients treated with adalimumab experienced loss of response and more clinical relapses than those without ADAs.28,30 In JIA, it was noted that transient ADAs (defined as measurable ADAs on up to two consecutive time points which disappeared on subsequent measurements without having any impact on treatment efficacy of toxicity) were not associated with diminished response to medication, whereas permanent ADAs did lower treatment response. 34
Most adult rheumatology studies found no detectable ADAs against etanercept.27,44 It has been suggested that neither etanercept concentrations nor ADA positivity correlated with JIA activity or remission states. 37
A meta-analysis of nine studies of infliximab in adult autoimmune diseases found that the presence of ADAs decreased the odds of response by 58%. 25 After 52 weeks of treatment with infliximab, non-responder RA patients were significantly more likely to be ADA positive. 47
Adult RA studies found that ADAs against golimumab were associated with a poorer clinical response.28,56 ADA-positive RA patients (15.2% at 24 weeks) had a worse EULAR response and higher DAS-28 compared with ADA-negative patients. 56 However, one study which utilised a more sensitive method of ADA detection (drug-tolerant enzyme immunoassay, DT-EIA) in adults, reported no effects of ADAs to golimumab on clinical responses at 24 and 52 weeks, across RA, PsA and AS. 40 This highlights the importance in sensitivities of assays used. Studies in children with JIA found that ADAs to golimumab did not appear to have impact on clinical responses.39,57 Brunner et al. 39 reported that none of the eight JIA patients found with high ADA titres >1:1000, experienced flares.
ADAs against certolizumab appeared to have an impact on RA clinical response at 3 months, where the majority of ADA-positive patients were non-responders, 42 but there was no independent correlation with the 12-month EULAR response, 43 suggesting that there was a time-dependent relationship. There are no paediatric studies.
A meta-analysis performed on 12 observational prospective cohort studies in adults demonstrated that the development of ADA reduced the anti-TNF response rate (RR) by 68% [RR = 0.32; 95% confidence interval (CI) 0.22, 0.48], 85 while in children with JIA, a qualitative analysis found that antibodies to infliximab and adalimumab were associated with treatment failure. 35
Additional methotrexate treatment decreased the rate of ADA formation against anti-TNF-α treatments
Generally, for both adults and children, concomitant DMARD therapy was beneficial and resulted in a decrease in ADA positivity, but the impact of DMARDs on ADA formation was not always analysed to enable reliable conclusions9,30 (Table 1). Most studies looked at concomitant methotrexate (MTX) therapy, but azathioprine, leflunomide and mycophenolate have also been shown to be associated with lower ADA prevalence, suggesting that all DMARDs may be associated with benefits against drug-induced immunogenicity.23,28,32,52 Unfortunately, none of the studies evaluated comparatively the impact of individual DMARDs on immunogenicity in inflammatory arthritis because of small numbers of patients on DMARDs other than MTX, and because some patients were treated with more than one conventional DMARD. Concomitant use of MTX was associated with lower rates of ADAs against infliximab in RA.28,32,45,50,86 Moreover, RA patients treated with infliximab were less likely to develop ADAs if they received high biologic doses/induction therapy, or if they received continuous versus intermittent therapy.28,33,44,45,86 A randomised controlled trial (RCT) of infliximab plus MTX for the treatment of JIA, found that more patients achieved clinical response in the ADA-negative group (79% versus 67%). 36
Similar evidence has been found in children, with studies suggesting a protective effect with the addition of MTX.34,35,57 Interestingly, DMARD use in children was found to be significantly lower in those who developed permanent ADAs to adalimumab. 34 It has also been suggested that MTX reduces immunogenicity against adalimumab in a dose-dependent manner,44,50 as patients who did not develop ADAs were on a higher MTX dose. 55 However, a paediatric study found that there was no difference in ADA rates in JIA patients with longer exposure to MTX. 30
In adults, concomitant use of MTX was associated with lower incidence of ADAs to golimumab.28,40,87 A study found that the mean trough golimumab level at 24 weeks was comparable in ADA-positive versus -negative patients, with or without concomitant MTX. 87
ADAs against infliximab and adalimumab have been associated with side effects to therapy
In both adults and children, there was no clear consensus on whether ADAs have an impact on safety (Table 1). As expected, most reports included a small number of cases experiencing side effects. Adverse events more frequently mentioned included injection-site or infusion reactions, serum sickness and thromboembolic events. Some studies suggested that adverse events occurred more frequently in patients with ADAs to adalimumab,28,31,33 with others showing no significant differences.27,54 In paediatric studies, despite limited information available, no association between the presence of ADA and adverse events was reported. 35 There was a suggestion of a possible increase in minor upper respiratory tract infections in children with detectable ADAs; however, this conclusion was limited by the small sample size. 34
ADAs against infliximab have been reported to confer a higher likelihood of adverse drug reactions.25,28,33,44,45,48,50 In an RA study, 48 ADA-positive patients had an increased risk of adverse drug reactions compared with ADA-negative patients over 52 weeks [21 (18%) versus 7 (7%), p < 0.018]. 50 Similarly, JIA infusion reactions to infliximab were more commonly seen in ADA-positive patients (58% versus 19%). 36 A retrospective chart review of children with JIA and paediatric inflammatory ocular diseases found that patients with ADAs had a 15-fold increased risk of infusion reactions to infliximab compared with patients without ADAs. 29 This study also found that ADA-positive children were significantly younger (mean age 7.01 versus 9.88 years, p = 0.003).
Limited data were available regarding the impact of immunogenicity against etanercept on safety. Studies across age did not report an association between ADA positivity and adverse events.35,57 In JIA studies, the proportion of patients with ADAs did not differ between responders and non-responders to etanercept. 37
Studies in both paediatric and adult populations did not report an association between ADAs and adverse effects to golimumab.39,56,57 Similarly, multiple adult studies reported no association between the presence of ADAs against certolizumab and adverse effects;42,43,59 in addition, RA patients who experienced adverse effects did not have ADAs.42,43
Immunogenicity to anti-TNF-α biosimilars is similar to or lower than that of their originators
Biosimilars are new biological products which are highly similar to their biological reference drug and have comparable clinical efficacy. At present, the use of biosimilars in JIA is limited, thus most evidence related to their immunogenicity is available from adult studies. Multiple studies have shown similar clinical efficacy and immunogenicity profiles when comparing biosimilars with their reference products.28,88–96 For example, ADA-positive CT-P13 (an infliximab biosimilar) patients showed less clinical improvement. 28 ADA against infliximab and adalimumab biosimilars were associated with lower drug concentrations.93,97 The PLANETRA study found that peak serum CT-P13 concentrations were reduced in the ADA-positive group (Cmax = 85.1 µg/ml) compared with the ADA-negative subset (Cmax = 96.7 µg/ml). 93 One meta-analysis reported on the pooled response rates (RRs) of ADA against anti-TNF-α biosimilars compared with their reference product. 90 There were no significant differences in ADA formation rates between the infliximab and adalimumab biosimilars and their reference drugs at 24 to 30 weeks. The etanercept biosimilars showed significantly lower rates of ADA formation compared with the reference product, with a pooled RR = 0.05 at 24–30 weeks. 90 A study of etanercept biosimilar GP2015 did not detect any neutralising ADAs, and all ADA responses were transient (absent by week 24). 96
Clinical relevance of ADAs against other biologic agents in adult and paediatric inflammatory arthritis studies
ADAs against abatacept are mainly non-neutralising and do not have significant impact on clinical efficacy unless treatment is temporarily discontinued
The prevalence of ADAs to fusion proteins, such as abatacept (which comprises an Fc region of IgG1 fused to the extracellular domain of CTLA-4) is generally acknowledged to be lower than to therapeutic mAbs. The prevalence of ADAs to abatacept ranged from 1% to 20% in adult studies,28,44,51,65 and from 8.7% to 23.3% in paediatric studies 35 (Table 2). Younger children with JIA (2–5 years) had a higher prevalence of ADAs than older children (6–17 years). 63 One JIA study compared the prevalence of abatacept specific ADA with anti-CTLA-4-specific antibodies and found the latter to be much higher (1.2% versus 20.7%). 97 In terms of timing of the development of ADAs in children, one study found that ADA concentration increased with a longer duration of exposure to abatacept, 62 whereas another found no increase with continued exposure. 64
Similar to etanercept, abatacept generated ADAs which bind to the Fc fragment (hinge region) and have no neutralising activity. 28 Non-neutralising ADAs decreased the circulating levels of abatacept by enhancing drug clearance in adults.44,51 In children, ADAs were also found to be non-neutralising but were not found to be associated with low abatacept concentrations.62,97
No loss of efficacy due to ADA against abatacept was found in JIA studies,35,62,64,97 while in contrast, in adults with RA, intermittent treatment discontinuation led to higher incidence of immunogenicity and loss of clinical response. 65 It was observed that adult patients who discontinued the treatment temporarily had higher ADA rates than those on continuous treatment (7.4% versus 2.6% respectively). 44 Similarly, ADAs were more frequent in children with JIA who interrupted treatment and had abatacept concentration below therapeutic levels, suggesting that higher treatment doses may be beneficial against immunogenicity. 97
Some adult studies suggested that intravenous therapy was associated with less immunogenicity than subcutaneous administration,28,98 while other studies found no difference. 44 In JIA, no difference was found between the two routes of administration. 35
In RA, concomitant MTX therapy did not significantly affect immunogenicity. 65 In paediatric studies, the impact of MTX has not been studied. 35 Reassuringly, ADAs against abatacept were not associated with increased risk for injection site reactions, hypersensitivity or any other safety concerns,35,62,65,97 even when patients have been followed up to 7 years. 64
ADAs against B-cell-targeted therapies are dose dependent and have impact on clinical efficacy and risk of adverse reactions
Rituximab is a chimeric mAb against CD20. There have been no paediatric studies investigating the relevance of ADAs against rituximab. However, ADAs against rituximab have been reported in 0–21% of adult RA patients. 28 Additionally, ADAs were found to be associated with a reduced treatment response and higher rates of treatment serious adverse events.28,61 Lower serum rituximab concentrations have been reported in ADA-positive patients compared with ADA-negative patients in RA. 60 Moreover, the use of higher rituximab doses and induction therapy has been associated with a decreased incidence of ADAs in RA. 28
A meta-analysis reported that the pooled RR of ADA formation for rituximab biosimilars was 0.86 at weeks 24–28. 91 Of note, the pooled RR of neutralising ADA formation at the same time point was 1.16. Neutralising ADAs were also of a very low incidence at week 72 in the rituximab biosimilar CT-P10. 92 Multiple studies have demonstrated a similar side-effect profile for biosimilars, as higher rates of infusion-related reactions were present in ADA-positive patients compared with ADA-negative patients28,88,89,94,95 (Table 2).
Neutralising ADAs against tocilizumab has no clear impact on clinical efficacy and potential on side effects in adults, while there is a trend for clinical impact in children
Tocilizumab is a humanised mAb against the interleukin-6 receptor (IL-6R). Several studies have reported low ADA rates in RA patients.28,66,67 ADA positivity has been recorded in 1.5% and 1.2% of RA patients receiving intravenous and subcutaneous tocilizumab, respectively, with a high proportion of these being neutralising ADAs 68 (Table 2). The rate of ADA formation has not been seen to significantly differ in tocilizumab monotherapy versus combination therapy with conventional synthetic DMARDs. 68 No correlation has been found between ADA rates and adverse events or a reduced treatment efficacy in adults.51,68 Similarly, low levels of ADAs to tocilizumab have been reported in JIA patients, with a pooled prevalence of 2.3% across four studies. 35 However, neutralising antibodies against tocilizumab in JIA have indeed been shown to correlate with treatment failure, as well as with infusion and hypersensitivity reactions.35,69 Yokota et al. 69 found that out of five JIA patients treated with tocilizumab who developed ADA, four (80%) withdrew from the study due to infusion reactions.
ADAs to sarilumab seem to have limited impact on clinical efficacy and no impact on adverse events
Sarilumab is human recombinant mAb that blocks both the soluble and membrane-bound IL-6 receptor, similarly to tocilizumab, but with a higher affinity. Currently, there are no studies of immunogenicity in paediatric populations. The presence of ADAs did not appear to affect clinical efficacy in various trials.70–72 The MONARCH trial demonstrated that only 2.7% of RA patients had persistent ADAs, however, no neutralising ADA were detected. 70 It has been suggested that ADAs against sarilumab are, in most cases, transient. 99 Xu et al. 73 described a trend towards higher apparent linear clearance of sarilumab when ADAs were present. In addition, patients with persistent ADAs had a lower mean drug levels compared with ADA-negative patients. At a dose of 150 mg, treatment-emergent ADA incidence was 24.6% compared with 18.2% at a higher dose of 200 mg. Of those who had persistent ADA, the incidence of neutralising ADA was also higher in the group receiving 150 mg sarilumab compared with 200 mg (10.8% and 3.0% respectively). 71 Multiple studies have shown that ADA positivity was not associated with a higher incidence of adverse effects.70–72 Hypersensitivity reactions occurring during treatment were reported in 8.0% of ADA-negative patients and in 3.1% of ADA-positive patients. 72
Neutralising ADAs against IL-12/23 blockade have low prevalence but possible impact on clinical efficacy in inflammatory arthritis
Ustekinumab is a human immunoglobulin G1κ mAb against common sub-unit p40 of IL-12 and IL-23. The prevalence of ADAs was 8% to 11% in psoriatic arthritis adult patients treated with ustekinumab. 28 Moreover, a study evaluating the efficacy of subcutaneous ustekinumab in the treatment of RA reported that 7/123 (5.7%) of patients had ADAs, while 4/123 (3.3%) had neutralising ADAs. 77 In this study, serum concentrations of ustekinumab were generally lower in ADA-positive patients 77 (Table 2). There is evidence that neutralising ADAs against ustekinumab were associated with lower drug levels and loss of clinical efficacy in psoriasis and Crohn’s disease,100,101 suggesting overall that they may have similar impact in inflammatory arthritis. The relevance of ustekinumab immunogenicity is yet to be studied in children.
Very low prevalence of ADAs against IL-17 blockade has been reported, and no impact on side effects or clinical efficacy
Secukinumab is a mAb targeting IL-17A. The treatment is not licensed for children. In a recent systematic review, the prevalence of ADAs against secukinumab was 0–1%. 28 A study evaluated the prevalence of ADAs at 52 weeks in patients with psoriasis, PsA and AS treated with secukinumab and found it to be <1%; ADAs were not associated with loss of efficacy, changes in drug levels or adverse events. 74
Ixekizumab is a humanised mAb which targets IL-17A used for the treatment of plaque psoriasis, PsA and AS. The prevalence of ADAs was 5.3% 75 and 9% 76 in adult patients with psoriasis and PsA, respectively, and they occurred within the first 12 weeks of treatment. 76 ADAs were found to be non-neutralising and did not correlate with the rate of adverse reactions (Table 2). Patients with psoriasis or PsA who developed ADAs against ixekizumab had low and constant titres, which did not significantly impact clinical response. No data in children are available.
ADAs against IL-1 blockade do not have significant impact on clinical efficacy or side effects
Anakinra is a recombinant a human IL-1 recombinant receptor antagonist initially trialled in RA, where it has been associated with a prevalence of ADA ranging from 50.1% to 70.9%.78,79 Similar to other recombinant proteins, only a small proportion of ADAs were neutralising (25/1240, 1.9%) 78 (Table 2). Of these 25 RA patients, 13 (52%) reported disease progression; however, no relationships were found between neutralising antibody status and the occurrence of severe allergic reactions, malignancies, opportunistic infections, or serious infections. 78 One study assessing the efficacy of anakinra in patients with JIA found that the prevalence of ADAs increased from 75% at 12 weeks to 82% at 12 months. 80 At 12 weeks, all 4/64 (6%) of patients who had neutralising antibodies to anakinra were non-responders to treatment. 80 However, non-neutralising antibodies to anakinra were not associated with a reduced response to treatment. 80 There have been no studies analysing the association between ADAs to anakinra and adverse events in JIA.
Canakinumab is a fully human mAb against anti-IL-1β used in systemic-onset JIA (soJIA). Studies in children with systemic JIA found a prevalence of ADAs against canakinumab of 3.1% (6/196), 81 and 8%, 82 and ADAs had no neutralising capacity and did not affect the drug levels or the rate of side effects.
Rilonacept is a fully human dimeric fusion protein that acts as a soluble decoy receptor which blocks IL-1β. An RCT in soJIA did not find an association between ADA positivity and clinical response. 83 This trial found that 54.2% (13/24) of patients developed ADA during the 23-month period of open-label treatment (following a 4-week double-blind treatment phase). There was no correlation between ADA positivity and plasma levels of rilonacept. 83 Although the sample size was small, this study noted that the patients who developed at least three injection-site reactions were all ADA positive, thus suggesting there is an association between ADAs and adverse effects.
Conclusion
Immunogenicity to biologic treatment has been investigated in various types of inflammatory arthritis in children and adults. The overall impression is that immunogenicity to biologics used in rheumatology was not particularly confounded by clinical indication or significantly affected by patients’ age (Table 3). However, a direct comparison between the studies evaluated by this report is not possible, because of the high study heterogeneity, a low number of studies investigating less commonly used biologic treatments and high variability between the methods of ADA detection and time points of ADA measurements, study design and concomitant MTX therapy.
Comparison between the prevalence ranges for ADAs to various biologic agents in adult versus paediatric populations.
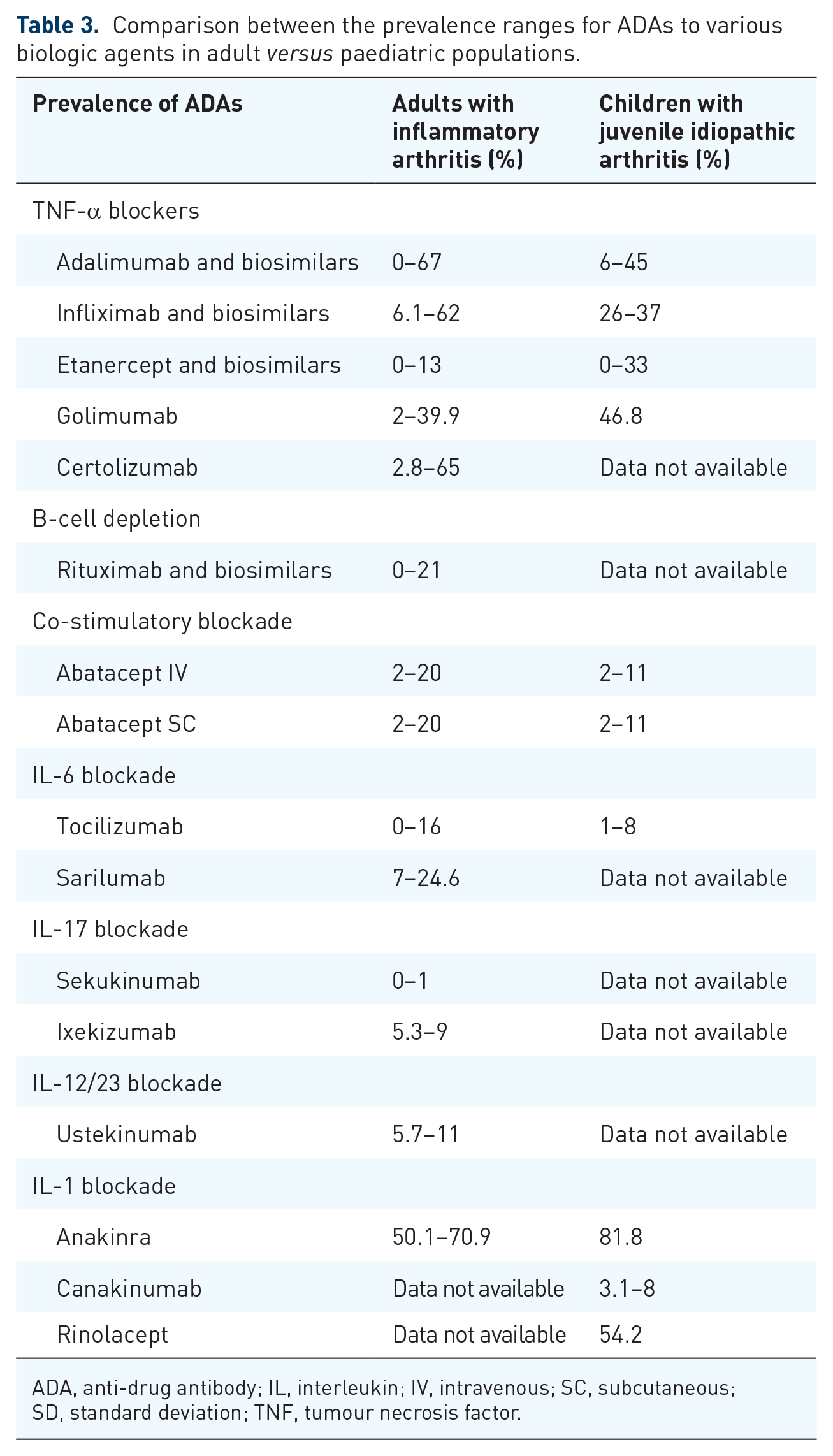
ADA, anti-drug antibody; IL, interleukin; IV, intravenous; SC, subcutaneous; SD, standard deviation; TNF, tumour necrosis factor.
As there are some differences between the biologic agents approved for use in paediatric versus adult rheumatic diseases, in some cases there were no data available to enable comparisons between the two populations (e.g. certolizumab, sarilumab, secukinumab, ustekinumab and ixekizumab have no studies in children, while rilonacept and canakinumab are not commonly used in adults). The discrepancy found between the rate of ADAs against golimumab is not easy to interpret because they have been investigated only in one study in JIA.
This literature review provided evidence for variable prevalence of ADAs depending on the study methodology, sample size, time points for sample evaluation, concomitant DMARD therapy, as well as laboratory assays used for ADA detection. Overall, the highest ADA prevalence was found in patients treated with mAbs against TNF-α and recombinant human IL-1 receptor antagonist (anakinra), although the impact of ADAs on clinical efficacy was clearly influenced by their neutralising properties and impact on drug levels. In contrast to immunogenicity to IL-1 blockade, which had minimal or no impact on clinical efficacy as the proportion of neutralising ADA was very low, ADA against adalimumab, infliximab, certolizumab, and to a certain extent, golimumab had a significant impact on clinical efficacy. As a consequence, the choice of biologic therapeutic agent for individual patients influences their immunogenicity monitoring strategy.
All mAbs against TNF-α (and their biosimilars) were associated with higher prevalence of ADAs than etanercept (a fusion protein) and this is probably explained by the structure of the biologic agent as well as frequency of administration, which in the case of etanercept, ensures more constant serum drug levels. It is recognised that anti-idiotypic ADAs against therapeutic mAbs usually target the drug-binding site, as this does not belong to the patient immunoglobulin repertoire, therefore these ADAs have neutralising properties with impact of drug efficacy and they are clinically relevant. 33 The detection of neutralising ADAs in certain patients should be monitored and correlated with clinical response and drug levels to guide further therapeutic decisions. 102 Neutralising ADAs have been found in patients treated with adalimumab, infliximab, certolizumab pegol and golimumab, as well as tocilizumab, ustekinumab and secukinumab.
By contrast, in the case of fusion proteins which comprise a naturally occurring receptor fused with the constant region of human Ig, the immunogenicity process is primarily triggered by the recognition of the fusion part of the molecule with no direct impact on the drug-binding site. Overall, these therapeutic agents were associated with less immunogenicity, although neutralising ADAs against fusion proteins have also been described with both etanercept and abatacept,65,103 suggesting that their monitoring could be relevant in selected categories of patients, especially if the treatment has been discontinued temporarily.
Despite the potential side effects associated with the presence of ADAs overall, irrespective of their neutralising properties, detection of ADAs does not preclude loss of clinical response, as long as it does not reduce the serum concentration of the biologic agent below the therapeutic threshold, 33 therefore monitoring of ADA without drug levels has no clinical relevance.
High ADA concentration correlated with lower drug levels and impact on clinical efficacy when patients of all ages were treated with adalimumab, infliximab, golimumab, certolizumab, rituximab, abatacept, anakinra, canakinumab, and possibly ustekinumab, while the presence of ADA had less impact on clinical efficacy in adult patients treated with IL-6 and IL-17 blockage and children treated with rilonacept (IL-1β decoy receptor). Patients with higher ADA titres and lower or not/detectable drug levels are probably at risk of losing clinical efficacy and need to be monitored more closely.
It is clinically important to take into consideration the fact that not all detectable neutralising ADAs had impact on clinical outcomes (e.g. tocilizumab ADAs lowered treatment response in children with JIA but less in adults with RA). Neutralising ADAs were more commonly found in patients treated with mAbs compared with fusion proteins; however, not all ADAs against mAbs had neutralising properties or impact on clinical efficacy (e.g. ADAs against ixekizumab were predominantly non-neutralising and did not influence clinical response).
The timing of developing ADAs varied according to the type of biologic treatment and patients’ age. Patients developed ADAs against adalimumab earlier in their disease course, while ADAs in children with JIA treated with abatacept increased with longer time exposure to the drug.
Although data from paediatric studies are scarce overall, studies found that younger age in children with JIA was associated with a higher prevalence of ADAs, as well as side effects to certain biologics, suggesting that caution in monitoring younger patients is advisable.
There is good evidence that higher doses of rituximab and infliximab, as well as more regular administration (as in the case of etanercept) were associated with lower ADA prevalence, suggesting that medication discontinuation and tapering biologic treatment doses could have impact on clinical efficacy. Monitoring patients’ compliance and taking into consideration their dosing regimen, route and frequency of biologic medication administration are important aspects of immunogenicity risk assessment. Increasing treatment dose as well as switching to intravenous formulations can lower the ADAs and restore treatment response; therefore, these are useful therapeutic strategies to address the clinical impact of drug-induced immunogenicity.
In addition, the large variability of ADA levels against biologic agents detected in various adult and paediatric studies of inflammatory arthritis is very likely influenced by the sensitivity of the assay used, concomitant MTX dose, time point of sample collection, as well as patients’ characteristics (genetic background, smoking, age). The overall impact of ADAs on drug efficacy, as well as therapeutic drug monitoring, are particularly relevant in guiding future therapeutic strategies of tapering biologic treatments in inflammatory arthritis patients,102,104 although further research related to their impact on clinical decision making is required.16,84
Based on data available in the literature, concomitant treatment with MTX to address the risk of immunogenicity is recommended in patients treated with abatacept, infliximab, golimumab, while in the case of treatment with etanercept, abatacept and tocilizumab, the impact of additional MTX is not significant.
We propose a potential strategy for drug immunogenicity monitoring for improved clinical benefit (Figure 1). The main clinical instances when ADAs and drug levels should be monitored is loss of clinical efficacy, monotherapy with biologic agents recommended to be prescribed in addition to MTX, clinical reasons for frequent dose intermittent discontinuation, in patients who tapered biologics (especially administered subcutaneously), patients who develop infusion/injection reactions and other side effects to therapy. Further research especially focused on patient individual risk to develop immunogenicity to biologics is required to enable personalised therapy selection.

Potential clinical applications of the assessment of immunogenicity to biologic treatments.
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: ECJ and CC were supported by NIHR UCLH Biomedical Research Centre grants (BRC772/III/EJ/101350 and BRC525/III/CC/191350). LC was supported by the UCL and Birkbeck MRC Doctoral Training Programme. This work was performed within the Centre for Adolescent Rheumatology Versus Arthritis at UCL. UCLH and GOSH were supported by grants from versus Arthritis (21593 and 20164), GOSCC, and the NIHR-Biomedical Research Centres at both GOSH and UCLH. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.