
Abstract
Background:
Intra-articular corticosteroids are commonly used for pain relief in patients with knee osteoarthritis. Simultaneous intra-articular corticosteroid (CS) knee injections may be beneficial for the ~80–90% of patients who present with, or develop, bilateral knee osteoarthritis, but concurrent injections may increase systemic CS exposure and data on safety/tolerability are lacking. Triamcinolone acetonide extended release (TA-ER) has shown decreased systemic triamcinolone acetonide exposure compared with traditional triamcinolone acetonide crystalline suspension (TAcs) after a single knee injection in patients with knee osteoarthritis. This phase IIa study was designed to assess the safety and systemic triamcinolone acetonide exposure following injections of TA-ER or TAcs into each knee of patients with bilateral knee osteoarthritis.
Methods:
Patients (⩾40 years) meeting American College of Rheumatology criteria for knee osteoarthritis in both knees received concurrent single intra-articular injections of TA-ER 32 mg or TAcs 40 mg into each knee (total: 64 mg and 80 mg, respectively) and were followed for 6 weeks. Safety was evaluated based on treatment-emergent adverse events (TEAEs). Blood samples for pharmacokinetic analysis were collected pre-injection, and at the following postinjection time points: 1, 2, 3, 4, 5, 6, 8, 10, 12, and 24 h, and days 8, 15, 29, and 43.
Results:
Baseline characteristics were balanced between patients randomly assigned to TA-ER (n = 12) or TAcs (n = 12). Both treatments were well tolerated with comparable TEAE profiles. Peak plasma triamcinolone acetonide concentrations (Cmax) were lower following bilateral TA-ER injections [geometric mean, 2277.7 pg/ml (95% CI, 1602.13–3238.04)] compared with bilateral TAcs injections [7394.7 pg/ml (2201.06–24,843.43)], with median times to Cmax (Tmax) of 4.5 and 6.5 h, respectively.
Conclusions:
In patients with bilateral knee osteoarthritis, intra-articular injection of TA-ER into both knees was well tolerated. Consistent with pharmacokinetic profiles observed after a single knee injection, plasma triamcinolone acetonide concentrations were lower after bilateral TA-ER injections compared with the higher and more variable concentrations observed after bilateral TAcs injections.
ClinicalTrials.gov identifier:
NCT03378076
Keywords
Introduction
Osteoarthritis is a chronic disease characterized by varying degrees of joint pain, stiffness, swelling, and decreased flexibility. 1 Osteoarthritis affects more than 30 million US adults and is associated with progressive loss of function, leading to diminished health-related quality of life and varying levels of disability.2–4 Inflammation plays a role in articular cartilage degeneration and osteoarthritis development, and contributes to increased joint pain and swelling.5,6 As such, anti-inflammatory intra-articular corticosteroid injections are often used to alleviate synovial inflammation and pain in patients with osteoarthritis, including knee osteoathritis. 7
More than one-quarter (26%) of patients with chronic knee pain initially present with bilateral radiographic evidence of knee osteoarthritis, and 80% of patients who initially present with unilateral knee pain also subsequently develop radiographic evidence of knee osteoarthritis in both knees over the following 12 years. 8 Compared with unilateral knee pain, bilateral knee pain may be associated with further functional limitations, decreased health-related quality of life, and inadequate symptom relief with topical or oral pain medications.9–11 In clinical practice, however, physicians may hesitate to perform simultaneous bilateral intra-articular corticosteroid injections, given that rapid efflux of corticosteroid from the joint after injection of a traditional intra-articular corticosteroids [e.g. triamcinolone acetonide crystalline suspension (TAcs)] into both knees may increase the risk of systemic adverse effects.12,13 At this time, there is limited data on the safety and tolerability of simultaneous bilateral intra-articular injections using traditional corticosteroids, and there are no published clinical treatment guidelines for the management of patients with bilateral disease.14–16
Triamcinolone acetonide extended-release (TA-ER), approved in 2017 by the United States Food and Drug Administration for pain associated with knee osteoarthritis, was designed to limit the rapid efflux from the joint and increase the duration of pain relief. 17 The pharmacokinetics, safety, and efficacy of a single intra-articular injection of TA-ER (32 mg) have been previously studied in patients with unilateral knee osteoarthritis, or in patients with bilateral knee osteoarthritis for whom only the more painful knee was treated.12,18,19 Quantifiable triamcinolone acetonide levels were detected in synovial fluid through 12 weeks following injection, and plasma triamcinolone acetonide concentrations indicated some systemic absorption and a plateau in plasma triamcinolone acetonide concentrations through 24 h postinjection, followed by a slow systemic elimination, further suggesting prolonged residence in synovial tissues. Patients treated with TA-ER had markedly lower systemic triamcinolone acetonide concentrations compared with TAcs (geometric mean peak plasma concentrations were 836.4 pg/ml and 9628.8 pg/ml for TA-ER and TAcs, respectively).12,17 The unique pharmacokinetic profile of TA-ER may contribute to the greater magnitude and duration of effect observed in clinical trials using knee osteoarthritis-specific outcome measures. In a phase III study, a single intra-articular injection of TA-ER improved Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)-A (pain), -B (stiffness), and -C (function) and Knee Injury and Osteoarthritis Outcome Score Quality of Life (KOOS-QOL) scores compared with TAcs at Weeks 4, 8, and 12 (p < 0.05; prespecified exploratory secondary endpoints), while offering a comparable safety profile. 19
In order to examine whether concurrent intra-articular corticosteroid injections into both knees result in a different triamcinolone acetonide pharmacokinetic profile or an additive adverse effect profile, this study was designed to assess the safety and systemic triamcinolone acetonide exposure of simultaneous bilateral intra-articular injections of TA-ER or TAcs in patients with knee osteoarthritis in both knees.
Methods
Patient eligibility and study design
A phase IIa, randomized, open-label, parallel-group study of TA-ER in patients with bilateral knee osteoarthritis was performed at three centers in the United States. This study was conducted per Declaration of Helsinki and International Council on Harmonisation Good Clinical Practice guidelines. A central institutional review board approved the protocol (IRB # 201707059 Schulman Central IRB, Cincinnati, OH, USA) and patients provided written informed consent prior to any study-related procedures. This study was registered on ClinicalTrials.gov before the first patient was enrolled (ClinicalTrials.gov identifier: NCT03378076).
The study enrolled ambulatory men and women ⩾40 years of age who had symptoms consistent with knee osteoarthritis in both knees for ⩾6 months and pain in both knees for ⩾15 days during the preceding month (patient self-reported). Patients were also required to meet the American College of Rheumatology criteria (clinical and radiological) for knee osteoarthritis in both knees (i.e. knee pain, radiographic evidence of osteophytes, and at least one of the following: >50 years of age, morning stiffness <30 min, or crepitus). 20 Inclusion criteria also included body mass index ⩽40 kg/m2 and morning serum cortisol within normal range (171–535 nmol/l). All patients indicated willingness and ability to comply with the study procedures and visit schedules, and ability to follow verbal and written instructions prior to enrollment, including abstaining from using intravenous, intramuscular, oral, inhaled, intranasal, or topical corticosteroids, intra-articular corticosteroids in any joint, intra-articular viscosupplementation (hyaluronic acid derivatives) in either knee, immunomodulators, immunosuppressive or chemotherapeutic agents, or live or live-attenuated vaccines. Exclusion criteria included systemic inflammatory joint disease (including reactive arthritis, rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, or arthritis associated with inflammatory bowel disease), a history of infection in either knee joint, clinical signs and symptoms of active knee infection or crystal disease in either knee within 1 month, or an unstable joint (i.e. torn anterior cruciate ligament) in either knee within 12 months. Patients who had received any intra-articular therapy with corticosteroids (including TA-ER) or biologic agent in any joint within 6 months; hyaluronic acid in either knee, within 6 months, or parenteral or oral corticosteroids within 3 months; inhaled, intranasal, or topical corticosteroids within 2 weeks; or other investigational drug, biologic, or device within 3 months were also excluded, as were patients using insulin or oral medication as treatment for diabetes or who had hemoglobin A1c > 7.5% (>59 mmol/mol). Patients fulfilling inclusion/exclusion criteria were enrolled and randomly assigned 1:1 to receive TA-ER or TAcs using a centralized randomization system. Patients received single intra-articular injections of TA-ER 32 mg (the FDA-approved dose 17 ) or TAcs 40 mg (a dose routinely used in clinical practice) into each knee (totals: 64 mg and 80 mg, respectively) and were followed for 6 weeks.
Procedures
TA-ER (Zilretta®, Flexion Therapeutics, Inc., Burlington, MA, USA) and TAcs (Kenalog®-40, Bristol-Myers Squibb, Princeton, NJ, USA) were prepared per manufacturer’s instructions.17,21 Intra-articular injections were administered by a qualified medical practitioner at the study site, who chose the position of the knee (e.g. extended or flexed) and the approach for the injection (e.g. medial or lateral). Aspiration of each knee was attempted prior to administration, followed by injection of 5 ml reconstituted TA-ER or 1 ml TAcs into the synovial space. The injection into the second knee was administered within 15 min of the injection into the first knee. Patients were asked to avoid strenuous activities or prolonged weight-bearing activities for 24–48 h after injection and maintain a stable level of physical activity during study participation.
Blood samples for pharmacokinetic analysis were collected at pre-injection (within 1 h) and 1, 2, 3, 4, 5, 6, 8, 10, 12 (day 1), and 24 h (±2 h, day 2) postinjection into the first knee and at days 8, 15, 29, and 43 (as convenient). Each patient contributed a total of 15 samples with each sample representing 4 ml of blood, for a maximum estimated total volume of 60 ml of blood collected from each patient for triamcinolone acetonide concentration measurements. Blood samples for pharmacodynamic analysis of morning cortisol levels were also obtained between 7 a.m. and 9 a.m. at screening (within 14 days of dosing) and on days 1 (predose), 2, 8, 15, 29, and 43.
Analysis
Assuming a 10% noncompliance rate for providing complete blood samples for pharmacokinetic analysis, a sample size of 12 patients per treatment arm was considered sufficient to characterize the comparative pharmacokinetic profiles of TA-ER and TAcs. The safety population included all patients receiving at least one dose of study drug. The pharmacokinetic population included all patients who received both intra-articular injections (one into each knee), completed scheduled blood sampling, and had sufficient plasma concentration data to allow calculation of pharmacokinetic parameters. Descriptive statistics were calculated by time point for pharmacokinetic parameters. Bioequivalence testing was performed using average bioequivalence methods in accordance with US Food and Drug Administration guidance. 22
Safety was evaluated for the safety population based on treatment-emergent adverse events (TEAE), physical exams, bilateral knee assessments, vital signs, and clinical laboratory evaluations on day 1 and through the final visit.
Plasma triamcinolone acetonide concentrations were determined using a validated liquid chromatography-mass spectrometry/mass spectrometry method. Pharmacokinetic parameters were calculated for each patient in the pharmacokinetic population using model-independent methods (i.e. noncompartmental analysis) and actual sampling times in Phoenix 7, WinNonlin® (version 7; Certara, L.P., Princeton, NJ, USA). Maximum concentration (Cmax) and time to Cmax (Tmax) were based on observed triamcinolone acetonide concentrations. Area under the curve (AUC) from time 0 to 24 h (AUC0–24h) and to the last quantifiable concentration (AUC0–t) were estimated using the trapezoidal rule. AUC extrapolated to infinity (AUC0–inf), total body clearance (CL), terminal half-life (T½), mean residence time (MRT), and volume of distribution at steady state [V(ss)] were estimated using the slope estimate for the terminal elimination rate constant.
Pharmacodynamic assessment of serum cortisol was evaluated for the safety population.
Results
A total of 24 patients were enrolled, and 12 patients were randomly assigned to each study arm (Figure 1). All patients (n = 24) met the American College of Rheumatology classification criteria (clinical and radiological) for knee osteoarthritis in both knees. 20 Baseline characteristics of patients randomized to each arm were well balanced (Table 1). All 24 patients received both intra-articular injections of study drug, one into each knee.
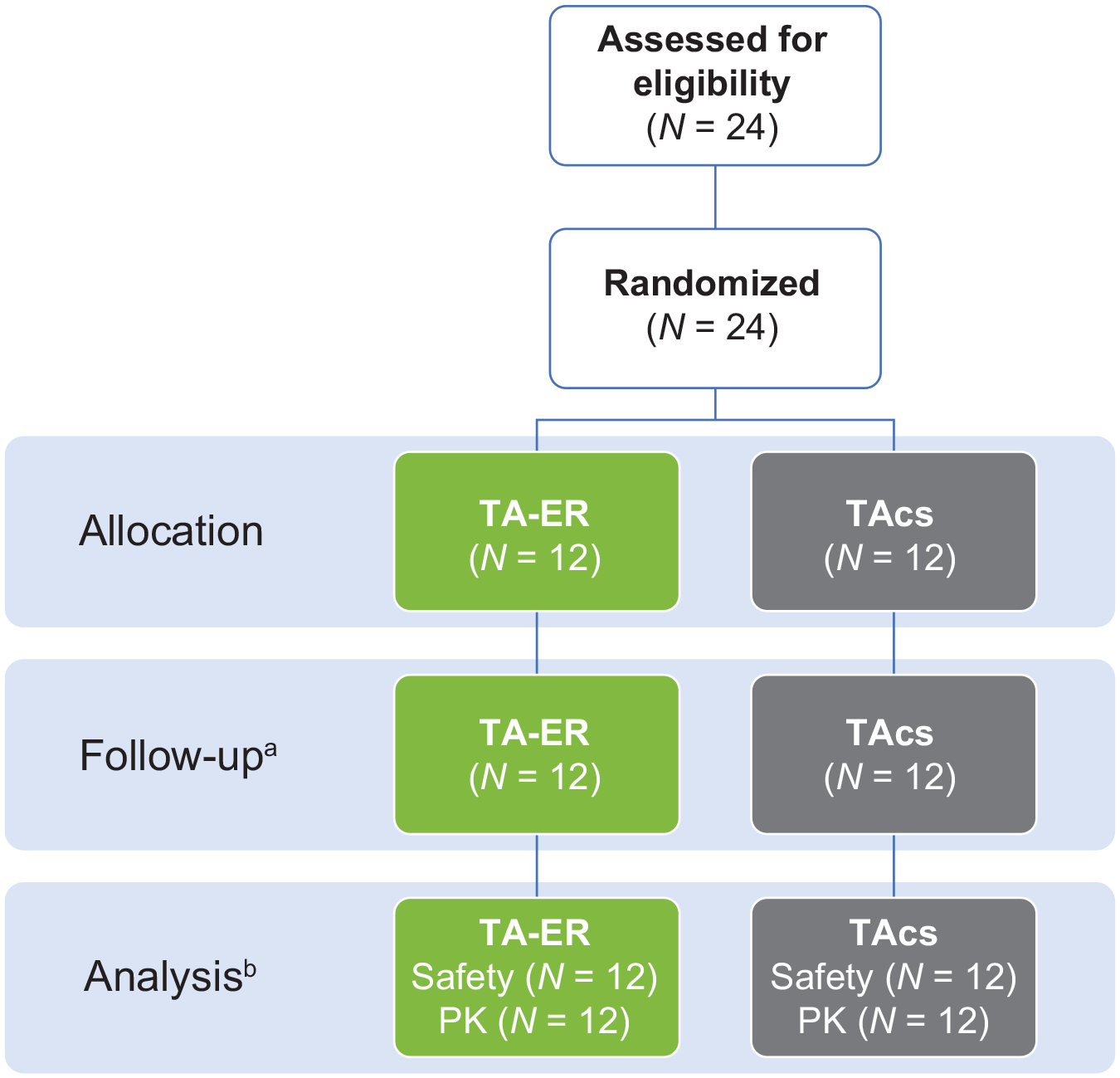
Study design.
Demographics and baseline characteristics.

Patients may have been counted in more than one category.
SD, standard deviation; TAcs, triamcinolone acetonide crystalline suspension; TA-ER, triamcinolone acetonide extended-release.
Safety analysis
TA-ER and TAcs were well tolerated and exhibited comparable safety profiles (Table 2). TEAEs occurred in eight patients (67%) receiving TA-ER and five patients (42%) receiving TAcs. Most TEAEs were Grade 1 or 2 and unrelated to the study drug. One patient receiving TA-ER had simultaneous TEAEs of Grade 3 decreased neutrophil count and Grade 2 decreased white blood cell count; no concurrent infection was reported and treatment was not required. Both events were resolved upon follow-up 1 month later. No patient in either treatment arm experienced a serious TEAE or had a TEAE leading to study discontinuation.
Summary of adverse events.
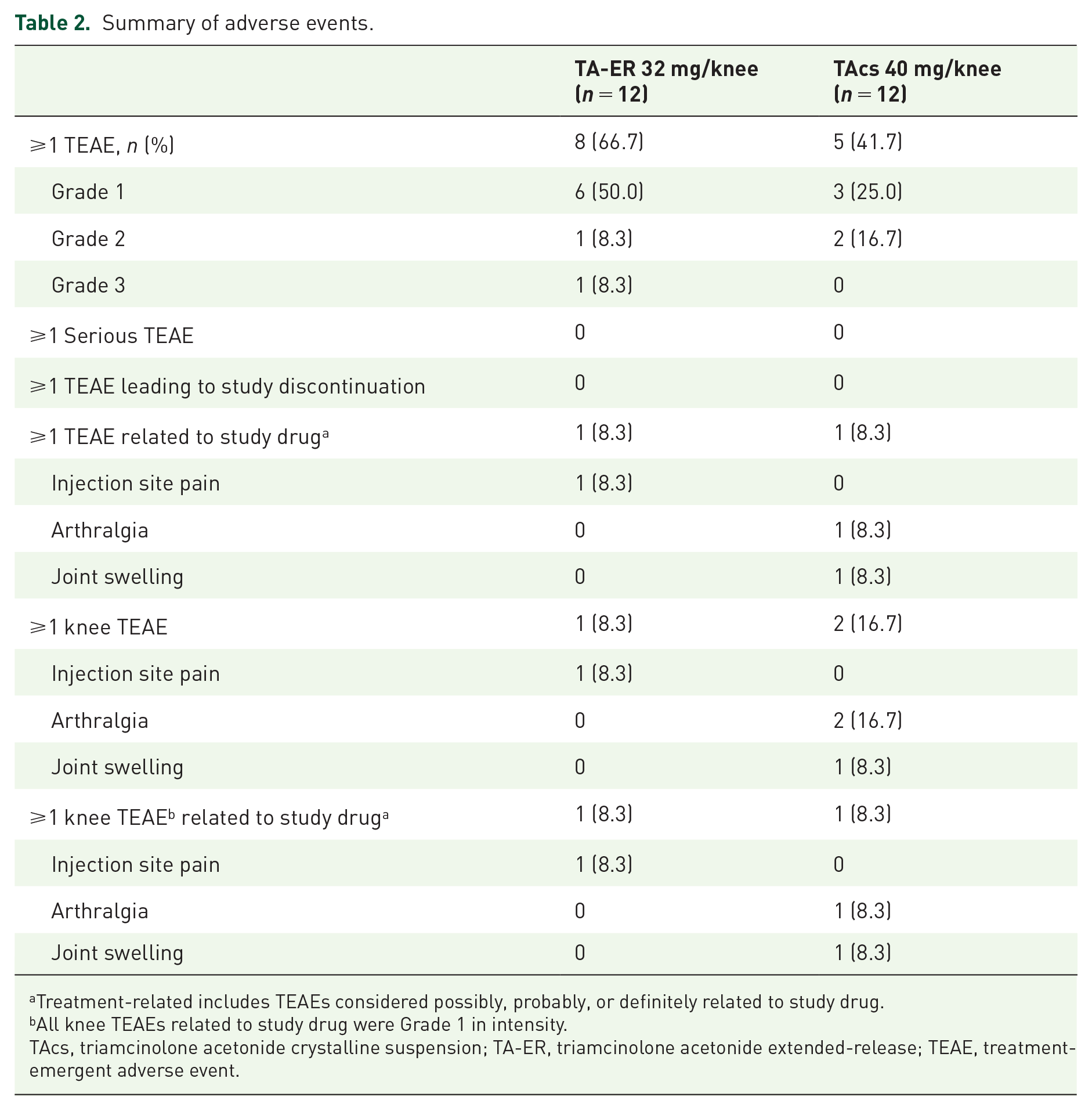
Treatment-related includes TEAEs considered possibly, probably, or definitely related to study drug.
All knee TEAEs related to study drug were Grade 1 in intensity.
TAcs, triamcinolone acetonide crystalline suspension; TA-ER, triamcinolone acetonide extended-release; TEAE, treatment-emergent adverse event.
Plasma pharmacokinetic analysis
All patients contributed samples for determination of plasma concentrations from baseline through day 43. After TA-ER injection, triamcinolone acetonide plasma concentrations peaked after a median of 4.5 h with a geometric mean Cmax of 2277.7 pg/ml (95% CI, 1602.13–3238.04), whereas, after TAcs injection, triamcinolone acetonide plasma concentrations peaked after a median of 6.5 h with a geometric mean Cmax of 7394.7 pg/ml (95% CI, 2201.06–24,843.43) (Figure 2 and Table 3). Overall, systemic exposure, as measured by AUC, was also lower for TA-ER than TAcs, but TA-ER use was associated with a longer MRT (Table 3). Bioequivalence testing confirmed that the systemic exposures of TA-ER and TAcs were not equivalent.

Plasma triamcinolone acetonide concentrations over time after bilateral injection of TA-ER or TAcs. (a) Log-linear geometric mean (95% CI) baseline to day 43. (b) Linear-linear geometric mean (95% CI) baseline to day 43. (c) Log-linear geometric mean (95% CI) baseline to 24 h. (d) Linear-linear geometric mean (95% CI) baseline to 24 h.
Plasma pharmacokinetic parameters.

AUC0-24 h, area under the concentration-time curve from time 0 to 24 h post-injection; AUC0-inf, area under the concentration-time curve from time 0 extrapolated to infinity; AUC0-t, area under the concentration-time curve from time 0 to the last quantifiable concentration (t).
CI, confidence interval; CL, total body clearance; Cmax, maximum plasma concentration; GM, geometric mean; MRT, mean residence time; TAcs, triamcinolone acetonide crystalline suspension; TA-ER, triamcinolone acetonide extended-release; T1/2, terminal half-life; Tmax, time to maximum concentration; V(ss), volume of distribution at steady-state.
Morning serum cortisol analysis
The pharmacodynamic effects of TA-ER and TAcs on function of the hypothalamic-pituitary-adrenal axis were evaluated by morning serum cortisol measurement. Serum cortisol fell below the normal range (171–535 nmol/l) on day 2 postinjection for both treatments (Table 4). Cortisol returned to within normal range by the day 8 visit for patients in the TAcs group and the day 29 visit for patients in the TA-ER group (Table 4).
Morning serum cortisol concentration (nmol/l) over time, mean (SD).
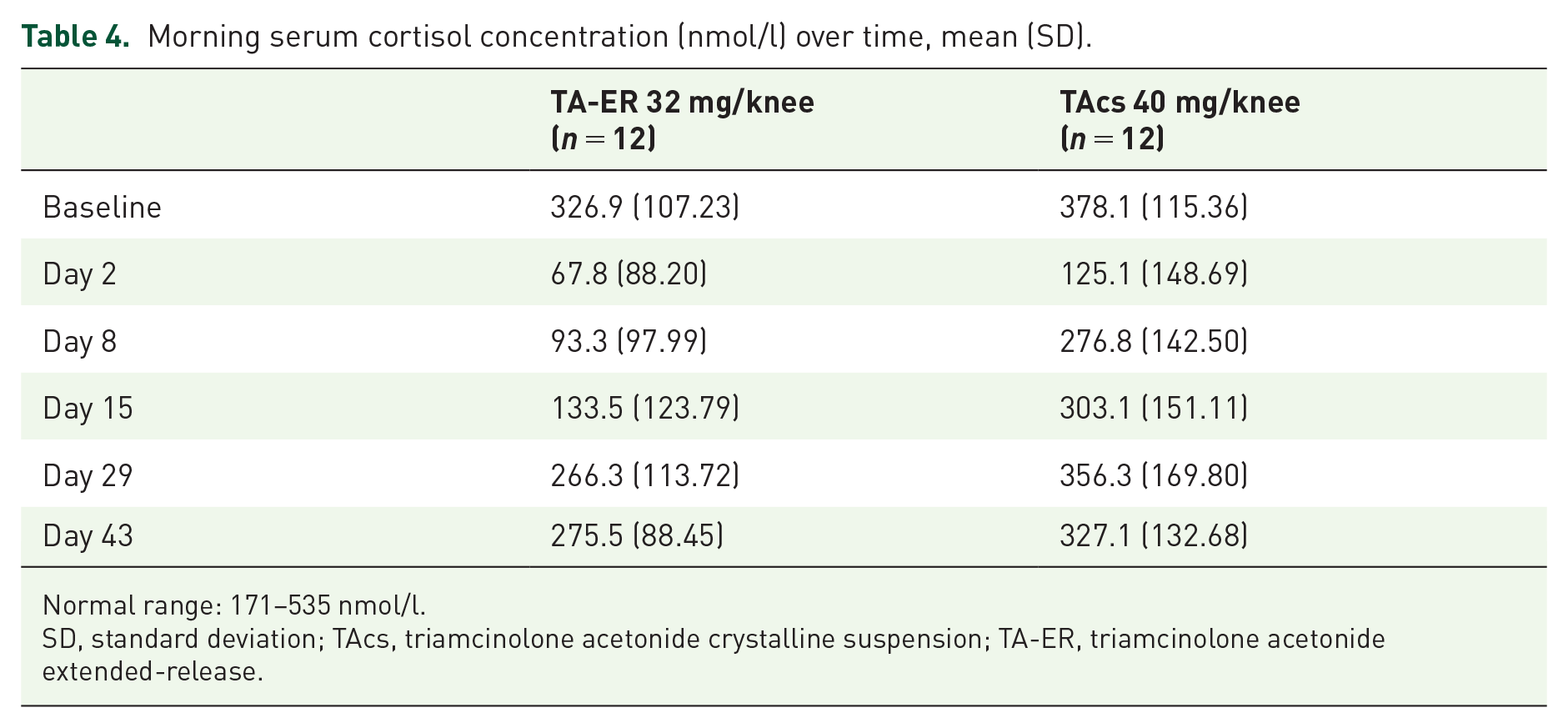
Normal range: 171–535 nmol/l.
SD, standard deviation; TAcs, triamcinolone acetonide crystalline suspension; TA-ER, triamcinolone acetonide extended-release.
Discussion
A substantial proportion of patients with knee osteoarthritis develop bilateral disease, leading to increased pain and functional limitations.8,9 However, among randomized/quasi-randomized controlled clinical trials designed to assess the safety and efficacy of intra-articular corticosteroids, 7 less than half specifically address inclusion of patients with bilateral knee osteoarthritis, and few include treatment of both knees. Due to a lack of evidence, current clinical treatment guidelines do not provide guidance on the appropriateness of simultaneously treating both knees in patients with bilateral knee osteoarthritis.14–16 Given the prevalence of bilateral knee osteoarthritis, it is important to understand the risks and benefits of simultaneously treating both knees with intra-articular corticosteroid injections, particularly given the potential for additive adverse effects associated with increased systemic corticosteroid levels.
Results from this phase IIa randomized, open-label, parallel group study demonstrated that an extended-release poly (lactic-coglycolic acid) microsphere-based formulation of triamcinolone acetonide (TA-ER), injected bilaterally in patients with osteoarthritic knees, was well tolerated and no new or unexpected safety concerns were identified. This is consistent with results from previous single-injection studies, in which TEAEs were predominantly mild or moderate (Grade 1 or Grade 2), nonserious, and considered to be unrelated to the study drug.12,18,19
Overall, the triamcinolone acetonide pharmacokinetic profile associated with bilateral TA-ER injection was generally similar to that observed for single-injection TA-ER administration.12,14 As expected, peak plasma triamcinolone acetonide concentrations were higher, and times to peak triamcinolone acetonide concentrations were shorter, in patients receiving TA-ER into both knees (Cmax; geometric mean: 2277.7 pg/ml; Tmax: 4.5 h) compared with administration to a single knee (966.7 pg/ml; 7.0 h). These differences were roughly dose-proportionate (64 mg for bilateral injections, 32 mg for single injections). 12
Although initial systemic absorption of triamcinolone acetonide was rapid following bilateral injection of TA-ER or TAcs (Tmax of 4.5 and 6.5 h, respectively), peak plasma triamcinolone acetonide concentrations were substantially lower (approximately threefold) in patients treated with TA-ER. An order of magnitude of difference in systemic triamcinolone acetonide exposure was observed in patients who received a single intra-articular injection of TA-ER or TAcs into one osteoarthritic knee, 12 and is supported by the longer MRT for TA-ER, which indicates a slower release of triamcinolone acetonide into the systemic circulation and continued drug presence in the synovium compared with TAcs.
There was wide variability in plasma triamcinolone acetonide concentrations over time in the TAcs treatment group, as shown by large standard errors in Figure 2. This contrasts with the TA-ER treatment group, wherein triamcinolone acetonide concentrations were relatively consistent at each collection point throughout the study. The high level of variability in the plasma triamcinolone acetonide concentrations with TAcs treatment versus the reproducibly low plasma triamcinolone acetonide levels with TA-ER treatment are in line with pharmacokinetic and pharmacodynamic findings from four previous phase II studies comparing single injections of either treatment into one knee (sponsor data on file).12,23 In the pharmacodynamic study in patients with knee osteoarthritis and well-controlled type 2 diabetes, a single injection of TAcs into one knee resulted in greater and widely variable increases in average blood glucose levels, whereas TA-ER treatment produced significantly smaller increases that were less variable. 24 It is possible that triamcinolone acetonide concentrations within the joint vary just as widely as plasma concentrations, and this may explain the wide variations in magnitude and duration of symptom relief observed following traditional intra-articular corticosteroid injections.7,25
Reduced morning serum cortisol levels were observed from day 2 following bilateral intra-articular injections of TA-ER or TAcs. Serum cortisol concentrations remained below normal range with TA-ER at days 8 and 15, possibly because of continued systemic absorption of triamcinolone acetonide from the injected TA-ER. The observed suppression of adreno-cortical secretion reflected in reduced cortisol concentration was transient and cortisol levels returned to within normal range by the day 29 visit following TA-ER. It is notable that cortisol levels were above the threshold for predicting low hypothalamic-pituitary-adrenal axis response (128 nmol/l) 26 by day 15 following TA-ER. The continued reduction in cortisol concentration from pre-injection values observed at days 29 and 43 following TA-ER is not expected to compromise the ability to mount a stress response in patients with a functional hypothalamic-pituitary-adrenal axis. Confirmation would require provocative testing with adrenocorticotropic hormone. These reductions in basal/unstimulated morning cortisol levels build upon the results observed by Habib and colleagues for bilateral intra-articular knee injections of methylprednisolone acetate. 13 Habib and colleagues went on to confirm secondary adrenal insufficiency with adrenocorticotropic hormone stimulation in 60% of methylprednisolone acetate-treated patients 1 week following bilateral injection decreasing to 10% at 8 weeks following injection. 13
Although limited by the small sample size, the study was powered to detect significant differences in exposure means between TA-ER and TAcs.
Conclusion
This phase IIa, randomized, open-label, parallel-group trial demonstrated that intra-articular injection of TA-ER into both knees of patients with bilateral knee osteoarthritis was well tolerated and resulted in reduced systemic triamcinolone acetonide exposure relative to higher and more variable triamcinolone acetonide levels associated with bilateral knee TAcs injection. Plasma triamcinolone acetonide concentration profiles resulting from a single knee injection or bilateral knee TA-ER injections were generally similar, and consistent with TA-embedded microspheres remaining in the synovium after TA-ER injection, with a subsequent slow release into synovial fluid and corresponding slow systemic absorption.
Footnotes
Acknowledgements
The authors thank the patients who participated in this trial and their enrolling investigators.
The authors thank Teresa Curto (Cytel, Waltham, MA, USA) for biostatistical support. Professional medical writing and editing assistance were provided by Kathleen Richards (ApotheCom, Yardley, PA, USA); this support was funded by Flexion Therapeutics, Inc. (Burlington, MA, USA).
Some of the information in this paper was presented in abstract form at the ACR/AHRP 2018 Annual Meeting (Kivitz A, Kwong L, Shlotzhauer, Lufkin J, Curto T, Kelley S. Systemic exposure of triamcinolone acetonide following bilateral injection of extended-release triamcinolone acetonide and standard triamcinolone in patients with bilateral knee osteoarthritis. Arthritis Rheum. 2018; 70[s9]. Abstract 1371)
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and publication of this article: Sponsorship for this study and article processing charges were funded by Flexion Therapeutics, Inc. (Burlington, MA, USA).
Conflict of interest statement
AK has served on a speaker’s bureau for Flexion Therapeutics, Inc. LK has received research grants from Flexion Therapeutics, Inc. AC and SK are employees of Flexion Therapeutics, Inc. and own stock/stock options in Flexion Therapeutics, Inc. TS declares no conflicts of interest. JL is a former employee of Flexion Therapeutics, Inc. and owns stock/stock options in Flexion Therapeutics, Inc.
Data sharing statement
The datasets analyzed within this publication are available from the corresponding author on reasonable request.