
Abstract
This article reviews recent evidence on urate deposition and the opportunity for a therapeutic approach. We reviewed Pubmed 2013–2015 literature using the search terms ‘deposition’ with ‘hyperuricaemia’, ‘gout’, ‘ultrasonography’, ‘DECT’ (dual-energy computed tomography), ‘radiography’, ‘CT’(computed tomography), ‘MRI’ (magnetic resonance imaging), or ‘cardiovascular’, in addition to a digital bibliographic library compiled by the authors with 2072 papers on hyperuricaemia and gout. Relevant papers on the topic were selected. Recent evidence, mostly based on imaging studies, showed a continuum from hyperuricaemia to deposition and clinical manifestations. Chronic inflammation and structural damage may be present even in asymptomatic patients with crystal-proved deposition. The impact of early intervention in patients with asymptomatic deposition either on vascular outcomes or further structural joint damage has not been demonstrated yet. In conclusion, a worldwide definition of gout is still lacking, stages from hyperuricaemia to clinical gout not being definitively defined. Although there is increasing interest on the impact of early deposits on joint damage and cardiovascular outcomes, robust evidence is still lacking to fully support interventions.
Introduction
Gout has been considered as the clinical consequence of the nucleation, growth and aggregation of monosodium urate crystals (MSUCs) in tissues, mostly in structures of the musculoskeletal system. Although academically gout has been divided into different clinical stages, namely acute, intercritical and chronic, this classification may be misleading for both patients and physicians [Perez-Ruiz et al. 2014a], especially as to consider whether gout is not present neither has consequences in the absence of clinical manifestations [Perez-Ruiz et al. 2015], and may subsequently lead to mismanagement [Doherty et al. 2012].
As an example, indications for a recent urate-lowering medication (ULM), such as febuxostat, may differ as definitions of gout vary. Whereas in the EU it is labelled for the ‘treatment of chronic hyperuricaemia in conditions where urate deposition has already occurred (including a history, or presence of, tophus and/or gouty arthritis)’ [EMA, 2015], which may include unequivocal evidence based on imaging or tissue deposits, in the USA, febuxostat is labelled ‘for the chronic management of hyperuricemia in patients with gout’ [FDA, 2015], not specifying a definition for gout, and in Australia it is indicated for the ‘treatment of chronic symptomatic hyperuricaemia in conditions where urate deposition has already occurred (gouty arthritis and/or tophus formation) in adults with gout’ (TGAeBS, 2015), that is, symptoms are needed to apply for an indication.
Definitions
Unfortunately, there is no common definition of gout accepted worldwide, as there is for diabetes or hypertension, which are not necessarily associ-ated with symptoms [Perez-Ruiz et al. 2014a]. Therefore, the pathway from sustained or chronic hyperuricaemia to hyperuricaemia with deposition and gout is nowadays a matter of debate. Making the following definitions ‘crystal-clear’ may help the following discussion.
Hyperuricaemia
Despite the definition of hyperuricaemia being commonly based on the distribution of serum urate (sUA) in the population, which therefore may vary depending on age and gender, from the pathophysiological point of view of MSUC deposition, hyperuricaemia is defined as sUA levels above the threshold for saturation of urate in body fluids, which is considered to be over 0.40 mmol/L [Becker and Ruoff, 2010]. A recent change of definition for hyperuricaemia of gout to a more operative definition has been proposed to overlap that of the therapeutic target for urate-lowering interventions, that is, 0.36 mmol/L [Bardin and Richette, 2014].
Hyperuricaemia with deposition
Imaging studies based on ultrasonography have shown the continuum from hyperuricaemia to deposition [Chowalloor and Keen, 2013]. In 26 asymptomatic subjects showing hyperuricaemia over 2 years, ultrasonography examination of the knees and first metatarsophalangeal joints showed findings of urate deposition in 11/26 (42%), ultrasonography-guided aspiration demonstrating MSUCs in 9/11 (82%) [De Miguel et al. 2011]. These results were confirmed in a controlled study, in which 8/50 (16%) asymptomatic hyperuricaemic subjects also showed intra-articular tophi [Pineda et al. 2011]. More recently, dual-energy computed tomography (DECT) imaging showed urate deposits in 6/25 (24%) subjects with asymptomatic hyperuricaemia, in 11/14 (79%) patients with early (< 3 years) gout, and in 16/19 (84%) patients with established gout (> 3 years) [Dalbeth et al. 2015], suggesting that a critical amount of MSUC deposits may be needed for the development of clinical manifestations.
Therefore a gout condition defined as ‘asymptomatic MSUC deposits’ has been proposed [Bardin and Richette, 2014]. Also, a staging classification has been proposed to differentiate ‘hyperuricaemia, without evidence of MSUC deposition’, asymptomatic MSUC deposition (by microscopy or advanced imaging), but without signs or symptoms of gout [Dalbeth and Stamp, 2014].
Gout
Taking into account the previous considerations, it seems that the definition of gout implies the presence of symptoms. Nevertheless, it seems to be more simply and conceptually applicable to consider gout as ‘the presence of a nonphysiological material (MSUCs) in tissues, independent of the presence or absence of clinical manifestations’ [Perez-Ruiz et al. 2014a]. This definition is applicable to patients with crystal-proved MSUC deposits, including subclinical, early and late gout with typical, atypical, acute or chronic clinical manifestations.
Pathophysiological importance of urate deposition
The key point to consider in therapeutic intervention in subjects with asymptomatic MSUC deposition would be to demonstrate that such deposits are not inert in tissues, and that there is a positive outcome when such interventions are performed. Imaging that captures inflammation, namely ultrasonography or gadolinium-enhanced magnetic resonance imaging (MRI) may help to evaluate further the relationship between MSUC deposition, inflammation and vascular outcomes [Perez-Ruiz et al. 2015].
Inflammation
In patients with gout, MSUCs were found in 36/37 (97%) of knee joints with previous involvement but patients were asymptomatic and in 8/37 (22%) of never-affected joints. The presence of MSUCs was shown to be associated with low-grade inflammation as demonstrated by increased neutrophil counts in the synovial fluid [Pascual, 1991]. Therefore, the MSUCs are not as inert as supposed, even in the absence of clinical manifestations.
An increased power-Doppler signal in ultrasonography, a surrogate for increased vascularity of inflammation, was observed in 67% of 12 asymptomatic patients with MSUC deposition [Puig et al. 2008]. Nevertheless, in a controlled study, power-Doppler positivity was not observed either in hyperuricaemic or normouricaemic controls [Pineda et al. 2011].
There is robust epidemiological evidence of an association between hyperuricaemia and gout with vascular outcomes, probably related to increased risk of atherosclerosis [Krishnan et al. 2011]. Vascular outcomes such as myocardial infarction were associated with gout independently of the presence of hyperuricaemia [Krishnan et al. 2006]. Both high-level hyperuricaemia and deposition (as in patients with subcutaneous gout) are associated with increased mortality in patients with gout [Perez-Ruiz et al. 2014b], but high-level hyperuricaemia may also be associated with subclinical deposition. Recently, an association of ultrasonography detection of MSUC joint deposits with more severe coronary calcification in hyperuricaemic subjects with acute coronary syndrome has been reported [Andres et al. 2014]. Therefore, this raises the question of whether MSUC deposition and low-grade inflammation, among other plausible candidates, are determining factors contributing to vascular outcomes [Richette et al. 2014].
Structural damage
The structural damage in gout is related to the interaction between resident cells in the tissues where MSUCs deposit, both an innate and an adaptative immune response being present [Dalbeth et al. 2010]. The presence of MSUCs in the synovial membrane is associated with the development of chronic foreign body-like granulomas [Schumacher, 1975], similar to those observed in subcutaneous tophi [Dalbeth et al. 2010]. In addition, interaction between MSUCs and other cells such as osteoclasts [Dalbeth et al. 2008] osteoblasts [Chhana et al. 2011] or tenocytes [Chhana et al. 2014] may indicate that MSUCs are not inert crystalline structures and can induce cell responses. Chronic synovitis and deposition may be observed without any structural damage at the onset of symptoms, as shown in Figure 1.
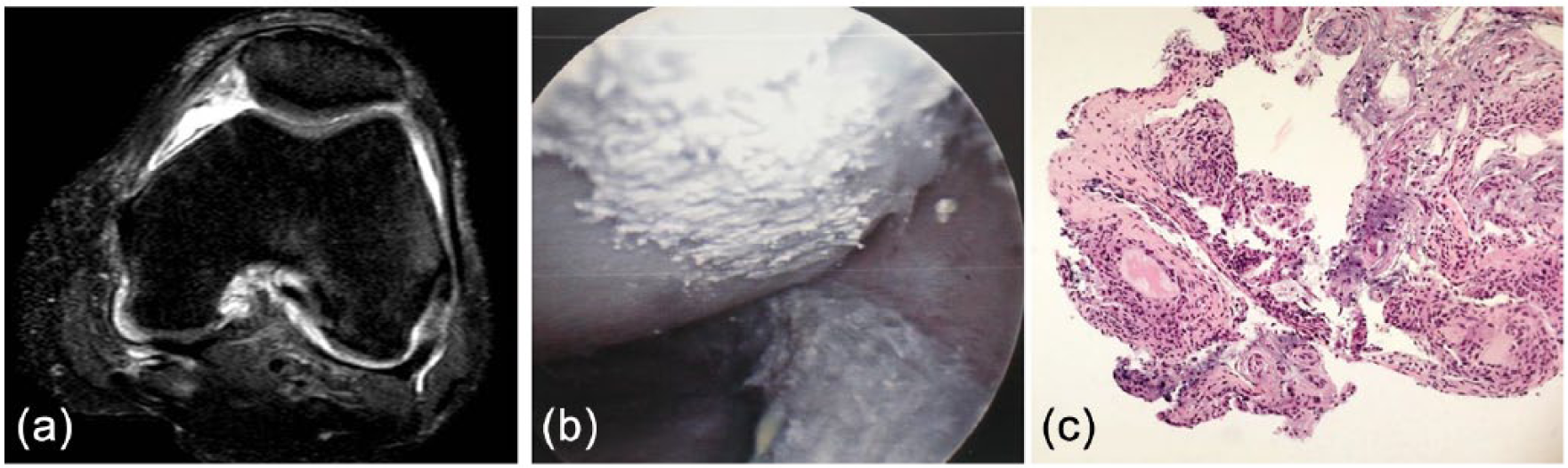
(a) Magnetic resonance imaging of the knee showing no deposition or structural damage at the first presentation of gout. (b) The patient underwent arthroscopy due to suspected infection, with urate deposits showing on the cartilage surface. (c) Synovial biopsy showing areas with chronic, foreign body-like granulomas. (reproduced from Perez-Ruiz et al. [2015] with permission).
Structural damage in gout is mainly evaluated using imaging techniques [Perez-Ruiz et al. 2009b]. Plain X-ray is not sensitive enough to detect early changes in patients with gout, namely bone erosions, compared with ultrasonography [Wright et al. 2006]. Erosions have been observed in a ultrasonographic study in 12% of asymptomatic hyperuricaemic patients versus 5.7% in normouricaemic controls, reported by the authors not to be significant, but further analysis of the frequency of erosions in subjects with and without deposition was unfortunately lacking, so no association between deposition and erosions can be ascertained [Pineda et al. 2011].
Erosions were observed with ultrasonography in 45% of 22 first metatarsophalangeal joints of patients with gout that were completely asymptomatic for such joints, and tophi were observed in 32% of them [Wright et al. 2006].
Increased deposition has been associated not only with erosions and structural damage, but also with a greater number and intensity of acute episodes of inflammation [Gutman, 1973], disability [Dalbeth et al. 2007b], loss of patients` perception of quality of life [Khanna et al. 2011], as well as increased healthcare resource use [Khanna et al. 2012b].
Clinical manifestations
As mentioned above, gout has been academically stratified into consecutive stages, namely acute gout, intercritical gout and chronic gout. This clinical staging is frequently found in clinical practice, but may be misleading in different ways [Perez-Ruiz et al. 2014a]. First, intercritical gout may be considered as an asymptomatic period with no underlying pathogenic process, such as inflammation or tissue damage, and therefore not requiring any therapeutic intervention [Doherty et al. 2012]. Second, the definition may imply that gout, a true deposition disease, is not a chronic condition because of absence of symptoms or apparent clinical manifestations. Lastly, patients presenting with clinical manifestations, considered therefore to be atypical, are not correctly classified and so are misdiagnosed [Perez-Ruiz et al. 2009a].
Untreated, persistent hyperuricaemia in patients with gout has been associated with increasing numbers of episodes of acute inflammation and development of polyarticular joint involvement distribution [Gutman, 1973].
Despite our previous statements, it is not uncommon to observe extensive asymptomatic MSUC deposition in patients treated with corticosteroids [Vazquez-Mellado et al. 1999], as in the patient shown in Figure 2.

Ultrasonography of the knee (a) and finger pad (b) showing hyperechoic areas (tophi) with a power-Doppler signal in a patient with systemic lupus erythematosus treated with corticosteroids. No previous flare, but unspecific arthralgia was retrieved from careful anamnesis. The patient was fully asymptomatic after 6 months of intensive urate-lowering therapy. (reproduced from Perez-Ruiz et al. [2015] with permission).
Detecting deposition, inflammation and structural damage
Although clinical examination may give a sense of the presence of deposition (subcutaneous or periarticular tophi that may be palpated), structural damage (joint limitation and deformity), and inflammation (erythema, swelling or limitation), in clinical practice imaging is becoming the main source of information. This is especially true for early detection of MSUC deposition and subclinical structural damage and inflammation, as shown before. Three core domains for imaging in gout have been recently endorsed by the initia-tive Outcome Measures in Rheumatology (OMERACT): urate deposition (tophi), inflammation and structural damage [Grainger et al. 2015].
Radiographic scores have been used to evaluate structural damage in gout, but are only applied to patients with persistent, or chronic, clinical manifestations [Dalbeth et al. 2007b]. Increasing radiographic scores are associated with an increasing burden of intraosseous tophi [Dalbeth et al. 2009], which was shown half a century ago to be associated with time of exposure to untreated gout and increasing sUA [Gutman, 1973].
Ultrasonography is an office-based imaging technique used to evaluate MSUC deposition, as mentioned above. The double-contour sign (deposits in the articular surface of the hyaline cartilage) and hyperechoic areas surrounded by a hypoechoic halo (tophi) have been considered to be highly specific for gout in the hands of trained observers [Peiteado et al. 2012]. The main limitations to ultrasonography is that inter-observer reliability for the double-contour sign has been reported recently to be moderate (kappa 0.52) in a well-designed study [Naredo et al. 2013]. In addition, ultrasonography can capture structural damage (erosions and joint-space narrowing), synovial thickening (synovitis) and power-Doppler signal (active synovitis and peritophaceous inflammation) [Perez-Ruiz et al. 2009b]. It has also been shown to be sensitive to change during urate-lowering therapy [Perez-Ruiz et al. 2007]. Two different approaches have been studied: extensive ultrasonography scanning of cartilage, tendons and articular space for diagnosis [Naredo et al. 2013], and short (6 min) four-joint (first metatarsophalangeals and knees) ultrasonography scan [Peiteado et al. 2012], but both studies were performed in patients with longstanding gout in whom tophi were not uncommon.
Computed tomography (CT) is useful to evaluate structural damage compared with plain radiographs [Dalbeth et al. 2009]. Limitations include a lack of sensitivity in capturing deposition and inflammation. DECT is an imaging technique that has been shown to be highly specific and reproducible (as it is software based) in detecting MSUC deposits. Although the specificity of DECT is better than that of ultrasonography, the sensitivity of DECT does not seem to be better [Gruber et al. 2014], and ultrasonography performs best in detecting early deposits [Huppertz et al. 2014]. DECT, as CT, is not able to capture inflammation. Artefacts are a common false positive finding with DECT, especially around the nails or skin, but are easily recognized [Mallinson et al. 2014].Technical adjustment of the software has been considered to be a cause of false negative findings with DECT [McQueen et al. 2013]. Sensitivity to change during implementation of urate-lowering therapy has shown conflicting results [Choi et al. 2012; Rajan et al. 2013]. Digital tomosynthesis has recently been proposed as a low radiating, good quality, more feasible and inexpensive alternative to plain radiographs and CT [Dalbeth et al. 2014].
MRI is a multipurpose imaging technique that can evaluate bone, cartilage and soft tissue including tendons, ligaments, synovial membranes and nodules. It can also capture swelling, either in bone and soft tissue, and inflammation (if enhanced with gadolinium) [Perez-Ruiz et al. 2009b]. MRI 3 tesla can be especially useful in evaluating cartilage damage [Popovich et al. 2014], but studies have been limited to wrists.
Treating hyperuricaemia with deposition
As discussed in the introduction, the definition of gout itself may influence the prescription of ULMs as to whether they should only be considered in the presence of symptoms. We will discuss further whether clinical or imaging findings would be needed to consider intervention in patients with asymptomatic deposition. The presence of symptoms such as acute and chronic inflammation, evident tophaceous deposition on physical examination or evident X-ray structural damage are well accepted indications for urate-lowering intervention in guidelines and recommendations [Khanna et al. 2012a; Richette et al. 2014; Zhang et al. 2006); heretofore, the presence of subtle structural damage or small tophaceous deposits observed with imaging techniques still remains to be controversial as an indication for ULT .
Pros
Ultrasonography can be a useful, reliable and accurate office-based tool, compared with CT and DECT, to evaluate the amount and impact of deposits in joint structures. Ultrasonography-guided puncture may also enhance the achievement of gold-standard (observation of MSUCs in microscopy) diagnosis.
Early intervention on hyperuricaemia in patients with crystal-proved deposition, even if asymptomatic, could be considered and discussed with patients, when early structural damage, such as subclinical ultrasonographic findings of bone erosions, deposition shown as articular, nonpalpable tophi, and sound subclinical inflammation, as shown with power-Doppler signal, is present. These findings are not infrequent but present in a number of subjects with asymptomatic hyperuricaemia, what may be called asymptomatic gout or hyperuricaemia with deposition and the starting point for new therapeutic approaches [Perez-Ruiz and Punzi, 2015]. The rational use of colchicine, according to labels, recommendations and guidelines, and ULMs available, is associated with a low rate of serious adverse events [Jennings et al. 2014; Terkeltaub, 2009], and therefore could overweigh the risk of adverse events. Allopurinol initiation in patients with hyperuricaemia or gout has been shown to be associated with a modest reduction in mortality rate, the authors concluding that it probably outweighs the impact of adverse events [Dubreuil et al. 2014].
Evaluation of subclinical inflammation associated with MSUC deposits and the impact of intervention, either colchicine [Crittenden et al. 2012], or ULMs to deplete deposits, and therefore inflammation, could also be considered in patients with early demonstration of urate deposition and high risk for cardiovascular events [Grimaldi-Bensouda et al. 2014], or even chronic kidney disease [Goicoechea et al. 2010, 2015 ]. Targeting different mechanisms, such as hyperuricaemia, inflammation and xanthine oxidase has been proposed [Richette et al. 2014].
Cons
The first formal consideration is that the prescription of ULMs for asymptomatic hyperuricaemia is not widely approved, except in some countries such as Japan, and in certain situations, such as high cardiovascular risk or chronic kidney disease. The indication for hyperuricaemia with proved deposition even in the presence of mild structural damage has not yet been considered, and therefore not labelled.
In the second place, even sophisticated imaging techniques such as high-sensitivity ultrasonography and DECT have not been shown to be fully specific for urate deposition. Therefore, even in the theoretically optimal situation in which crystal-proved deposition is demonstrated associated with early structural damage and inflammation, there is no information available on the impact of such findings on further structural damage or the risk of appearance of meaningful clinical manifestations during the life expectancy of the subject.
In addition, medical errors in prescription and adherence to quality indicators are not infrequent [Mikuls et al. 2005, 2006] adverse events associated with increased rate of comorbid conditions [Franchi et al. 2014]; a systematic review of the allopurinol hypersensitivity syndrome has recently shown that 60% of patients did not have an approved indication for its prescription [Ramasamy et al. 2013], although prescription habits may greatly contribute to the risk of toxicity [Mikuls et al. 2005].
To the authors knowledge there is no definitive study, and a prospective one specifically designed for this purpose is much needed, on whether the impact of early intervention in patients with hyperuricaemia with true urate deposition on the natural history of gout, renal function and cardiovascular events would overweigh the risk of exposure to ULMs. This therefore remains an unanswered question to date.
Footnotes
Funding
This research has received a grant from Asociación de Reumatólogos del Hospital de Cruces.
Conflict of interest statement
FPR has been an adviser/speaker for AstraZeneca, Cymabay and Menarini, and received investigation funds from Ministerio de Sanidad, Gobierno de España, Departamento de Tecnología e Innovación, Gobierno Vasco, Fundación Española de Reumatología, and Asociación de Reumatólogos del Hospital de Cruces.