
Abstract
In the complex system of bone remodeling, the receptor activator of nuclear factor κB ligand (RANKL)/osteoprotegerin (OPG) pathway is the coupling factor between bone formation and bone resorption. RANKL binds to the RANK receptor of pre-osteoclasts and mature osteoclasts and stimulates their activation and differentiation. The production of RANKL/OPG by osteoblasts is influenced by hormones, growth factors and cytokines, which each have a different effect on the production of RANKL and OPG. Ultimately, the balance between RANKL and OPG determines the degree of proliferation and activity of the osteoclasts. In rheumatoid arthritis (RA), bone erosions are the result of osteoclastic bone resorption at the sites of synovitis, where RANKL expression is also found. Furthermore, magnetic resonance imaging (MRI) bone edema in RA indicates the presence of active inflammation within bone and the presence of osteitis, which is also associated with the expression of RANKL. Bone loss has been documented in the cortical and trabecular bone in the joints of the hand of RA patients. Both synovitis and periarticular bone involvement (osteitis and bone loss) are essential components of RA: they occur early in the disease and both are predictive for the occurrence and progression of bone damage. RANKL knockout mice and mice treated with OPG did not develop focal bone loss, in spite of persistent joint inflammation. Inhibition of osteoclasts by denosumab, a humanized antibody that selectively binds RANKL, has revealed in patients with RA that the occurrence of erosions and periarticular bone loss can be halted, however without affecting synovial inflammation. This disconnect between inflammation and bone destruction opens new ways to separately focus treatment on inflammation and osteoclastogenesis for preventing and/or minimizing the connection between joints and subchondral bone and bone marrow.
Introduction
It has long been known that in healthy young adults bone formation and resorption are tightly connected in location, direction, timing and quantity [Evans, 2007; Parfitt, 1982]. Bone remodeling replaces old bone by new bone in order to preserve optimal bone strength and to support calcium homeostasis, but the underlying molecular mechanisms of this connection remained unknown until the end of the last century. The discovery of the receptor activator of the nuclear factor κB ligand (RANKL)/RANK/osteoprotegerin (OPG) pathway enabled us to better understand this equilibrated connection between bone formation and resorption and to understand diseases with disconnection between bone resorption and formation, such as glucocorticoid osteoporosis, Paget’s disease and bone destruction in rheumatoid arthritis (RA) and metastatic bone disease [Lorenzo et al. 2008, 2011; Takayanagi, 2009]. RANK and RANKL are members of the tumor necrosis factor (TNF) superfamily and OPG is a member of the TNF receptor family [Lorenzo et al. 2008, 2011; Takayanagi, 2009]. OPG was initially identified as a soluble factor that was capable of inhibiting osteoclastogenesis in vitro [Simonet et al. 1997; Tsuda et al. 1997]. Mice that were made transgenic for OPG developed osteopetrosis [Simonet et al. 1997] while OPG KO mice had had a phenotype of osteoporosis and developed spontaneous fractures [Bucay et al. 1998]. OPG was found to be a decoy receptor that binds RANKL [Simonet et al. 1997]. RANKL was originally identified as a product of dendritic cells and of activated T cells [Anderson et al. 1997; Kong et al. 1999] and was subsequently identified as soluble osteoclast activating factor produced by osteoblasts [Fuller et al. 1998; Lacey et al. 1998]. RANKL deficient mice have osteopetrosis and no osteoclasts [Fuller et al. 1998]. RANKL binds to the RANK receptor on the surface of osteoclast precursors and mature osteoclasts, resulting in differentiation and activation of osteoclasts [Boyle et al. 2003]. OPG binds to RANKL and in that way inhibits osteoclastic bone resorption [Simonet et al. 1997; Tsuda et al. 1997]. The findings of the connection between the immune system and bone have contributed to the birth of osteoimmunology [Lorenzo et al. 2008, 2011; Takayanagi, 2009] and, in the field of rheumatic diseases, of osteorheumatology (this congress).
In the complex system of bone remodeling, which includes the sequential phases of activation, resorption, reversal, formation and termination, the RANKL/OPG pathway is the coupling factor between bone resorption and formation [Raggatt and Partridge, 2010]. Ultimately, the balance between RANKL and OPG determines the degree of proliferation and activity of the osteoclasts [Lorenzo et al. 2008].
RANKL and joint damage
Bone erosions in RA were first described macroscopically in the finger joints in 1878 as ‘caries of the joint ends’ [Weichselbaum, 1878]. It was more than 100 years later that multinucleated cells were identified that were attached to bone and cartilage in RA at sites of pannus in the subchondral bone region [Bromley and Woolley, 1984]. These cells were initially described as ‘chondroclasts’ and stained positive for acid phosphatase [Bromley and Woolley, 1984]. In 1998 these cells were found to have the osteoclast phenotype, as demonstrated by positive staining with specific markers of osteoclasts such as cathepsin K, tartrate resistant alkaline phosphatase (TRAP), the calcitonin receptor and β-integrins [Gravallese et al. 1998]. These osteoclasts were specifically found at the pannus-bone connection at the sites of bone erosions. Subsequently, RANKL expression was documented at these sites of active bone erosions [Pettit et al. 2006]. These findings demonstrate that bone erosions in RA are the result of osteoclastic bone resorption at the sites of synovitis.
On histological examination, it became clear that osteoclasts can penetrate deeply into the subchondral bone and can also invade the calcified compartment of cartilage [Schett and Firestein, 2010]. The importance of involvement of subchondral bone in RA became even more evident with the introduction of magnetic resonance imaging (MRI). Bone marrow lesions (BMLs) in RA, described as MRI ‘bone edema’, were demonstrated to reflect osteitis, as they contain inflammatory cells, replacing adipose bone marrow and bone [Dalbeth et al. 2009; Geusens and Lems, 2011; Jimenez-Boj et al. 2007; McQueen et al. 2007; Schett, 2009]. In postoperative joint specimens of patients with RA, osteoclasts and RANKL expression were also found in these MRI lesions, but not at locations without MRI bone edema [Dalbeth et al. 2009]. These findings indicate that MRI edema in RA reflects the presence of active osteitis with active inflammation within bone.
The involvement of peri-inflammatory and juxta-articular osteitis in bone has been quantified using measurements in the hands by X-ray, dual X-ray absorptiometry (DXA) and quantitative ultrasound (QUS) [Fouque-Aubert et al. 2010; Geusens and Lems, 2011] (Figure 1). Cortical and trabecular bone loss in the hands was found in early RA [Haugeberg et al. 2006] and was associated with the severity of damage in the joints [Haugeberg et al. 2006; Hoff et al. 2009]. More importantly, bone loss in the hands and the presence of MRI osteitis predicted bone damage [Boyesen et al. 2009; Haavardsholm et al. 2008; McQueen et al. 2003; McQueen and Dalbeth, 2009; Mundwiler et al. 2009]. It so became clear that both synovitis and periarticular bone involvement (osteitis and bone loss) are essential components of RA: they occur early in the disease and both are predictive for the occurrence and progression of bone damage.

Methods of measurements of bone in the hands.
Cells that control RANKL/OPG production
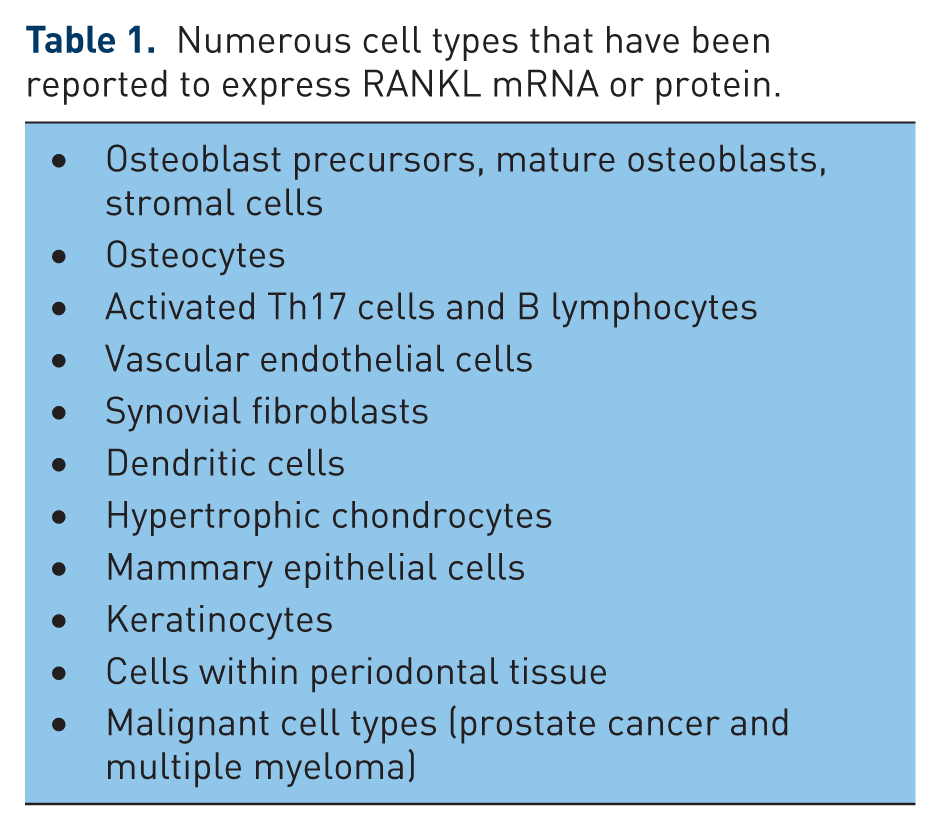
Osteoblasts and stromal cells produce RANKL and OPG under the direct or indirect influence of hormones (such as PTH, calcitriol, estrogens, prolactin, glucocorticoids), growth factors (BMP, IGF1, TGFb, oncostatin M, PDGF) and cytokines (TNFa, IL-1, IL-6, IL-17, PGE) [Lorenzo et al. 2008]. However, osteoblast/ stromal cells are far from the only cells that can produce and regulate RANKL/OPG production [Goldring and Schett, 2011] (Table 1). In RA, RANKL is also produced by activated Th17 cells [Okamoto and Takayanagi, 2011], synovial fibroblasts, macrophages, dendritic cells and activated B cells [Yeo et al. 2011]. Furthermore, it has recently been shown that, at least in normal physiological bone remodeling, osteocytes are a major, and probably the greatest, source of RANKL [Nakashima et al. 2011]. RANKL and OPG are also found in vascular endothelium [Osako et al. 2010] and atherosclerotic lesions [Dhore et al. 2001], in hypertrophic chondrocytes, keratinocytes and in periodontal, mammary epithelial and malignant cells [O’Brien, 2010].
Numerous cell types that have been reported to express RANKL mRNA or protein.
The macrophage colony-stimulating factor (M-CSF) and RANKL are critical factors in the differentiation and activation of osteoclasts [Boyle et al. 2003; Fuller et al. 1998]. Although osteoclast-like cells can form in vitro in the absence of RANKL when exposed to a cocktail of growth factors and cytokines, in most instances cytokines and growth factors other than RANKL, which are produced at sites of inflammation or physiologically during bone remodeling, such as IL-1, IL-6, TNFa and yet unidentified ligands for the osteoclast-associated receptor (OSCAR), act as cofactors that enhance or modulate the response of osteoclasts and their precursors to RANKL–RANK stimulation [Braun and Zwerina, 2011; Lorenzo et al. 2008; Nemeth et al. 2011].
RANKL/OPG in RA
In animal models of RA (such as collagen- or adjuvant-induced arthritis), RANKL was expressed already within 4 days of the start of arthritis [Stolina et al. 2005]. RANKL knockout (KO) mice and mice treated with OPG did not develop focal bone loss, in spite of persistent joint inflammation, indicating the essential role of RANKL/OPG in bone damage by osteoclasts in animal models of arthritis [Pettit et al. 2001; Stolina et al. 2005].
In patients with early untreated RA, it has been shown that the baseline RANKL/OPG ratio in serum predicted bone damage after 5 and 11 years of follow up, independent of other predictors, such as erythrocyte sedimentation rate (ESR), C-terminal crosslinked telopeptide type II collagen (CTX-II) and baseline joint damage [Geusens et al. 2006; van Tuyl et al. 2010]. The highest degree of long-term radiographic progression of joint damage was found in patients with a combination of high ESR and high RANKL/OPG ratio at baseline. These results indicate that the combination of the degree of inflammation and bone destruction is a, possibly constitutional, determinant of progression already early in the disease. A shortcoming of this study was that measurements of antibodies against cyclic citrullinated peptides (ACCPs) were not available at the time of the study, so that the additional role of auto-antibody formation could not be analyzed.
Denosumab, a fully humanized antibody that specifically binds RANKL, has been shown in the FREEDOM study to decrease the risk of vertebral, nonvertebral and hip fractures in postmenopausal women with osteoporosis [Cummings et al. 2009]. Denosumab was also studied in patients with RA given subcutaneously (SC) in doses of 60 and 180 mg at baseline and after 6 months [Cohen et al. 2008]. Denosumab inhibited the occurrence of MRI erosions at 6 months with the 180 mg does (the primary endpoint) and the progression of erosions on radiographs after 6 months (with the 180 mg dose) and after 12 months (with both doses). As expected, no effect was found on inflammation, nor on joint space narrowing. Interestingly, in this study bone loss was also prevented in the hands, measured by dual-energy X-ray absorptiometry (DXA) [Deodhar et al. 2010] and by digital X-ray radiogrammetry (DXR) using computer-assisted measurement of cortical thickness and shaft width at midshaft levels of the second through fourth metacarpal bones of both hands [Sharp et al. 2010] and bone mineral density (BMD) increased in the spine and hip, in all treated patients, whether or not they were concomitantly treated with bisphosphonates or glucocorticoids [Dore et al. 2010].
Bone erosions: opening the battle field between synovium and bone marrow
Prevention of joint damage on X-rays and MRI, together with clinical evaluation of synovitis, has become the gold standard for analyzing the effect of medication in RA [Bird et al. 2005; Geusens and Miller, 2008; Scott et al. 2010; Smolen et al. 2010]. The main reason for including bone damage (erosions) is that prevention of bone destruction should prevent future handicap [Skapenko et al. 2009]. However, the early combination of synovitis and osteitis raised new questions about the role of erosions already early in the disease, as suggested by Schett and others [Geusens and Lems, 2011; Jimenez-Boj et al. 2007; Schett and Firestein, 2010] (Figure 2).

High-resolution peripheral quantitative computer tomography of finger joints showing multiple cortical perforations near the joint ends (images from the Maastricht Xtreme CT project).
Anatomical barriers are of utmost importance in health and disease, such as the blood–brain barrier and the basement membrane in the kidney [Jarad and Miner, 2009; Redzic, 2011]. These barriers are dynamic and allow a controlled interaction and equilibrium between two separated organ structures. Destruction of these barriers plays a major role in diseases, such as multiple sclerosis [Larochelle et al. 2011] and kidney diseases such as Alport’s diseases [Ooi et al. 2008] and Goodpasture’s syndrome [Heidet and Gubler, 2009]. In analogy, intact bone surfaces are a barrier between synovium/enthesis and bone marrow, which allow only limited interaction by its vasculature. A bone erosion is a destruction of this barrier, which opens a direct anatomical connection between these previously anatomically separated sites.
It has been shown that bone erosions in the hands are rare in the normal population (in <1% on X-rays and <2% on MRI) [Ejbjerg et al. 2004]. In RA without bone erosions at baseline it has been found that bone erosions preferentially occur at the bone site depraved from periost in the joint, the so-called ‘bare area’ [McGonagle et al. 2009; Theumann et al. 2002]. It is the localization where osteoclasts derived from the synovium can start to attack the nude bone in RA, as osteoclasts can only degrade mineralized tissue and not nonmineralized tissue [Parfitt, 1976]. Surprisingly, nearly 40% of clinically apparent healthy subjects have small bone erosions when studied with high-resolution quantitative computed tomography (HRqCT) [Stach et al. 2010]. Studies of the anatomy of the finger joints has shown that erosions can occur at sites of pressure by ligaments on bone without any sign of RA [McGonagle, 2010; McGonagle et al. 2009]. Furthermore, in patients with RA MRI osteitis was more pronounced at sites of pressure, e.g. the ventral site of MTP joints [Jimenez-Boj et al. 2007].
These observations have potential consequences for the pathophysiology of RA (Figure 3). Indeed, quiescent osteoclast precursors derived from the stem cells in the bone marrow can enter the synovial cavity by the circulation, the so-called ‘osteoclast odyssey’ [Muto et al. 2011; Warde, 2011], and even more so in hypervascularized synovitis, which is so typical for RA [Koch, 2003]. Similarly, if there is no erosion present, a first bone erosion occurs most probably from the inflammatory attack of synovitis on bone with recruitment of circulating osteoclast precursors. However, if an erosion is already present before the start of RA, or has developed during the course of RA, it can be hypothesized that the erosions allow a direct anatomical contact between the synovial cavity and the bone marrow [Ritchlin et al. 2003]. This would allow hematopoietic stem cells (HSCs), including T and B cells and pre-osteoclasts, to be directly available and to locally invade the synovial cavity from inside bone [Schett et al. 2005]. The suppression of osteoblasts in RA could also be involved, as stromal/osteoblast cells control the HSC niches [Calvi et al. 2003; Raisz, 1981; Yin and Li, 2006]. Intrinsic bone marrow abnormalities have also been described in RA [Fujii et al. 1999]. In this way, both the synovitis and osteitis could reinforce each other’s inflammation in a vicious circle [McInnes and Schett, 2011]. If confirmed, this could explain why erosions and osteitis and the presence and level of auto-antibodies such as ACCP at baseline predict long-term progression of bone damage.

Interactions between inflammation and bone in rheumatoid arthritis (RA).
These findings indicate that RANKL and subsequent bone damage is driven by cellular and molecular mechanisms in both the synovium and bone marrow, and that osteitis is probably as important to predict joint damage as synovitis, already early in the disease process of RA. Having the possibilities to quantify these periarticular bone changes opens new windows for further research in the etiology and progression of joint damage, not only in RA, but also in other rheumatic diseases, such as ankylosing spondylitis and osteoarthritis, and in enthesitis.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.