
Abstract
Introduction
Neurogenic Thoracic Outlet Syndrome (NTOS) is a complex condition that can be encountered in musculoskeletal and hand therapy services. Rehabilitation is recognised as the primary treatment for NTOS however, detail on rehabilitation components are poorly described. This scoping review aimed to identify and describe the physical assessment and rehabilitation components alongside clinical reasoning strategies that may aid therapists in the conservative management of adults with NTOS.
Methods
Four databases (MEDLINE, EMBASE, CINAHL and Cochrane) were searched, utilising the PRISMA-ScR guidelines. The Template for Intervention Description and Replication (TIDieR) checklist was used to organise data regarding rehabilitation interventions for NTOS.
Results
Twenty-Nine out of 1381 studies identified, met the eligibility criteria. NTOS Provocation tests (16/18 89%) were the most frequently described assessment components, followed by palpation of pertinent structures (11/18 61%) and assessment of posture (10/18 56%). ‘Decompressing the thoracic outlet’ was the main aim encountered for rehabilitation programmes. Exercise (17/19 90%) was the most frequent rehabilitation intervention identified, with stretching (n = 15), strengthening (n = 14) and neural mobility (n = 7) exercises being most prevalent. The Scalenes and Pectoralis muscles (n = 10) were the main targets for stretching whilst the Scapula (n = 9), Trapezius and Serratus Anterior muscles (n = 5) were the main targets for strengthening exercises. Other interventions identified included, posture improvement (n = 13), manual therapy (n = 10), adjuncts (n = 8) and activity modification (n = 7).
Discussion
The reporting of rehabilitation techniques for NTOS is generally poor, particularly regarding treatment intensity. There is an essential need for a standardised and reproducible rehabilitation intervention for NTOS to be developed.
Introduction
Thoracic Outlet Syndrome (TOS) is a complex clinical condition as highlighted in a Cochrane review in 2014. 1 TOS is believed to be caused by congenital, acquired or traumatic factors, which subsequently create a compromised space for neurological (brachial plexus) and/or vascular (subclavian vein/artery) structures to pass through. Presenting symptoms vary and diagnosis is challenging due to the existence of three main subgroups (Vascular, Arterial and Neurogenic) depending on the main structures that have been compromised. Authors describe three pertinent anatomical spaces of compression in TOS: the scalene triangle, costoclavicular and subcoracoid space.2–4
Neurogenic Thoracic Outlet Syndrome (NTOS) accounts for up to 95% of TOS cases and is regarded as the more controversial and complex TOS subgroup due to the complexity of diagnosis and the constellation of signs and symptoms.1,3,5 NTOS is estimated to have a prevalence of 10 cases per 100,000 with an incidence of 2–3 cases per 100,000 per year. 6
NTOS refers to an assumed dynamic positional compression of the brachial plexus, 7 which can present with an array of symptoms including neck, shoulder, arm and hand pain, paraesthesia and weakness. These symptoms are often exacerbated by repetitive overhead motions and can lead to significant functional disabilities, including compromised hand function.3,5,8,9 Risk factors include anatomical abnormalities, female gender, previous trauma and repetitive use of upper limbs-particularly in activities such as sports that involve overhead motions. NTOS often affects individuals in the working age population. 7 People with NTOS are known to have poor Quality of Life and high disability scores, with similar baseline physical disability scores to that of chronic heart failure and rotator cuff tear populations.7,10–13
Specialist rehabilitation is deemed the ‘mainstay’ of conservative management for NTOS. 9 NTOS is often encountered and treated by therapists working in musculoskeletal (MSK) and hand therapy contexts, due to common differential diagnoses such as carpal and cubital tunnel syndrome and cervical radiculopathy 14 and is viewed as a clinically complex condition to manage, requiring treatment by experienced therapists. 15
A Cochrane review on the treatment of NTOS, updated in 2014, concluded that the field was dominated by low-quality evidence. 1 Since then, progress has been made in NTOS research, including the publication of an agreed clinical diagnostic criterion (CDC) 16 which provided a standardised framework for diagnosing NTOS. Validation of these criteria against Patient Reported Outcome Measures (PROMs) was completed in 2017. 10 Furthermore, reporting standards have been published to encourage increased homogeneity of care through consistent reporting. 17 However, progress in advancing the evidence base for therapy management has been slower.
Conservative care
Currently, literature suggests the effectiveness of therapy for NTOS is suboptimal, with 60–70% of people choosing surgery due to ‘failing’ conservative care.7,10,11
Conservative treatments typically include rehabilitation, manual therapy, hot and cold therapy, electrophysical modalities, and the utilisation of braces and taping. 18 A systematic review in 2011 18 examining the effectiveness of physiotherapy treatments in NTOS, concluded they could not make a judgement about the effect of exercise on NTOS, due to the low-quality evidence.
Several narrative review articles.18–20 including a scoping review from 2022 21 summarising the evidence up to 2021, have provided an overview of proposed theories and rationales for exercises included in rehabilitation programmes. However, none have described or compared programmes in detail or examined the PROMs used in NTOS studies. Furthermore, several new publications since 2022 have partially explored rehabilitation for NTOS,22–27 including the first randomised clinical trial which compared continued physiotherapy with surgery for persistent NTOS, which was refractory to change with initial physiotherapy. 8
Therefore, an up-to-date synthesis of the literature is warranted, focussed on this current gap in knowledge around the content of rehabilitation programmes and the outcomes used. A scoping review is the most appropriate method to map the current therapy management of NTOS, while still maintaining a rigorous and transparent search strategy 28 to underpin a) future consensus-based recommendations for NTOS, and b) to test the effectiveness of treatment based on such recommendations (e.g. our planned future IMPETUS (optIMal Physiotherapy for nEurogenic Thoracic oUtlet Syndrome) feasibility trial). This scoping review will lay the foundations of the IMPETUS study’s goal of developing an optimal therapy intervention for NTOS, and its findings will inform consensus-building exercises and intervention testing.
Research aims and question
The primary aim of this scoping review was to identify and describe the physical assessment and rehabilitation components alongside any clinical reasoning strategies that may aid therapists in the conservative management of adults with NTOS. The secondary aim was to synthesise reported approaches to diagnosing NTOS and the use of PROMs.
Our over-arching research question was: What are the key physical assessment and rehabilitation components used to manage adults with NTOS as part of conservative care?
Methods
This review was conducted in accordance with the Joanna Briggs Institute methodology for scoping reviews 29 and reported according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) extension for Scoping Reviews. 30
Data sources and search
Search terms for MEDLINE.
Inclusion/exclusion criteria and study selection
The following study designs, published in English, were eligible for this review: literature reviews, systematic reviews, Cochrane reviews, primary empirical studies, treatment guidelines and clinical commentaries. Eligible participants were adults (>16 years old), with a clinical diagnosis of NTOS. This review considered studies in any context where adults (>16) could receive rehabilitation, if it was part of conservative care. This included hospital inpatient units, outpatient clinics and community settings.
Eligibility criteria for this systematic scoping review.
Using a specialist systematic review tool, Rayyan, 33 two reviewers (JOS & CR) independently screened the titles and abstracts of all identified studies against pre-defined eligibility criteria. The full text articles for the remaining studies were retrieved and reviewed for eligibility. Any disagreement on eligibility was resolved by discussion and a third reviewer for consensus (CM). AI technologies were not used in any part of this review process.
Data extraction and categorisation
Two reviewers (JOS & CR) extracted data from the full text articles using a custom Excel spreadsheet developed by the research team which included study design, location, method of recruitment, inclusion and exclusion criteria, participant numbers and characteristics, physical assessment and rehabilitation description, PROMs, results and clinical reasoning strategies. The spreadsheet was piloted by the research team to ensure it would extract relevant information prior to full data extraction (Supplemental information 1). A dual extraction method was undertaken to reduce errors in data collection. 34
The Template for Intervention Description and Replication (TIDieR) checklist 35 was used by both reviewers (JOS & CR) to extract consistent and detailed information on each of the studies intervention components and mode of delivery. The TIDieR checklist is a validated tool to describe and report interventions in studies 36 and has been used to extract intervention data from multiple study designs. 37
As per the PRISMA guidelines for scoping reviews, quality appraisal of included articles for this study was not completed. 30
Data synthesis
The extracted data was collated, summarised and reported by the lead author (JOS) and checked by the second reviewer (CR) and discussed with the research team. The TIDieR checklist was used to organise the results of the rehabilitation interventions. As the physical assessments and rehabilitation interventions were comprised of multiple components, these were identified, defined and tabulated by the research team. Clinical Reasoning strategies were assessed on merit subjectively by the lead author and discussed with the second reviewer, based on their own clinical experience of managing patients with NTOS.
Results
Study selection
The results of our search strategy are presented in the PRISMA flow diagram in Figure 1. After omitting duplicates, 1381 records remained for screening. Following title and abstract screening based on the study’s eligibility criteria, 76 studies (n = 2 identified from citation tracking) remained for full text retrieval and review. Of these, a further 47 studies were excluded, leaving a final dataset of 29 studies to be included in this review. The main reasons for full text exclusion were as follows; insufficient detail on rehabilitation (n = 19), study not specific to NTOS (n = 11), non-full text/abstract only (n = 10), non-English language (n = 4) and surgical studies (n = 3). PRISMA flow diagram for study selection.
Characteristics of included studies
Most of the included studies were literature/narrative reviews or expert opinion pieces (n = 13), followed by: prospective studies (n = 4), randomised controlled trials (RCT), retrospective analysis and consensus studies (all n = 3), case reports (n = 2) and one cross sectional study.
Characteristics of included studies.
CDC: clinical diagnostic criteria; CORE-TOS: consortium of research and education on thoracic outlet syndrome; EANS: the European association of neurosurgical societies; ER: external rotation; FHP: forward head posture; GERD: glenohumeral external rotation deficit; INTOS: international neurogenic thoracic outlet syndrome hand surgery workgroup; LS: levator scapulae; LT: Lower fibres of trapezius; MDT: multidisciplinary team; MT: middle fibres of trapezius; N/A: not applicable; NM: neuromuscular; NTOS: neurogenic thoracic outlet syndrome; PM: pectoralis minor; PMS: pectoralis minor syndrome; PROMs: patient reported outcome measures; PT: physical/physiotherapy; RCT: randomised control trial; Rx: treatment; SA: serratus anterior; SCM: sternocleidomastoid; SS: statistically significant; SSN: suprascapular nerve; SVS: society of vascular surgeons; TENS: transcutaneous electric nerve stimulation; TO: thoracic outlet; TOP: tender on palpation; TRMdiff: total rotational movement difference; USS: ultrasound.
Review findings
Primary aim-physical assessment and rehabilitation components and clinical reasoning strategies
Physical assessment
The most prevalent physical assessment components encountered were provocation tests- Roos/EAST (16/18 89%), ULTT (14/18 77%) and Adson’s (10/18 56%). Additionally, 11 (61%) studies mentioned, Palpation of pertinent structures (pectoralis muscles/scalene/supraclavicular space/subcoracoid space), whilst 10 studies (56%) mentioned; Posture assessment and Scapulothoracic assessment.
Less frequently encountered physical assessment components such as, first rib mobility (n = 3)9,20,43 and breathing assessment (n = 1) were also noted. 44 Three studies,8,10,38 suggest that their physical assessment of NTOS is based on patients fulfilling existing CDC’s. 17
Due to the overlap in the description of physical assessment components, further coding and synthesis was conducted to allow a visual representation of a comprehensive physical assessment of NTOS, based on the findings of the included studies (Figure 2). Further information on assessment is available in Supplemental Information 2. A body chart to visually represent a comprehensive physical assessment of NTOS, based on the content of included studies (n = number of studies each component included). Further information in supplementary information 2. ACJ: acromial-clavicular joint; SCJ: sternoclavicular joint; mobs: mobilisations; EAST: elevated arm stress test; ULL: upper limb tension test; Pec: pectoralis.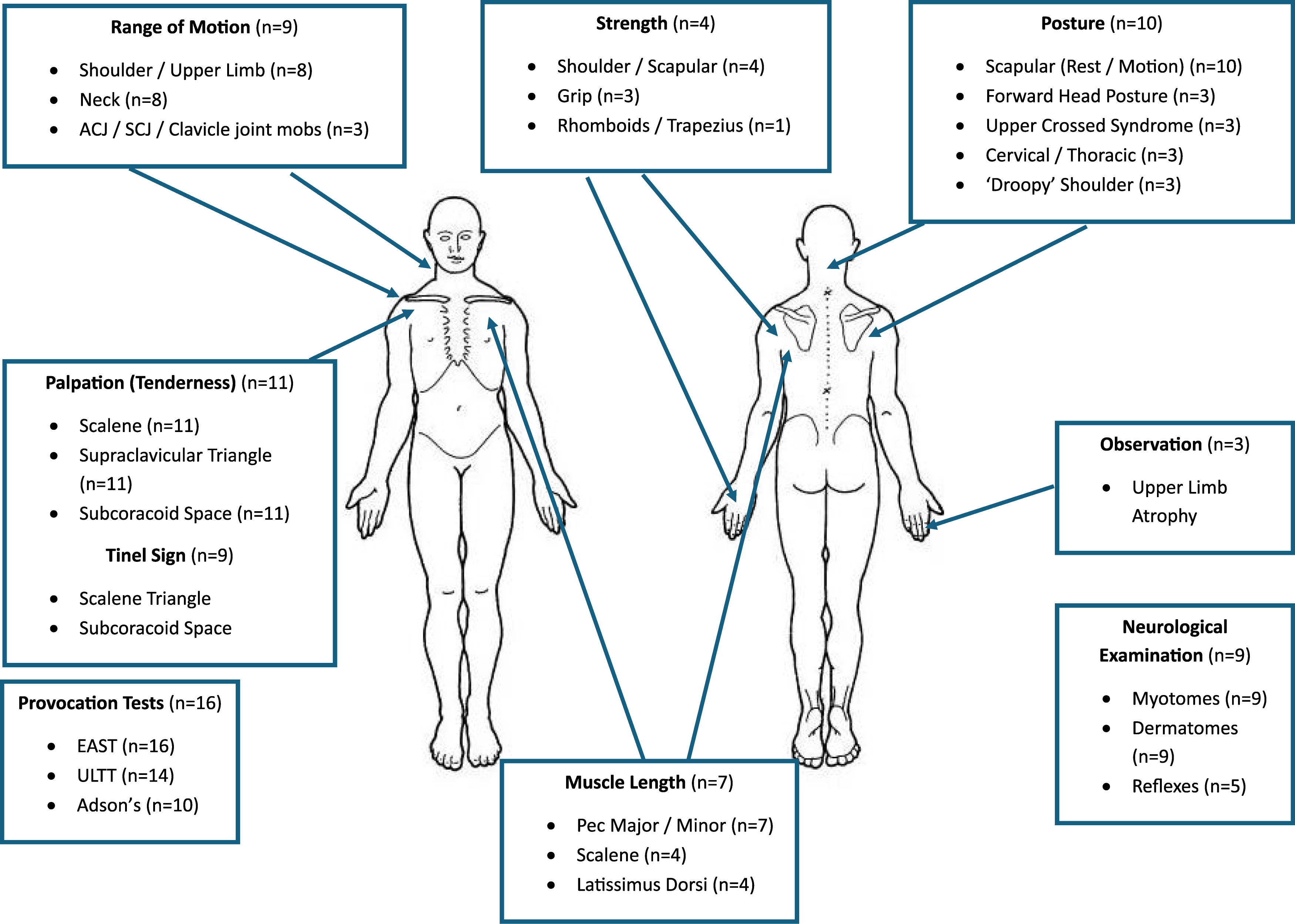
Rehabilitation
Summary of rehabilitation interventions of included studies, using a modified version of the TIDieR checklist.
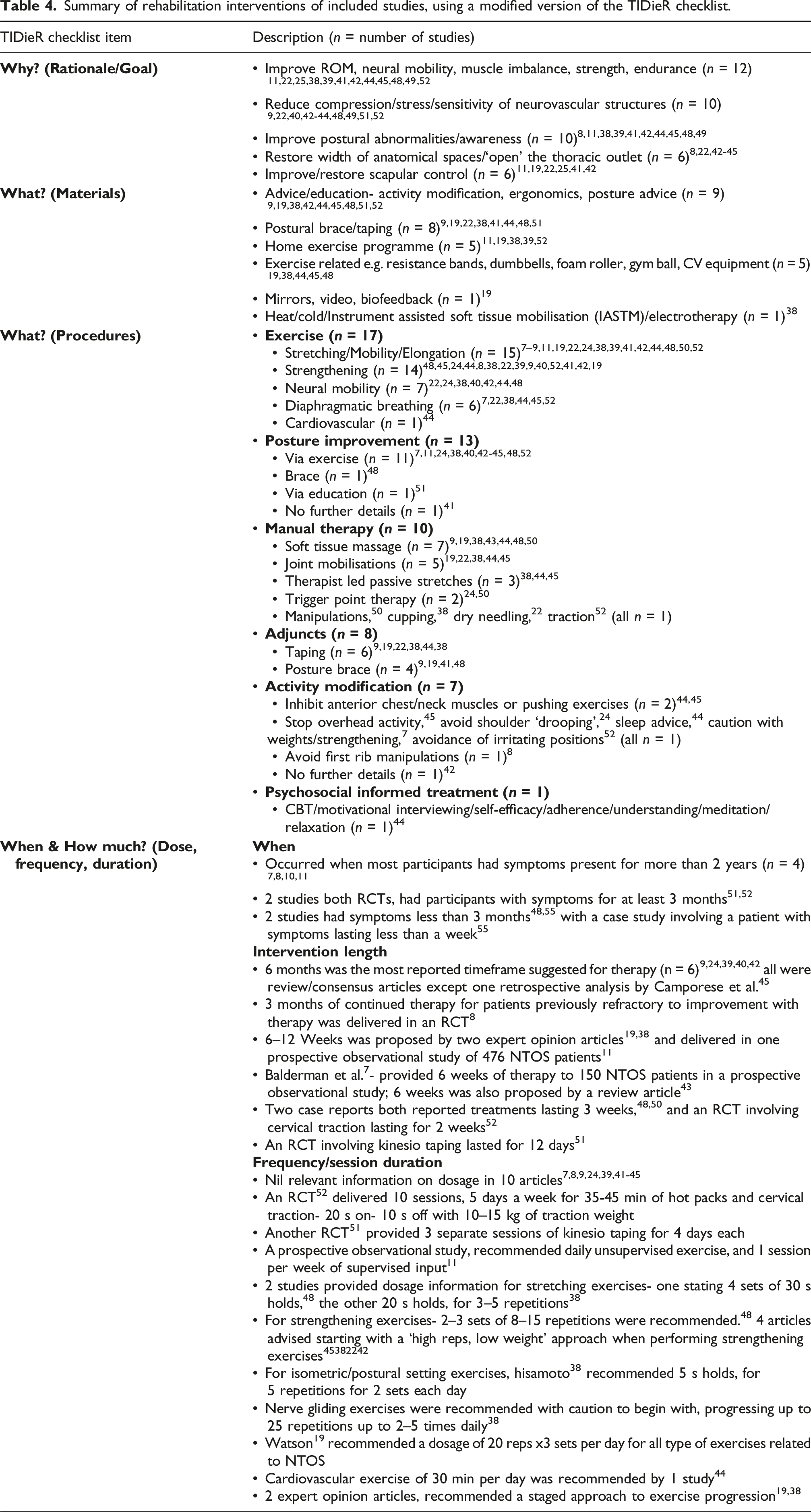
Most of the included studies describing rehabilitation interventions (17/19) included exercise as a core element. Stretching (n = 15), strengthening (n = 14), neural mobility (n = 7) and diaphragmatic breathing (n = 6) were the most prevalent exercise components encountered. Additional rehabilitation interventions were: ‘Posture Improvement’ (n = 13), ‘Manual Therapy’ (n = 10), ‘Adjuncts’ (n = 8) such as taping or braces, and advice on ‘Activity Modification’ (n = 7). Only one study
44
proposed using a ‘Psychosocial informed treatment’. Figure 3 provides more details. A nested pie chart to represent the main rehabilitation elements and their components found in the included studies, and their frequency (n = ). The size of the inner segments represented the frequency of the element being encountered within the studies.
Most interventions were provided by a physical or physiotherapist (n = 14), via face-to-face means (n = 11) in a clinic setting (n = 11). Patients receiving treatment often had chronic symptoms of at least 2 years (n = 4). Information on intervention frequency, duration and dosage was typically sparsely described within the included studies, with nil relevant information on dosage in 10 articles. When describing strengthening exercises for NTOS, a ‘high repetition, low weight’ approach was suggested in four studies.22,38,42,45
The Scalene and Pectoral muscles (n = 10) were most frequently mentioned muscles when describing stretching exercises. Scapular Stabilisation (n = 9) was the most common feature of strengthening exercises, followed by mid-lower Trapezius and Serratus Anterior (n = 5). Minimal detail for neural mobility exercises other than ‘upper limb neural glides’ (n = 6) was provided, and no further details concerning diaphragmatic breathing exercises were provided by any of the six studies. Further information on specific exercises that were mentioned in the included studies can be found in Supplemental Information 2.
Clinical reasoning
Prognosis
Balderman et al., in their two studies7,10 of 150 NTOS patients, displayed some significant differences between the groups of patients that improved with rehabilitation alone (31%), and those that did not (69%). The group that improved with rehabilitation were on average less tender to palpation (1.7 ± 0.1 vs 2.0 ± 0.1 p < 0.05), had less positive CDC signs (9 ± 0.3 vs 10.1 ± 0.1 p < 0.05), less severe Cervical Brachial Symptom Questionnaire (CBSQ) (68.0 ± 4.1 vs 78.0 ± 2.7 (p < 0.05) and Short Form 12 (SF-12) physical component (35.6 ± 1.5 vs 32.0 ± 0.8 p < 0.05) scores and could tolerate a longer EAST test before failure (103 s ± 10.2 vs 97 s ± 6.3 p > 0.05). However, there was no between group differences noted in age, gender, symptom duration, previous injury, QuickDASH or other PROMS.
Two review articles9,20 proposed that patient compliance to rehabilitation, resulting in lasting lifestyle/postural modifications and a sedentary job were positive prognostic factors for response to rehabilitation in NTOS whilst obesity, depression, previous upper limb trauma and chronicity of symptoms were negative factors.
NTOS management decisions
A two-part consensus study by members of the European Association of Neurosurgical Societies (EANS) proposed a subclassification of NTOS to guide clinical management decisions.46,47
The group proposed that patients with atrophy/objective weakness (NTOS 1) should be assessed urgently for potential surgery. Conservative management including rehabilitation should be the first treatment for NTOS 2 & 3a patients and failing that, may progress to surgery. Whereas NOTS 3b & 3c patients should only progress from conservative care to surgery in rare circumstances and these patients would need to be counselled on the risks of potentially unsuccessful surgery. A further consensus study, from the International Neurogenic Thoracic Outlet Syndrome (INTOS) Hand Surgery workgroup, 24 agreed with a 3–6-months conservative care first approach for all NTOS patients, except those with atrophy or weakness, but did not fully support the EANS subclassification. Further information is available in Supplemental Information 2
Secondary aim-diagnosis and measurement
Diagnosis
As diagnosing NTOS can be complex, a secondary aim of this study was to examine how the included studies chose to clarify the diagnosis of NTOS.
Of the 16/29 (55%) of studies in this review to specifically discuss diagnosis of NTOS, 56% (9/16) of them quoted either the Society of Vascular Surgeons (SVS) CDC (n = 6) 17 or the Consortium of Research and Education on Thoracic Outlet Syndrome (CORE-TOS) CDC (n = 6). 16 Two studies7,24 referenced both. Other studies (n = 5) were less specific, but their description encompassed elements of both previously mentioned CDCs, for example the requirement of positive provocation tests (Elevated Arm Stress Test (EAST), Upper Limb Tension Test (ULTT) and Adson’s)46,48,49 and the absence of other more likely diagnoses.40,50
Two studies, both RCT’s,51,52 offered their own criteria for the diagnosing NTOS. Ortac et al.’s (2020) criteria, while less comprehensive, would still align with the CDC proposed by Thompson. 16 However, Taskaynatan et al.’s 52 would not sufficiently justify the diagnosis of NTOS according to more widely accepted CDC’s, potentially questioning the validity of their study findings.
Additionally, Balderman et al. 10 described the most prevalent elements of the CORE-TOS CDC found within their study (n = 150 patients). Elements encountered in more than 90% of patients included: pain (99%), symptoms exacerbated by elevation (97%), tenderness to palpation of scalene triangle/subcoracoid space (96%), numbness, paraesthesia or weakness in arm and/or hand (94%) and positive EAST test (94%). The least prevalent positive elements were a history of previous clavicle/first rib fracture or presence of a cervical rib (8%), previous cervical or peripheral nerve surgery (20%), previous treatment for ipsilateral TOS (21%) and weak handgrip/hand intrinsic atrophy (23%).
Two consensus studies24,46 both emphasised the importance of patient history and physical examination in the diagnosis of NTOS, along with arm symptoms referring along the C8/T1 distribution, which is also proposed by multiple other studies.25,38,42,48,52
Measurement
Twelve out of 18 (67%) studies used/proposed to use the QuickDASH. The CBSQ was less frequently observed (8/18 44%), with the TOS Disability score featuring in only 2 of the 18 studies.8,11 The Short Form 12 (SF-12) was used 6 times, whereas the Pain Catastrophising Scale and the Zung Self-Rating Depression score were only encountered twice.7,10 Four studies assessed functional changes such as isokinetic strength of shoulder rotators, 53 grip strength, 54 changes in range of motion or tenderness to palpation 50 and time to return to play. 55 Further information regarding measurement is available in Supplemental Information 2.
Discussion
The primary aim of this scoping review was to identify and describe the components of physical assessments, rehabilitation and clinical reasoning strategies that may assist therapists in managing adults with NTOS. The secondary aim was to examine approaches to diagnosing NTOS and the use of PROMs. This review examined literature published since 2000, with most studies (n = 22) published since 2020.
This review highlights the wide range of assessment and rehabilitation components associated with the therapy management of NTOS. A continued emphasis on the biomedical model is evident in the assessment and rehabilitation of NTOS, with many studies stating their aim of treatment is to reduce ‘stress/compression’ of neurovascular structures and ‘open’ the thoracic outlet. This echoes the findings of the 2022 scoping review on exercise and NTOS. 21
Assessment
The most frequently encountered physical assessment components appear to focus on confirming a diagnosis of NTOS, rather than identifying targets for therapy intervention. Commonly used methods include provocation tests (EAST n = 16) and palpation of pertinent structures (n = 11). Postural assessment also features prominently (n = 10), particularly in relation to scapular positioning. This emphasis is likely tied to the perceived impact of scapular alignment on thoracic outlet space; however, this association remains largely anecdotal. 19 Notably, only one article proposes an objective method for measuring scapular position, 19 and none of the studies provide follow-up data assessing postural changes as an outcome of treatment. A similar pattern is seen in the assessment of muscle length in pectoral (n = 7) and scalene muscles (n = 4). While these assessments are often based on presumed symptom contributors, they are rarely conducted in an objective or reproducible manner, nor are they re-evaluated following interventions. This raises two important questions: firstly, ‘Do we need to assess these aspects if we are not going to re-assess them?' and secondly ‘How do we know the perceived effect that rehabilitation is having on NTOS patients?'.
Logic modelling has been described as a practical way of representing theoretical data on how a treatment programme may be effective. 56 Proposing a logic model to illustrate the potential effects of rehabilitation on NTOS may help address current gaps in understanding and further our knowledge of both the underlying causes of NTOS symptoms and the impact of specific interventions. Several studies included in this review provide potential starting points for such a model.
Two prospective observational studies assessed and identified that NTOS patients had weaker grip strength on the symptomatic side 54 and significantly decreased shoulder rotation strength compared to controls. 53 Additionally, Garrison, Hannon and Conway 49 identified that NTOS patients had significantly reduced total shoulder rotational movement compared to controls in their cohort of baseball players. Tenderness to palpation is another physical assessment component that is commonly encountered, although reliably being able to objectify this may be challenging. In general, the physical assessment components reported in this review align with a recent UK survey of NTOS clinicians. 15
Future research should prioritize consistent, measurable assessment criteria to support logic model development and standardise therapy approaches.
Rehabilitation
Rehabilitation interventions for NTOS were vast, with considerable overlap in their descriptions. This review has summarised the main elements, their components and their potential therapeutic targets, which is hopefully helpful to the clinician when building a rehabilitation programme. Exercise was the most frequent element encountered (n = 17), with both stretching (n = 15) and strengthening (n = 14) exercises targeting the neck and shoulder girdle. These interventions were commonly proposed to “decompress” the thoracic outlet. Neural mobility exercises (n = 7) were also included to reduce sensitivity in the neurovascular structures. Postural improvement was a feature of several studies included in this review (n = 13), with most (n = 11) suggesting exercise as the primary method to achieve this. However, few studies either assessed or re-tested functional markers before and after treatment, making it difficult to draw firm conclusions about the efficacy of these interventions. Only four studies in this review reported objective functional markers in NTOS patients.50,53–55 PROMs, such as the QuickDASH (n = 12), CBSQ (n = 8) and SF-12 (n = 6) dominated the outcome measures, perhaps due to the increasing awareness of and adherence to the SVS reporting guidelines. 17
Clinical reasoning
Inconsistencies were identified within the included studies regarding the justification for rehabilitation components for NTOS. Studies cautioned against the use of neural mobility 44 and resistance 7 exercises for fear of exacerbating symptoms, despite both featuring prominently in most rehabilitation descriptions. Additionally, manual therapy to the first rib was encouraged in five studies,19,22,38,44,45 but excluded from a rehabilitation package in an RCT 8 as they felt it may aggravate pain. The scapula also emerged as a prominent rehabilitation focus within the included articles in this study (n = 9), mirroring its frequent role in posture assessment. Studies proposed that improving the stabilisation of the scapula can help decrease symptoms, but how this was purported to be achieved differed. Several studies proposed completing scapular depression/retraction exercises,24,38,45,48 whereas two studies advised against them.19,44 The latter argued that excessive scapular depression may increase compression or mechanical stress on neurovascular structures within the thoracic outlet, instead promoting exercises that enhance scapular elevation and upward rotation.
In the authors' opinion, both approaches may be valid. For example, patients with shoulder protraction and forward head posture may benefit from retraction exercises, while strengthening into elevation and upward rotation supports accepted functional scapular kinematics required for efficient shoulder function. 57
Additionally, there are notable discrepancies between the rehabilitation programmes delivered in primary studies and those proposed in review articles. A six month duration of rehabilitation was the most recommended timeframe across five review articles.9,24,39,40,42 However, none of the larger prospective studies provided rehabilitation over this timeframe (Table 4).7,8,11
Shorter durations may reflect research constraints, though 6 months is commonplace in NHS practice in the authors' experience, and this is supported by UK survey data. 15
Only one study 44 proposed psychologically informed treatment for NTOS, despite its widespread use in the management of chronic pain conditions. 58 This highlights a persistent biomedical bias in NTOS care. Incorporating holistic PROMs could guide more comprehensive therapies, for which excellent long-term results have been recently published for chronic disabling low back pain. 59
Predicting which NTOS patients are likely to benefit from therapy would be highly advantageous, both for optimising patient outcomes and for the efficient allocation of healthcare resources. Balderman et al. 7 identified characteristics associated with a favourable response to rehabilitation compared to those who eventually opted for surgery. In general, patients who responded positively had less severe symptoms, including reduced tenderness to palpation, less severe CBSQ and SF-12 (Physical Component) scores, fewer positive clinical diagnostic criteria, and a trend to a greater tolerance of the EAST test. This observation is consistent with our clinical experience and is supported by findings in other upper limb conditions, where less severe symptoms have been identified as positive prognostic indicators for rehabilitation response. 60 Further cohort studies focusing on NTOS patients undergoing rehabilitation would help advance this area of research. Notably, some studies included in this review did not provide detailed profiles of patients who responded positively to rehabilitation, 11 limiting our ability to draw stronger conclusions about predictive factors.
Finally, the classification and terminology surrounding NTOS remains inconsistent and, at times, confusing. Multiple variations, such as “true,” “disputed,” “symptomatic,” and “miscellaneous” were still evident in the studies reviewed, despite the presence of generally accepted reporting standards. 17 The EANS consensus study 47 proposed a new classification system (NTOS 1, 2, 3a/b/c), which may offer some value, particularly in identifying patients who may not be suitable candidates for rehabilitation, such as those with NTOS 1, who present with objective intrinsic muscle atrophy and weakness. However, adding another classification system risks further confusion within both clinical and research settings. A unified classification would improve diagnostic clarity, treatment planning, and research consistency.
Treatment reporting
This review used the TIDieR checklist to extract and organise data on rehabilitation interventions, which we hope has been useful to readers. However, it also highlights the generally poor reporting of rehabilitation for NTOS. Rehabilitation descriptions are often superficial, making it difficult to replicate the methods across different settings. Excluding case studies, only two expert opinion pieces19,38 provide sufficiently detailed rehabilitation protocols that could be reproduced with confidence. However, these protocols remain untested. To advance NTOS rehabilitation, standardised, reproducible protocols are needed to enable comparison across studies. A dedicated study focused solely on therapy management for NTOS, designed and delivered by therapists, would significantly strengthen the evidence base.
Recommendations
Based on the aims and findings of this review, we propose recommendations for physical assessment, rehabilitation, and the use of PROMs in NTOS (Figure 4). Recommendations for the physical assessment, rehabilitation and measurement of NTOS based on studies main aims and results. (CBSQ: cervical brachial symptoms questionnaire; EAST: elevated arm stress test; PROMs: patient reported outcomes measures; SF-12: short form 12; ULTT: upper limb tension test). 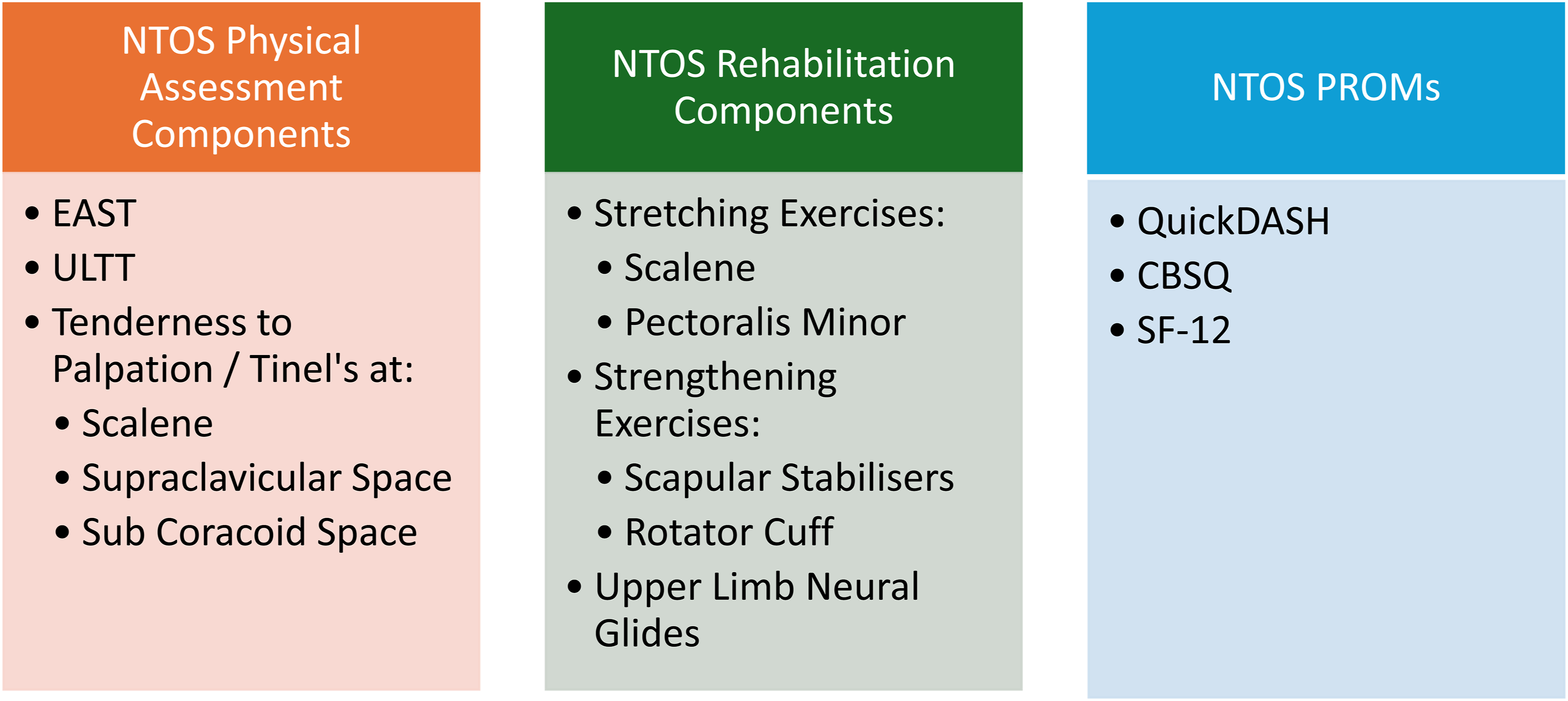
Limitations
This review aimed to use transparent and rigorous methods, but there are some limitations. Firstly, scoping reviews strike a balance between breadth and depth of research, 61 and as such, there are areas we were unable to address (such as imaging and injections). Additionally, despite our efforts to identify and describe the included studies physical assessment and rehabilitation components for NTOS, it is still apparent that this remains a complex area, with no widespread conformity on the diagnosis or classification of NTOS, therefore interpretations that this article draws may not be widely generalisable. Moreover, a known limitation of scoping reviews, is the lack of quality appraisal or risk of bias assessment of included articles, therefore it is possible that studies with poor methodological quality may have led to misleading interpretations, which contrasts with a systematic review. 28 Nevertheless, we believe this review has met its objectives and that the scoping review methodology was the most appropriate approach. Additionally, we acknowledge that some studies published before 2000 or in foreign languages may have been missed in this review.
Finally, when selecting articles based on the inclusion criteria, it was subjective to determine whether a study had described physical assessment or rehabilitation “sufficiently.” However, both reviewers (JOS & CR) discussed any disagreements until consensus was reached.
Conclusion
NTOS is a clinically complex condition to both assess and rehabilitate for therapists working within musculoskeletal and hand therapy settings. A vast array of potential assessment and rehabilitation components for the management of NTOS are reported but are generally untested. The reporting of rehabilitation interventions for NTOS is generally insufficient, inhibiting the creation and evaluation of homogenous rehabilitation programs, which are needed to advance the evidence base concerning the therapy management of NTOS.
There is a critical need for a standardised, reproducible rehabilitation treatment regime for NTOS, ideally co-designed by both experienced NTOS clinicians and NTOS patients. The use of consistent outcomes, including both PROMs and functional markers measured pre- and post-treatment, could help establish a logic model to assess the effectiveness of rehabilitation.
Supplemental material
Supplemental Material - Physical assessment and rehabilitation for neurogenic thoracic outlet syndrome (NTOS): A scoping review
Supplemental Material for Physical assessment and rehabilitation for neurogenic thoracic outlet syndrome (NTOS): A scoping review by Joel O’Sullivan, Christian Rushton, Marcus Bateman, Caroline Miller, Claire Stapleton and Jonathan Hill in Hand Therapy
Supplemental material
Supplemental Material - Physical assessment and rehabilitation for neurogenic thoracic outlet syndrome (NTOS): A scoping review
Supplemental Material for Physical assessment and rehabilitation for neurogenic thoracic outlet syndrome (NTOS): A scoping review by Joel O’Sullivan, Christian Rushton, Marcus Bateman, Caroline Miller, Claire Stapleton and Jonathan Hill in Hand Therapy
Footnotes
Acknowledgements
We would like to thank Jennifer Davis-Manders, Library site manager at University Hospitals Birmingham NHS Foundation Trust, for her assistance with literature searches.
Author contributions
JOS, CS and JH conceived the presented idea. JOS and CR completed the search and collected the data. JOS analysed and interpreted the data with help from CR, MB, CM, CS and JH. The article was drafted by JOS. Article was reviewed and edited by all authors. All authors were involved in the final approval of the version of the article to be presented.
Funding
JOS is currently on a National Institute for Health Care Research (NIHR) Doctoral Clinical and Practitioner Academic Fellowship (NIHR304106). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
JOS.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.