
Abstract
Introduction
Non-traumatic wrist disorders (NTWD) are commonly encountered yet sparse resources exist to aid management. This study aimed to produce a literature map regarding diagnosis, management, pathways of care and outcome measures for NTWDs in the United Kingdom.
Methods
An interdisciplinary team of clinicians and academic researchers used Joanna Briggs Institute guidelines and the PRISMA ScR checklist in this scoping review. A mixed stakeholder group of patients and healthcare professionals identified 16 questions of importance to which the literature was mapped. An a-priori search strategy of both published and non-published material from five electronic databases and grey literature resources identified records. Two reviewers independently screened records for inclusion using explicit eligibility criteria with oversight from a third. Data extraction through narrative synthesis, charting and summary was performed independently by two reviewers.
Results
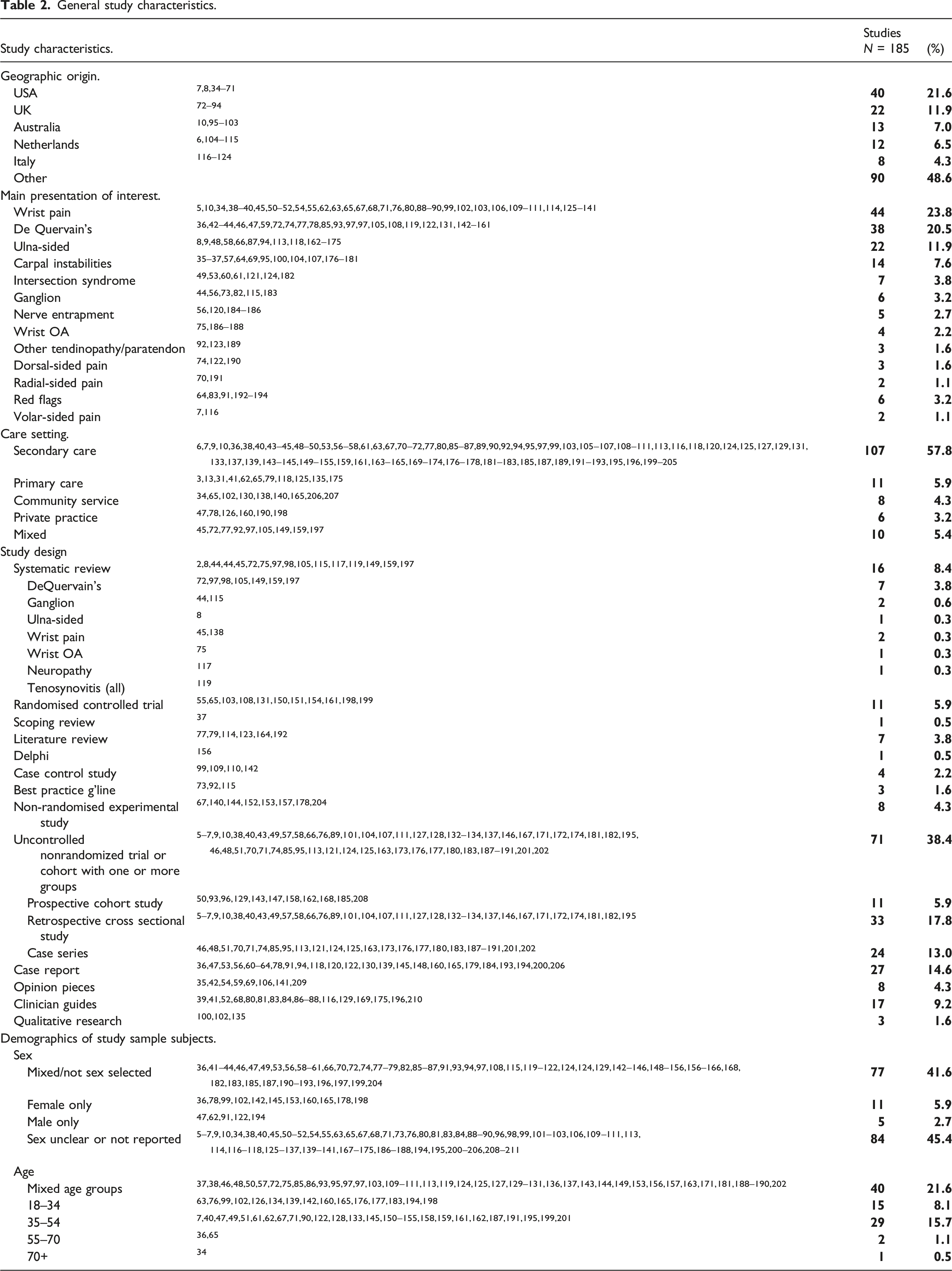
Of 185 studies meeting eligibility criteria, diagnoses of wrist pain, De Quervain’s syndrome and ulna-sided pain were encountered most frequently, with uncontrolled non-randomised trial or cohort study being the most frequently used methodology. Diagnostic methods used included subjective questioning, self-reported pain, palpation and special tests. Best practice guidelines were found from three sources for two NTWD conditions. Seventeen types of conservative management, and 20 different patient-reported outcome measures were suggested for NTWD.
Conclusion
Substantial gaps in evidence exist in all parts of the patient journey for NTWD when mapped against an analytic framework (AF). Opportunities exist for future rigorous primary studies to address these gaps and the preliminary concerns about the quality of the literature regarding NTWD.
Introduction
Wrist pain is commonly encountered with an annual consultation rate of 58 in 10,000 patients in primary care in the UK. 1 Its incidence increases in people who engage in physically demanding occupations and for sportspeople where 10% have been found to have short-term pain, and 24% have medium-term pain. 2 Non-modifiable associations with wrist pain include older age and female sex. 2 In the UK’s National Health Service (NHS), a typical clinical pathway for patients with wrist disorders would see initial diagnosis and management in primary care, with referral through a musculoskeletal service for further diagnostic assessment and treatment in secondary care based on clinical need.3,4
The main pathological causes of non-traumatic wrist disorders (NTWD) include carpal osteoarthritis (OA), tendinopathies (including De Quervain’s and intersection syndrome), ulnar-sided wrist pathologies (itself made up of sub-groups with poor diagnostic validity),5–11 and ganglion. NTWD are distinct from basal thumb and hand osteoarthritis based on the clinical burden, risk factor profile, clinical relevance of synovial inflammation and established therapeutic interventions, however there is a degree of overlap between pantrapezial and wrist OA.12,13 Other presentations considered distinct from NTWD due to established diagnostic criteria, and condition-specific care pathways and management strategies include rheumatoid arthritis, 14 carpal tunnel syndrome15–17 and complex regional pain syndrome, 18 and were excluded from this study.
Uncertainty in various parts of the journey of care for people with wrist and hand pain was highlighted in a James Lind Alliance Priority Setting Partnership.19,20 Specifically, stakeholders identified a need for more information on which surgical and conservative methods enable efficient return to function, and which patient-reported outcomes are most useful in measuring the effectiveness of management. Although this review is limited to non-surgical literature these findings were a motivating factor to assessing the literature regarding NTWD in this review. In order to set research questions that are derived from stakeholder and patient involvement, 21 this review convened a mixed stakeholder group to identify key areas for investigation.
The NHS Long Term Plan 22 recommends patient-centred models of care through ‘shared decision making’ over historic paternalistic models which emphasise expert opinion and passive care and states this is a pressing need as rates of non-communicable diseases rise and questions around musculoskeletal management are increasingly raised. 23 Lewis and O’Sullivan caution that trends toward an unwarranted specific musculoskeletal diagnosis in non-traumatic conditions are placing strain on health budgets and may divert resources from ‘high-value’ person-centred care, to the prioritisation of ‘low-value’ interventions targeted at uncertain diagnostic categories. 24 When evaluating musculoskeletal care for the shoulder, low back and knee, pathoanatomical diagnosis frequently fails to explain the sufferers’ pain experience and disability in non-traumatic disorders, nor improve outcomes, leading to recommendations for the use of grouped conditions to frame management.25–27 This viewpoint has synergy with The Management of Wrist Pain Group (MOWP) which suggests grouping specific non-traumatic wrist diagnoses into a broader category of non-traumatic wrist pain 28 to promote holistic rather than lesion-specific management. Through mapping the literature of all diagnoses making up NTWD, the areas of strength for particular categories can be identified.
This scoping review aims to identify the evidence for the diagnosis, management, pathways of care and outcome measures for both grouped and individual NTWD and produce a coherent and comprehensive map of key evidence gaps to direct future research.
Methods
A protocol for the review was registered on the Open Science Framework prior to conducting any searches: https://osf.io/mxz59/.
Study team composition
The review team of six comprised clinicians, academics, subject area specialists and a design-led expert.
Scoping review framework
Scoping review methodology allows a systematic approach to map evidence into poorly understood areas 29 and draws on evidence from both empirical research and grey literature sources. The current study adopted the academic standard Joanna Briggs Institute (JBI) methodology 29 for scoping reviews and the PRISMA-ScR checklist. 30
Developing a rationale and identifying the research questions
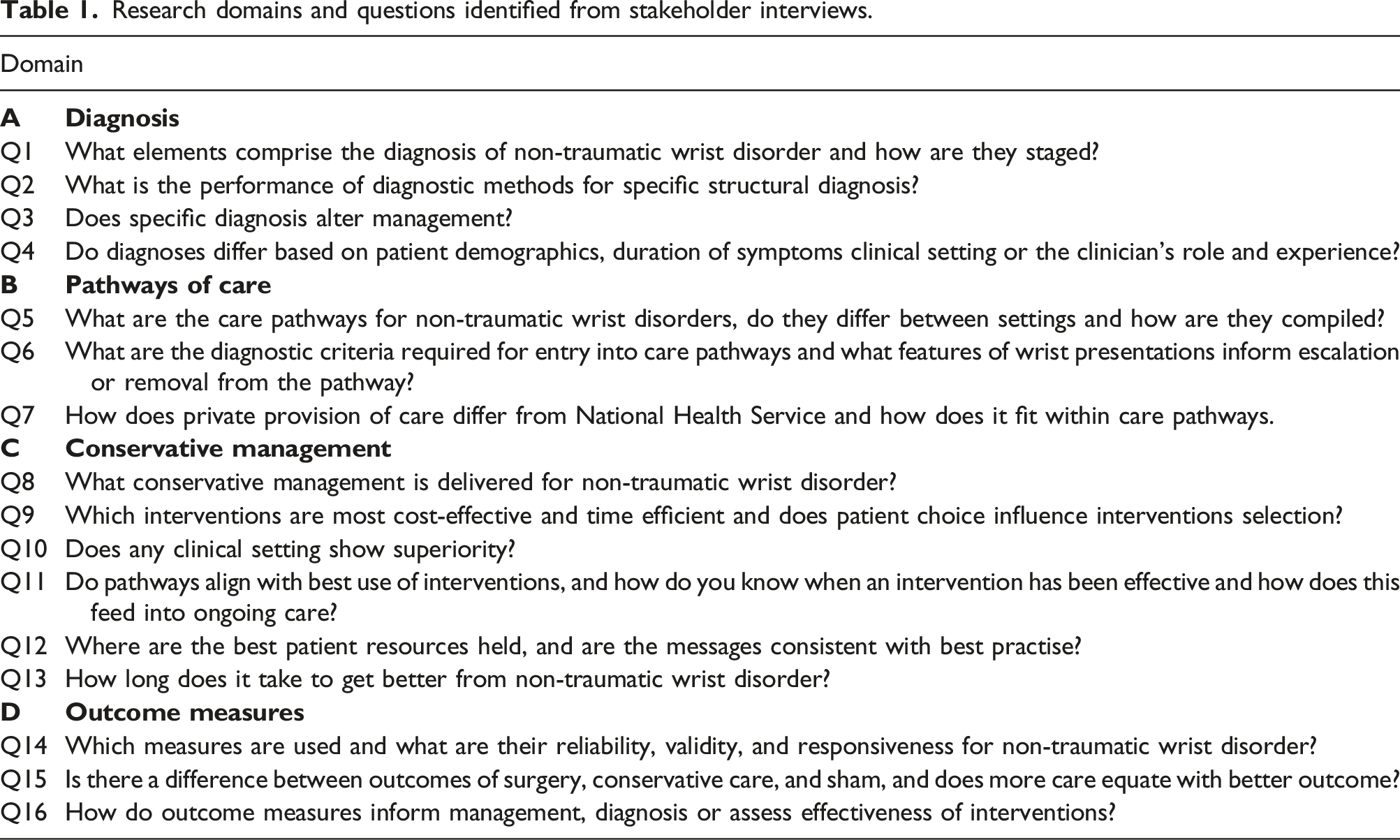
Research domains and questions identified from stakeholder interviews.
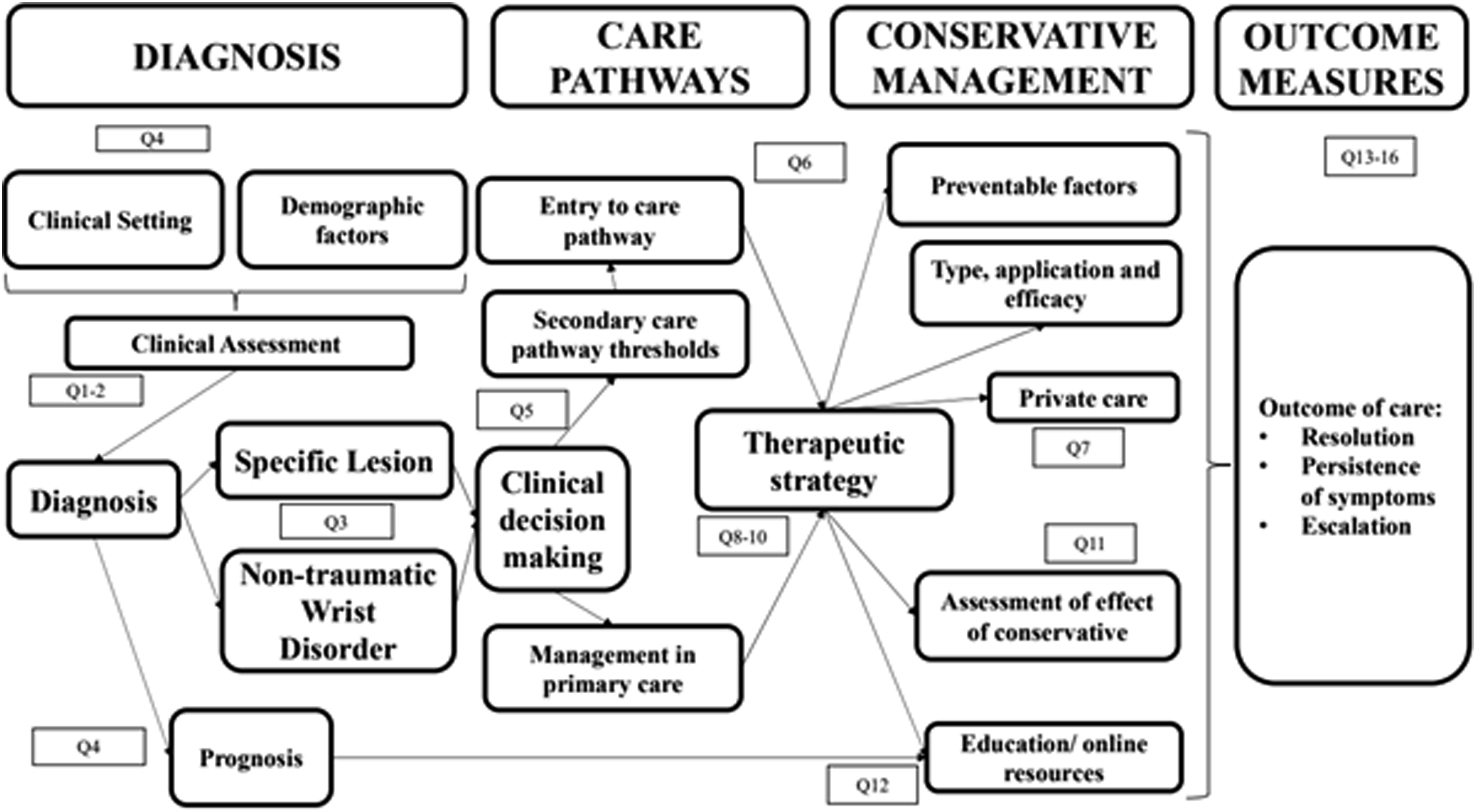
Analytic framework based on clinical journey of NTWD with key domains and related research questions.
Identifying relevant studies
The three-step method recommended by the JBI guidelines for scoping reviews was followed. The search strategy was intended to be broad to identify both published and unpublished (grey) literature. Initially a narrow search of Google Scholar and MEDLINE database was used to identify key literature with additional studies identified through a snowballing technique using SCOPUS to identify related literature and citations from more recent work. The University of Tasmania guide to developing search terms 33 was applied, and we performed an analysis of the found studies to identify text words and key words relevant to the area. MeSh terms were collated via Medline to create the search strategy for Step 2 of the review (Supplementary section - 1). We applied this to MEDLINE then to PUBMED, OT Seeker, PeDRO and SPORTDiscus with minor adaptations made ad hoc to fit database requirements. Finally, a snowballing technique and citation search from key articles using SCOPUS was applied, combined with asking experts in the field for their recommended papers.
To allow non-journal and grey literature sources to be identified, we searched a variety of ‘grey literature’ databases and library catalogues via OpenGrey and Library Hub Discover (formally COPAC). Doctoral theses were identified via Ethos and ProQuest and clinical trial registers were screened via the World Health Organisation International Clinical Trials Registry Platform and the NIHR’s ‘Be Part of Research’ platform. Finally, clinical resources from BMJ Best Practice, NICE Evidence Standards Framework, the Cochrane Library and Trip were searched.
Study selection
The titles and abstracts of studies identified in the literature search were uploaded into Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia) and duplicates removed.
Explicit a priori eligibility criteria (Supplementary Section 1) were applied at Level 1 (title and abstract) and Level 2 (full text) screening. A record was included if it provided an answer to at least one of the 16 research questions (Table 1) in the analytic framework (Figure 1) and did not meet any of the exclusion criteria. The Population, Concept and Context (PCC) method proposed by JBI were used to guide the identification and inclusion of published studies of all methodologies.
Population
Studies of people diagnosed with wrist disorders without traumatic origin were identified as the population. Those with clear history or radiological evidence of substantial trauma were excluded (i.e., scaphoid fracture/distal radius fracture/fracture clinic patients). Those with a history of less substantial minor trauma were not excluded. People who have had surgical management for their non-traumatic wrist disorder were excluded as were athletes.
Concept
The concept of interest in this review included the means of assessment for non-traumatic wrist disorders, conservative/non-operative interventions commonly administered, and the pathways of care and outcome measures used in primary and secondary care.
Context
This review considered both primary and secondary healthcare settings as each are part of the continuum of care for non-traumatic wrist disorders in the UK. The research questions arose from the consultation exercise to allow a broad approach considering the patient journey, clinician input and wider management structures.
Screening
Material that appeared to meet the initial screen of title and abstract was retrieved as complete reports and matched against the inclusion criteria leading to acceptance or discard by two reviewers (TM & SR), followed by a review of the full texts (TM & SR). Disagreements that arose between the reviewers were resolved through discussion, or consulting with a third reviewer (BD).
Data extraction and synthesis
The two primary researchers (TM & SR) extracted the following data for each included article: • Authors, year of publication, country of origin. • Research question, aims and domains selected by study authors. • Methods: study design. • Participants: number of participants included, eligibility criteria, sociodemographic data (sex and age). • Non-traumatic wrist disorder diagnostic method. • Pathways of care. • Management modality administered including its parameters. • Outcome measures and indications for escalation discharge or self-management.
Literature was appraised using qualitative synthesis and related to the analytic framework and its key domains and research questions. A knowledge map assessing the extent to which the analytic framework met by the literature was formed and used to identify gaps in the literature and research priorities in future clinical research.
Results
The initial search strategy identified 8767 documents, with 16 added from a search of cited references giving a total of 8783 sources (Figure 2). 1528 duplicates were removed, and screening of titles and abstracts resulted in 901 documents selected for full-text assessment. There were 47 instances where full text was unavailable, 669 did not meet the eligibility criteria, leaving 185 suitable for inclusion (Supplementary Section 2). PRISMA flow diagram for NTWD scoping review.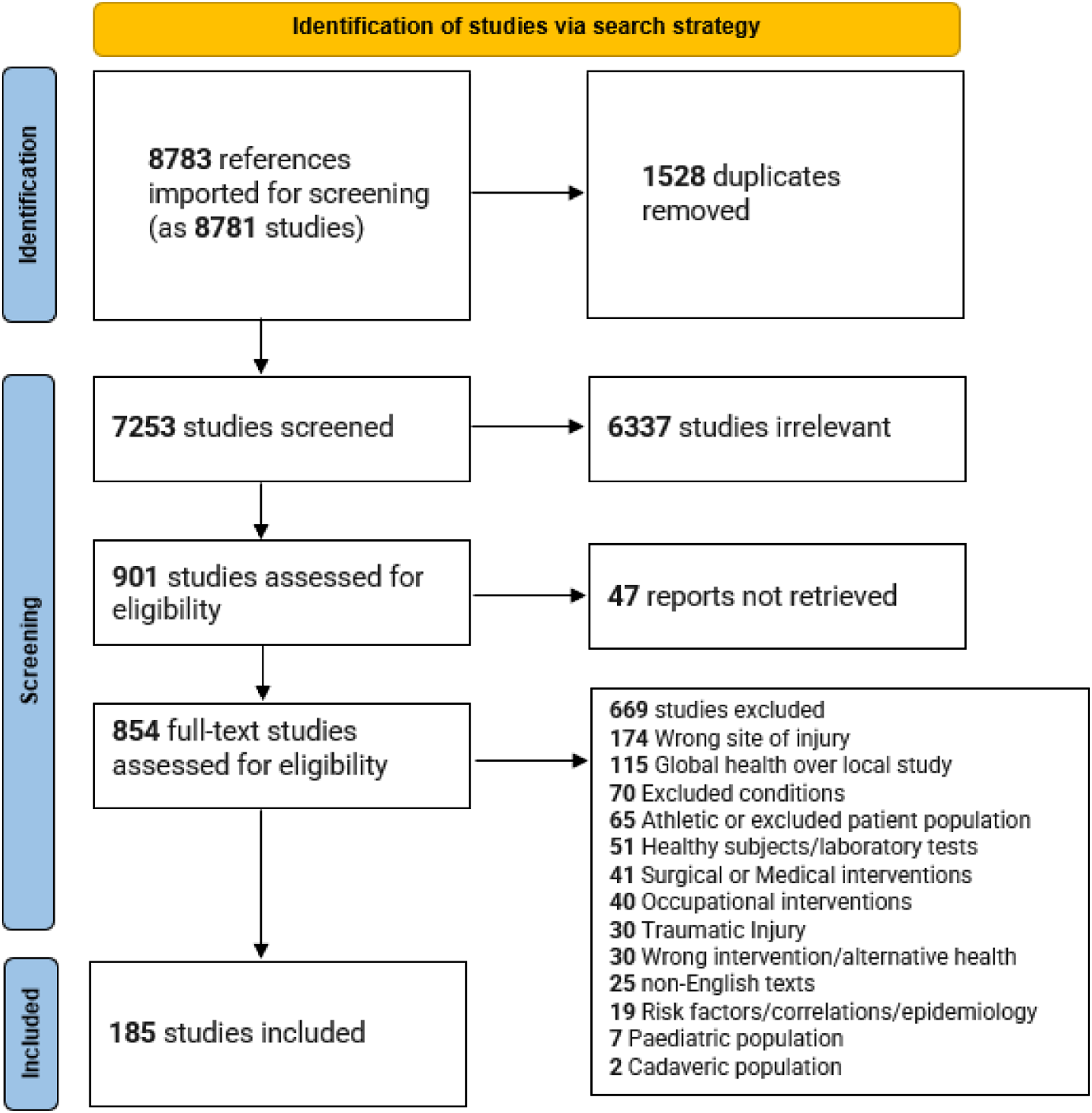
General study characteristics.
Studies that addressed research questions in domain A: diagnosis
Methods of diagnosis (Supplementary Section 3) were commonly stated (Q1) with subjective questioning, (36, 19.5%), self-reported pain (35, 18.9%) and heat maps (1, 0.5%) representing patient-described symptoms. The use of special tests (51, 27.9%), palpation (33, 17.8%), range of motion assessment (28, 15.1%), manual accessory motion (20, 10.8), grip (7, 3.8), weighing scale and push-off tests (2, 1.1%), and laterality assessment (1, 0.5%) represent clinician-dependent examination methods stated. The range of individual special tests referred to in the literature numbered 25. Finklestein’s was the most commonly mentioned special test, however divergence in how this was described and confusion between this and Modified Eichoff was noted.157,158 Six studies (3.2%) described algorithms for the staging of the methods of assessment. MRI/MRA scans (35, 18.9%), X-ray (30, 16.2%), ultrasound scan (24, 13.0) nerve conduction studies (5, 2.7%), CT scans (3, 1.6%), and arthroscopy (11, 5.9%) were the most common advanced diagnostic methods found.
The performance of various diagnostic methods (Q2) were assessed in 37 papers (20%), with six studies detailing how specificity of diagnosis informed management (3.2%, Q3), of which three were best-practice guidelines, with the remaining referring to the benefits of early diagnosis, 139 staged management of de Quervain’s 159 and ulnar-sided wrist pain. 169 The impact that individual patient related factors had on diagnosis was found in 17 studies (9.2%), specifically age, clinic setting and sociodemographic factors (4, 2.2%), and three for sex (1.6%) (Q4).
Studies that addressed research questions in domain B: pathways of care
Two care pathways from the British Medical Journal were found for ganglion and tenosynovitis of the wrist (Q5) and composed through literature reviews from area experts (Q6). Other care pathways involved a chronic wrist pain algorithm, management of ganglion and a consensus document on the treatment guidelines for De Quervain’s. The interaction between private and public health provision was not explored (Q7). All pathways identified are displayed in Supplementary Section 4.
Studies that addressed research questions in domain C: Conservative management
Seventeen different conservative/non-operative management adjuncts to manage NTWD were referenced (Q8) in (Supplementary Section 5). The most common being injection (25, 13.5%), splinting (23, 12.4%), local exercise and manual therapy (18, 9.7%), activity modification (20, 10.8%), global exercise (9 studies, 4.9%), manual therapy sensorimotor and proprioceptive training (8 studies, (4.3%).
Cost implications of investigations were raised in five studies (2.7%), one finding routine X-ray was not cost-effective, three cautioning against the costs of investigations when they rarely change management but without scaling of costs, and one suggesting ultrasound sonography represents best value in emergency departments (Q9). Cost assessment was found for the use of injection and splints as first-line treatment for de Quervain’s, but no assessment of time efficiency nor the impact of patient choice in conservative/non operative options (Q9) was found. The effect of the clinical setting was discussed in one article which found that Primary Care was as effective in the delivery of injection as secondary care (Q10). For Q13 there were three studies which looked at the expected natural history of NTWD, one related to de Quervain’s, one regarding primary care presentations and one on the expected recovery following surgical management of ulna-sided pain.
Studies that addressed research questions in domain D: Outcomes
The recommendation for the use of, or investigation of the validity of outcome measures of interventions (Q14) was common, with 20 different Patient Reported Outcome Measures (PROMs) found (Supplementary Section 6). The Disabilities of the Arm, Shoulder and Hand (DASH) or QuickDASH 212 (16, 8.6%) and Patient-related Wrist and Hand Evaluation 138 (8, 4.3%) were most frequently referenced. Other methods of assessing outcomes were self-reported pain (26, 15.1%), changes in range of motion (28, 15.1%), visual analogue scale (VAS) (16, 8.6%), patient reported numerical score (6, 3.2%), grip strength (7, 3.8%) and changes on investigation findings were used in four instances (2.2%). Six studies (3.2%) were found which addressed Q15 in creating a hierarchy superiority of management approaches. Two related to de Quervain’s and the case for injection of steroid as an effective alternative to surgery, and two related to ganglion where injecting cortisone was not indicated over conservative/non-operative management. No studies were identified which specifically looked at the how outcome measures inform management (Q16).
Mapping onto the analytic framework
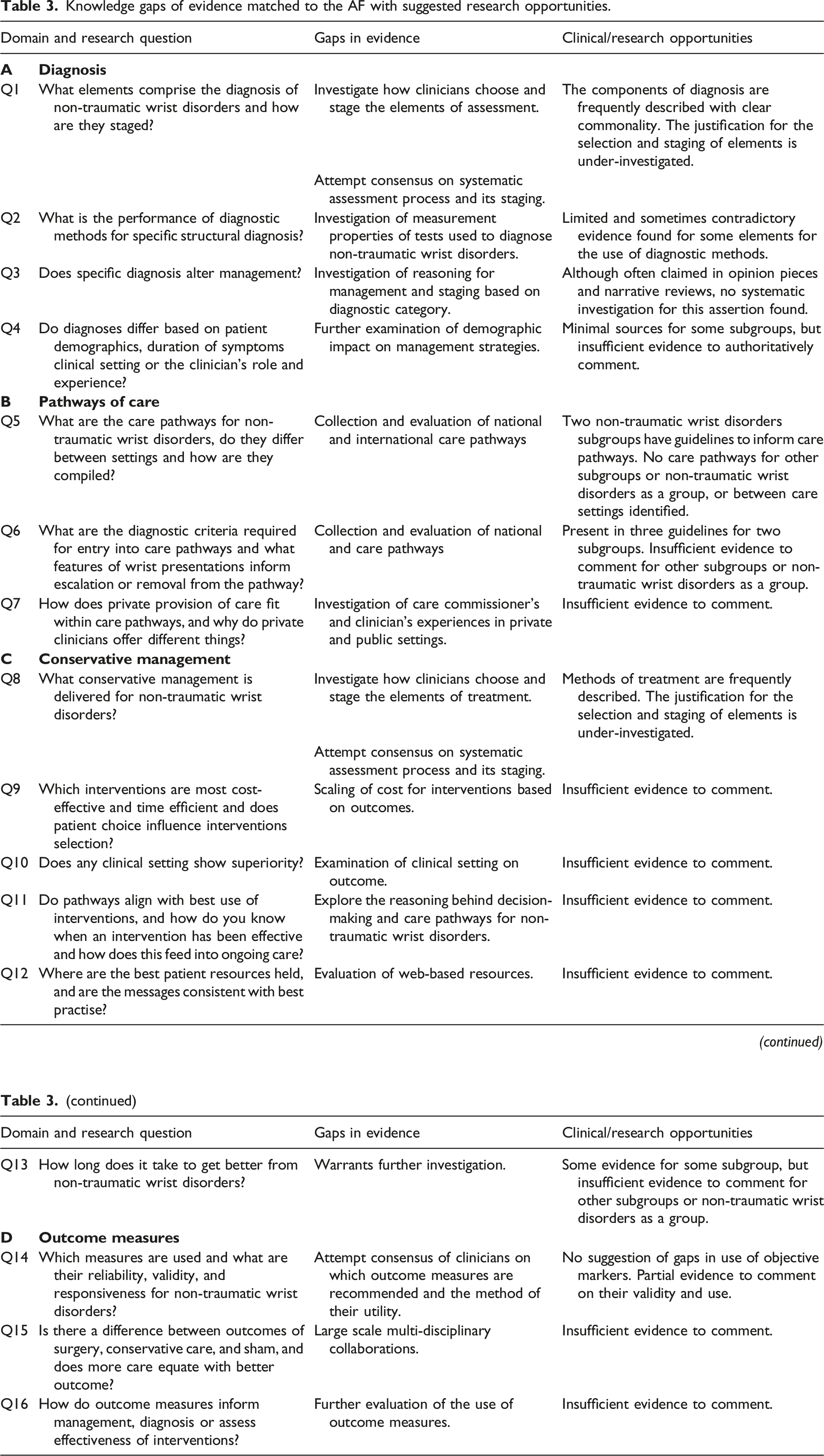
Knowledge gaps of evidence matched to the AF with suggested research opportunities.
Discussion
The general study characteristics revealed a substantial proportion of the included sources comprised of evidence such as clinician guides, opinion pieces and case reports (52 studies, 28.1%). There is a risk that the volume of poor-quality evidence may ‘wash out’ the evidence derived from more rigorously designed and conducted studies and suggests peer learning is prominent in this field. The predominance of secondary care settings may indicate higher concentrations of research-active clinicians in secondary care rather than revealing the extent of NTWD presenting in this setting. It is likely higher rates of presentation of NTWD occur in primary and community settings at earlier stages of the care pathway that do not progress to secondary care which may be relatively under-researched. It is notable that uncontrolled nonrandomized cohort trials (71, 38.4%) were more prevalent than RCTs or experimental studies (19, 10.3%). This is driven partly by the large number of evaluations investigating the performance of advanced diagnostic machines when compared to either consultant clinical diagnosis or arthroscopic findings. The appetite for investigating new forms of scanning equipment or to validate new clinical tests for biomechanical diagnosis is consistent, however it is interesting that some authors have questioned the reductionist premise that biomechanical lesions are the modifiable factors to target in assisting patients with NTWD.7,9,10,28,157,162,172,202 The other reviews (systematic, literature and scoping) represent well-conducted enquiries into the methods of conservative/non-operative management of wrist disorders and provide good information on the risk factors and epidemiology of wrist pain.
There was sufficient evidence to identify the range of assessment techniques, treatment techniques and outcome measures (Q1, Q8 & Q14), however all domains have evidence gaps related to the AF questions allowing ample opportunity for further investigation. The absence of care pathways returned from searches for subgroups and NTWD as a whole reveals a pressing requirement to understand what care is currently being delivered and how a person with NTWD navigates toward optimal management.
That a plethora of diagnosis methods, conservative/non-operative management types and means of assessing outcomes have been identified, indicates a lack of consensus in best practice for navigating the journey of care for people with NTWD. Future work should prioritise the calculation of the burden of cost and care, which NTWD represents, to give staging of research priorities.
Potential opportunities for further studies
There is a need for further enquiry amongst clinicians and patients to identify what meaningful assessment looks like and how outcomes are best contextualised. To this end, the development of best practice guides for assessment, conservative/non-operative management options and outcome measures for NTWD would be beneficial, with recommendations on their staging. Further investigation of patient information would be useful. The means of achieving this is likely to require a mix of methodologies.
Strengths and limitations of the review
The strengths of this review include its pre-registration on the Open Science Framework. The use of an interprofessional study team, rigorous search strategy, broad sources of literature, and engagement with a mixed stakeholder group of patients and healthcare professionals to create key questions, which were refined and expanded to form an AF based on the clinical journey of patients with NTWD in the UK, add to this strength. Limitations are in part related to the nature of scoping reviews as the broad search strategy and research question resulted in the inclusion of a large number of studies of great heterogeneity. At full-text-level review, 289 sources were excluded due to ‘wrong site of injury’ or ‘global disorders’ reflecting wrist and hand being used interchangeably. The restriction of studies selected to those of the English language was a further limitation.
Conclusion
Significant uncertainty exists across all domains of the NTWD patient journey. There is a need for knowledge synthesis to guide musculoskeletal practitioners to administer effective, evidence-based interventions at all points along the clinical care pathway. This scoping review’s findings will help guide further research and assist us in the long-term goal of generating knowledge synthesis.
Supplemental Material
Supplemental Material - A scoping review to map evidence regarding key domains and questions in the management of non-traumatic wrist disorders
Supplemental Material for A scoping review to map evidence regarding key domains and questions in the management of non-traumatic wrist disorders by Thomas Mitchell, Nick Hamilton, Ben Dean, Sarah Rodgers, Sally Fowler-Davis and Sionnadh McLean in Hand Therapy
Footnotes
Acknowledgements
We would like to thank Professor George Peat for his assistance as a contributor in this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was made possible through the funded Graduate Teaching Associate scheme which was awarded to TM from Sheffield Hallam University as part of his PhD programme.
Guarantor
SM.
Contributorship
TM, BD and SM conceived the study and developed the search strategy. TM, BD and SR reviewed the literature and TM wrote the initial manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.