
Abstract
Introduction
Youth with brachial plexus birth injuries (BPBI) have an increased risk of mental health issues such as depression, anxiety, and diminished self-confidence. Despite this evidence, current standards of care focus on physical interventions. Evaluation of psychological and emotional concerns is rarely prioritized in clinical settings. Therefore, mental health needs are unmet and poorly understood.
Methods
An interpretivist qualitative approach was used to understand the perspectives of youth with BPBI and their caregivers on the barriers and facilitators of addressing mental health concerns, to inform practice guidelines, and promote meaningful participation within this population.
Results
A purposeful sample of nine youth with BPBI between 10 to 20 years and eight caregivers participated in in-depth interviews. The interviews were semi-structured and an average of 60 min (35–85 min) long. Three themes emerged from these data: (i) physical disability identity and mental health; (ii) pursuit of “normal” body image; and (iii) paradox of advocacy. Findings illuminated the intersection of physical and mental health in these youth and provides actionable practice recommendations. Areas of need were identified including mental health support around the challenges of advocacy, body image, surgery, and preparation for the ‘aging out’ process for youth and their families.
Conclusions
The well-being of youth with BPBI is a result of the intersection between their physical and mental health. Further research on optimizing mental health resources within physical health settings is needed to better support the holistic needs of these youth and their families.
Introduction
Youth with brachial plexus birth injury (BPBI) have upper limb physical impairments and appearance-related concerns that place them at risk for poor mental health. 1 The resultant loss in sensory and motor function from damage to some or all of the spinal roots (C5-T1) results in orthopaedic sequelae including muscle imbalances, joint contractures and dysmorphology. 2 At a basic level, the stress of living with physical impairments, pain, and ongoing medical care negatively affects their health-related quality of life (HRQoL).3,4 Youth with BPBI report decreased participation in self-care and leisure activities such as bathing, handwriting, swimming and eventually, choice of employment and education pursuits.5,6 Though youth report decreased participation in these domains, it is unknown how these difficulties affect their mental health. Evidence from studies using patient-reported outcomes indicates that these youth have reduced self-confidence, subjective well-being, and psychosocial functioning.3,7,8,9 However, it is unclear if these factors directly link to poor mental health outcomes and mental disorders in these children. As participation is influenced by mental and physical factors, exploring mental health experiences that include mental well-being and disorder, is an important step to characterizing participation of youth with BPBI.
Despite known risks, resources to support mental health promotion, prevention, and interventions to address mental health are limited. 1 There is a paucity of literature on standards of care to support mental health in these youth and their families. Current models of care focus on physical rehabilitation and reconstructive surgery to improve function and appearance. 11 For example, the BPBI outpatient clinic at the Hospital for Sick Children (SickKids) in Toronto, Canada offers a multidisciplinary approach to care including plastic and orthopaedic surgery, nursing, physical and occupational therapy, and social work. As physical needs take precedence, there are often few routine resources to address mental health concerns. 1 Consultative social work services, mutual support education days, and peer-to-peer support may be offered. 12 However, identified mental health programs are short-term, rarely extend beyond standard care and are not accessed by all youth. It is not known how to adequately address the psychological and psychosocial needs of these youth. Therefore, the purpose of this study was to elucidate the mental health experiences of youth with BPBI and their caregivers, as well as their perceived barriers and facilitators of the healthcare approach in addressing mental health within a multidisciplinary BPBI clinic.
Methods
The study design of this research is an interpretivist qualitative approach 13 to elicit depth and appreciation for individual experiences of youth and their caregivers in the SickKids BPBI clinic. In this approach, the discipline and clinical contexts of the researchers frame the inquiry and define the conditions of the research. 13 The integrity of our purpose derives from our practice goal of providing interdisciplinary care to youth with BPBI and their families, and acknowledgement that empirical evidence influences our interpretive lens. The study was executed through in-depth, semi-structured interviews of youth with BPBI and their caregivers. The study was approved by the research ethics board at SickKids and the University of Toronto.
Participants for this study included youth and their caregivers who were existing patients of the SickKids BPBI program. Participants were identified by a healthcare professional within their circle of care and engaged in the informed consent and assent process with a research team member if interest in the study was expressed. Homogenous purposive sampling was used to identify and select youth and caregivers with specific experiences pertaining to mental health within the clinic. 14 Participants were no longer recruited once the depth and breadth of the information gleaned from the interviews were sufficient to achieve thematic saturation. 15 The inclusion criteria were: youth with BPBI aged 10–20 years and caregivers to explore mental health experiences that represented the continuum from pre-adolescence, adolescence, and the transition period out of paediatric care. The initial plan was to recruit youth with BPBI and a diagnosed mental disorder; however, this criterion was expanded to include those with and without mental health symptoms to obtain a diversity of mental health experiences. Priority was given to individuals who were identified by their attending healthcare team as able to richly describe their experiences with healthcare access and management. The exclusion criteria for youth participants included: comorbidities affecting both upper and lower limb function, diagnosis of a syndrome, severe cognitive or neurodevelopmental delay, or an inability to communicate in English at a minimum of a grade four level. Caregiver participants were excluded if they did not communicate in English at a minimum of a grade four level.
Study demographic data were collected from participant health records and managed using REDCap® electronic data capture tool. Virtual in-depth interviewing of youth and their caregivers was conducted by two researchers (HP, CN) over Microsoft (MS) Teams on a secure Wi-Fi network. The interviewers were two graduate students who were trained in qualitative interviewing by the senior author (ESH). The interviews followed a predetermined interview guide (Supplementary online file: Appendix I) that was developed in consultation with patient partners with BPBI aged 18–28 years. The interview guide focused on the mental health experiences of youth with BPBI, as well as barriers and facilitators to mental health support within the current practice model. The interviews were audio-recorded, auto-transcribed in MSTeams, and the exported transcripts were converted to MSWord documents, verified for accuracy and edited by the researchers.
Thematic analysis of the transcribed interviews was conducted procedurally using Braun & Clarke’s (2006) six steps as an outline. 16 Our analytical approach was grounded in our social constructionist perspective that recognizes that meanings are co-constructed by the parties involved, setting, and contextual processes. 17 The researchers repeatedly read the entire data set, taking preliminary notes on emerging codes, and reported new insights and patterns in the transcribed data from the interviews. 18 Deductive codes were generated from the interview guide, while inductive codes emerged from reflexive analysis through individual (HP, CN) and collective processes via journaling and dialogue respectively. 19 Informed by our BPBI clinic practice viewpoint, definitions of mental well-being and health, 10 and constructivist interpretive process, meanings were generated from the narratives of the youth and parents. Common ideas were established and categorized into main themes. 20 Thematic analysis was conducted through iterative discussions between the researchers and senior author (HP, CN & ESH). Aligning with the substantive approach to the qualitative research process, we formed a coherent and logical plan from design to dissemination that has congruency in our inquiry, methods, and analysis. 21 An audit trail was used to ensure analytic transparency. Depth was achieved by evaluating the context of data from various viewpoints, as well as branching out to reflect a wider scope of social context. 22
Results
Participant demographics and pseudonyms.
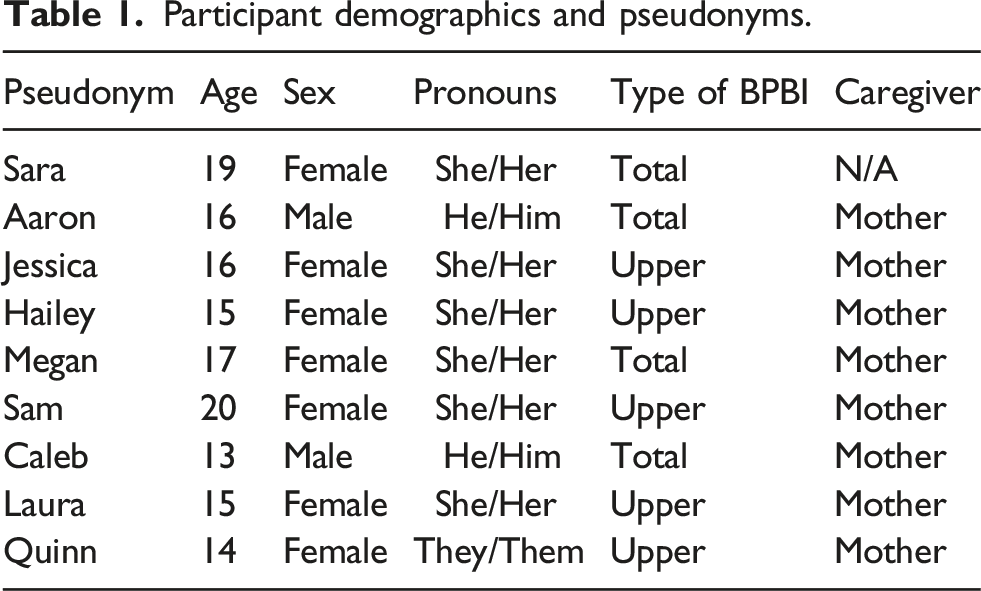
There were three major themes in these data: (i) physical disability identity and mental health; (ii) pursuit of “normal” body image; and (iii) paradox of advocacy. Several actionable practice recommendations were also expressed. These themes and practice recommendations are discussed below alongside quotes that are denoted with pseudonyms (Table 1).
Physical disability identity and mental health
The disability identity of the youth interviewed were centred around the physical aspects of their arm and hand including pain, function, appearance, and sensation. The activities that these youth chose to participate in, or were unable to do, had a significant effect on how they view themselves and their mental health. The focus of their narratives was on the physical manifestations of their limb impairment; however, social and emotional concerns were interwoven into their accounts.
Megan (17 years, she/her) spoke of her desire to play hockey. Coming from a “hockey family,” she watched everyone around her play hockey, and her motivation to play this sport was strong. However, the lack of intrinsic muscle function in her hand did not allow her to hold onto the hockey stick, and she felt that “there wasn’t really a way for me to do it.” She shares: “That was probably the main thing that was really frustrating. Because that was the sport that I really, really wanted to play, but I just couldn't play it. And so that was sort of making me feel kind of bad about myself that there wasn't like a way that I could do it.”
The focus of Meghan’s experience was her physical performance and its negative affect on her ability to play hockey, but the emotional toil (i.e., frustration) and negative self-perception (i.e., feel bad about myself) warranted equal or greater attention.
Two families shared their concerns with participating in dance classes and performances. The focus of their accounts was about finding an activity that best aligned with the interests and physical abilities of the youth. Yet, concerns regarding perceived or actual negative social interactions infiltrated their thoughts. Jessica (16 years, she/her) made the decision not to continue with dance because of the visibility of her difference. “I did dance for a while too, but I didn't really like it 'cause you can totally see my arm. So, I just kinda chose stuff that my arm wasn’t the main focus and it wasn’t standing out.”
Similarly, Sam’s (20 years, she/her) mother wanted to avoid the possibility of Sam being singled out: “I wanted to put her in dance but I didn't 'cause she couldn't lift her arm high enough and I didn't want anybody making her feel bad.”
In this way, these participants illustrated that their physical ability played a large role in their choice of leisure pursuits; however, this intersected with concerns of social inclusion and unwanted attention related to the visibility of their BPBI.
In contrast to the other participants, Sara (19 years, she/her) was the only youth that readily disclosed her struggle with mental disorder. She felt a constant lack of motivation to do things. Her symptoms began in junior high and eventually led to the diagnosis of major depression. Yet, despite being aware of her mental health symptoms and having access to care (i.e., counselling, art therapy), she stated that she “just wasn’t seeking [help].” She revealed how the dual diagnosis of BPBI and depression made her feel: “I already saw myself like disabled in one front and okay, if I tell people that I think I might be depressed, they'll think I'm seeking attention.”
Although Sara’s narrative centred on her mental health, her experiences were akin to the others in that her physical diagnosis of BPBI influenced the expression and management of her mental health symptoms. She hesitated to seek mental health support because of her perceptions about her physical disability. In this way, the narratives of the youth’s disability identity illuminated an intersection of physical and mental health concerns.
Pursuit of “normal” body image
Among the youth interviewed, increased concerns and social pressures surrounding body image occurred in the adolescent years. The use of the word “normal” in the following text is based on societal perception of “normal” appearance, and intentionally chosen to reflect the language used by some of the participants.
Youth spoke of an increased awareness of the perceived and actual attention that their visual difference brought upon them. To avoid this unwanted attention, Laura (15 years, she/her) tried to conceal her difference:
“It just made me very self-conscious about it all the time. And that’s why, you know, I used to hold the back loop of my pants with my right arm so I could hide the fact that it was so bent out weird. I could just keep it hidden away.”
Similarly, Jessica’s (16 years, she/her) strategy of avoidance was to be the photographer rather than be photographed: “I’d rather take pictures of people instead of being in pictures ‘cause you can see my arm. So, if we are taking pictures, I always find a way to hide my arm so you can’t really see it.”
Others, including Caleb (13 years, he/him) expressed that the unwanted attention took an emotional toll on them, “I feel kind of sad ‘cause everybody stares at my hand weirdly, ‘cause my hand is smaller than my right hand. And it also looks different, and it makes me feel sad.”
Jessica (16 years, she/her) and Megan (17 years, she/her) were able to articulate how their concerns with the visibility of BPBI arose in adolescence and associated this with the desire to belong. Jessica shared:
“I think it was like age ‘cause like as I grew up, you know, like people are getting older and they’re like worrying about their looks and stuff.”
The importance of appearance, fashion, and fitting in emerged with age. In the following narrative, Megan illustrated how she chose hairstyles and clothing to accommodate for her physical limitations when she was younger; however, she got tired of these adaptations as she got older because of the desire to be like everyone else: “As I started to get older and more aware of the way that other people were living their lives and doing things. For a good while when I was little [I saw that] other kids wear jeans. I didn't think anything of it, and I would just stick with pants that didn't require like buttons or zippers or anything. And then as I got older, and I was more into actually having a nice outfit that I was excited to wear, I don’t want to have to panic because I have to go to the bathroom, but I can't undo or button back up my zipper.”
This illustrates how the shift to adolescence resulted in increased frustration with physical adaptations as belonginess took precedence. Megan recognized how this negatively affected her mental health: “...when I realize like ‘oh my clothes don’t fit like the same that another person’s clothes would fit’, then it started to kind of like negatively impact me.”
Megan also expressed struggles with self-acceptance as she shared her feelings about pursing reconstructive surgery. Despite the functional gains of the procedure, she felt that:
“...I was actually just altering my body because I didn't like how it looked. At 15-16, I was making drastic changes to my body. It wasn't like I was doing anything illegal. I wasn't getting lip fillers or something like that. But it was a medical modification to my body because I didn't like how I looked. I think that was definitely a big hit on my mental health. For a while, I definitely would take my cast off, and just stare at my arm in the mirror and it was a very surreal experience because, oh, that's so weird that it looks somewhat normal now.”
Accepting one’s body image and physical difference was important to the mental health of these youth. Their journey of self-acceptance was intertwined with societal messages around ‘normal’ body image.
The paradox of advocacy
The physical impairments resulting from a BPBI affect how youth perform a task, but do not necessarily limit them from pursing or engaging in activities. Voicing their needs to influential parties was critical in facilitating experiences of inclusion and equity. In their interviews, youth and their parents expressed that the necessity for a high-level of advocacy affected their mental health. Laura’s (15 years, she/her) mother expressed: “Through my mental or Laura’s disability journey, I’ve learned that you have to be the crazy one to get attention sometimes. I don’t like playing that role, but I'll do it because that seems to be what gets the results, unfortunately.”
Laura and her mom felt systems-level frustrations related to seeking accommodations at school. Requests were assignment-specific and dependent on individual teachers. Laura shared her struggles with one teacher and how she pushed through shoulder pain to get her art project completed: “I've had this teacher before, she is very much a problem when it comes to understanding my shoulder. So, she didn't get why I needed an extension on the clay and she said 'no.' Whatever, I got it done. But it was just … it was more painful than it had to be.”
Stress of not having their needs met, being misunderstood by others, or being pitied were also expressed by other youth as outcomes of advocacy. Aaron (16 years, he/him) shared: “I don’t want people to help me because of my arm I want people to help me just because of me.”
Other youth described how they internalized the stress of advocacy. Some expressed not wanting to ask for help as a result of feelings of guilt, invalidation, and embarrassment. Quinn’s (14 years, they/them) mother speaks of her child’s struggles with seeking help in gym class: “If they're in gym class with their peer group, quite often they’ll try their best to ignore [the pain in their arm] until it's maybe too painful that they can’t, just because they don't want people to give them a hard time.”
When struggling and needing to ask for help, Sara (19 years, she/her) bargained in her head and worked through potential judgement from others: “It's also the fact that my disability isn’t that bad. Yeah, I can’t do certain things. But there’s people … I know that I shouldn’t compare my disability to other people’s disabilities, but it’s hard to when you’re told that you should feel happy that you're born with an arm. And it's just like, “Well, least you got an arm. Some people don’t.” Oh, alright, I guess.”
Even with the identified personal, societal, and systems-level barriers, it was felt that youth and their families were expected to continuously advocate for their needs to obtain the support and understanding of peers, teachers, and coaches. Often, advocacy resulted in emotionally and mentally draining outcomes. In this way, narratives about advocacy were paradoxical. Advocacy led to youth support and inclusion; however, advocacy was a process that was associated with complex feelings and emotions that caused internal strain on parents, youth, and their families.
Actionable practice recommendations
Mental health practice recommendations.
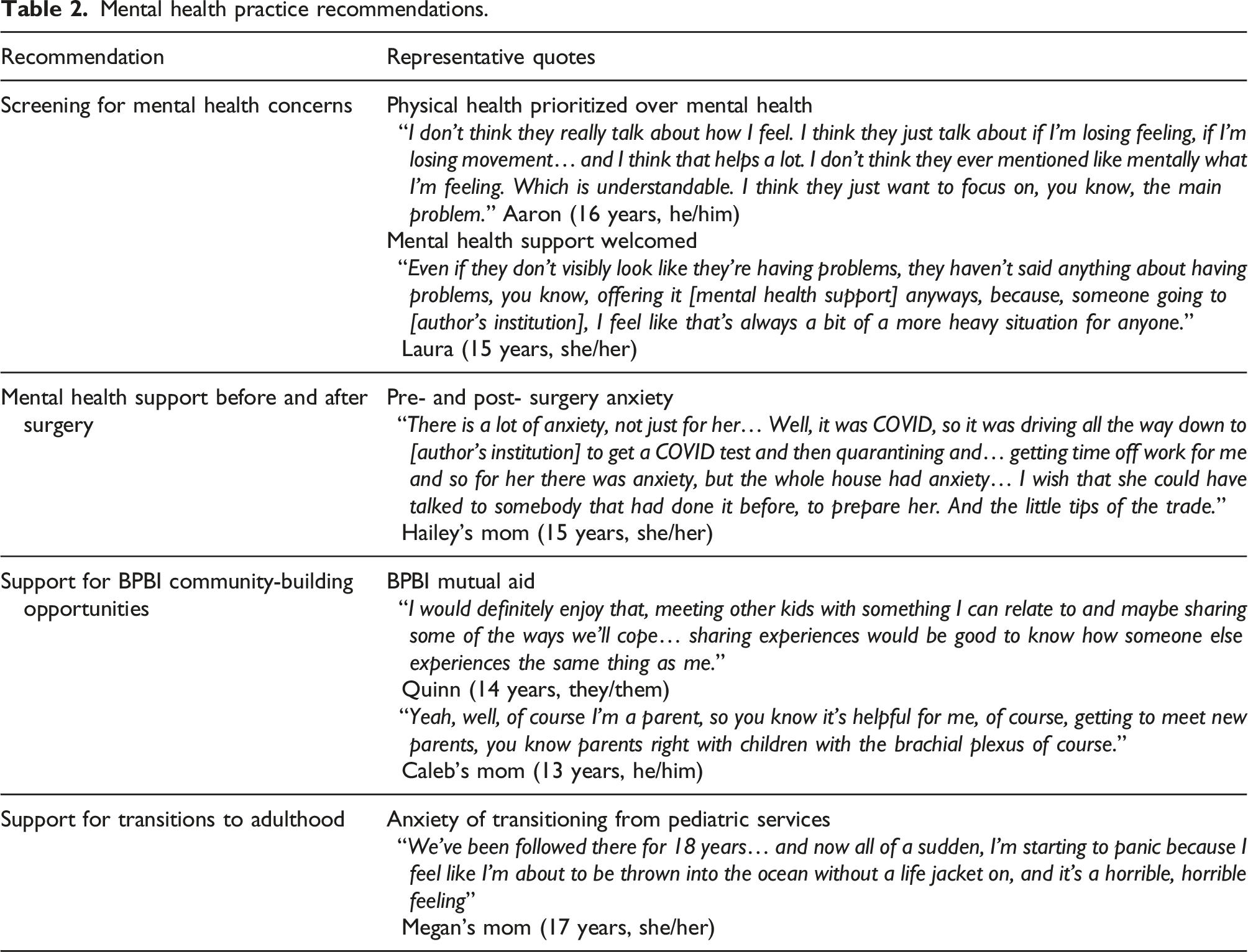
Among those interviewed, it was expressed that it may be helpful to screen for and to talk about mental health concerns in the BPBI clinic. Both youth and parents expressed that mental health was not asked about during standard appointments at their BPBI clinic visit. Accordingly, physical health was the priority at clinic visits; therefore, families also expressed that they did not have an expectation that mental health would be screened. One specific practice area recommended for improvements in the future was mental health support surrounding anxiety related to the surgery process. Other recommendations made by youth and parents related to surgical counselling were: education about preparing for wound care, suggestions about clothing needed to accommodate for the post-operative cast, feelings around explaining or not explaining surgery to peers, and the stress of change in routine post-surgery. Practical suggestions made by participants included opportunities to share practical tips between youth and families within the clinic setting, offering additional support during the decision-making process and mental health check-ins post-surgery.
Lastly, several families expressed the need for more community-building opportunities like the Family Day mutual aid events, 12 or additional advertisements about these events. Support for older youth transitioning into adult services and out of the paediatric healthcare system was also expressed. Barriers were identified associated with this ‘ageing out’ process which may represent an important window for additional mental health support, as well as ongoing research.
Discussion
In examining the mental health experiences of youth with BPBI and their caregivers, this study aimed to identify barriers and facilitators of mental health care for these families in an outpatient BPBI clinic practice context. The findings from this study found that youth mental health experiences were expressed through intersections with their physical disability identity. Their physical concerns were encumbered with social, emotional, and psychological stressors. Isolated mental health concerns were not readily expressed. In the BPBI clinic, youth and families did not find that mental health was well supported; however, they also felt that this was not expected to be a primary concern within this health delivery context. In reflecting on their experiences, additional support for mental health by means of fostering BPBI community support, preparation and education around surgical procedures, and support for transitioning to medical care beyond the paediatric setting are recommended.
The finding that youth mental health was not separated from physical health aligns with the World Health Organization’s definition of mental health: “A state of mental well-being that enables people to cope with the stresses of life, to realize their abilities, to learn well and work well, and to contribute to their communities”. 23 That is, mental health involves the youth’s own evaluation of the quality and purpose of their life. 24 Such an evaluation involves cognitive and affective processes and is influenced by social relationships.24,25 Mental health concerns existed for these youth regardless of whether they had a mental disorder. This is important, as youth, caregivers, and clinicians may miss the opportunity to promote and foster mental health if they focus solely on mental disorders. This may happen if mental health is compartmentalized rather than seen as integral to the youth’s overall well-being and health.
This research supports the findings of previous studies that youth with BPBI experience poorer HRQoL associated with mental health as well as participation restrictions.3,9,26 Further, this study extends previous research in identifying that not only is participation reduced, but that this had direct negative effects on the mental health of these youth. Using mixed methods, previous studies have shown that these youth have appearance-related and body image concerns and socio-emotional health risks.27,28 Using an interpretative approach, this study is unique in prioritizing the voices of youth and parents by consolidating and contextualizing their perspectives on mental health support in the BPBI clinic practice context.
Using an interpretive qualitative approach is a primary strength of this research in elucidating the mental health experiences of youth with BPBI and their caregivers. A limitation of this study involves the sample selection. The participant pool was limited to those with access to the BPBI program at a large urban pediatric hospital. This may be restricted to those with severe BPBI and those with more financial, time, and educational means. Further, in prioritizing participants who were able to provide rich accounts of their experiences, the sample may be more representative of families with higher educational levels. Therefore, the results of this study provide insight into mental health care for youth with BPBI; however, are not transferable to all BPBI clinics. A few limitations also arose from the virtual interview format, including technical issues, lack of nonverbal cues, and interruptions from family members, which may have affected what the participant chose to share.
This study illuminated immediate and actionable practice recommendations for the SickKids BPBI clinic that may be informative for other BPBI programs. Importantly, mental health concerns in youth with BPBI may not be readily disclosed. Acknowledging the socio-emotional aspects of living with the physical consequences of a BPBI and screening for mental health concerns are ways to introduce mental health care into standard appointments. Targeted program development in transitional care to adult health services, staffing of a mental health clinician within the clinic, and opportunities for youth and parent-peer connections are important considerations. If the well-being of youth with BPBI is a result of the intersection between their physical and mental health, then, should we not have trained specialists in both physical and mental health to support youth with BPBI in our clinics? Overall, the findings of this study support the need for further research on optimizing mental health resources within physical health settings to better support the holistic needs of these youth and their families.
Supplemental Material
Supplemental Material - Intersection of physical and mental health of youth with brachial plexus birth injuries: A qualitative study
Supplemental Material for Intersection of physical and mental health of youth with brachial plexus birth injuries: A qualitative study by Halle Purther, Cora Nitert-Brown, Diba Vahidi Ferdosi and Emily S Ho in Hand Therapy
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by the University of Toronto Departments of Family and Community Medicine, Rehabilitation Sciences, and Psychiatry Cass Family Grants for Catalyzing Access and Change.
Ethical Approval
Ethical approval for this study was obtained from the Hospital for Sick Children REB# 1000075069 and the University of Toronto #41063.
Informed Consent
Informed consent was obtained from all participants for being included in the study. The authors of this study verify that the medical research was conducted according to the World Medical Association Declaration of Helsinki. The methods section met the relevant ethical consideration of the local institutional Research Ethics Board. Informed consent and assent (when applicable) were obtained from all participants prior to participating in this study.
Guarantor
ESH.
Contributorship
CRediT (Contributor Roles Taxonomy). HP: methodology, data collection and analysis, writing – original draft, reviewing and editing; CN: methodology, data collection and analysis, writing – original draft, reviewing and editing; DVF: proposal writing, recruitment, consent, data collection, writing – review and editing; ESH: project administration, conceptualization, methodology, resources, supervision, writing original draft, review and editing.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.