
Abstract
Introduction
Research investigating psychometric properties of multi-joint upper body strength assessment tools for older adults is limited. This study aimed to assess the test–retest reliability and concurrent validity of novel clinical strength measures assessing functional concentric and eccentric pushing activities compared to other more traditional upper limb strength measures.
Methods
Seventeen participants (6 males and 11 females; 71 ± 10 years) were tested two days apart, performing three maximal repetitions of the novel measurements: vertical push-off test and dynamometer-controlled concentric and eccentric single-arm press. Three maximal repetitions of hand-grip dynamometry and isometric hand-held dynamometry for shoulder flexion, shoulder abduction and elbow extension were also collected.
Results
For all measures, strong test–retest reliability was shown (all ICC > 0.90, p < 0.001), root-mean-squared coefficient of variation percentage: 5–13.6%; standard error of mean: 0.17–1.15 Kg; and minimal detectable change (90%): 2.1–9.9. There were good to high significant correlations between the novel and traditional strength measures (all r > 0.8, p < 0.001).
Discussion
The push-off test and dynamometer-controlled concentric and eccentric single-arm press are reliable and valid strength measures feasible for testing multi-joint functional upper limb strength assessment in older adults. Higher precision error compared to traditional uni-planar measures warrants caution when completing comparative clinical assessments over time.
Introduction
The ability to weight-bear through the upper limb is integral for activities of daily living (ADL), such as pushing oneself up from a chair or toilet, pushing open a door or moving objects and utilising a walker, cane or handrail.1–4 In addition, the upper limb can play a role in balance preservation and fall injury reduction by diminishing the impact of a forward fall.5,6
Assessment of upper extremity (UE) strength and force production has traditionally been completed through the use of hand-held dynamometry (HHD), single axis isokinetic dynamometry and hand-grip (HG) assessments.7,8 The psychometric properties of these traditional measurement tools in assessing the strength of the upper limb in older adults has been reported in previous studies.8–11 The disadvantages of these strength measures are that they are isometric tests and/or focus on an isolated single joint muscle contraction, which may not be reflective of UE functional movements such as the pushing and weight-bearing activities important to maintain functional independence. Functional multi-joint ADL movements, such as UE pushing and pulling, have not been captured via these single axis strength tests or gripping strength assessment methods.
Isokinetic dynamometry can provide a detailed strength profile with the ability to assess an individual’s isometric, concentric (CON) and eccentric (ECC) strength components. However, similar to the traditional strength measures, isokinetic dynamometry is limited to single isolated joint movements. Measuring multiple single axis strength tests to achieve a thorough strength profile is tiring, time consuming and costly, particularly for an older adult population. Additionally, functional multi-joint ADL movements, such as UE pushing and pulling are not captured via these single joint assessment methods. One option to address the assessment of multi-joint UE functional pushing and pulling movements is a newly available cable and wheel attachment for the Humac NORM isokinetic dynamometer (CSMi, Stoughton, MA) (Figure 1(a)). Functional multi-joint ADL movements, such as UE pushing and pulling, are possible with the cable wheel attachment. Only one previous study has reported reliability of push–pull closed chain isokinetic assessment of the UE where high same day reliability in peak force and average power was determined in a healthy, young population but ECC strength was not measured. 12 Research investigating the application of functional multi-joint isokinetic UE strength testing in older adults is lacking, despite the important functional relevance for this population.
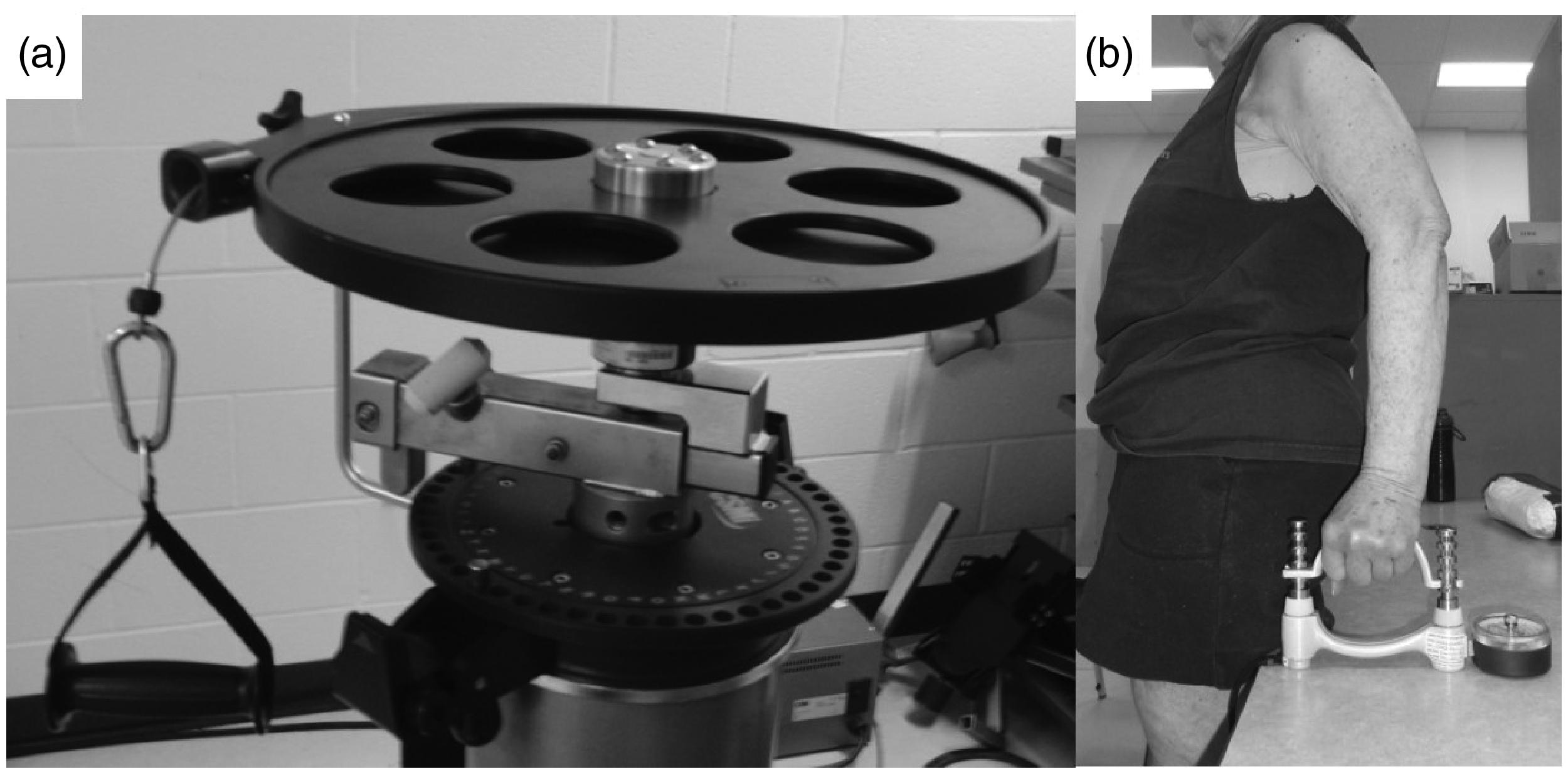
The Humac NORM Wheel attachment (a, CSMi, Stoughton, MA) and the push-off test set-up (b).
The challenge of utilising isokinetic dynamometry is the cost and inconvenience of testing in a laboratory or clinic. In contrast, the push-off test (POT), a relatively new test developed to assess unilateral weight-bearing capacity, is performed with a hand-held dynamometer (Figure 1(b)). 3 This is proposed as a practical measure of functional weight-bearing ability applicable to an older adult population. The multi-joint strength assessment set-up is representative of UE functional actions of ADLs, such as pushing oneself up from a chair. The POT is a simple and feasible strength assessment that could be readily incorporated into clinical practice for assessing older adults. The reliability of the POT has been established in a symptomatic rehabilitation population, but not yet in a non-symptomatic population or an older adult population.3,4 The validity of the POT in comparison to commonly utilised strength assessments has yet to be investigated.
The proposed novel measures of functional multi-joint isokinetic dynamometry and the POT may provide practitioners with alternative strength measures of the upper limb that capture important functional multi-joint weight-bearing and pushing activities in older adults. The purpose of this study was to assess the test–retest reliability and concurrent validity of the POT and functional multi-joint isokinetic dynamometer (CON and ECC strength) in older adults as compared to the more traditional measures of HHD and HG. The hypotheses were:
The novel multi-joint upper limb strength measures (POT, CON and ECC) have high test–retest reliability similar to the more traditional strength measures, The novel multi-joint strength measures have concurrent validity showing moderate to high associations with each other and to the traditional measures.
Methods
A repeated measures design with two separate testing sessions 48 h apart was conducted on older adults over the age of 60 years to investigate the reliability and validity of UE strength measures.
Participants
A convenience sample of 20 participants over the age of 60 years was recruited from the local community via posters and a posting on the University intranet noticeboard. All participants were informed of the experimental risks (muscle and joint soreness and other potential cardiovascular risks related to strenuous exercise) and provided signed informed consent. To ensure testing safety, participants were excluded if they had any recent upper body (hand, wrist, shoulder, trunk, neck) injury or painful joint problem that limited day to day activities or results in pain on a daily basis, prior distal radius fracture in the past two years, or multiple fractures of the wrist or forearm, any history of UE neurological problems (i.e. Stroke, multiple sclerosis, Parkinson’s disease, reflex neuropathy) or any other conditions where they were advised not to participate in balance and strengthening exercise and those who were unable to safely ambulate independently (with or without a walking aid) in the community.The study was approved by the University of Saskatchewan Biomedical Ethics Review Board.
Procedure
Participants visited the testing site at the same time of day on two separate occasions 48 h apart. Participants performed: (1) upper limb functional tests (HG, HHD and POT) and (2) the isokinetic dynamometry testing (CON and ECC). The testing order (starting with 1 or 2) was alternated between participants and the same order was maintained on the second day. This process was chosen to ensure all participants did not experience the same order of testing which may influence fatigue and/or a learning effect. On Day 1, height and weight were collected using a standard protocol. Participants also completed a Medical Demographics Questionnaire, the Physical Activity Scale for the Elderly, 13 the Mini Falls Risk for Older People in the Community screen (FROP-Com) 14 and the Waterloo Handedness Questionnaire. 15 Testers were the same on both Days 1 and 2, were blinded to other measurements and measurements from the previous test and trained and practised the protocol prior to testing. Two trained physical therapy students performed the POT and all of the traditional tests (1: POT and HG, 2: HHD) and one of the authors (HSL) performed all of the isokinetic dynamometer testing. For all tests, participants were given one familiarisation trial prior to performing three maximal efforts, alternating between hands and separated by one-minute rest. The two arms were tested in random order for Day 1. This order was maintained for the second session. For all tests, the same motivational cues and motivational tone were used such as ‘push, push, push and relax’.
Upper limb functional tests
HG (Figure 2) was assessed using a calibrated HG dynamometer (Model #5030J1, JAMAR, DMM Canada) with the handle positioned in the second notch for all participants. The participant was seated in a chair, back supported, feet flat on the floor with the elbow at 90°, wrist in neutral and the shoulder adducted to the body. 16 Participants received the same instruction and motivational cues, resulting in a hold of approximately five seconds.

The traditional strength measurements utilised. L–R: hand-grip (HG), hand-held dynamometry (HHD) elbow extension (EE), HHD shoulder flexion (SF) and HHD shoulder abduction (SA). The arrow denotes the direction of effort from the participant.
The same HG dynamometer was utilised for the POT protocol. Following the protocol outlined by Vincent et al., 3 the dynamometer handle was reversed and locked in the second notch. Participants stood with their buttocks against a standard table. 3 With the shoulder joint adducted to the body, whilst gripping the dynamometer, the participant’s arm was standardised to the ranges previously outlined: 10–40° of elbow flexion and 10–40° of shoulder extension. 3 Joint positions were verified with a goniometer. If needed, the participant stood on high-density rubber mats to adjust their height and achieve the desired joint range. The tester held the dynamometer in place during each trial to aid stabilisation and to prevent the dynamometer from moving. Participants were instructed to initiate the trial by lightly pressing and gradually increasing until they had applied maximal force. In addition, participants were told to avoid leaning whilst maintaining a neutral trunk, to maintain full foot contact and to not unload or sit on the table. If participants failed to meet these criteria, as deemed by the assessor through visual inspection, the trial was repeated.
Participant descriptives.
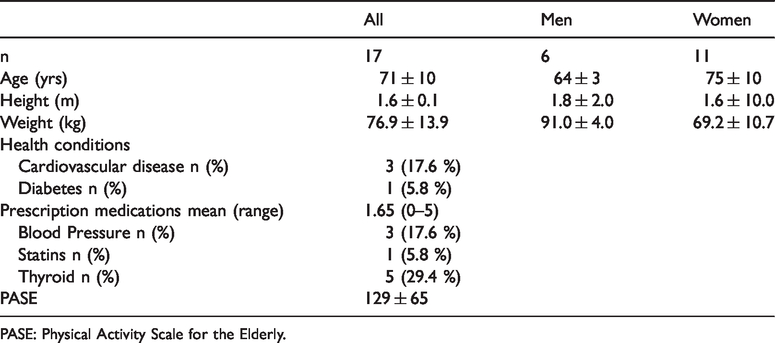
PASE: Physical Activity Scale for the Elderly.
A hand-held dynamometer (Model #01165, Lafayette Instrument Inc., Lafayette, Indiana) was used to test the strength of the arm muscles using a standard protocol (Figure 2) with a five second hold make test. 17 The positions tested consisted of shoulder flexion (SF), shoulder abduction (SA) and elbow extension (EE). 18 The participants were positioned supine on a standard plinth for all HHD tests. For SA, the shoulder was abducted to 45° with the elbow fully extended. The dynamometer was placed on the lateral surface of the upper arm, proximal to the elbow joint whilst the tester provided stabilisation by placing their hand on the superior aspect of the ipsilateral shoulder. During SF, the shoulder was flexed to 90° with 90° of horizontal adduction. The forearm was neutrally rotated with the palm facing medially. The dynamometer was placed proximal to the elbow joint on the anterior border of the UE whilst the tester provided support at the lateral border of the scapula. Finally, for EE, the participant was positioned with their upper arm adducted to the body their elbow flexed to 90° with a small towel roll underneath the arm to ensure stabilisation of the upper arm. The participant’s forearm was neutrally rotated with the palm facing medially and the dynamometer was placed on the lateral border and proximal to the styloid process of the ulna. The tester provided support at the distal end of the biceps muscle near the elbow joint.
Functional isokinetic dynamometry
Maximal voluntary strength measures from CON pushing and ECC resisting trials were obtained using an isokinetic dynamometer with a custom linear motion dynamometer attachment (Wheel attachment, Humac NORM Isokinetic Dynamometer, CSMi, Stoughton, MA). The participant was secured in the dynamometer chair with stabilising lap and vertical shoulder straps. Prior to three maximal efforts, participants performed two submaximal repetitions for each contraction mode as an initial familiarisation with the isokinetic exercise and as a specific warm-up.
For the CON contractions, the participants started with their shoulder abducted to 45° and elbow flexed at 120°. Participants were instructed to ‘punch out’ until the elbow was extended. During the ECC contractions, the participants initiated the movement with a partially extended arm with 60° elbow flexion and resisted the cable movement to an elbow angle of 120°. Participants were instructed to ‘resist as hard as you can whilst the cable pulls you back’. For both contraction protocols, the linear cable speed was set constant at 17 mm/s for the full movement. Prior to familiarisation repetitions, all joint positions were confirmed with the use of a goniometer. Data were obtained successively in the CON contraction mode, followed by the ECC contraction mode in the same arm before swapping arms. Each repetition was separated by a rest period of one minute.
Data analysis
The data were separated between dominant and non-dominant limbs for all analyses. A mean and standard deviation (SD) of the three maximal efforts for the HG, HHD and POT were used for analysis. For the CON and ECC, the mean peak values of the three trials were utilised for analysis. To establish test–retest relative reliability, two-way mixed with absolute agreement intraclass correlation coefficient (ICC) analyses were used. ICC values to define the strength of reliability were based on ranges of poor (<0.69), fair (0.70–0.79), good (0.80–0.89) and high (0.90–1.00).
19
The absolute reliability was assessed by calculating the Standard Error of Mean (SEM) for each test. SEM was calculated utilising the SD of the difference between session one and two divided by the square root of the sample size. The minimal detectable change (MDC) at the 90% confidence interval was calculated using
A strength composite score was established for each strength measure by summing the mean values of the dominant and non-dominant sides. Pearson’s product moment correlation coefficients were utilised to assess concurrent validity between the novel and traditional strength measures. To confirm validity, the following cut-offs were utilised; high: >0.70, moderate: 0.50–0.69, low: 0.25–0.49 and negligible correlation: 0–0.24. 22 The level of significance was set at p < 0.05. All statistical analyses were performed with SPSS software (Version 25, SPSS Inc, Chicago, USA).
Results
Seventeen participants (6 men, 11 women, Table 1) completed the full testing protocol (Figure 3). Twelve participants reported no history of falls, four participants reported one fall and one participant reported having two falls in the last 12 months, defined as anybody part unintentionally coming to rest on the floor or with a lower surface that was not a result of fainting. 23 For falls risk, measured via the FROP-Com, the range was 0–2, indicating a low level of risk for all participants. One participant utilised a roller walker on a daily basis to ambulate in the community.
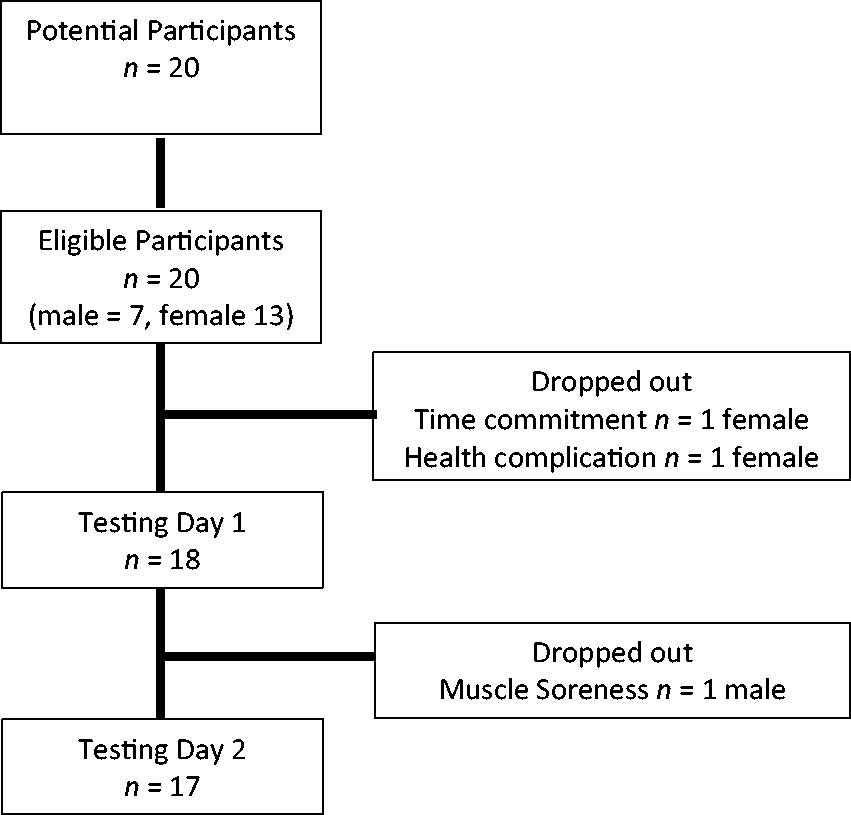
Flow of participant progress throughout the study.
Table 2 presents the mean peak ± SD, ICC, SEM, CV%RMS, MDC and differences between sessions one and two for the novel (POT, CON and ECC) and traditional strength measures (HHD and HG) collected during the two testing sessions. ICC analyses showed high test–retest reliability between the two data collection days (all ICC > 0.9, p < 0.001). Absolute reliability reported via precision errors for all strength measures were between CV%RMS: 5.5–13.6%; SEM: 0.17–1.15; and MDC90: 2.1–9.9%. Pearson’s correlation coefficient (Table 3) identified the novel strength measures had significantly high positive correlations to each other (r > 0.90, p < 0.001) and to the traditional measures (r > 0.83, p < 0.001).
Differences between sessions one and two for the novel and traditional strength measures.
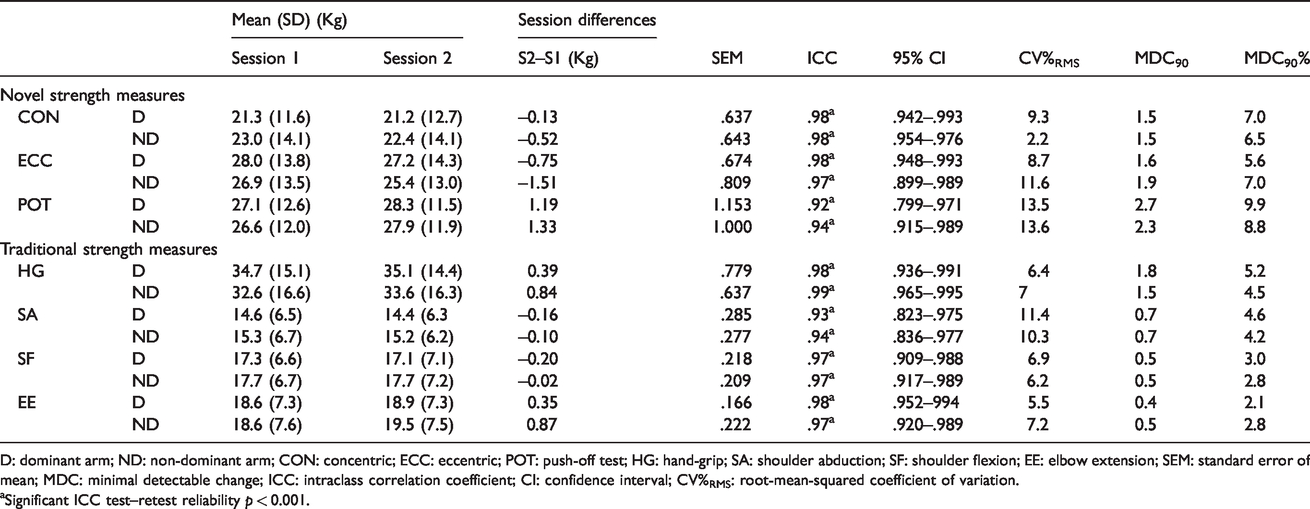
D: dominant arm; ND: non-dominant arm; CON: concentric; ECC: eccentric; POT: push-off test; HG: hand-grip; SA: shoulder abduction; SF: shoulder flexion; EE: elbow extension; SEM: standard error of mean; MDC: minimal detectable change; ICC: intraclass correlation coefficient; CI: confidence interval; CV%RMS: root-mean-squared coefficient of variation.
aSignificant ICC test–retest reliability p < 0.001.
Correlation values of strength composite of D and ND arms for the novel and traditional strength measures.
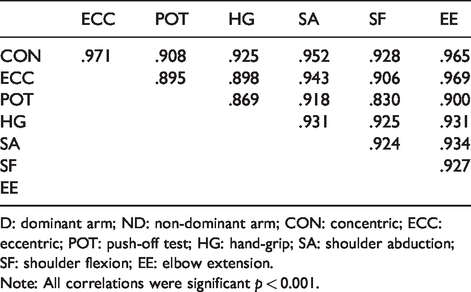
D: dominant arm; ND: non-dominant arm; CON: concentric; ECC: eccentric; POT: push-off test; HG: hand-grip; SA: shoulder abduction; SF: shoulder flexion; EE: elbow extension.
Note: All correlations were significant p < 0.001.
Discussion
The purpose of this study was to assess the test–retest reliability and concurrent validity of novel functional multi-joint upper limb strength measures (POT, CON and ECC) in older adults. The results of this study support the principle hypothesis, demonstrating high test–retest reliability in both the novel multi-joint strength measures and the traditional strength measures. The findings also support the secondary hypothesis in this study, demonstrating concurrent validity of the novel strength measures to each other and to the traditional strength measures.
The current findings add new knowledge of strong psychometric properties of the POT in older adults, similar to previous findings in a younger healthy population and a patient population.3,4 The comparable and high test–retest reliability and concurrent validity found in this study supports the clinical use of the POT as a tool to assess UE multi-joint weight-bearing function in older adults.
For the novel multi-joint isokinetic dynamometry tests (CON and ECC), the high intra-tester reliability values were similar to those reported in a comparable study utilising a push–pull linear attachment for CON measurement with an active young adult population. 12 This study adds to the literature by determining reliability for ECC measurements. In addition, absolute reliability (MDC and SEM) have not been previously reported with this protocol. This study provides some insight into true change that may occur between assessments in an older adult population. The current isokinetic dynamometer set-up can provide a reliable and detailed strength profile assessing an individual’s CON and ECC strength capacity during a functional multi-joint UE movement that is representative of many ADL requirements (e.g. pushing oneself up from a chair or toilet, pushing open a door or moving objects, and utilising a walker, cane or handrail).1–4 Isokinetic dynamometry is an expensive and time-consuming undertaking, if isokinetic dynamometry is a viable option for the practitioner, the novel set-up (CON and ECC) allows for a single multi-joint strength testing protocol, as opposed to isolated single joint assessments, for an older adult during pushing and resisting UE movements. The wheel attachment utilised in this study could provide a broader range of testable movements, without the need for time-consuming equipment changes. The isokinetic dynamometer protocol investigated in this study provides insight to UE strength capacity during movements commonly seen during a forward fall arrest in older adults 5 and can provide clinicians with a wider understanding of UE CON and ECC strength capabilities in older adults.
Each of the traditional strength measures demonstrated high intra-rater reliability. The current findings for the traditional strength measures (HHD and HG) are in agreement with previous research,9,24 providing further evidence that HHD and HG are suitable and reliable tools for linear, isometric UE strength assessment in older adults.
For absolute reliability (MDC% and SEM) and precision error (CV%RMS), the traditional strength measures generally performed better than the novel strength measures. Holt et al. 25 had similar findings, with the HHD having superior absolute reliability compared to an isokinetic dynamometer set-up assessing internal and external rotators of the shoulder. The increased movement complexity of the novel measures compared to isometric traditional strength measures may account for the discrepancies in absolute reliability between the different strength measures. The higher precision error reported for the novel strength measures (POT, CON and ECC) should be considered when evaluating longitudinal changes during clinical assessment. Precision errors allow practitioners to identify meaningful change in repeat assessments or after interventions26,27 and should be utilised by practitioners to identify a threshold where change has occurred and is not due to measurement errors or participant variability.
The second study hypothesis was supported, demonstrating significant concurrent validity via high associations (correlation >0.7) between the novel POT, CON and ECC to each other and to the traditional measures of the HG and HHD. Due to the strong relationships with the traditional strength measurements, the novel strength measures may be a suitable assessment of multi-joint UE strength in adults over 60 years.
The novel measures provide a strength assessment that is representative of a push and resist upper limb movement (CON and ECC) and an individual’s ability to load through the entire upper limb isometrically in the POT.3,4 By utilising the same dynamometer that is commonly used for HG assessment, the additional implementation of the POT into a clinical setting is highly feasible.3,4 The validation of the new novel measures through this study provide practitioners with alternative strength measures of the upper limb that may be more representative of important weight-bearing functional movements important to maintain independence and potentially to reduce injury.
There are several limitations associated with this study. First, this study addressed intra-rater test–retest reliability; further investigations need to be conducted to establish the inter-rater reliability for the novel strength measures in an older population. In order to inform sample size calculations for future study, we conducted a post-hoc analysis, utilising a power of 80% and an alpha of 0.05, and determined a minimum sample size of 15 was sufficient to detect an ICC value of 0.6. 28 The population utilised in this study were generally healthy and active, 13 had a relatively low risk of falling and no history of UE pathology in the last two years. The purpose of this was to establish reliability and validity in a population not at a high risk of potential side effects or injury; future studies could expand the sample size to include older adult male and female comparisons across a range of functional abilities. In addition, currently there is a lack of normative data reported for the CON, ECC and POT multi-joint novel strength measures. Exploring normative values across a wide spectrum of ages would inform clinicians of typical performance capabilities for these strength assessments.
The new novel multi-joint dynamic upper limb push strength measures (POT, CON and ECC) are a reliable and valid assessment of older adults’ muscle strength and may provide insight into the profile of functional multi-joint strength important for ADL as compared to more traditional single joint isometric strength measurements (HHD and HG) currently utilised by clinicians. The POT is a simple and portable assessment of the upper limb’s multi-joint weight-bearing capacity. The POT set-up provides a strength assessment of the UE that is representative of UE functional actions of ADLs, such as pushing oneself up from a chair. It is a feasible tool for clinicians and health care providers to implement into their current practice and provides a tool to assess an older adult’s multi-joint functional strength capacity that is not currently addressed by the traditional measures (HHD and HG). The novel strength measures (CON, ECC and POT) used in this study may provide practitioners with alternative strength measures of the upper limb that capture important weight-bearing and functional pushing movements important to maintain independence and potentially reduce fall-related injury in an older population. The increased precision error present in the novel measures may be due to the complexity of the multi-joint movement pattern requiring greater control and warrants caution when completing comparative clinical assessments over time.
Footnotes
Acknowledgements
Thank you to Fabian Dale and Anthony J Miko for their contributions in data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of thisarticle: Internal research funding received from the 992 Major Project Fund, School of Rehabilitation Science, College of Medicine, University of Saskatchewan, Canada.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.
Ethical approval
The study was approved by the University of Saskatchewan Biomedical Ethics Review Board. Ethics number: Bio 17–30.
Guarantor
HSL is the guarantor for this article.
Contributorship
HSL, JLL and CMA were involved in analysis and interpretation of the data and preparation of the manuscript. HSL, JS, RD and SS completed data acquisition. All authors approved the manuscript and were involved in research design.