
Abstract
Introduction
Trapeziometacarpal osteoarthritis is associated with more pain and restrictions than other hand osteoarthritis due to the functional importance of the thumb. While the effectiveness of surgical and pharmacological interventions has been widely examined, there is a lack of specific evidence about conservative non-pharmacological trapeziometacarpal osteoarthritis therapies. The objective of this systematic review was to provide evidence-based knowledge on the effectiveness of physiotherapy and occupational therapy on pain, function and quality of life.
Methods
A literature search of Medline, CINAHL, PEDro, OTseeker, EMB Dare Cochrane Database of Systematic Reviews and Cochrane CENTRAL was performed. Randomized and quasi-randomized controlled trials and corresponding systematic reviews, observational studies, pragmatic studies and case–control studies were included. The risk of bias was assessed.
Results
Out of 218 studies, 27 were retained. A narrative summary and a series of meta-analyses were performed. Concerning pain reduction, the meta-analysis showed parity of pre-fabricated neoprene and custom-made thermoplastic splints: standardized mean difference (SMD) –0.01 (95%CI −0.43, 0.40) (p=0.95). Multimodal interventions are more effective on pain compared to single interventions: standardized mean difference −3.16 (95%CI −5.56, −0.75) (p = 0.01).
Discussion
Physical and occupational therapy-related interventions, especially multimodal interventions, seem to be effective to treat pain in patients with trapeziometacarpal osteoarthritis. Pre-fabricated neoprene splints and custom-made thermoplastic splints may reduce pain equally. Single interventions seem not to be effective. Significant evidence for effectiveness on function and quality of life could not be found.
Introduction
The ability to oppose the thumb is made possible primarily by the anatomy and biomechanics of the trapeziometacarpal joint. Its special anatomical shape allows a high degree of mobility, i.e. the freedom to move in all directions. But it may also favor instability which can facilitate osteoarthritis of this joint. 1 Depending on the selected diagnostic criterion (radiological or clinical), the prevalence rates of trapeziometacarpal osteoarthritis (TMC OA) may vary between 35.8% (radiological 2 ) to 15% in women and 7% (radiological 3 ) to 1.4%(clinical 4 ) in men. This quantitative discrepancy is explained by the fact that radiological findings do not necessarily correlate with clinical findings. 2 The clinical diagnosis-based prevalence may seem low but because of the important functional significance of the thumb, TMC OA causes, in addition to considerable pain, more significant restrictions in work and everyday life compared to osteoarthritis of other fingers. 5
The aetiology of TMC OA has yet to be confirmed, and the treatment strategy may be surgical or conservative. 6 This decision depends on the patient and their complaints. While the results of surgical procedures have been well studied, gaps remain in research regarding the effectiveness of conservative, occupational and physiotherapy treatment interventions in TMC OA patients.
As Davenport 7 stated, hand therapists use a range of treatment modalities whose efficacy and efficiency need to be examined. Many interventions are based on research evidence on osteoarthritis (OA) affecting other joints or on expert opinion, while evidence for treatment modalities of OA in the TMC joint is still lacking. Despite this lack of evidence, conservative treatment seems beneficial. Berggren et al. 8 observed a significant reduction in the number of patients requiring surgery after conservative treatment. O'Brien and Giveans 9 suggested that assessment and treatment by a non-surgical healthcare provider were associated with a decrease in the rate of surgical interventions, underscoring the importance of conservative hand therapy.
Several systematic reviews have examined conservative treatment modalities of hand OA, regardless of the specific joints.10–13 Two recent systematic reviews have examined specifically TMC OA.14,15 However, Spaans et al. 14 included pharmacological interventions and neither examined important physiotherapeutic interventions (e.g. exercise therapy) nor differentiated between different types of splints. Bertozzi et al. 15 did not focus solely on treatments for TMC OA but included, in addition, studies on treatment modalities for hand OA in general. 15 Further, both systematic reviews included only randomized controlled studies (RCT) and excluded all studies with another research design. Meanwhile, because of the specifics of research in rehabilitation, and to obtain a full picture of the problem, it may be appropriate to include also non-RCT studies in a systematic review. 16
Therefore, the aim was to conduct a systematic review and meta-analysis to explore the effectiveness of physical and occupational therapy-related interventions on pain, function and quality of life in patients with TMC OA.
Methods
A research protocol was developed and submitted for registration with PROSPERO (accepted on 30 November 2013; registration number CRD42013006282). All protocol revisions were accepted.
Search terms.
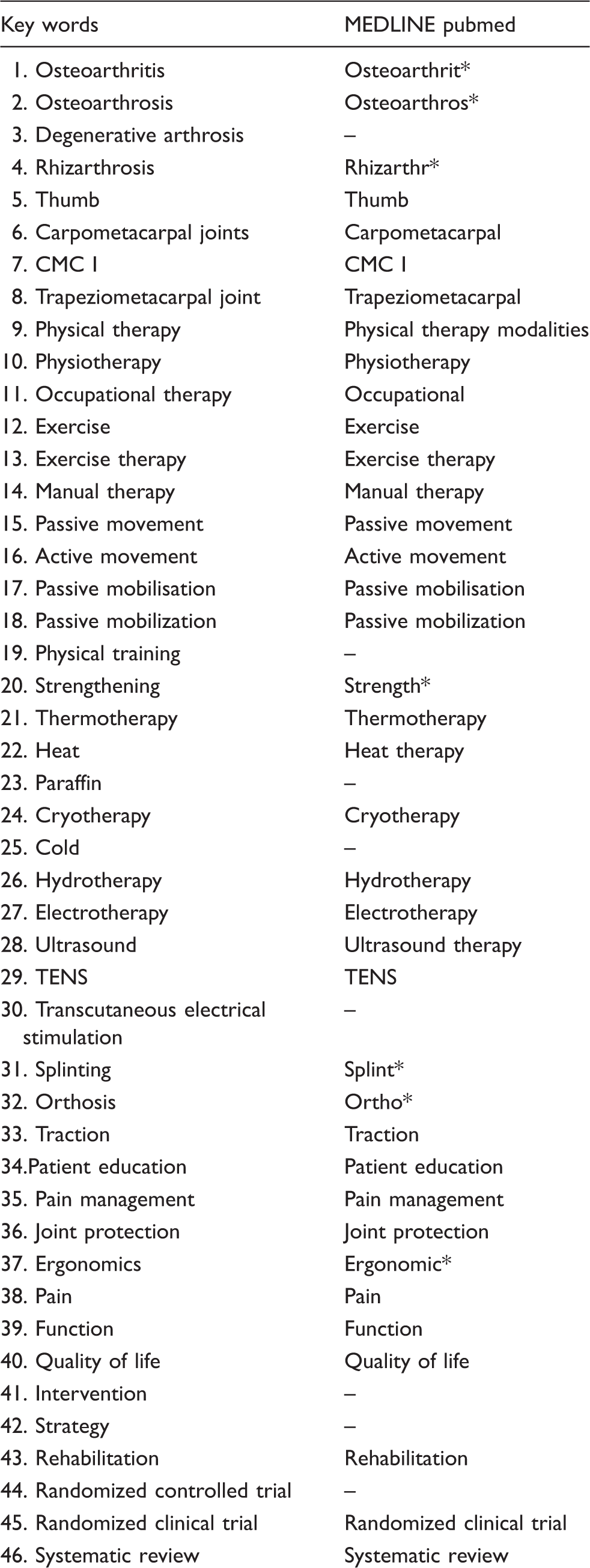
After removing duplicates, two reviewers (BA and SE) independently screened titles and abstracts for studies which did not meet inclusion criteria. Subsequently, the two reviewers extracted all data from the included studies onto a standardized, pre-defined data form. Risk of bias was assessed independently by the same two reviewers by means of the pre-defined RevMan criteria (Review Manager 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014).This risk of bias assessment tool can be used for both RCTs and non-RCTs (Cochrane Handbook for Systematic Reviews of Interventions 13.5.2.3). Any disagreement was resolved through discussion.
As a first step, a narrative review was carried out. For each study, we assigned symbols (+ = positive effect/− = no positive effect) for the outcome of an intervention as reported in the authors' conclusions. Where different time points were available, we chose the outcome closest to the end of the intervention. Then, in an attempt to quantify objectively the narrative summary, different meta-analyses were conducted. For the studies included in the meta-analyses, effect sizes have been calculated. These meta-analyses were computed only when the key elements were comparable (population, intervention and outcome). For pragmatic reasons, a certain amount of heterogeneity and risk of bias were accepted. The standardized mean difference (SMD) to express individual studies' effect sizes and a random effects model were chosen a priori. Hedge's g was used to correct for possible small sample bias. It is implemented in RevMan 5.3 algorithms. Weights of the individual studies were based on the inverse variance method. RevMan 5 in the non-Cochrane Mode was used for the calculations. Cohen's d benchmarking was used to allow a clinical interpretation of the observed overall weighted mean effect sizes. 17
Results
Two hundred and eighteen studies were found initially and assessed for eligibility. After removing duplicates, 93 studies remained. After screening of titles and abstracts, 38 studies were excluded. Reasons for exclusion were studies being related to drugs, surgery, non-clinical study, other condition and other language. The full texts of the remaining 55 studies were read leading to the exclusion of another 28 studies (for reasons of other language, surgery and drugs). Twenty-seven studies totaling 1179 patients could be included for analysis: 10 RCTs with sham intervention or usual care for the control group, seven parallel group studies without control group, five cross-sectional design studies, three observational studies and two retrospective studies (Figure 1). The outcome time frame presents a very wide range, from 1 week to 7 years, for most studies from 2 weeks to 3 or 4 months. Risk of bias was assessed for seven criteria (online supplementary tables 2 and 3). All studies presented at least one high or unclear risk of performance bias (blinding of participants and personnel). Furthermore, 11 studies had a high risk in two or more out of seven criteria. Only eight studies had no high risk of bias, despite presenting at least two unclear risk assessments."]
Flow chart.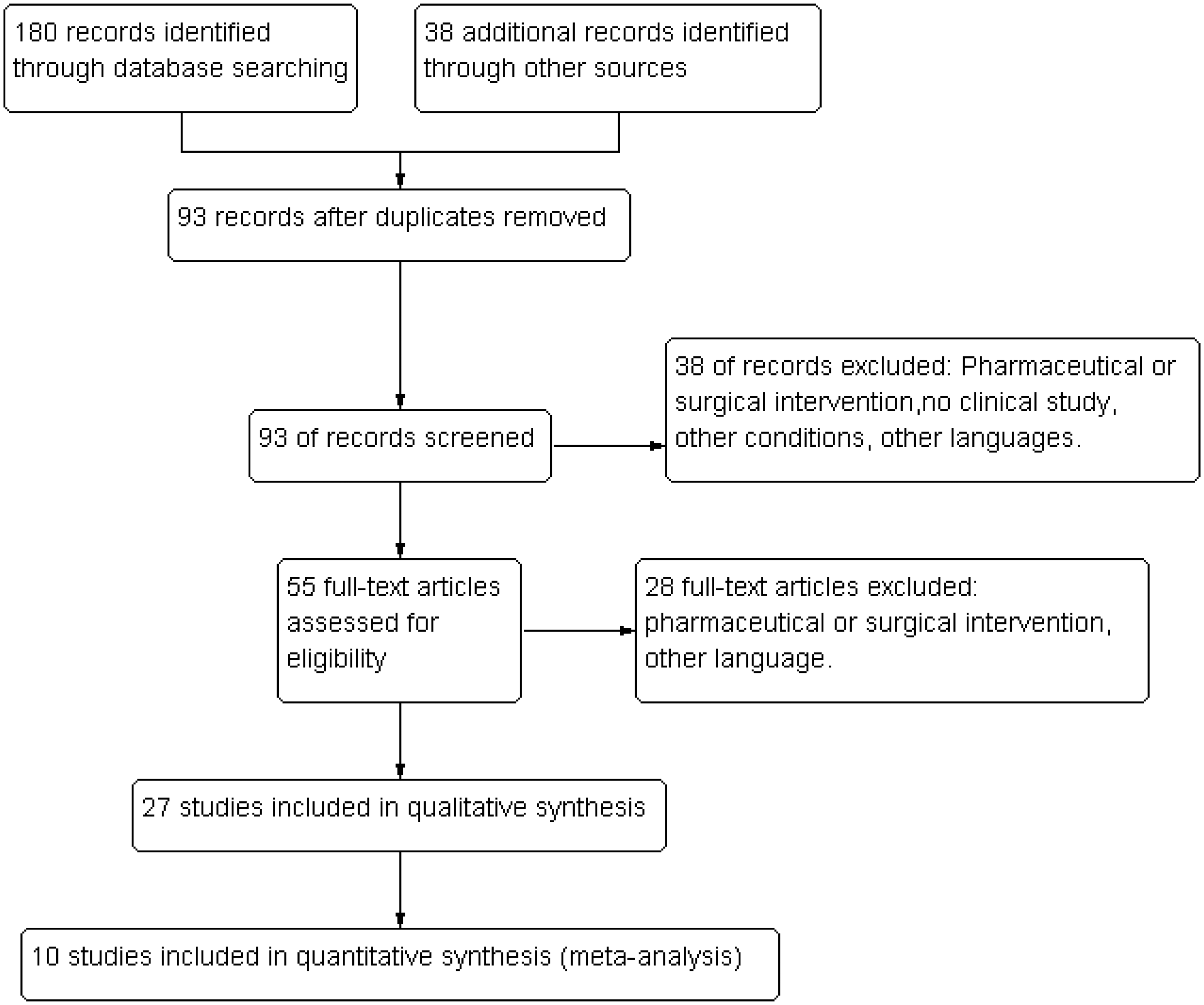
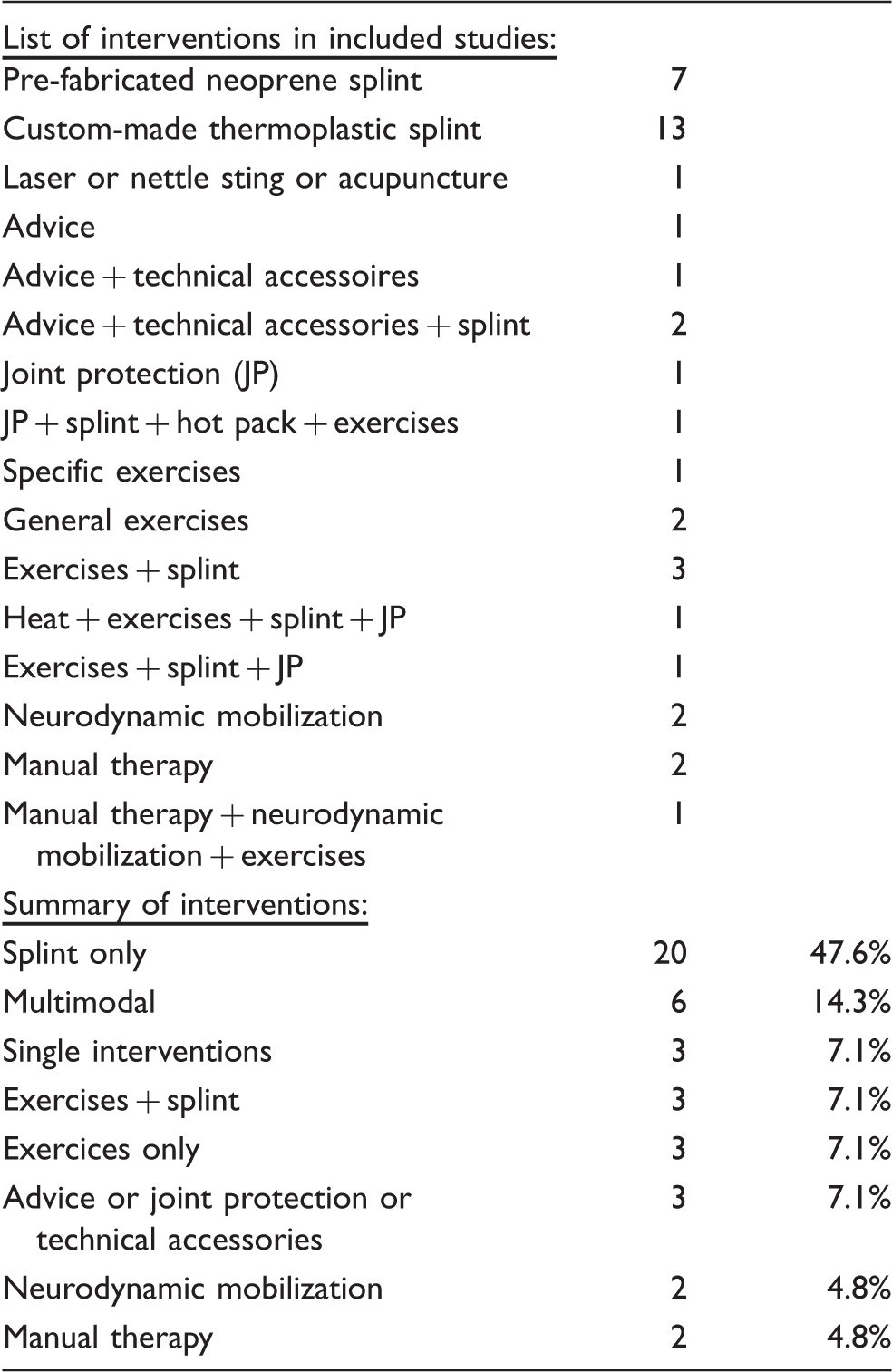
Interventions (numbers refer to frequency with which an intervention was examined).
Effects on outcomes.

Pain was reduced by all but one intervention. 19 Function was improved in all but three studies (custom-made thermoplastic splint, 20 joint protection 21 and custom-made thermoplastic long splint 22 ). Analyzing the interventions, we found that all splints seem to bring a positive result for pain regardless of their make and design. Likewise, all splint studies except two report improvement of function. The exceptions are Carreira 20 for custom-made thermoplastic splint and Weiss 22 for long custom-made thermoplastic splint. All multimodal interventions improved pain and function. Interventions consisting of exercises with or without splint improved all outcomes. The exercise regimens consisted of stabilization, standardized range of motion, general strengthening, abduction, pinch and thumb web exercises and were different in each study. Joint protection solely improved pain but not function. Neurodynamic mobilization (mobilization of median or radial nerve) and manual therapy (Kaltenborn passive posterior-anterior gliding) improved pain. Laser was tested only for pain without positive effect. Acupuncture was tested positively for pain. Nettle sting showed positive results for pain and function. Basford et al. 19 could not confirm a pain reducing effect of laser therapy in TMC OA patients. This narrative summary showed a positive overall effect of physiotherapy and occupational therapy-related interventions on pain and function in patients with TMC OA.
Two meta-analyses on the main outcome of pain could be performed. The first meta-analysis compared the pain reducing effect of pre-fabricated neoprene splint versus custom-made thermoplastic splint in five studies totaling 332 patients. This analysis found no difference between the study groups. The overall weighted mean effect size expressed as SMD was −0.01 (95%CI = −0.43, 0.40) (p = 0.95) (Figure 2).
PFN vs. CMT/pain.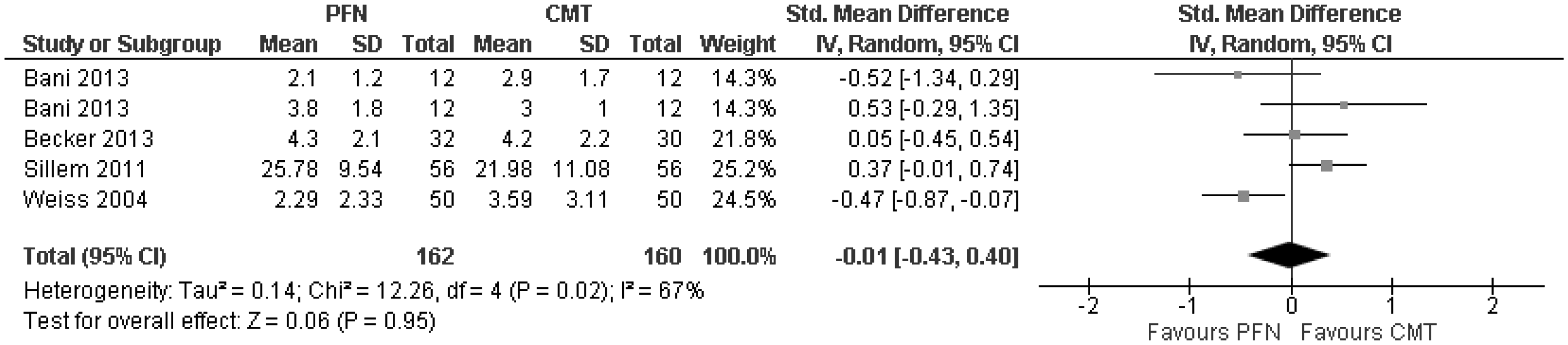
A second meta-analysis including four studies and 175 patients compared multimodal interventions to reduce pain versus control in TMC OA patients. This analysis showed a very high effect size favoring the multimodal interventions: SMD = −3.16 (95%CI = −5.56, −0.75) (p = 0.01) (Figure 3).
Multimodal vs. control/pain.
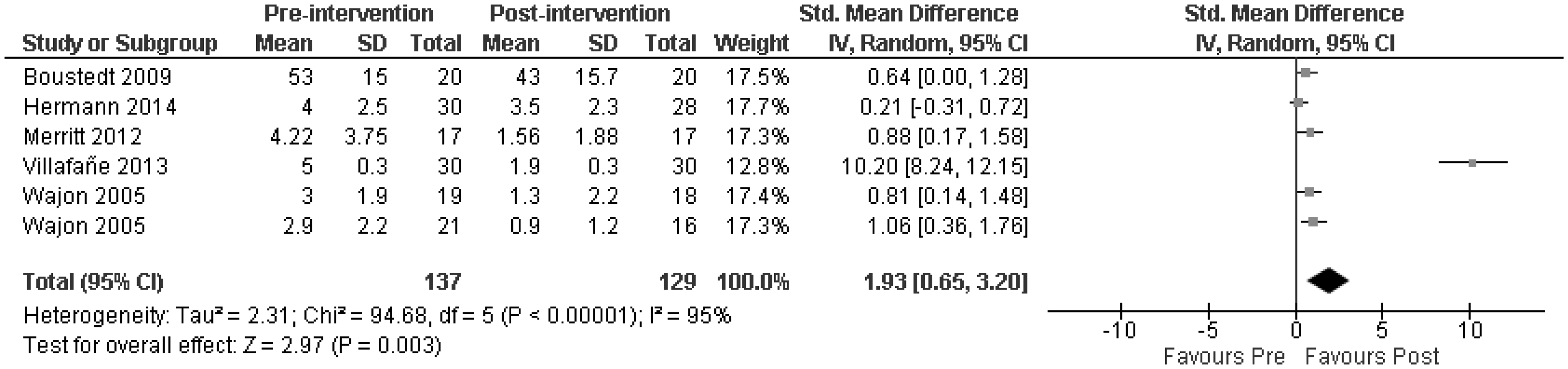
A third meta-analysis was conducted to compare the effect of multi-modal interventions on function in TMC OA patients versus control. The overall weighted effect size expressed as SMD was high: SMD = −0.66 (95%CI = −1.55, 0.23) (p = 0.15) (Figure 4), but without statistical significance. A last meta-analysis was conducted to explore the before and after effect of multimodal interventions on pain (no controls) including six studies totaling 266 patients. The overall weighted mean effect size was very high: SMD = 1.93 (95%CI = 0.65, 3.20) (p = 0.003) (Figure 5).
Multimodal vs. control/function. Multimodal pre–post/pain.
Discussion
Summary of evidence
This review including a systematic review and meta-analyses explored the effectiveness of physical and occupational therapy related interventions on pain and function in patients with TMC OA. The main finding was that there is moderate to high evidence that multimodal physiotherapy and occupational therapy related interventions have beneficial effects on pain. Concerning improvement of function, there is only narrative but no statistical evidence. Interestingly, quality of life was not examined by any of the studies. It can be assumed that absence of symptoms (e.g. pain and functional disorder) is associated with a higher quality of life. 18 If this assumption holds, then the results of this review suggest that most physiotherapy or occupational therapy related interventions also improve quality of life. Valdes et al. 11 referred to different studies which underscore the relation between pain reduction and improved hand functioning and global rating of disease in patients with hand OA. Frouzakis et al. 23 confirm that most patients seek treatment to reduce pain and not to improve function or activities of daily living (ADL).
Despite major differences in design or outcomes, three studies (need for surgery; 8 retrospective chart review; 9 retrospective cohort study 18 ) were included in this systematic review because of their clinical interest.
The narrative interpretation of the results, based on the conclusions of the individual studies, suggested that pain was improved with all intervention modalities except for laser therapy. 19 However, on many occasions in this overview, a certain discrepancy between the authors' conclusions and the reported data was observed. In some of the studies, data were missing or even contradictory to the conclusions. Some conclusions were based on selected time points, while other time points with other results were not further mentioned, indicating a high risk for reporting bias.
As Marks et al. 24 already highlighted, all studies had in common a wide variety of measurement methods for all outcomes, e.g. for pain: pain in the most recent week, pain during motion, pain at rest, pain during or after strength measurement, and so on. Moreover, the scales used in the included studies varied widely. For pain VAS, NRS, AUSCAN pain subscale, 10-point scale or verbal rating scale. For function, DASH, Quick DASH, AUSCAN, Green Test, Cochin hand function scale, Stanford Health Assessment, 10-point PRWHE scale and others.
Taken together, most studies showed poor quality and the across study heterogeneity was high, making pooling of the data to assess a true effect on population level difficult. Therefore, the reader would be reduced to pure vote-counting, which can lead to erroneous conclusions. To counter this risk, we decided to add meta-analyses for the studies presenting enough homogeneity in the key factors. This procedure is acceptable in the context of the chosen goal. 25 Based on the findings of Marks et al., 24 we decided a priori to calculate the SMD instead of the mean difference.
Neither the narrative summary nor the meta-analyses showed a difference between pre-fabricated neoprene splints and custom-made thermoplastic splints, while there is moderate to high evidence that multimodal interventions may be efficient forms of treatment in patients with TMC OA. This finding is confirmed by Berggren et al. 8 and O'Brien and Giveans. 9 The SMDs found in the two meta-analyses for multimodal interventions (−3.17 and 1.93) have clinical significance. 26
There is not enough evidence to support single interventions such as exercises, joint protection, neurodynamic mobilization, manual therapy, laser, nettle sting or acupuncture.
This review showed evidence that a multimodal physical or occupational therapy may be effective in the treatment of patients with TMC OA. Such multimodal approach could consist of splint application combined with an exercise program, patient education on joint protection, advice about technical accessories (e.g. ergonomic bottle openers or key holders) and techniques to increase the local metabolism (heat, deep frictions, ultrasound and others). Based on the evidence, the type of exercises (specific or general) integrated into a multimodal intervention seems to be irrelevant. The parity of splints concerning pain reduction has been shown. Therefore, the choice of the best splint has to be checked individually. The chosen splints should be adapted to the type of activity (hard work = thermoplastic splint, normal ADL and sleep = soft splint).
Strengths
This review included not only RCTs, but also studies with other designs, allowing a broader analysis of the effectiveness of physiotherapy or occupational therapy-related interventions on patients with TMC OA. The inclusion of the studies in the meta-analyses was done on the assumption of clinical value and based on clinical expertise.
This review may have clear clinical relevance. While there is no evidence to support single interventions, there seems to be moderate to high evidence that multimodal physical or occupational therapy related interventions may be effective in the treatment of pain and function of the hand in patients with TMC OA.
Limitations
Overall, the included studies present a moderate to high risk of bias. While the risk for performance bias through lack of blinding of participants and personnel is inherent in physical rehabilitation studies, other risks could theoretically be avoided. This elevated level of risk of bias asks for a conservative interpretation of the results. Another limitation of some studies is the lack of indication whether the participants had only isolated TMC OA or not. It may well be that patients with OA in several finger joints react differently to interventions and at measurements.
A number of other limitations of this review are recognized. First, non-published trials were not systematically searched for and this exclusion may have resulted in a biased selection of trials which were more likely to include positive trials. Second, other language publications were only included if they had an accompanying English abstract which summarized sufficient details of the trial report. Third, the procedure to include the studies in the meta-analyses was based on subjective clinical values and expertise of the authors after a consensus meeting. And finally, the number of the studies and patients included in the pooling was low.
Conclusions
This review included a systematic review with a narrative summary and a series of meta-analyses. Physical and occupational therapy-related interventions, especially multimodal interventions, seem to be effective to treat pain in patients with TMC OA. The use of pre-fabricated neoprene splints and custom-made thermoplastic splints may result in similar pain reduction. There is only narrative but not statistical evidence for effectiveness of single interventions on pain. The same has been found for improvement of function.
Multimodal interventions may need more resources. Therefore, more large and high quality studies, with embedded economic analyses are needed to further strengthen the evidence and cost-effectiveness of different types of multimodal physiotherapy or occupational therapy related interventions in patients with TMC OA.
Footnotes
Acknowledgements
The authors thank Roger Hilfiker for peer-reviewing the search strategy, Anne-Kathrin Rausch-Osthoff for peer-reviewing the manuscript and Daniel Fooder for the English editing and proof-reading.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support from the Swiss Society for Hand Rehabilitation SGHR and the Swiss Physiotherapy Association physioswiss.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.