
Abstract
Background:
The management of hormone receptor-positive (HR+), HER2-negative early breast cancer in young women presents unique challenges due to the absence of standardized guidelines and variability in clinical decision-making. In Latin America, these challenges are compounded by disparities in healthcare systems and limited access to genomic testing and supportive services.
Objectives:
To evaluate current attitudes, diagnostic strategies, and treatment practices among Latin American oncologists regarding the care of young women with HR+ early breast cancer.
Design:
A cross-sectional survey study targeting practicing oncologists across Latin America.
Methods:
A 30-item online questionnaire was distributed to 329 oncologists from 17 Latin American countries. The survey explored physician demographics, access to diagnostic tools, treatment preferences, and availability of support services, including genetic counseling and fertility preservation.
Results:
The findings revealed significant heterogeneity in clinical practices. Among patients with a Recurrence Score (RS) of 20–25, 53.8% of oncologists recommended adjuvant chemotherapy, while 23.4% considered additional clinicopathologic features. Fertility preservation counseling was inconsistently offered: 29.5% provided it routinely, whereas 12.5% never did. Ovarian function suppression (OFS) was universally recommended by 46.2% of respondents, with breast cancer specialists showing more nuanced use than non-specialists (p = 0.019). Access to genetic counseling was limited, with 12.5% reporting no access. Temporary interruption of endocrine therapy to pursue pregnancy was supported by 41.0% of respondents, though approaches varied. Female oncologists were more likely to recommend extended endocrine therapy (73.2% vs 60.8%, p = 0.019) and to refer patients for sexual health support (19.3% vs 8.7%, p = 0.05).
Conclusion:
This study highlights considerable variability in the management of young women with HR+ early breast cancer across Latin America. Physician gender, specialty, and resource availability significantly influence treatment decisions. These findings underscore the urgent need for regionally tailored clinical guidelines and improved access to diagnostic and supportive care resources to ensure equitable and evidence-based care.
Plain language summary
This study explored the therapeutic decision-making of Latin American oncologists regarding HR+, HER2-negative breast cancer in young women through a survey conducted across 17 countries, with 329 specialists participating, mainly from Argentina, Mexico, Ecuador, and Colombia. Given the unique challenges of treating young breast cancer patients, such as balancing recurrence risk, quality of life, and fertility preservation, physicians face significant variability in their approaches due to gaps and disparities in healthcare resources. The results highlighted inconsistencies in adjuvant therapy recommendations, genetic counseling referrals, and access to genomic tools, often influenced by physician specialty, gender, and years of experience. Notably, many oncologists were unaware of epidemiological databases specific to young patients, and access to key diagnostic and supportive care services—particularly genetic testing and genomic platforms used to predict benefit from adjuvant chemotherapy—remained limited. Female oncologists were more likely to recommend longer endocrine therapy durations and refer patients for sexual health support. These findings underscore the urgent need for standardized treatment guidelines and improved resource availability to optimize care for young women with HR+, HER2-negative breast cancer in Latin America.
Keywords
Introduction
Breast cancer in young women is defined as a diagnosis of breast cancer occurring before the age of 40. 1 The management of breast cancer in young women presents unique challenges, not only due to the biological and prognostic characteristics of the disease but also because of the complex therapeutic decisions faced by physicians. 2 While breast cancer predominantly affects older women, approximately 5%–7% of cases in developed countries and up to 20% in certain regions of Latin America occur in women under 40 years old. In this younger population, hormone receptor-positive (HR+), HER2-negative breast cancer often requires nuanced decision-making that balances the risk of recurrence with considerations for quality of life, fertility preservation, and long-term outcomes.3 –5
A significant challenge in treating young breast cancer patients is the variability in physicians’ attitudes and approaches to care. Evidence suggests that younger patients are often underrepresented in clinical trials, leading to gaps in evidence-based guidelines for this group.6 –8 Although clinical guidelines provide recommendations, younger patients are frequently overtreated in practice. 9 For instance, tools like Oncotype DX are more commonly associated with chemotherapy use in younger patients, yet their application varies widely. Similarly, decisions regarding the use of novel adjuvant therapies, fertility preservation, and genetic counseling are inconsistent, reflecting differing attitudes among physicians toward the needs and priorities of this patient population.10 –12 As a result, therapeutic decisions often reflect individual clinical judgment shaped by experience, available resources, and regional patterns of care. In Latin America, these challenges are compounded by disparities in healthcare systems, limited access to genomic and prognostic tools, and cultural differences in patient-physician interactions. Understanding how physicians approach the management of young women with HR+, HER2-negative breast cancer in this region is crucial for identifying gaps and opportunities to improve care delivery.
This study represents a Latin American survey of breast cancer specialists focusing on their attitudes, perceptions, and decision-making processes in managing young patients with HR+, HER2-negative breast cancer. By examining how physicians balance clinical evidence, patient preferences, and resource availability, this work aims to uncover trends and variations in care. Ultimately, these insights will inform strategies to optimize treatment approaches and address the unique needs of this underserved patient population.
Methods
Survey design
The survey was developed in Argentina by breast cancer experts from the SUMA Group (Argentine Group for Breast Cancer Research) and comprised 30 items addressing topics identified as particularly controversial or variable in daily clinical practice. These topics included epidemiological knowledge, access to care, decision-making processes, and therapeutic strategies. The questionnaire consisted of two main sections: the first collected information on physician demographics, practice characteristics, and patient population profiles, while the second focused on assessing physician attitudes and behaviors regarding breast cancer treatment decisions and access to therapeutic options. Demographic data included physician specialty (e.g., oncologists exclusively treating breast cancer patients, those managing both breast and gynecological patients, and those treating all tumor types), gender, age, country of practice, and years of experience. Practice characteristics covered the type of practice (private, public, or mixed). To evaluate therapeutic decision-making, a Likert scale was used to measure attitudes, opinions, and perceptions. The questionnaire underwent pre-testing by clinical oncology residents to enhance clarity and face validity, and to determine an average completion time of 15 min. Details of the survey design and questionnaire are provided in Appendix 1.
The reporting of this observational study conforms to the STROBE statement guidelines (Supplemental File 1).
Survey distribution
The study was conducted using an online questionnaire, disseminated via professional societies to oncologists involved in breast cancer management. Participants included oncologists from 17 Latin American countries, and the survey was written exclusively in Spanish. The questionnaire was distributed through scientific academic entities in each participating country or via designated oncologist coordinators responsible for local dissemination. Social media platforms, oncology-related blogs, and newsletters across Latin America were also used to encourage participation. The survey was shared via email, with respondents encouraged to forward it to other oncology professionals. Completion and submission of the questionnaire implied consent to participate. No monetary or other incentives were offered. The survey was hosted on Google Forms and was available from April 16 to June 21, 2024. Partially completed responses were excluded. Since each scientific society or delegate managed survey distribution, the overall response rate could not be determined. To avoid duplicate responses, each participant was required to enter their full name and hospital affiliation.
Statistical analysis
Descriptive analyses included frequency distributions for categorical variables and mean values with standard deviations for continuous variables. Responses were analyzed by stratifying results based on gender, age, professional experience, specialty, practice type (public or private), and country. Multivariable logistic regression was employed to identify associations between participant characteristics and therapeutic indications. The analysis also examined whether therapeutic decisions varied based on the oncologists’ areas of focus. Statistical significance was set at p < 0.05 (two-tailed). All analyses were performed using SPSS version 27 and R Studio.
Results
A total of 329 oncologists from 17 Latin American countries participated in the survey, with the majority from Argentina (50.2%), followed by Mexico (9.7%), Ecuador (7.0%), and Colombia (6.7%). The gender distribution was relatively balanced, with 54.1% women and 45.9% men. Regarding physician demographics, 74.5% of the respondents treated patients with all tumor types, 14.6% specialized in breast and gynecological tumors, and 10.9% focused exclusively on breast cancer. More than half of the participants (56.1%) had over 10 years of oncology practice, and 23.0% had between 5 and 10 years of experience. In terms of workplace settings, 45.0% of oncologists worked in both public and private sectors, while only 17.0% were dedicated exclusively to public healthcare. The characteristics of the participating oncologists are presented in Table 1.
Characteristics of participating oncologists.

When asked about their knowledge of epidemiological databases reporting on breast cancer in young women, 87.2% of oncologists indicated they were unaware of any such databases. Among those who were familiar, 13.0% cited Globocan as a reference.
Group-specific indications
Magnetic resonance imaging (MRI) was the preferred diagnostic tool for suspicious breast lesions in young women, selected by 60.5% of participants. In terms of screening recommendations, 51.5% believed that the starting age for screening should be lowered, irrespective of family history.
In terms of ovarian function preservation, only 38.0% of oncologists consistently recommended the use of GnRH analogs during adjuvant chemotherapy, while 17.0% rarely did so. In contrast, for ovarian function suppression (OFS) as a therapeutic approach in women under 40 years with hormone receptor-positive (HR+) breast cancer, 46.2% of oncologists recommended its use for all patients, regardless of additional risk factors. The most recommended protocol was monthly administration (59%). Regarding hormonal profile monitoring for patients undergoing OFS, 34.7% of oncologists monitored every 6 months, 35.3% every 3 months, and 23.4% did not conduct any monitoring.
Contraceptive discussions were held by 65% of oncologists during adjuvant treatment, with 81.0% recommending barrier methods as the preferred option. However, referrals to sexual health specialists were infrequent, with 42.6% of respondents rarely making such recommendations. Moreover, 45.65% of oncologists did not suggest the use of local estrogen creams for vaginal dryness caused by adjuvant hormonal therapy. Regarding pregnancy considerations, 41.0% of oncologists recommended the temporary suspension of adjuvant hormonal therapy for women who had completed at least 18 months of treatment, regardless of cancer stage or other risk factors. Furthermore, 46.2% of respondents always used multidisciplinary tumor boards to discuss young patients with luminal breast cancer, while 29.2% did so most of the time.
Resources and access
In terms of resources and access, 12.5% of oncologists reported a lack of access to genetic counseling services for young breast cancer patients, while 53.8% always recommended genetic counseling in this population. Fertility counseling also had limited referrals, with only 29.5% of oncologists stating they always or most of the time referred young patients for fertility counseling, and 12.5% never making such referrals.
Adjuvant treatment recommendations
For young women with low clinical and genomic risk breast cancer, 66.3% of oncologists considered a 5-year duration of adjuvant hormonal therapy sufficient. When adjuvant chemotherapy was indicated, 24.0% of oncologists consistently used anthracyclines, while 21.9% considered age as a factor in some cases. Genomic testing was routinely employed by 42.6% of respondents to guide treatment decisions, although 27.1% reported not having access to genomic platforms. For patients with recurrence scores (RS) between 16 and 19, 14.9% of oncologists always recommended chemotherapy, while 42.2% based their decisions on additional clinical criteria. In contrast, for patients with a higher RS between 20 and 25, 53.8% of participants indicated they would recommend adjuvant chemotherapy, while 23.4% would do so only based on accompanying clinical parameters.
Attitudes according to physicians’ characteristics
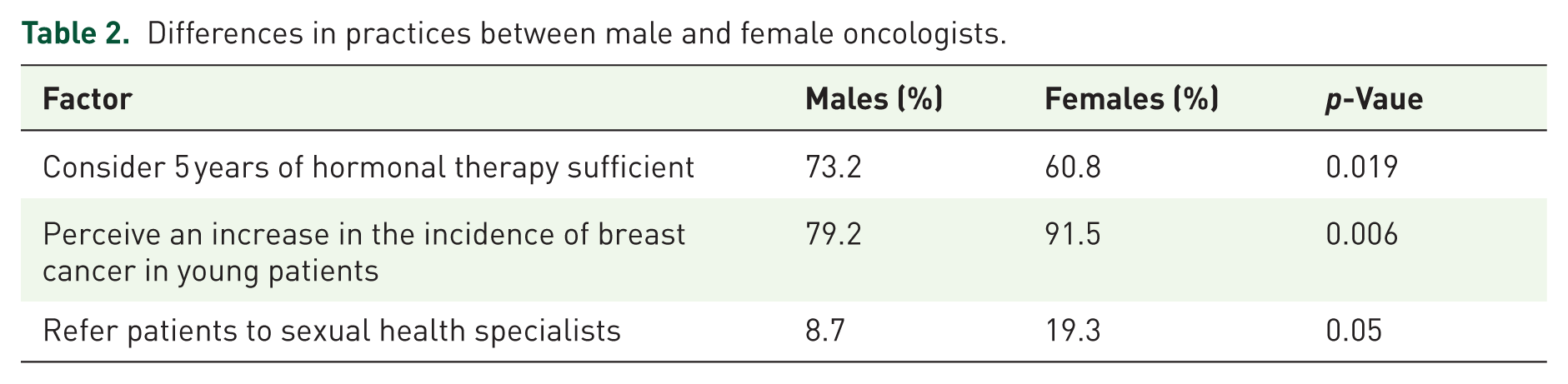
Female oncologists were less likely to consider 5 years of hormonal therapy sufficient even in low genomic and clinical risk patients compared to their male counterparts (60.8% vs 73.2%; p = 0.019) and were more likely to perceive an increasing incidence of breast cancer in young patients (91.5% vs 79.2%; p = 0.006). They also referred patients to sexual health specialists more frequently (19.3% vs 8.7%; p = 0.05). Table 2 provides a detailed comparison of clinical practices between male and female oncologists.
Differences in practices between male and female oncologists.
Professional specialty also influenced recommendations. Oncologists treating all tumor types were less likely to refer patients for genetic counseling (47.8% vs 71.4%; p = 0.003) or to use genomic platforms (38.8% vs 53.6%; p < 0.001) compared to breast cancer specialists. Similarly, multidisciplinary tumor board discussions were less frequent among general oncologists, particularly in private practice settings, where breast cancer specialists discussed their patients in 81.0% of cases, compared to only 38.6% among general oncologists (p < 0.001). Tailored OFS recommendations were more common among specialists (67.9%) than non-specialists, who prescribed OFS universally to all patients under 40 (48.6%; p = 0.019). No significant differences were observed in recommendations for fertility counseling, contraceptive measures, sexual health discussions, or temporary suspension of endocrine therapy for pregnancy. The influence of specialty on clinical decisions is illustrated in Figure 1.

Influence of specialty on clinical decisions: (a) referral to genetic counseling, (b) use of genomic platforms, (c) multidisciplinary tumor board discussions.
No clear pattern of treatment indications emerged based on the physician’s country of practice. Similarly, no statistically significant differences in treatment decisions were observed between physicians working in public versus private healthcare settings.
Discussion
This study highlights the complexities and disparities in managing young women with HR+, HER2-negative early breast cancer across Latin America. Our findings reveal significant variability in clinical practice, influenced by physician specialty, gender, and resource availability. These challenges are aggravated by the underrepresentation of young patients in clinical trials, limited access to genomic tools, and structural barriers within healthcare systems. Addressing these gaps requires targeted interventions to standardize care and improve equity.
One of the most striking observations was the divergence in treatment strategies between breast cancer specialists and non-specialists. Specialists were more likely to adhere to evidence-based practices, whereas non-specialists, who constitute the majority of oncologists in the region, often relied on universal approaches or lacked access to key resources. This discrepancy mirrors global trends but is exacerbated in Latin America by the concentration of subspecialists in urban centers, leaving general oncologists in smaller or rural settings to manage a broad spectrum of malignancies with limited support.
Clinical decision-making for young women with breast cancer remains complex and variable. OFS is a critical component of treatment for high-risk luminal tumors in young women. Although trials such as SOFT and TEXT have clarified its role in high-risk patients, our findings reflect a gap in consistent OFS use. Prescription variability among physicians has been previously documented, as noted by Kelly et al., who reported substantial heterogeneity in the use of GnRH analogs among oncologists. 13 Similarly, in our study, such variation was also evident, with breast cancer specialists demonstrating greater adherence to guideline-based recommendations. 14 The structural reality previously mentioned contributes to the variability observed in clinical practice and poses a barrier to consistent implementation of guideline-recommended care. This reinforces the need for expanded dissemination and implementation of existing guidelines, and for case discussions in multidisciplinary teams, something not always accessible in lower-resource or decentralized settings. One potential solution is the development of inter-institutional collaborations, where reference centers mentor smaller hospitals and provide remote access to tumor boards, ensuring more equitable care.
In clinical practice, younger patients are more likely to receive aggressive treatments, such as anthracyclines and taxanes, compared to their older counterparts9,15 and access to precision medicine tools remains a critical barrier. While platforms like Oncotype DX or MammaPrint are increasingly used to inform chemotherapy decisions, more than a quarter of the respondents reported no access to these platforms. Even among those with access, interpretations varied. This situation reflects both the lack of young patients in validation studies and the financial constraints limiting test availability. To bridge this gap, partnerships between academic institutions, government agencies, and private insurers could subsidize testing costs, while Latin American-specific studies could generate data more relevant to regional populations. Underrepresentation of young women does not limit to precision medicine studies and involves all type of pivotal trials, limiting the strength of evidence in this subgroup with participation rates below 5%, except in specific trials.4,14,16 –20 This lack of representation complicates treatment decisions and contributes to heterogeneity in clinical practice.
Fertility preservation and pregnancy planning emerged as another area of unmet need.6,7 A low rate of oncologists routinely referred young patients for fertility counseling. Regarding the strategy of temporary interruption of endocrine therapy, as investigated in the POSITIVE trial, less than half supported this approach even for patients with low clinical risk. Our data suggest that clinicians tend to reserve this option for highly selected cases – particularly those with low clinical and genomic risk after completing at least 18 months of endocrine treatment. A key methodological limitation is that this item in the questionnaire was framed using only affirmative options (i.e., agreement with the strategy), which prevents us from quantifying the proportion of respondents who categorically exclude this approach for all patients. These data may stem from cultural stigma, lack of oncofertility infrastructure, or insufficient awareness of guidelines. Female oncologists were more proactive in addressing these concerns, emphasizing the role of physician gender in patient-centered care. Interventions such as standardized referral pathways, patient navigation programs, and collaborations with reproductive specialists could mitigate these disparities. 20 Educational initiatives for non-specialists focused on fertility preservation and pregnancy during or after treatment could play a key role in expanding safe and informed access to these strategies.
Similarly, genetic counseling was underutilized, a concerning finding given that 10%–15% of young patients carry pathogenic BRCA mutations.21,22 While studies in high-income countries report referral rates of 73% for eligible patients, our data suggest Latin America lags behind. 22 This underscores the need for systemic improvements to ensure equitable care. Possible solutions include creating partnerships with high-complexity centers, negotiating institutional agreements with testing providers, and advocating for coverage through public or private healthcare systems. Even more, tele-genetics and train-the-trainer programs could expand access, particularly in remote areas.
The rising incidence of breast cancer in young women, as documented in the GRELL study, further underscores the urgency of these interventions. 23 Our findings align with prior research showing that younger patients often receive more aggressive treatments, yet paradoxically face gaps in supportive care (e.g., sexual health referrals). The patient experience deserves greater attention. Young women often face unique emotional, social, and reproductive challenges that impact their quality of life throughout diagnosis and treatment. Patient navigation programs specifically designed for this population could help facilitate timely access to multidisciplinary care and psychosocial support. Multidisciplinary care models, such as the 4R framework (Right information/care/time/team), could streamline coordination and address psychosocial needs.24,25
This study has several limitations inherent to its survey-based design. First, the results reflect physician perceptions and self-reported practices rather than objective measures of resource availability or patient outcomes. Second, participation bias is likely, as physicians with greater interest in young breast cancer patients or academic affiliations may have been more inclined to respond. Additionally, the survey’s distribution through professional societies could exclude clinicians in remote or underfunded settings, further skewing the data toward urban perspectives. Finally, the cross-sectional nature of the study limits our ability to assess causal relationships between physician characteristics and treatment decisions. Future research should combine qualitative insights with real-world data (e.g., hospital registries) to validate these findings.
In summary, this study identifies actionable gaps in the management of young Latin American women with HR+ breast cancer, from inconsistent adoption of OFS and genomic testing to systemic barriers in fertility preservation and genetic counseling. Solutions must be multifaceted: (1) education campaigns to align non-specialists with guidelines, (2) policy reforms to improve access to precision medicine, and (3) patient navigation programs to integrate supportive care. By leveraging regional collaborations and technology, Latin America can move toward equitable, evidence-based care for this vulnerable population.
Conclusion
Our findings underscore significant variability in the management of breast cancer in young premenopausal women across Latin America, influenced not only by medical specialization but also by physician gender and practice setting. Breast cancer specialists were more likely to recommend genomic testing, fertility preservation, and OFS compared to non-specialists. These disparities across physician subgroups reflect persistent gaps in the implementation of standardized, evidence-based care. This study offers valuable real-world insight into how clinical heterogeneity manifests in practice and reinforces the urgent need for targeted strategies to harmonize care. Addressing inequities in access to genetic counseling, oncofertility services, and advanced therapies is critical to improving outcomes for this vulnerable population. Future efforts should focus on developing educational initiatives, promoting interdisciplinary collaboration, and expanding access to personalized medicine through coordinated regional and institutional actions.
Supplemental Material
sj-docx-1-tam-10.1177_17588359251384846 – Supplemental material for Physician treatment decisions for hormone receptor-positive, HER2-negative early breast cancer in young patients: a Latin American survey
Supplemental material, sj-docx-1-tam-10.1177_17588359251384846 for Physician treatment decisions for hormone receptor-positive, HER2-negative early breast cancer in young patients: a Latin American survey by Dana Narvaez, Federico Waisberg, Cynthia Villarreal-Garza, Sergio Rivero, Cristian Alexis Ostinelli, Matías Chacón, Fernando Namuche Ojeda, Alvaro Encinas Casanave, María Lucila González Donna, Cinthia Gauna, Juana Vazquez, María Paulina Molina Espinosa, Sara C. Altuna Mujica, Ronald Limón, Kayra Sanchez Muñoz, Claudia Martinez, Vanesa Lopez, Edgar Danilo Aguirre, Adrian Nervo, Gonzalo Gomez Abuin, Andrea Aguilar, Victoria Costanzo, Santiago R. Bella, Pablo Mandó and Valeria Caceres in Therapeutic Advances in Medical Oncology
Footnotes
Appendix 1: Latin American survey on therapeutic decisions in young patients with localized HR+ HER2-negative breast cancer
Acknowledgements
To the Argentine Collaborative Group for the Study of Breast Cancer (SUMA Group) for their financial sponsorship of the publication fee of this article.
To the academic institutions and national oncology associations from the participating countries for their support in this collaborative effort.
Declarations
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.