
Abstract
Background:
Encorafenib plus cetuximab (EC) is the standard of care for pre-treated BRAF V600E mutated metastatic colorectal cancer (mCRC). Depth of response (DpR) and early tumour shrinkage (ETS) previously showed a strong correlation with survival outcomes of first-line chemotherapy ± biological agents.
Objectives:
We aimed to assess potential predictors of primary resistance to EC ± binimetinib (B) and relationships of DpR/ETS with survival outcomes and clinical characteristics.
Design:
This is a retrospective real-world cohort study of BRAF V600E mutated mCRC patients treated with second-line EC ± B at 20 Italian centres.
Methods:
Measurable disease according to Response Evaluation Criteria In Solid Tumour (RECIST) 1.1 at baseline and at least one subsequent computed tomography (CT) scan were mandatory for inclusion. Clinical features associated with primary resistance, DpR and ETS were investigated. Relationships of DpR and ETS, both as binary, according to conventional (30% for DpR and 20% for ETS) and median cut-off values, and continuous variables, with progression-free (PFS), overall survival (OS) and duration of response (DoR) were assessed in non-primary resistant patients.
Results:
A total of 105 patients were included. The primary resistance rate was 28% (29/105) and was associated with baseline peritoneal metastases (p = 0.04). Disease control and overall response rates were 72% (76/105) and 24% (25/105), respectively, with a median DpR of 15% and an ETS rate of 37% (28/76). Mucinous histology was associated with a significantly lower magnitude of DpR (p = 0.005) and a lower rate of ETS (p = 0.002). In the multivariable models, DpR significantly correlated with longer PFS as a dichotomous variable, according both to conventional (hazard ratio (HR)DpR ⩾30%: 0.52, 95% CI: 0.30–0.90, p = 0.02) and median cut-off values (HRDpR⩾15%: 0.55, 95% CI: 0.33–0.92, p = 0.03), and as a continuous variable (HR per 10% increment: 0.88, 95% CI: 0.78–0.98, p = 0.02), while correlations with OS were not confirmed. DpR was also significantly associated with longer DoR (pDpR⩾30% = 0.04; pDpR⩾15% = 0.04; pcont. = 0.02), whereas no relationships of ETS with PFS, OS or DoR were detected.
Conclusion:
A DpR of at least 15% independently predicts PFS benefit in BRAF V600E mutated mCRC patients treated with second-line EC ± B.
Introduction
The BRAF (v-Raf murine sarcoma viral oncogene homolog B1) V600E mutation–where valine (V) is substituted by glutamic acid (E) at amino acid position 600–commonly referred to as BRAFV600E, occurs in approximately 10% of metastatic colorectal cancers (mCRC) and defines a clinically and molecularly distinct subgroup of tumours with poor prognosis and refractoriness to cytotoxic agents.1,2 Some advances have been recently achieved with a combinatory targeted strategy consisting of the BRAF inhibitor encorafenib plus the anti-epidermal growth factor receptor (anti-EGFR) cetuximab (EC) ± the mitogen-activated protein kinase kinase (MEK) inhibitor binimetinib (B), that in the pivotal phase III BEACON CRC trial showed improved overall survival (OS), progression-free survival (PFS) and overall response rate (ORR) as compared to a standard irinotecan plus cetuximab-based treatment in pre-treated patients with BRAF V600E -mutated mCRC.3,4 Since the addition of binimetinib to EC did not result in better survival outcomes and, at the same time, was related to a less favourable safety profile, EC is now a guideline-recommended therapeutic option for mCRC patients with BRAF V600E mutated tumours who received at least a prior treatment regimen. 5 Nevertheless, a significant proportion of patients experience primary resistance or short-term clinical benefit when receiving EC.
To date, several efforts have been conducted towards the identification of potential predictive and prognostic biomarkers to stratify patient candidates for this therapeutic approach. A previously published real-world series 6 suggested worse Eastern Cooperative Oncological Group Performance Status (ECOG PS), peritoneal metastases, and more than one prior treatment as independent prognostic factors. Additionally, inactivating mutations in ring finger protein 43 (RNF43)–which encodes a negative regulator of the Wingless-related integration site (WNT) pathway–are suggested to be related to a better prognosis in patients with proficient mismatch repair/microsatellite stable (pMMR/MSS) BRAFV600E mutated mCRC treated with the anti-BRAF targeted approach.7,8 Most recently, a secondary analysis of the BEACON trial 9 reported potential associations between clinical outcomes of patients with BRAF V600E -mutated mCRC treated with EC ± B and immune gene signatures but not with RNF43 mutational status. Molecular correlates of acquired resistance were also characterized in depth suggesting a context of adaptive mutability as the potential reason for targeted treatment failure. 9 Furthermore, novel radiological parameters emerged as tools able to implement the conventional Response Evaluation Criteria In Solid Tumours (RECIST)-defined metrics in the assessment of the dynamics of tumour response. Among them, early tumour shrinkage (ETS) and depth of response (DpR) have been developed to describe temporal and quantitative longitudinal changes in disease burden during anti-tumour treatments. Post hoc exploratory analyses of several randomized clinical trials exploring first-line strategies with chemotherapy ± targeted agents in mCRC showed that both ETS and DpR are valuable predictors of survival outcomes in mCRC patients.10–14 More remarkably, increasing evidence suggests that these parameters may more accurately measure the quality and magnitude of response to targeted therapies in mCRC than the conventional RECIST metrics.15,16
This concept takes particular relevance in patients with BRAF V600E mutated tumours treated with EC ± B, characterized by relatively short-term clinical benefit and poor outcomes following resistance to targeted therapy.3,4 However, no data linking DpR and ETS to survival outcomes in patients with BRAF V600E mutated mCRC treated with EC ± B are currently available.
Based on these considerations, we aimed to investigate DpR and ETS as tumour dynamic response parameters and assess their relationships with baseline characteristics and clinical outcomes in a retrospective well-annotated cohort of patients with BRAF V600E mutated mCRC treated in a real-world setting with EC ± B after progression to one previous systemic therapy.
Methods
Study design and population
This was a retrospective cohort study in consecutive patients with BRAF V600E mutated mCRC treated with EC ± B at 20 Italian hospitals in a real-life setting, between May 2019 and October 2022. Patients were initially treated with EC ± B within a nominal use program, launched in Italy in May 2019, and since February 2020 they received only EC, as per clinical indication. For the present analysis, patients who had received only one systemic treatment for metastatic disease prior to EC ± B, with at least one measurable lesion according to the RECIST 1.1 criteria and availability of at least one radiological disease re-assessment using computed tomography (CT) scan as per clinical practice, were selected. Treatment was administered until disease progression, unacceptable toxicities or the patient’s refusal. Investigators retrospectively collected data on all consecutively enrolled patients from medical records after obtaining their informed consent. A waiver of consent was considered for deceased patients or those lost to follow-up. The study was approved by local Ethic Committees (Oncologic Institute of Veneto, code 2017/34) and its reporting conforms with the ESMO Guidance for Reporting Oncology real-World Evidence (ESMO-GROW) (Supplemental File). 17
Endpoints
The primary endpoint was to assess the impact of ORR, DpR and ETS on PFS and OS. Secondary endpoints were to explore the influence of ORR, DpR and ETS on the tailor-defined duration of response (DoR) and to characterize potential predictors of primary resistance to treatment, magnitude of DpR and rate of ETS. PFS was calculated as the time from the start of treatment with EC ± B to the evidence of progressive disease (PD) or death from any cause, whichever occurred first. Patients alive and not experiencing disease progression at the time of the analysis were censored at the date of the last tumour assessment.
OS was calculated as the time from the start of treatment with EC ± B to death from any cause. Censoring was performed at the date of the last follow-up for patients who were alive at the time of the analysis. DoR was defined as the time from the first documentation of tumour shrinkage (i.e., ⩾1%) to PD or death from any cause.
Assessment of radiological parameters
Tumour objective response dynamics were based on investigator-reported measurements and assessed according to the RECIST 1.1 criteria by the evaluating medical oncologist. ORR was calculated as the percentage of patients achieving complete response (CR) or partial response (PR). ETS rate was defined as the percentage of patients achieving a decrease of at least 20% in the sum of the longest diameters of the RECIST target lesions at the first radiological re-assessment as compared to baseline, and DpR was defined as the relative change in the sum of the longest diameters of the RECIST target lesions at the nadir, in the absence of new lesions or progression of non-target lesions, as compared with baseline.
The impact of ORR, ETS and DpR on survival outcomes (i.e., PFS, OS and DoR) was assessed only in the subset of patients achieving at least disease stabilization (SD) as the best response. Patients experiencing PD at the first radiological assessment (i.e., primary resistance) were analysed separately.
Statistical analysis
DpR and ETS were considered either binary (adopting the median and conventional values as cut-off) or continuous variables, with 10 levels based on decile distribution. When both parameters were analysed as continuous variables, hazard ratios (HRs) were referred to each increment of one decile point. According to RECIST 1.1 criteria, patients were dichotomized as responders (i.e., achieving CR or PR) or non-responders (i.e., achieving SD). Analyses involving response-related parameters were based on an 8-week landmark approach (i.e., coinciding with the earliest time of CT scan reassessment for tumour response).
PFS and OS curves were plotted with the Kaplan-Meier method and compared by the log-rank test. HRs and relative 95% confidence intervals (CIs) were estimated by the Cox proportional hazards model. Median values and interquartile ranges (IQR) were adopted to describe the distribution of continuous variables. Chi-squared test, Fisher’s exact test, Kruskal-Wallis and Mann-Whitney U tests were adopted as appropriate to examine baseline differences between groups. Covariates with p < 0.10 at univariable analyses were included in multivariable Cox proportional hazard models. Statistical significance was set at a p-value of 0.05. All analyses were carried out with MedCalc v22.002 (https://www.medcalc.org/), RStudio 2023.06.1+524 ‘Mountain Hydrangea’ Release (https://www.R-project.org/) and JMP PRO 17 (https://www.jmp.com/).
Results
In all, 105 patients were eligible for the present analysis. Their baseline demographic, clinical, molecular and treatment characteristics are summarized in Supplemental Table 1.
Overall, the median age at the beginning of targeted therapy was 66 years (IQR 57.4–74.1), 54% were female, and 91% had an ECOG PS of 0 or 1. Tumours were mostly right-sided (69%) and involved more than one metastatic site in 73% of cases, including the peritoneum in 49% of patients. Deficient mismatch repair (dMMR)/Microsatellite instability-high (MSI-H) status and mucinous histology were detected in 7% and 28% of patients, respectively. Among four patients with dMMR/MSI-H tumour, none of them received immune-checkpoint inhibitors (ICIs) before or after the study treatment, because in the timeframe of their clinical course, ICIs were not a standard of care for this molecular subgroup. Previous treatment consisted of a triplet, doublet or single-agent chemotherapy backbone in 44 (42%), 56 (53%) and 5 (5%) patients, respectively. Sixteen (15%) patients received binimetinib in combination with EC.
At the time of this analysis (data cut-off: February 6th, 2023), the median follow-up was 19.3 months (IQR 12.6–28.7). Ninety-two (88%) and 75 (71%) events of disease progression and death occurred, respectively. In the overall population, mPFS and mOS were 5.2 (95% CI: 4.6–5.8) and 10.3 (95% CI: 7.8–11.6) months, respectively (Supplemental Figure 1A and B).
Tumour response and its dynamics at different timepoints are summarized in Figures 1 and 2. Seventy-six (72%) patients achieved disease control; among them, 25 (24%) and 51 (48%) had an objective response and disease stabilization, respectively. Primary resistance was observed in 29 (28%) subjects.

Waterfall plot for response to encorafenib plus cetuximab ± binimetinib.
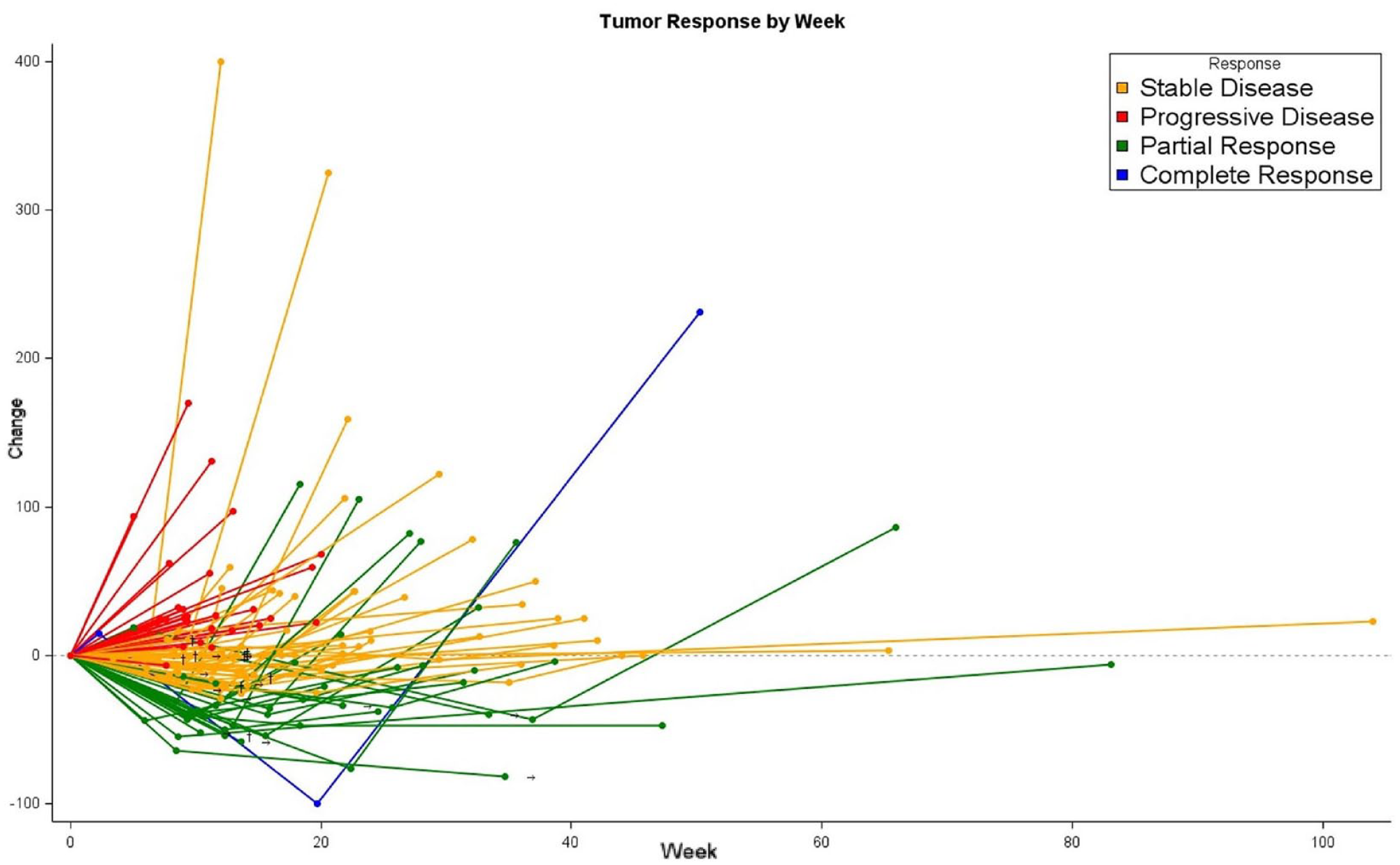
Spider plot for response to encorafenib plus cetuximab ± binimetinib.
Predictors of primary resistance to treatment
Baseline characteristics of patients experiencing primary resistance (n = 29) are reported in Supplemental Table 2; they did not significantly differ from those of patients achieving clinical benefit, except for a higher prevalence of baseline peritoneal metastases (66% versus 43%, p = 0.04).
Tumour response parameters in patients achieving disease control
Among 76 patients experiencing at least disease control, the median DpR was 15% (IQR 2–37), and a reduction in the sum of the highest diameters of the target lesions (i.e., ⩾1%) was observed in 61 (80%) out of 76 cases. ETS occurred in 28 (37%) patients and the median ETS was 12% (IQR 0–28).
Baseline patients’ characteristics according to ETS and DpR are detailed in Supplemental Table 3. No significant association was observed between baseline characteristics and radiological parameters, except for the lower magnitude of ETS (0% versus 14%, p = 0.002) and DpR (2% versus 19%, p = 0.005) in the subgroup of tumours with mucinous histology (Supplemental Table 3).
Expectedly, responders (n = 25) experienced longer PFS (mPFS: 7.5 versus 5.4 months; HR: 0.54, 95% CI: 0.33–0.88; p = 0.02) and OS (mOS: 13.3 versus 11.1 months; HR: 0.58, 95% CI: 0.33–1.04; p = 0.08) as compared to non-responders (n = 51) (Figure 3(a) and (b)). The association of RECIST response with PFS but not with OS was confirmed in the multivariable analyses (Table 1).
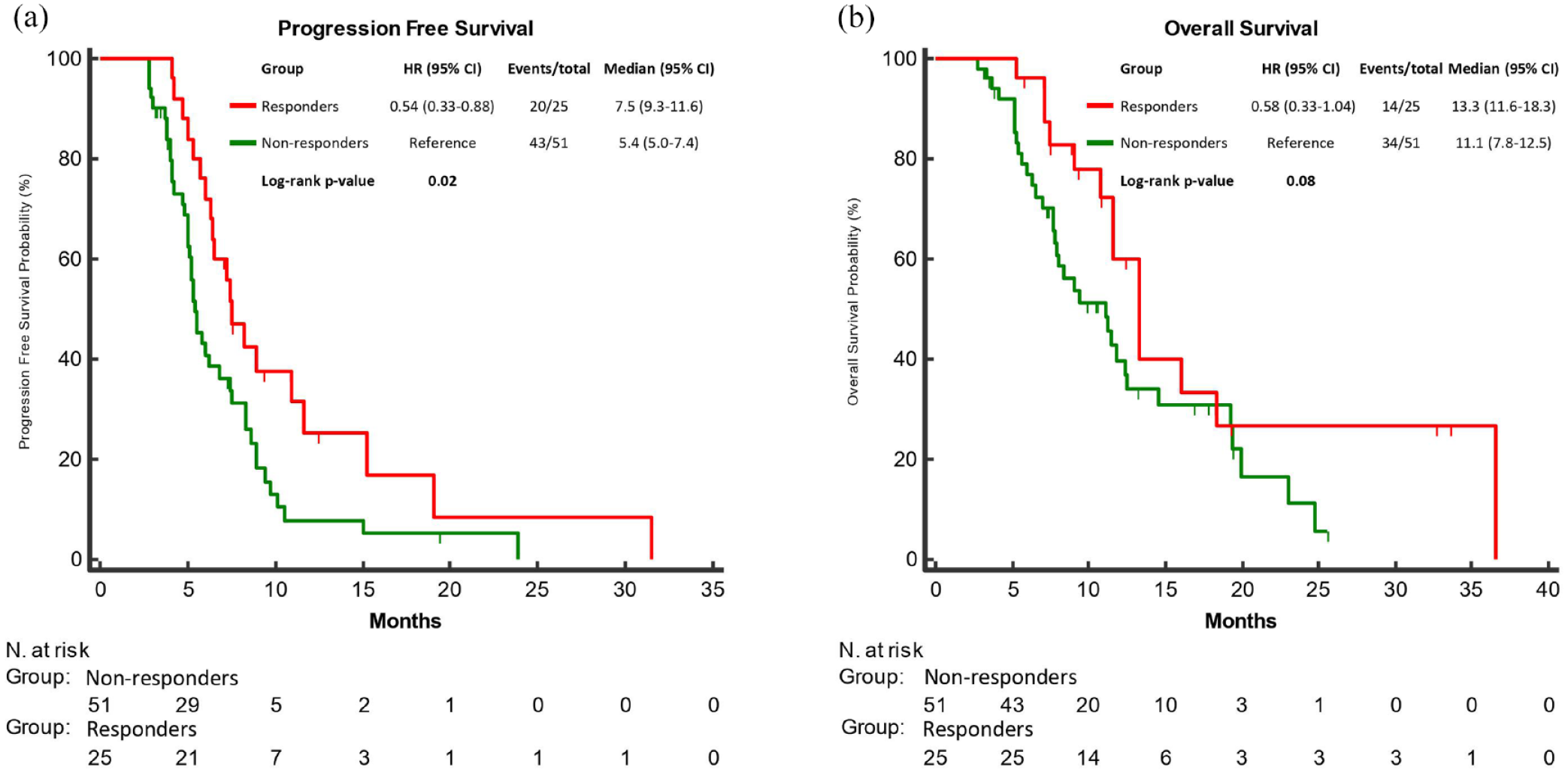
PFS (a) and OS (b) according to RECIST response (responders (CR/PR) vs non-responders (SD)) to encorafenib plus cetuximab ± binimetinib.
Uni- and multivariable analyses for progression-free survival and overall survival according to RECIST response to encorafenib plus cetuximab ± binimetinib.

Ca 19.9, carbohydrate antigen sialyl Lewis a; CEA, carcinoembryonic antigen; DpR, depth of response; ECOG PS, Eastern Cooperative Oncology Group Performance Status; HR, hazard ratio; MS, microsatellite status; Mts, metastases; NA, not available.
Statistically significant p values (i.e., <0.10 and <0.05 for uni- and multivariable analyses, respectively) are highlighted in bold.
Furthermore, a highly significant association of DpR as a binary variable, according to the median value (15%), with both PFS and OS was found. Indeed, patients with a DpR ⩾15% reported longer PFS (mPFS: 7.5 versus 5.3 months; HR: 0.56, 95% CI: 0.33–0.93; p = 0.02) and OS (mOS: 13.3 versus 9.4 months; HR: 0.61, 95% CI: 0.34–1.07; p = 0.08) as compared to those with a DpR < 15% (Figure 4(a) and (b)). Comparable results were observed when DpR was considered as a continuous variable, with a significant association with both PFS (HR per 10% increment: 0.87, 95% CI: 0.77–0.96, p = 0.01) and OS (HR per 10% increment: 0.88, 95% CI: 0.76–0.99, p = 0.04) (Table 2). Both as a continuous and a binary variable, DpR was independently correlated with PFS in the multivariable analyses (Tables 2 and 3), while the same correlations with OS were not confirmed (Tables 2 and 3).

PFS (a) and OS (b) according to tumour shrinkage using a 15% DpR threshold for response to encorafenib plus cetuximab ± binimetinib.
Uni- and multivariable analyses for progression-free survival and overall survival according to DpR as a continuous variable.

For a 10% increment.
Ca 19.9, carbohydrate antigen sialyl Lewis a; CEA, carcinoembryonic antigen; DpR, depth of response; ECOG PS, Eastern Cooperative Oncology Group Performance Status; HR, hazard ratio; MS, microsatellite status; Mts, metastases; NA, not available.
Statistically significant p values (i.e., <0.10 and <0.05 for uni- and multivariable analyses, respectively) are highlighted in bold.
Uni- and multivariable analyses for progression-free survival and overall survival according to a 15% DpR threshold for response to encorafenib plus cetuximab ± binimetinib.

Ca 19.9, carbohydrate antigen sialyl Lewis a; CEA, carcinoembryonic antigen; DpR, depth of response; ECOG PS, Eastern Cooperative Oncology Group Performance Status; HR, hazard ratio; MS, microsatellite; mts, metastases; NA, not available.
Statistically significant p values (i.e., <0.10 and <0.05 for uni- and multivariable analyses, respectively) are highlighted in bold.
Conversely, achieving ETS (⩾20%) was not associated with either PFS (HR: 0.81, 95% CI: 0.49–1.34, p = 0.41) or OS (HR: 0.82, 95% CI: 0.46–1.47, p = 0.51) (Supplemental Figure 2A and B). Consistently, when the median value was adopted as a cut-off, patients achieving an ETS ⩾12% had the same outcome as those achieving an ETS < 12%, in terms of both PFS (HR: 0.81, 95% CI: 0.49–1.32, p = 0.38) and OS (HR: 0.87, 95% CI: 0.49–1.53, p = 0.62) (Supplemental Figure 3A and B). Similarly, no correlation between ETS, as a continuous variable, and both PFS (HR per 10% increment: 0.94, 95% CI: 0.84–1.04, p = 0.24) and OS (HR per 10% increment: 0.95, 95% CI: 0.83–1.08, p = 0.41) was detected.
Finally, relationships between DpR and DoR were explored. While RECIST response was expectedly correlated with longer DoR (HR: 0.56, 95% CI: 0.33–0.97, p = 0.04), comparable outcomes were also reported in patients achieving a DpR ⩾ 15% (HR: 0.60, 95% CI: 0.36–0.99, p = 0.04). These observations were confirmed when DpR was employed as a continuous variable (HR per 10% increment: 0.88, 95% CI: 0.79–0.98, p = 0.02).
Discussion
Although achieving an objective response is often regarded as a minimally meaningful endpoint in a purely palliative setting, among pre-treated patients with BRAF V600E -mutated mCRC achieving an early and deep tumour shrinkage may be crucial since the high burden and intrinsic aggressive behaviour of the disease make the relief of tumour-related symptoms and the prevention of patient’s clinical deterioration the primary objective of treatment.
To this regard, size-based RECIST criteria – commonly adopted in the daily practice to estimate the ability of a treatment regimen to induce tumour shrinkage – have been widely debated for their inability to fully characterize tumour response during targeted therapies, both in terms of timing and magnitude of depth over time. To explore alternative metrics that could capture different patterns of tumour dynamics potentially related to long-term outcomes, ETS and DpR have first been investigated in mCRC patients receiving first-line treatment with chemotherapy ± biologic agents.10,14 Conversely, their correlation with the outcome of patients treated with targeted agents is yet to be determined.
The present analysis is the first attempt to challenge the concepts of DpR and ETS in a retrospective, well-annotated and clinically homogeneous cohort of patients with BRAF V600E mutated mCRC receiving EC ± B as second-line treatment, which is currently the optimal positioning of this targeted approach. The prognostic accuracy of both radiological dynamic parameters in patients achieving disease control at the first radiological tumour assessment was investigated.
To the best of our knowledge, we provided the first evidence of the independent impact of both DpR and RECIST response on the clinical outcomes of this subgroup of patients. In particular, we observed that achieving a RECIST response or a DpR of at least 15% is associated with better outcomes in terms of PFS, even when adjusting for other established prognostic variables. From a clinical perspective, patients achieving a tumour shrinkage of at least 15% have a chance of disease control similar to that of patients achieving a RECIST response. This suggests that a less stringent shrinkage cut-off for response may still provide clinicians with a reassuring treatment marker of benefit from EC ± B. Further confirmation of the biological reliability of these observations is offered by the significant impact of DpR on PFS also as a continuous variable (i.e., per 10% increment in tumour shrinkage), which perfectly aligns with the underlying definition of DpR itself.
Nevertheless, in contrast with previous reports,10–12,15 we failed to demonstrate a significant association of DpR and RECIST response with OS. We hypothesize that the inherent disease aggressiveness after progression to second-line EC ± B and the overall dismal prognosis may have clouded the apparent impact of targeted therapy on the disease burden, with patients rapidly deteriorating regardless of previous response dynamics. Similarly, the limited sample size and potential confounding effect of subsequent lines of therapy might have hampered the results of these analyses.
Moreover, ETS was not associated with survival outcomes. This finding mirrors a historical pitfall of targeted therapies in the therapeutic management of mCRC probably due to the early selection of resistant clones leading to disease progression that becomes evident at the following radiological staging, irrespective of the initial dimensional reduction of lesions. Conversely, the reason why DpR analyses could intercept at least a confirmed PFS benefit in our cohort may be likely because this parameter can be measured at any timepoint and is, therefore, able to identify a subgroup of patients achieving confirmed and more durable responses, as shown in our dataset.
Focusing on the subgroup of patients who derived no benefit from EC ± B, we observed an enrichment of peritoneal involvement, corroborating the well-known aggressiveness of tumours spreading to this site. 1 Nevertheless, no definitive conclusions could be drawn regarding a potential negative predictive role since all patients in our population received the same EGFR- and BRAF- inhibitor-based treatment strategy. Moreover, among patients achieving clinical benefit, the presence of mucinous histology yielded a negative impact on tumour shrinkage, reflecting once again the well-established refractoriness to systemic treatments of mucinous mCRC.18,19
We acknowledge some limitations of our work, including the retrospective nature of the study, the lack of a blinded independent central review of CT scans, the unclear suitability of version 1.1 as compared to 1.0 of the RECIST criteria when evaluating tumour response dynamics, the not fully standardized timing of CT scans that followed standard clinical practice. Despite a relatively large sample size (considering the prevalence of BRAF V600E mutation in mCRC), hypothesis-generating conclusions can be drawn from these analyses given the overall limited number of included patients. However, it should be pointed out that the multicenter academic effort, and the consistency of activity and survival outcomes with those reported in the pivotal BEACON trial, mitigate the above-mentioned weak points and reassure on the reliability of our data. 20
Conclusion
While these results report for the first time the role of DpR as a predictor of clinical outcome in a cohort of patients with BRAF V600E mutated mCRC treated with targeted therapy, their further validation in post hoc analyses of randomized trials would be warranted.3,21
Supplemental Material
sj-docx-1-tam-10.1177_17588359241299975 – Supplemental material for Prognostic impact of depth of response and early tumour shrinkage in patients with BRAFV600E-mutated metastatic colorectal cancer treated with targeted therapy
Supplemental material, sj-docx-1-tam-10.1177_17588359241299975 for Prognostic impact of depth of response and early tumour shrinkage in patients with BRAFV600E-mutated metastatic colorectal cancer treated with targeted therapy by Guglielmo Vetere, Marco Maria Germani, Carlotta Antoniotti, Lisa Salvatore, Filippo Pietrantonio, Sara Lonardi, Maria Bensi, Filippo Ghelardi, Maria Alessandra Calegari, Rossana Intini, Alessandro Minelli, Francesco Giulio Sullo, Chiara Boccaccio, Ada Taravella, Alberto Puccini, Daniele Lavacchi, Laura Noto, Massimiliano Salati, Mario Scartozzi and Chiara Cremolini in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-2-tam-10.1177_17588359241299975 – Supplemental material for Prognostic impact of depth of response and early tumour shrinkage in patients with BRAFV600E-mutated metastatic colorectal cancer treated with targeted therapy
Supplemental material, sj-docx-2-tam-10.1177_17588359241299975 for Prognostic impact of depth of response and early tumour shrinkage in patients with BRAFV600E-mutated metastatic colorectal cancer treated with targeted therapy by Guglielmo Vetere, Marco Maria Germani, Carlotta Antoniotti, Lisa Salvatore, Filippo Pietrantonio, Sara Lonardi, Maria Bensi, Filippo Ghelardi, Maria Alessandra Calegari, Rossana Intini, Alessandro Minelli, Francesco Giulio Sullo, Chiara Boccaccio, Ada Taravella, Alberto Puccini, Daniele Lavacchi, Laura Noto, Massimiliano Salati, Mario Scartozzi and Chiara Cremolini in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-5-tam-10.1177_17588359241299975 – Supplemental material for Prognostic impact of depth of response and early tumour shrinkage in patients with BRAFV600E-mutated metastatic colorectal cancer treated with targeted therapy
Supplemental material, sj-docx-5-tam-10.1177_17588359241299975 for Prognostic impact of depth of response and early tumour shrinkage in patients with BRAFV600E-mutated metastatic colorectal cancer treated with targeted therapy by Guglielmo Vetere, Marco Maria Germani, Carlotta Antoniotti, Lisa Salvatore, Filippo Pietrantonio, Sara Lonardi, Maria Bensi, Filippo Ghelardi, Maria Alessandra Calegari, Rossana Intini, Alessandro Minelli, Francesco Giulio Sullo, Chiara Boccaccio, Ada Taravella, Alberto Puccini, Daniele Lavacchi, Laura Noto, Massimiliano Salati, Mario Scartozzi and Chiara Cremolini in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-pdf-7-tam-10.1177_17588359241299975 – Supplemental material for Prognostic impact of depth of response and early tumour shrinkage in patients with BRAFV600E-mutated metastatic colorectal cancer treated with targeted therapy
Supplemental material, sj-pdf-7-tam-10.1177_17588359241299975 for Prognostic impact of depth of response and early tumour shrinkage in patients with BRAFV600E-mutated metastatic colorectal cancer treated with targeted therapy by Guglielmo Vetere, Marco Maria Germani, Carlotta Antoniotti, Lisa Salvatore, Filippo Pietrantonio, Sara Lonardi, Maria Bensi, Filippo Ghelardi, Maria Alessandra Calegari, Rossana Intini, Alessandro Minelli, Francesco Giulio Sullo, Chiara Boccaccio, Ada Taravella, Alberto Puccini, Daniele Lavacchi, Laura Noto, Massimiliano Salati, Mario Scartozzi and Chiara Cremolini in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-tiff-3-tam-10.1177_17588359241299975 – Supplemental material for Prognostic impact of depth of response and early tumour shrinkage in patients with BRAFV600E-mutated metastatic colorectal cancer treated with targeted therapy
Supplemental material, sj-tiff-3-tam-10.1177_17588359241299975 for Prognostic impact of depth of response and early tumour shrinkage in patients with BRAFV600E-mutated metastatic colorectal cancer treated with targeted therapy by Guglielmo Vetere, Marco Maria Germani, Carlotta Antoniotti, Lisa Salvatore, Filippo Pietrantonio, Sara Lonardi, Maria Bensi, Filippo Ghelardi, Maria Alessandra Calegari, Rossana Intini, Alessandro Minelli, Francesco Giulio Sullo, Chiara Boccaccio, Ada Taravella, Alberto Puccini, Daniele Lavacchi, Laura Noto, Massimiliano Salati, Mario Scartozzi and Chiara Cremolini in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-tiff-4-tam-10.1177_17588359241299975 – Supplemental material for Prognostic impact of depth of response and early tumour shrinkage in patients with BRAFV600E-mutated metastatic colorectal cancer treated with targeted therapy
Supplemental material, sj-tiff-4-tam-10.1177_17588359241299975 for Prognostic impact of depth of response and early tumour shrinkage in patients with BRAFV600E-mutated metastatic colorectal cancer treated with targeted therapy by Guglielmo Vetere, Marco Maria Germani, Carlotta Antoniotti, Lisa Salvatore, Filippo Pietrantonio, Sara Lonardi, Maria Bensi, Filippo Ghelardi, Maria Alessandra Calegari, Rossana Intini, Alessandro Minelli, Francesco Giulio Sullo, Chiara Boccaccio, Ada Taravella, Alberto Puccini, Daniele Lavacchi, Laura Noto, Massimiliano Salati, Mario Scartozzi and Chiara Cremolini in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-tiff-6-tam-10.1177_17588359241299975 – Supplemental material for Prognostic impact of depth of response and early tumour shrinkage in patients with BRAFV600E-mutated metastatic colorectal cancer treated with targeted therapy
Supplemental material, sj-tiff-6-tam-10.1177_17588359241299975 for Prognostic impact of depth of response and early tumour shrinkage in patients with BRAFV600E-mutated metastatic colorectal cancer treated with targeted therapy by Guglielmo Vetere, Marco Maria Germani, Carlotta Antoniotti, Lisa Salvatore, Filippo Pietrantonio, Sara Lonardi, Maria Bensi, Filippo Ghelardi, Maria Alessandra Calegari, Rossana Intini, Alessandro Minelli, Francesco Giulio Sullo, Chiara Boccaccio, Ada Taravella, Alberto Puccini, Daniele Lavacchi, Laura Noto, Massimiliano Salati, Mario Scartozzi and Chiara Cremolini in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
The authors acknowledge all participating centres for their contributions and the GONO and ARCO Foundations for their support in the conduction of this study.
Declarations
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.