
Abstract
Background:
A large number of studies have proved that prostate-specific membrane antigen-positron emission tomography/computer tomography (PSMA-PET/CT) provides excellent accuracy in primary staging and restaging of prostate cancer. Less data exist with PSMA-single photon emission computed tomography (SPECT)/CT investigations.
Objective:
The aim of this study was to evaluate the performance of [99mTc]Tc-PSMA-I&S (for imaging and surgery) in prostate cancer.
Design and methods:
We retrospectively analysed PSMA-SPECT/CT scans of 20 healthy volunteers and 100 male patients with prostate cancer. All of them had histologically confirmed prostate cancer. In all, 28 patients were examined for primary staging and 72 for biochemical recurrence or progressive disease. Whole body SPECT/CT imaging was carried out 6 h after the intravenous administration of 666 ± 102 MBq [99mTc]Tc-PSMA-I&S. Images were evaluated visually and semi-quantitatively.
Results:
Patient-based sensitivity, specificity, positive predictive value, negative predictive value and accuracy for primary prostate cancer were 86%, 100%, 100%, 83% and 92%, respectively. For detecting metastases in primary staging, these values were 88%, 100%, 100%, 85% and 93%, respectively. The radiopharmaceutical uptake of primary prostate cancer was significantly higher than in normal prostate. The patient-based sensitivity, specificity, positive predictive value, negative predictive value and accuracy of the method in the visualization of local recurrence were 67%, 100%, 100%, 86% and 89%, and for detecting metastases in restaging were 91%, 92%, 98%, 75% and 91%, respectively. In restaging, detection rates were 37% under prostate-specific antigen level of 1 ng/mL, 74% between 1 and 5 ng/mL and 80% >5 ng/mL.
Conclusion:
[99mTc]Tc-PSMA-I&S-SPECT/CT can be easily integrated into the routine diagnostic practice, and it provides usable data in primary staging and restaging of prostate cancer. Quantitative assessment of PSMA-SPECT/CT has the potential to be used to differentiate between physiological and pathological intraprostatic tracer uptake.
Introduction
In the last few years, the development of small-molecule inhibitors of prostate-specific membrane antigen (PSMA) and their clinical application has become an inherent part of prostate cancer imaging and therapy.1–3 An increasing number of studies prove that PSMA-positron emission tomography/computer tomography (PET/CT) provides excellent accuracy and can be a suitable replacement for conventional imaging methods (CT and bone scintigraphy) in primary staging, as well as in restaging of patients with biochemical recurrence.4–7 PSMA-PET showed higher detection rates compared to the previously used choline-PET, even in early biochemical recurrence.8–10 Furthermore, PSMA-PET imaging can increase diagnostic accuracy for the localization of primary prostate cancer and could help targeted biopsy and improve the planning of surgical treatment and focal therapy. 11
Although PSMA-PET tracers have been extensively investigated, less data exist about investigation with PSMA-single photon emission computed tomography (SPECT) radiopharmaceuticals. Several studies have demonstrated that PSMA-SPECT/CT could be a reasonable and cost-effective alternative to PSMA-PET/CT.12–16 So far, there is no comprehensive data on the diagnostic accuracy and clinical utility of PSMA-SPECT/CT.
The aim of this study was to evaluate the performance of [99mTc]Tc-PSMA-I&S-PSMA-SPECT scans in primary diagnostics and biochemical recurrence and restaging of prostate cancer.
Patients and methods
Study population
We examined 21 healthy volunteers and 100 male patients with histologically confirmed prostate cancer.
In patient group 1, we retrospectively analysed the PSMA-SPECT/CT images of a total of 28 patients with prostate cancer prior to any definitive treatment. Inclusion criteria were histologically confirmed prostate cancer and the availability of at least 6 months of patient history after PSMA-SPECT/CT scans. Patients undergoing restaging for recurrent disease were excluded.
As a control group, we used the data of 20 healthy volunteers who underwent PSMA-SPECT/CT examination. Prior to SPECT/CT investigation, control subjects underwent routine urological examination. Based on pre-scan examination and follow-up clinical data control, volunteers did not have prostate cancer nor had evidence of any prostate or malignant disease.
In all, 72 patients were enrolled in patient group 2. Inclusion criteria were histologically confirmed prostate cancer (needle biopsy or histology after surgical procedure); completed primary treatment (radical prostatectomy or radiation therapy) or systemic therapy in advanced stages (androgen receptor targeted- or chemotherapy, combined with androgen deprivation therapy); biochemical recurrence [detectable prostate-specific antigen (PSA) value measured >6 weeks after prostatectomy or a PSA of 2 or more ng/mL rise above nadir following radiation therapy]; or progressive disease (two new lesions on the first follow-up bone scan and confirmatory bone scan at least 6 weeks later or progression based on RECIST (Response Evaluation Criteria in Solid Tumours) criteria for non-bone lesions) and the availability of at least 6 months of patient history after PSMA-SPECT/CT scans.
For all subjects, a relevant medical history and information about previous therapies were recorded.
Follow-up
After PSMA-SPECT/CT, patients were followed up for at least 6 months. Results of the histopathological report, focal radiation therapy response assessment by morphological [multiparametric magnetic resonance imaging (MRI), CT] and functional (bone scintigraphy) imaging methods and PSA monitoring were used. Patients were contacted regularly to obtain follow-up information.
Clinical data of patients are summarized in Table 1.
Study population characteristics.

iPSA, initial prostate-specific antigen level; IQR, interquartile range; ISUP, International Society of Urological Pathology; PCa, Prostate cancer; PSA, prostate-specific antigen level.
Radiosynthesis of [99mTc]Tc-PSMA-I&S
Synthesis of PSMA-I&S has been previously reported by Robu et al. 18 [99mTc]Tc-PSMA-I&S kit was labelled with 5.7 ± 0.88 GBq of [99mTc]Pertechnetate. Radiochemical purity tests were performed by instant thin-layer chromatography on silica gel (Butan-2-one was used as the mobile phase). The mean radiochemical purity was 99.6 ± 0.4%.
PSMA-SPECT/CT image acquisition protocol and image analysis
Mean activity of 666 ± 102 MBq [99mTc]Tc-PSMA-I&S (Institute of Isotopes Co. Ltd, Budapest, Hungary) was administered intravenously. Prior to imaging, patients were given an oral contrast agent (1000 mL of polyethylene glycol solution) to drink continuously, starting 60 min before the examination to promote bowel distention without introducing contrast material-induced attenuation correction artefacts. No adverse effects were observed in any of the patients after tracer injection. All scans were performed on an integrated whole-body SPECT/CT system (Mediso AnyscanTRIO; Mediso Medical Imaging Systems Ltd, Budapest, Hungary). Whole body SPECT imaging was carried out 6 h after the administration of the radiopharmaceutical (360°; 96 projections, 10 s/frame, matrix: 128 × 128, pixel: 4.22 mm). SPECT data collection was completed by low-dose CT (120 kV and 70 mAs) acquisition. Head–neck region imaging is conducted with a single field of view (FOV) measuring 40 cm. For torso imaging, the range extends from the supraclavicular region down to the mid-thigh, encompassing 2–3 FOVs (2–3 × 40 cm), with an overlap of at least 5 cm. The choice of 2 or 3 FOVs depends on the height of the patient.
PSMA-SPECT/CT images were visually evaluated for the presence of pathological radiopharmaceutical uptake by consensus reading of two nuclear medicine physicians with at least 20 years of experience. Physiological PSMA ligand uptake was found in the lacrimal gland, salivary glands, liver, spleen, small intestine, colon and kidneys. Patients were considered positive in the presence of markedly increased prostatic radiotracer uptake or at least one focal area of non-physiological PSMA expression in any region on SPECT scans.
The PSMA expression of pathological lesions was assessed by measurement of the maximum activity concentration [kBq/mL] in attenuation-corrected reconstructed images in each patient. The radiopharmaceutical uptake of the whole prostate gland in healthy volunteers was also measured.
As a reference, we used the mean activity concentration of gluteal muscles, aortic arch and healthy liver tissue. To obtain these values, at least 30 cm 3 of volume of interest (VOI) was defined on SPECT scans without any visible abnormalities on CT.
For patients with biochemical recurrence or progressive disease, detection rates were calculated, defined as the proportion of scans with at least one PSMA-positive lesion.
Statistical analysis
Patient-based diagnostic performances (sensitivity, specificity, overall accuracy) of PSMA-SPECT/CT were calculated based on post-treatment follow-up data.
A PSMA-SPECT/CT scan was considered as true positive if a biopsy, a histopathological report, or follow-up routine control imaging examinations (i.e. MRI, bone scan, CT scan) confirmed the results, or patients had consistent decrement of serum PSA values after focal radiation therapy.
Despite the evidence of biochemical recurrence or the presence of clinically proven prostate cancer lesions, PSMA-SPECT scans without pathological tracer uptake were considered false negatives.
Healthy volunteers without the presence of pathological tracer uptake and with a negative scan were considered true negatives in a primary setting. Patients without the presence of pathological tracer uptake on PSMA-SPECT and with no clinical evidence of metastatic disease were considered true negatives in the assessment of secondary involvement.
Positive PSMA-SPECT/CT scans without clinical or histological evidence of prostate cancer lesions were counted as false positives.
The Mann–Whitney U test was conducted to compare the relative radiopharmaceutical uptake between the primary prostate cancer group and healthy volunteers. p Value < 0.05 was considered statistically significant.
All statistical analyses were performed using IBM SPSS Statistics 24 (IBM Corp., New York, NY, USA).
Results
Primary prostate cancer
Patient-based diagnostic performance for detecting primary prostate cancer is as follows: sensitivity, specificity, positive predictive value, negative predictive value and accuracy of PSMA-SPECT/CT was 86%, 100%, 100%, 83% and 92%, respectively.
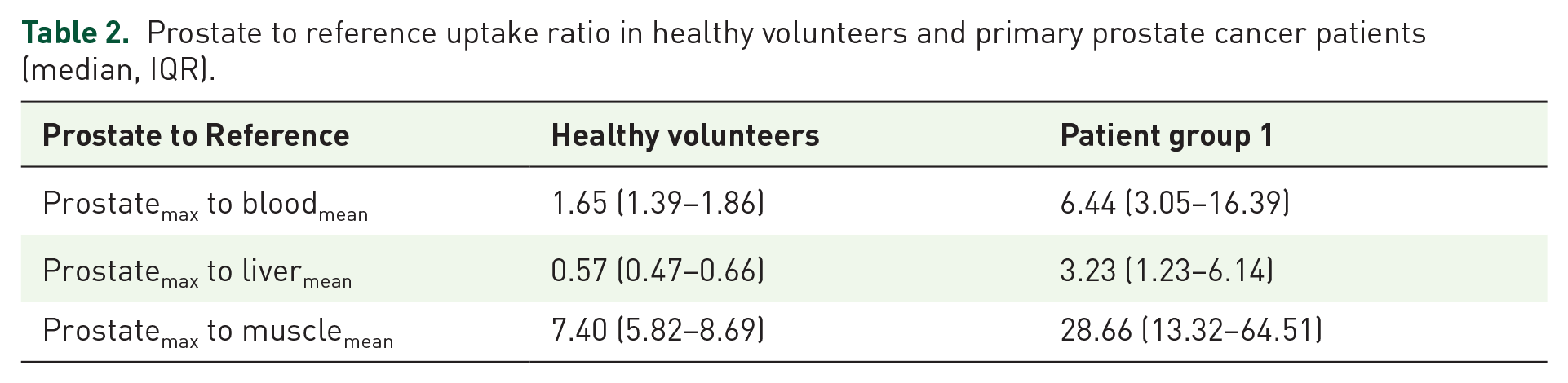
The radiopharmaceutical uptake of primary prostate cancer was significantly higher than that of healthy prostate tissue (p = 0.001) (Table 2). Figures 1 and 2 show representative PSMA-SPECT/CT images of a healthy volunteer and a primary prostate cancer patient.
Prostate to reference uptake ratio in healthy volunteers and primary prostate cancer patients (median, IQR).

[99mTc]Tc-PSMA-SPECT/CT scan of a 71-year-old healthy volunteer. The prostate shows homogeneous low radiopharmaceutical uptake.
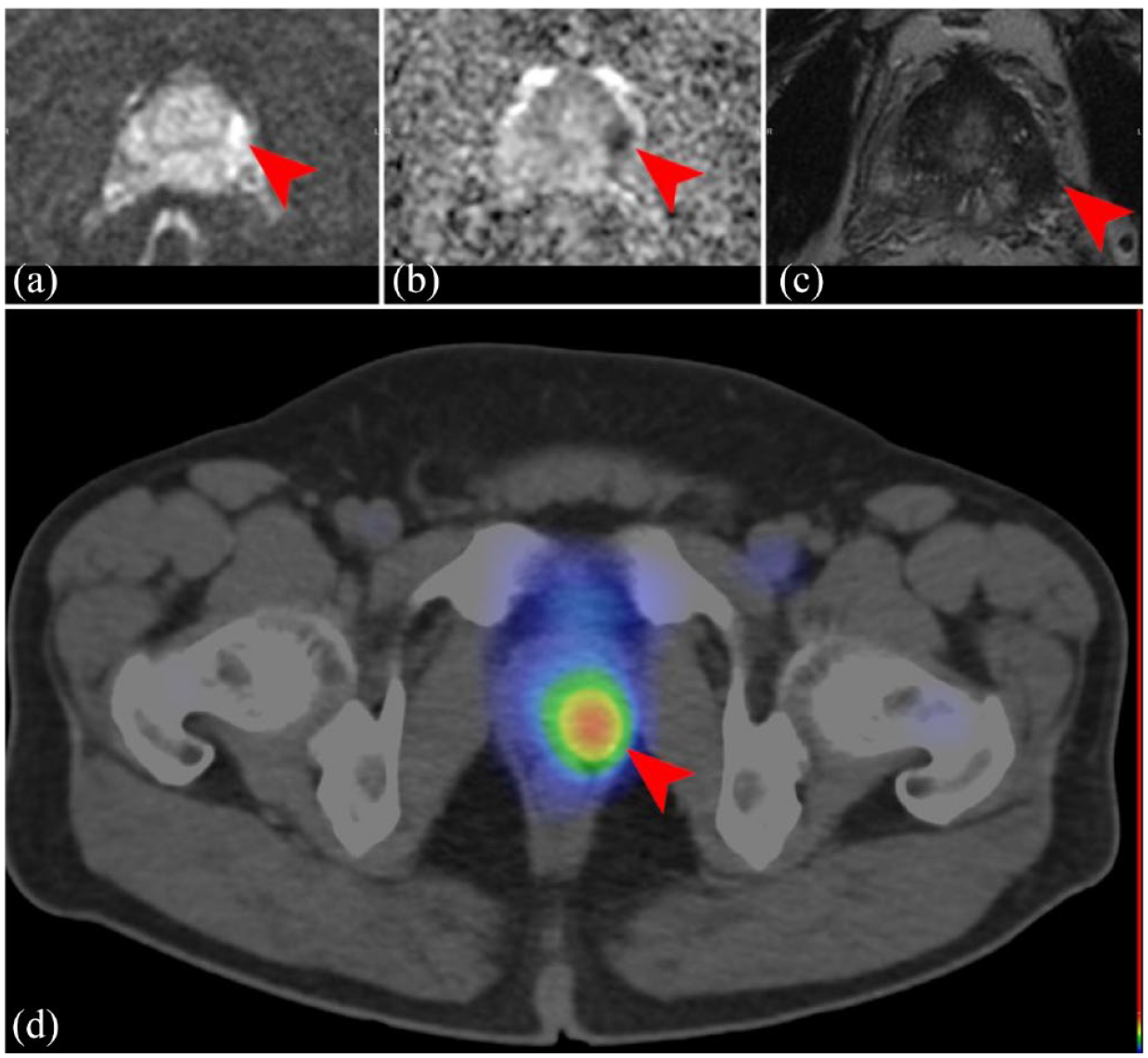
MRI and PSMA-SPECT/CT scan of a 59-year-old patient with primary prostate cancer (ISUP V/V.; PSA 19.20 ng/mL). The left posterolateral peripheral zone of the prostate demonstrates 16 mm mass with increased signal intensities (a) on the DWI images with focal ADC decrease (b) and decreased signal intensities on the T2w images (c), PSMA-SPECT/CT images (d) show increased radiopharmaceutical uptake in the same region (red arrowheads).
Primary staging (N, M)
In patient group 1, patient-based diagnostic performance is as follows: sensitivity, specificity, positive predictive value, negative predictive value and accuracy of PSMA-SPECT/CT for detecting metastases in primary staging were 88%, 100%, 100%, 85% and 93%, respectively.
One or more extraprostatic lesions were found in 15 (54%) patients. Overall, 49 PSMA-positive metastases were evaluated: local lymph node, n = 7 (14%); distant lymph node, n = 6 (12%); bone metastases, n = 34 (69%); and visceral metastases, n = 2 (4%).
Distant metastases and positive lymph node status were confirmed by conventional imaging modalities (bone scan, CT, MRI). For two patients, MRI found metastatic lesions despite the negative PSMA scan.
Six of these lesions (12%) had higher activity than blood, but lower than liver uptake, 43 of them (88%) showed higher activity than liver tissue.
The average short-axis diameter of 13 PSMA-positive lymph nodes was 8.5 ± 3.6 mm (5–17), and 76% (n = 13) of them were smaller than 10 mm.
Biochemical recurrence and restaging
In patient group 2, PSMA-SPECT/CT patient-based sensitivity was 72%.
In all, 12 patients received salvage radiotherapy to the prostate bed with pelvic lymph node regions and 5 patients received systemic treatment after a PSMA scan. In these patients, local recurrence or pelvic lymph node involvement could not be clearly distinguished only metastatic involvement could be confirmed (one case) so data from these patients were not included in the following calculations. This way, patient-based sensitivity, specificity, positive predictive value, negative predictive value and accuracy for local recurrence were 67%, 100%, 100%, 86% and 89%, and for detecting metastases 91%, 92%, 98%, 75% and 91%, respectively.
The overall detection rate was 71% (51/72) of patients with biochemical recurrence or progressive disease. The detection rate at PSA levels of 1 ng/mL or less was 37% (average PSA level of 0.44 ng/mL) and at 1 < PSA < 5 ng/mL was 74% (average PSA level of 2.8 ng/mL). The detection rate was 80% in patients with PSA levels >5 ng/mL.
Pathological tracer uptake in the prostatic fossa was found in 17 patients (23%). PSMA-positive local recurrences were confirmed histologically in six cases. For the other 11 patients, good therapeutic response (consistent decrement of serum PSA values after focal radiation therapy) or routine control MRI imaging confirmed local recurrence.
Semi-quantitative analysis of 17 PSMA-positive local recurrences showed higher radiopharmaceutical uptake than liver tissue in 10 cases (59%), lower than liver but higher than blood pool activity in seven cases (41%).
At least one extraprostatic lesion was found in 40 (56%) patients: local lymph node, n = 18 (25%); distant lymph node, n = 17 (23%); bone metastases, n = 21 (29%); and visceral metastases, n = 6 (8%). PSMA-positive metastatic diseases were confirmed histologically (biopsy or surgical specimen) in 11 cases. In the other 29 cases, we used follow-up clinical data to confirm our results. A total of 81/111 (73%) lesions had higher activity than normal liver tissue.
The average short-axis diameter of 75 PSMA-positive lymph nodes was 9.4 ± 4.4 mm (4–28), and 71% (n = 53) of them were smaller than 10 mm.
Figure 3 represents a case of a patient referred for a PSMA scan due to newly discovered suspected liver metastasis.

PSMA SPECT/CT – axial (a–c); coronal (d) and sagittal slices (e) – scan of 82-year-old metastatic prostate cancer patient (ISUP V/V.; PSA: 618 ng/mL) with newly diagnosed liver lesions by ultrasound. The PSMA SPECT/CT proved high PSMA expression in the hepatic lesions indicative of prostate cancer metastases. Multifocal bone metastases on the spine and pelvic bone and several moderately enlarged lymph nodes with high PSMA density were shown as well. Total liver tumour burden 320 mL.
Discussion
In this retrospective single-centre study, [99mTc]Tc-PSMA-I&S was used for detecting primary prostate cancer, primary staging and restaging in biochemical recurrence or case of suspected disease progression. Although PSMA-I&S was originally developed for radio-guided surgery purposes, it was found to be a suitable radiotracer for prostate cancer imaging, as 6 h post-injection scans showed high contrast and proper image quality. There are some advantages of PET/CT compared to SPECT/CT: PET/CT typically offers slightly higher spatial resolution (dependent on the specific devices used) and shorter uptake times (in this case 6 versus 1–2 h). During the current examination, the acquisition time averaged 35 min (median), which is comparable to the duration of most PET examinations commonly employed in general practice, though it may be longer than what is achieved with more recent PET camera technology. 19
This technique can be utilized in nuclear medicine departments where PET/CT or PSMA-PET tracers are not available. Simple and reliable radiolabelling procedures facilitate the use of this radiopharmaceutical so PSMA-SPECT/CT can be easily integrated into routine diagnostic practice.
Primary prostate cancer
The main purpose of PSMA imaging in the diagnosis of primary prostate cancer is not to detect the primary tumour, but it appears that PSMA-PET or even SPECT can discriminate between healthy and cancerous tissues based on the limited evidence available. In our study, [99mTc]Tc-PSMA-I&S-SPECT/CT demonstrated high sensitivity (86%) for detecting primary prostate cancer. Werner et al. reported 92% sensitivity in a smaller patient cohort for primary tumour (12/11 patients), so far this is the only comparable study with PSMA-I&S. Other 99mTc-labelled PSMA ligands (MIP-1404 and HYNIC (Hydrazinonicotinic acid)-PSMA) shown 94–100% sensitivity for detection of primary prostate cancer.13,20 It should be noted that 100% sensitivity of HYNIC-PSMA was demonstrated in a smaller number of patients (n = 10). In the case of MIP-1404, a higher detection rate may be caused by the better tumour to background uptake ratio (37.67 ± 52.60 versus 110.9 ± 100.5). PSMA-I&S has relatively high blood and background activity due to high plasma protein binding and higher consent rate of hepatobiliary clearance due to increased lipophilicity of the radiopharmaceutical. 18
More data are available about PET radiotracers. According to a recent meta-analysis, PSMA-PET/CT has high diagnostic accuracy but only moderate specificity. 21 Authors explain this moderate specificity using background prostate activity as the threshold for determining pathological findings in many of the studies.22–24
An increasing number of papers show PSMA-PET can facilitate a better definition of intraprostatic foci of prostate cancer and could help targeted biopsies and surgical treatment planning or focal therapy. The prospective multicentre clinical trial PRIMARY found that combined PSMA-PET with MRI improved negative predictive value and sensitivity compared with MRI alone in primary prostate cancer. 25
Primary staging (N, M)
PSMA-PET imaging has proved its advantage over conventional methods in primary staging.10,26–28 In this study, we demonstrate that even PSMA-SPECT/CT is a reliable and well-usable non-invasive imaging method in primary staging. Less data published about the diagnostic accuracy of PSMA-I&S in primary staging. 99mTc-labelled small molecule PSMA ligand, MIP-1404 showed a low sensitivity (50%), but good specificity (87%) at the patient level in detecting lymph node metastases in histologically proven cases. 13 We found higher sensitivity (88%) and 100% specificity for detecting metastases in the primary setting. These data are not fully comparable to our results because we used different (composite) reference standards; additionally, sensitivity and specificity were not calculated separately for bone and lymph node metastases. Lawal et al. 29 compared PSMA-PET/CT with PSMA-SPECT/CT for 14 patients and demonstrated 78.3% overall per-lesion sensitivity (62.5% lymph node, 91.7% bone metastases) of [99mTc]Tc-HYNIC-PSMA-SPECT/CT. They found that SPECT/CT is less sensitive in smaller lesions, only 28% of nodes <10 mm were detected. 29 In our study, the average short-axis diameter of detected PSMA-positive lymph nodes was 8.2 mm, and 76% of them were smaller than 10 mm. It should be mentioned that these lesions fall below the size criteria for lymph node involvement detected by conventional CT imaging or MRI. Pooled data of 244 patients in five studies demonstrated that PSMA-PET/CT has a 77% (33–100%) per-patient sensitivity and 97% (80–100%) per-patient specificity for the detection of lymph node metastasis of prostate cancer. 5 Our data suggest that the difference between PSMA-SPECT diagnostic performance and PSMA-PET in primary N, M staging is not remarkable.
Biochemical recurrence and restaging
In this study, PSMA-SPECT/CT was found to be a useful tool for restaging patients with progressive disease or with biochemical recurrence of prostate cancer. We found that PSMA-SPECT/CT has moderate (67%) sensitivity but high specificity (100%). Most of the PSMA radiopharmaceuticals [99mTc]Tc-PSMA-I&S is excreted primarily by the urinary system. Compared to the other small molecule PSMA ligands it is more lipophilic and has a higher consent rate of hepatobiliary clearance which led to increased intestinal activity. Due to physiologically high bladder or rectum activity, detection of pathological uptake can be difficult in a prostate bed and can explain moderate sensitivity. Five of the six false-negative local recurrences (83%) were in patients who underwent radical prostatectomy. Perera et al. 5 in their meta-analysis of PSMA-PET studies of 4790 patients, found a significantly higher proportion of positivity (52% versus 22%) in the prostate bed for those who underwent radiotherapy versus prostatectomy. This may be due to an unfavourable anatomical situation caused by the surgical intervention. Based on the data available so far, diagnostic accuracy of PSMA imaging in local recurrence could be further improved by the administration of diuretics, or contrast agents, or multi-time point or dynamic imaging, but there is no clear consensus about these premedications.30,31 In our investigations, we did not make use of them.
68Ga- or even 18F-PSMA-PET/CT has been used widely to assess prostate cancer metastases, particularly at the time of biochemical recurrence. Pienta et al., 32 in their prospective multicentre study, found that 93 patients with suspected recurrent/metastatic prostate cancer demonstrated excellent sensitivity (95.8%) and positive predictive value (81.9%) for detecting extraprostatic lesions. This is comparable to our results.
As expected, the detection rate increased along with the PSA values. We found detection rates of 37% at a PSA level of 1 ng/mL or less, 74% at a PSA level of 1–5 ng/mL and 90% above 5 ng/mL. Based on currently available data, PSMA-SPECT/CT detection rate ranged from 20% to 58% at PSA <1 ng/mL, 55% to 80% at PSA 1–4 ng/mL and 83% to 100% above 4 ng/mL.12,14,16 Our results were in good agreement with these data. According to a meta-analysis by Perera et al., percentages of positive PSMA-PET scans are higher than the PSMA-SPECT data showed. They reported 33%, 45%, 59%, 75% and 95% positive rates for PSA categories 0–0.19, 0.2–0.49, 0.5–0.99, 1–1.99 and ⩾2 ng/mL, respectively. 5
In comparison with other 99mTc-labelled PSMA compounds, PSMA-I&S has a higher tumour to background ratio than EDDA-HYNIC-iPSMA. 20 However, these ratios are not exactly comparable because reference VOIs were different. Schmidkonz et al. examined MIP-1404 in a larger group of patients with biochemical recurrence of prostate cancer. The patient characteristics (age Gleason-score; PSA level) of our cohort were quite similar. They found that 162 PSMA-positive lesions yielded an average tumour to normal ratio of 146.6 ± 160.5, ranging from 1.9 to 1482.4. PSMA-I&S also demonstrated a high tumour-to-background ratio as 81/111 (73%) lesions had higher activity than the liver. In comparison, the liver shows approximately 10 times higher radiopharmaceutical uptake than the gluteal muscle. 14
By the pharmacokinetic nature of the PSMA-I&S combined with the lower spatial resolution of SPECT, this method is less sensitive than PET-CT/MR in identifying smaller lesions, such as local recurrences especially after radical prostatectomy, in early relapse with low PSA values. In these selected cases, PSMA-PET could be more sensitive and can provide additional valuable diagnostic information. But PSMA-SPECT can exclude extrapelvic lymph nodes, bone or visceral metastases which is essential to determining the necessity of salvage radiation therapy.
New PSMA radioligand therapies that have emerged in recent years are now available for the treatment of prostate cancer. 33 Although PSMA-SPECT/CT has not yet undergone full validation, it is a reasonable option for patients when considering PSMA-SPECT, akin to its PET-based counterparts. PSMA exhibits the ability to effectively detect metastatic lesions in the pre-PSMA-targeted radioligand therapy metastatic castration-resistant prostate cancer (mCRPC) space, all while offering advantages such as reduced financial burden and lower radiation exposure.34–36 This positions it as an optimized tracer for the selection of mCRPC patients who are candidates for PSMA-based radioligand therapy, particularly in regions with resource constraints. In cases involving high PSA levels, its diagnostic performance remains favourable.
Limitations
This is a single-centre retrospective study that reduces the impact of these findings. PSMA-PET/CT would have been the ideal reference for assessing the clinical performance of PSMA-SPECT/CT. However, it is worth noting that during our study, PSMA-PET/CT was not accessible to our patients, even at the national level. Therefore, akin to the approach taken in the ProPSMA 4 study, we relied on clinical follow-up and the findings from conventional imaging as our reference points. Histopathology was not available for all lesions. Under these circumstances, treatment follow-up, based on imaging results and PSA monitoring, could confirm our results. Only one-time imaging was performed; dynamic and late-phase acquisitions were not conducted.
According to our data, [99mTc]Tc-PSMA-I&S can be easily integrated into routine diagnostic practice, and it provides usable data in both primary staging and restaging of prostate cancer. Preliminary data show that the quantitative assessment of PSMA-SPECT/CT scans has the potential to be used to differentiate between physiological and pathological intraprostatic tracer uptake. It can be broadly applied for primary and restaging in biochemical recurrence or progressive disease. Further studies with extensive histopathological evaluation and direct comparison with PSMA-PET are needed for better clarification of the clinical impact of PSMA-SPECT/CT.