
Abstract
Background:
Systemic inflammatory markers draw great interest as potential blood-based prognostic factors in several oncological settings.
Objectives:
The aim of this study is to evaluate whether neutrophil-to-lymphocyte ratio (NLR) and pan-immune-inflammation value (PIV) predict nodal pathologic complete response (pCR) after neoadjuvant chemotherapy (NAC) in node-positive (cN+) breast cancer (BC) patients.
Design:
Clinically, cN+ BC patients undergoing NAC followed by breast and axillary surgery were enrolled in a multicentric study from 11 Breast Units.
Methods:
Pretreatment blood counts were collected for the analysis and used to calculate NLR and PIV. Logistic regression analyses were performed to evaluate independent predictors of nodal pCR.
Results:
A total of 1274 cN+ BC patients were included. Nodal pCR was achieved in 586 (46%) patients. At multivariate analysis, low NLR [odds ratio (OR) = 0.71; 95% CI, 0.51–0.98; p = 0.04] and low PIV (OR = 0.63; 95% CI, 0.44–0.90; p = 0.01) were independently predictive of increased likelihood of nodal pCR. A sub-analysis on cN1 patients (n = 1075) confirmed the statistical significance of these variables. PIV was significantly associated with axillary pCR in estrogen receptor (ER)−/human epidermal growth factor receptor 2 (HER2)+ (OR = 0.31; 95% CI, 0.12–0.83; p = 0.02) and ER−/HER2− (OR = 0.41; 95% CI, 0.17–0.97; p = 0.04) BC patients.
Conclusion:
This study found that low NLR and PIV levels predict axillary pCR in patients with BC undergoing NAC.
Registration:
Eudract number NCT05798806.
Keywords
Introduction
Approximately 10–15% of breast cancer (BC) patients have evidence of extensive axillary nodal involvement at diagnosis. 1 These patients are usually offered neoadjuvant chemotherapy (NAC) to improve survival, increase local control, and strive for a de-escalation of axillary surgery in case of nodal response after treatment.
Depending on the tumor subtype, an axillary pathologic complete response (pCR) is achieved in 20–70% of initially node-positive (cN+) patients.2–6 This rate is as high as 74% in human epidermal growth factor receptor 2 (HER2)-positive BC patients treated with NAC and concurrent trastuzumab.7,8
When cN+ patients convert to clinically node negative (cN0), axillary lymphadenectomy (ALND) can be replaced by less invasive surgical approaches.9,10 In these cases, sentinel lymph node biopsy (SLNB) is performed as an alternative to ALND in several Institutions. However, relatively high false-negative rates are reported in different validation trials, thus questioning the decision not to have ALND.11–14 A large meta-analysis on 13 studies including over 1900 women documented a false-negative rate exceeding 10% for the SLNB technique in this setting. 15 A recent international EUBREAST survey among 349 international Breast Units demonstrated that standard ALND or target ALND is still the preferred approach in these patients. 16 In 2021, our group developed and validated a post-NAC predictive nomogram to select cN+ BC patients with a low risk of residual axillary disease after NAC in whom axillary surgery could be minimized. 17 To date, there are no validated tools to identify, before NAC, patients who are most likely to undergo node conversion.
Inflammatory response plays an important role in the development and progression of cancer. 18 The neutrophil response suppresses tumor surveillance activity of the cytotoxic T cells, thereby increasing malignant potential.19,20 Thus, the status of systemic inflammation before any treatment could provide useful a priori information on the likelihood of response to NAC.
In the last years, the predictive value of the blood-derived inflammation indexes, particularly the neutrophil-to-lymphocyte ratio (NLR), in NAC response has been increasing.21,22
Pan-immune-inflammation value (PIV) is a relatively novel biomarker integrating different peripheral blood immune cell subpopulations (neutrophil, platelet, monocyte, and lymphocyte) and has been reported as a promising predictor of long-term outcomes in cancers because it can precisely reflect the inflammatory and immune status of patients with malignancy.23,24
However, no solid data regarding the potential role of these biomarkers in predicting nodal pCR in cN+ BC patients undergoing NAC are currently available.
The aim of our study is to investigate whether pretreatment NLR and PIV can predict axillary pCR and thus be helpful in selecting those patients who are most likely to undergo node conversion under NAC.
Materials and methods
Study type and design
This is a multicentric, retrospective observational study, promoted and coordinated by the Breast Unit of Istituti Clinici Scientifici Maugeri IRCCS of Pavia (Italy). It was approved by the Ethical Committee of the coordinating Institution (Eudract number NCT05798806) and by the Ethical Committees of all the participating centers. Informed consent was signed by patients during admission to the Institute. A total of 10 Italian centers and 1 Swiss major Breast Units were involved in the study. Data were collected in a General Data Protection Regulation (GDPR)-compliant ad-hoc database accessed only by the study investigators. The aim of the study was to explore whether NLR and PIV were independent factors of axillary pCR after surgery, combined with all relevant clinical preoperative variables, in a cohort of BC patients treated with NAC.
Study population
Included patients were aged ⩾18 years, with histopathological diagnosis of invasive BC at core biopsy, clinical evidence of node metastasis, absence of distant metastasis at diagnosis, and they were treated with NAC and subsequent surgery. The enrollment years range from 2004 to 2020. cN+ disease was evaluated both clinically and by imaging (including ultrasound and/or magnetic resonance imaging and/or positron emission tomography), with or without a fine-needle aspiration cytology or core biopsy. A clinical and radiological re-assessment of the axilla was performed after NAC. NAC regimens agreed with standard clinical practice and were categorized in four groups: (1) anthracyclines/fluorouracil, epirubicin hydrochloride, and cyclophosphamide (FEC) (Type1), (2) anthracyclines/FEC + taxanes (Type2), (3) anthracyclines/FEC + taxanes + anti-HER2 (Type3), (4) all other particular types (Type4), where FEC is the combination of fluorouracil, epirubicin hydrochloride, and cyclophosphamide.
Analysis of inflammatory biomarkers
Blood counts obtained within the 2 weeks preceding NAC treatment were retrieved from the hospitals’ clinical data repository and included in the analysis. The absolute count of lymphocytes, neutrophils, monocytes, and platelets were collected and, if the leukocyte formula was expressed as a percentage of total white blood cells, cell counts were calculated starting from the total leukocyte concentration. Units of measure were standardized among centers and expressed as a number of cells/L. From laboratory data, the following parameters were calculated as inflammatory biomarkers: (1) NLR; (2) PIV: (monocyte * platelet * neutrophil) to lymphocyte ratio. Every biomarker value was graded as ‘low’ and ‘high’, according to optimal cutoff points determined from the receiver operating characteristic (ROC) analysis. These thresholds were calculated on a sample’s subset (n = 204 patients) and then analyses were conducted on the remaining cohort to consider a training set for cutoff determination and a development-independent set for multivariate analysis. A geographic criterion was adopted to select a set for thresholds’ identification.
Evaluation of clinical and pathological response
After NAC completion and before surgery, all patients were re-staged by clinical evaluation, digital mammography, breast and axillary ultrasound, and/or other imaging techniques to evaluate clinical response to chemotherapy treatment. Based on the clinical response of primary BC, breast-conserving surgery or total mastectomy was planned as appropriate. Axillary clinical response was evaluated based on the presence or absence of abnormal/enlarged lymph nodes (focally or diffusely >3 mm thickened cortex, deformed/absent fatty hilum).25,26 Based on axillary clinical response, patients were treated either by ALND or by SLNB. If isolated tumor cells, micro- or macro-metastases were identified in the sentinel lymph nodes, a complete axillary dissection was performed. Axillary pCR was defined as no micro- or macro-metastases in any excised lymph node (ypN0/isolated tumor cells+). 27
Statistical analyses
A preliminary outliers’ analysis of the selected sample was conducted. Steps were taken to identify those patients with biomarker values outside the adequacy range (extreme outliers 28 ), calculated as follows: biomarker value ⩾ 3 * biomarker IQR + biomarker Q3, where IQR = interquartile range and Q3 = 75th percentile. Variables were reported as median and IQR or as absolute numbers and percentages. Categorical variables were compared using the χ2 test, while continuous variables were compared using Student’s T test or nonparametric Wilcoxon test in case of non-normal distribution of the variable. Statistical significance was set at p < 0.05 (two-tailed).
A ROC analysis with relative area under curve was implemented to assess the optimal cutoffs for each blood biomarker. A multivariate analysis with a binomial logistic model was performed, the Akaike information criterion (AIC) was evaluated to select the appropriate number of variables, and the model performance measure given by explained variance (coefficient of determination R2) was assessed, using the definition proposed by Nagelkerke (N–R2). Data analysis was performed using SAS software (v. 9.4, SAS Institute Inc., Cary, USA) and R software (v. 3.5.1, © The R Foundation, Vienna, Austria).
Results
Baseline characteristics of the study population
A total of 1287 BC patients who met the inclusion criteria and had available pretreatment blood counts were considered for the study. Data missing were less than 9% of all information. Supplemental Table S1 shows the variables’ baseline distribution of the entire cohort. Baseline NLR and PIV were calculated from pre-NAC blood counts for each patient. From the outliers’ analysis, n = 13 patients were excluded due to their extreme values. The resulting sample consisted of n = 1274 BC patients and this was the cohort considered in the subsequent analysis. Clinical features and chemotherapy/surgical treatment are reported in Table 1. Axillary pCR was achieved in 586 (46%) patients. The median age at the diagnosis was 50 (IQR: 25–91) years in patients who achieved axillary pCR, and 52 (IQR: 25–85) in ypN+ patients; 70.5% of ypN0 patients had a negative post-NAC axillary clinical/radiological status, while, in ypN+ group, 61.2% of patients had a positive post-NAC axillary status. Most patients who achieved axillary pCR were estrogen receptor (ER)+/HER2+ (30.3%) while the majority of no-pCR cases were ER+/HER2− (58.6%) and 58.5% of patients who achieved axillary pCR showed also breast pCR. In the whole cohort, 428 patients (33.6%) experienced breast pCR at final histopathology, of them 342 patients (79.9%) achieved axillary pCR too. Finally, concentrations of the different immune cells (neutrophils, lymphocytes, monocytes, and platelets) were reported in Supplemental Table S2 to present the immune infiltrate general distribution in the study’s cohort.
Baseline features of the patients with or without axillary pCR.

Assessed on core biopsy before NAC.
Assessed before neoadjuvant treatment.
BMI, body mass index; cCR, complete clinical response; ER, estrogen receptor; FEC, fluorouracil, epirubicin hydrochloride, and cyclophosphamide; HER2, human epidermal growth factor receptor 2; IQR, interquartile range; Med., median; NAC, neoadjuvant chemotherapy; NLR, neutrophil-to-lymphocyte ratio; pCR, pathological complete response; PIV, pan-immune-inflammation value; SLNB, sentinel lymph node biopsy.
Inflammatory biomarkers predicting axillary pCR
The optimal cutoff values of NLR and PIV were calculated based on the analysis of the ROC curves for the prediction of axillary pCR (Supplemental Table S3 and Figures S1, S2). A multivariate logistic regression was performed (NLR: AIC = 947.7 and N–R2 = 0.36; PIV: AIC = 813.2 and N–R2 = 0.37) taking into account categorized blood-derived inflammatory markers together with patient’s age, clinical T stage, histological type, grading, biomolecular subtype, Ki67 level, and progesterone receptor status at core biopsy pre-NAC, NAC regimen, post-NAC clinical or radiological axillary re-staging and post-NAC breast clinical complete response (cCR).
Results reported in Table 2 showed that NLR and PIV were separately independent predictors of axillary pCR. Beyond the pretreatment NLR and PIV, other independent predictors for axillary response were age, histological type, biomolecular subtype, Ki67 levels, progesterone receptor status, and clinical or radiological axillary re-staging and breast cCR post-NAC.
Multivariate analysis of inflammatory biomarkers and clinical characteristics related to axillary pCR (ypN0). Comparison ypN0 versus ypN+ (computed the probability of ypN0).

Assessed before neoadjuvant treatment.
Assessed on core biopsy before NAC.
cCR, complete clinical response; ER, estrogen receptor; FEC, fluorouracil, epirubicin hydrochloride, and cyclophosphamide; HER2, human epidermal growth factor receptor 2; NAC, neoadjuvant chemotherapy; NLR, neutrophil-to-lymphocyte ratio; OR, odds ratio; pCR, pathological complete response; PgR, progesterone receptor; PIV, pan-immune-inflammation value; Type1, anthracyclines/FEC; Type2, anthracyclines/FEC + taxanes; Type3, Anthr/FEC + taxanes + anti-HER2; Type4, other types.
From the whole patients’ dataset, separate multivariate analyses were performed for the four different BC biomolecular subtypes obtained on the immunohistochemical characterization conducted on the core biopsy before NAC. Results reported in Supplemental Materials (Tables S4–S7) showed that PIV was an independent predictor of axillary pCR in ER−/HER2+ [Supplemental Table S6, odds ratio (OR) = 0.31; 95% CI, 0.12–0.83; p = 0.02] and ER−/HER2− (Supplemental Table S7, OR = 0.41; 95% CI, 0.17–0.97; p = 0.04) subtypes while NLR was not an independent factor for axillary pCR in any specific biomolecular subtypes.
Inflammatory biomarkers predicting axillary pCR in patients with cN1 before NAC
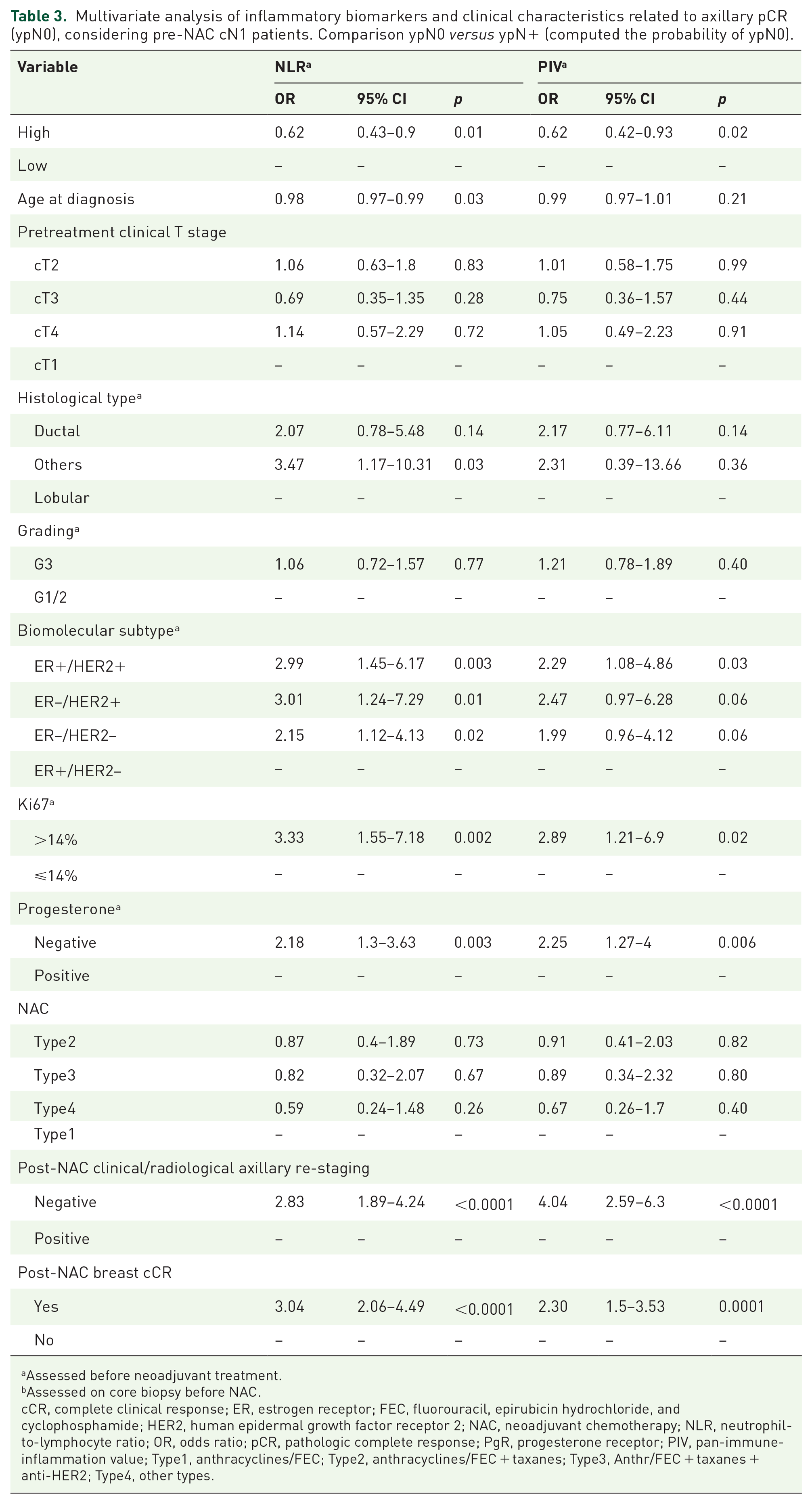
To further investigate the role of NLR and PIV in the evaluation of axillary pCR, we selected patients with clinical N = 1 stage (cN1) before NAC (n = 1075). Excluding patients used to calculate ROC optimal cutoff, a multivariate analysis was conducted on this patients’ subset (NLR: AIC = 779.3 and N–R2 = 0.37; PIV: AIC = 656.5 and N–R2 = 0.37). The results reported in Table 3 confirmed NLR and PIV as independent predictors of axillary pCR in cN1 BC patients, with low biomarkers’ levels significantly associated with axillary pCR to NAC (NLR: OR = 0.62; 95% CI, 0.43–0.90; p = 0.01; PIV: OR = 0.62; 95% CI, 0.42–0.93; p = 0.02). Age, histological type, biomolecular subtype, Ki67 level, progesterone status and clinical or radiological axillary re-staging, and breast cCR post-NAC were found as ypN0 independent factors in patients with cN1 assessed on core biopsy before NAC. For all the independent predictive factors retrieved from the multivariate analysis, we reported in Table 4 their distribution in NLR and PIV levels: no statistical significance was found except for a low difference between PIV levels in post-NAC breast cCR categories. These results confirm the independent role of NLR and PIV in predicting axillary pCR.
Multivariate analysis of inflammatory biomarkers and clinical characteristics related to axillary pCR (ypN0), considering pre-NAC cN1 patients. Comparison ypN0 versus ypN+ (computed the probability of ypN0).
Assessed before neoadjuvant treatment.
Assessed on core biopsy before NAC.
cCR, complete clinical response; ER, estrogen receptor; FEC, fluorouracil, epirubicin hydrochloride, and cyclophosphamide; HER2, human epidermal growth factor receptor 2; NAC, neoadjuvant chemotherapy; NLR, neutrophil-to-lymphocyte ratio; OR, odds ratio; pCR, pathologic complete response; PgR, progesterone receptor; PIV, pan-immune-inflammation value; Type1, anthracyclines/FEC; Type2, anthracyclines/FEC + taxanes; Type3, Anthr/FEC + taxanes + anti-HER2; Type4, other types.
Baseline features of pre-NAC cN1 patients with respect to NLR and PIV levels.

Assessed on core biopsy before NAC.
cCR, complete clinical response; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; NAC, neoadjuvant chemotherapy; NLR, neutrophil-to-lymphocyte ratio; PIV, pan-immune-inflammation value.
Discussion
NAC is able to convert cN+ BC patients into cN0 in about 70% of the cases for specific BC subtypes.7,8 For this reason, axillary involvement is usually considered an indication of NAC in most T1–T2 operable BC presenting nodal involvement at diagnosis. Unfortunately, when cN+ does not convert to cN0 after NAC, ALND is recommended. 16 Therefore, the identification of pre-NAC markers that are predictive of axillary response might be useful in selecting those patients who may benefit from chemotherapy in terms of lymph node downstaging.
In the present large multicenter study, two biological markers of systemic immune-inflammation (NLR and PIV) were evaluated as potential predictors of nodal response in a multivariable model, together with some relevant clinical-pathological variables.
NLR is the most extensively studied among inflammatory biomarkers. In primary operable BC, a recent meta-analysis on 42 studies demonstrated that higher NLR was associated with worse overall survival (OS) [hazard ratio (HR) = 1.75, 95% CI, 1.52–2.00; p < 0.001], disease-free survival (HR = 1.67, 95% CI, 1.50–1.87; p < 0.001), and BC-specific survival (HR = 1.89, 95% CI, 1.35–2.63; p < 0.001). 29 In particular, the prognostic role of this systemic inflammatory marker was investigated in some specific subsets where risk stratification is more challenging, like HER2-positive and triple-negative BC. A recent meta-analysis on triple-negative BC suggested that higher NLR is an indicator of poorer prognosis. 30 These data conferred a great interest in this biological marker for timely and noninvasive evaluation of the oncologic outcome.
In the NAC setting, a meta-analysis of eight relevant studies demonstrated that a lower NLR was associated with a greater rate of pCR (OR = 1.83, 95% CI, 1.15–2.91; p = 0.0003). 31 Another subsequent meta-analysis on 19 studies confirmed this result (OR = 1.6, 95% CI, 1.2–2.1; I2 66%; p > 0.001). 32 When specific subsets of BC were explored, NLR provided additional information regarding the likelihood of obtaining a pCR to NAC in postmenopausal Luminal B/HER2-positive 33 and triple-negative BC. 34
Studies on other blood cell ratios such as platelet to lymphocyte ratio and monocyte to lymphocyte ratio showed conflicting results about their value as a predictive and/or prognostic factor and there are conflicting reports about which index provides the best prediction for the efficacy of NAC in BC. 35 However, it has been hypothesized that the combination of multiple biomarkers could better define the patients’ inflammatory status. 36
PIV is a blood-based biomarker integrating different peripheral blood immune cell subpopulations such as neutrophils, platelets, monocytes, and lymphocytes. Due to its potential to represent comprehensively patient’s immunity and systemic inflammation, PIV was proposed as a stronger predictor of outcomes in advanced cancer patients receiving systemic therapies. 23
Two studies focused on PIV analysis reported that this index has a significant predictive value and outperforms other inflammatory biomarkers in predicting OS in HER2-positive advanced BC (HR = 7.96; 95% CI, 2.18–29.09; p < 0.0001) 24 and in predicting pCR to NAC (OR = 3.32; 95% CI, 1.53–7.21; p = 0.002). 37
In this study, we selectively investigated the role of both NLR and PIV in predicting the axillary response in cN+ BC patients undergoing NAC.
Baseline NLR and PIV were calculated in 1274 cN+ BC patients and their cutoff values were identified based on the analysis of the ROC curves for the prediction of axillary pCR. Classical BC poor prognostic factors, including Ki67 over 14%, HER2 positivity, pretreatment advanced T stage, were all associated with axillary clearance in our series. In addition, low NLR and low PIV independently predicted axillary pCR (OR = 0.71; 95% CI, 0.51–0.98; p = 0.04 for NLR; OR = 0.63; 95% CI, 0.44–0.90; p = 0.01 for PIV). PIV was also an independent predictor of axillary pCR in ER−/HER2+ (OR = 0.31; 95% CI, 0.12–0.83; p = 0.02) and ER−/HER2− subtypes (OR = 0.41; 95% CI, 0.17–0.97; p = 0.04).
It is interesting to note that when a sub-analysis was performed on cN1 patients, NLR and PIV were confirmed to be independent predictors of axillary pCR, with low levels of the biomarkers being significantly associated with axillary pCR to NAC (NLR: OR = 0.62; 95% CI, 0.43–0.90; p = 0.01; PIV: OR = 0.62; 95% CI, 0.42–0.93; p = 0.02).
Considering that a pCR in axillary lymph nodes after NAC can be considered an early surrogate marker of the long-term outcome,3,38,39 the identification of pre-NAC predictors of axillary response may provide timely additional information on the oncological outcome. In other words, as future perspective, a patient’s inflammatory phenotype could discriminate a population of newly diagnosed BC patients with poor prognosis. This potential role would be particularly relevant in cN1 BC patients.
Furthermore, in literature, it was clearly demonstrated that the presence of tumor-infiltrating lymphocytes (TILs) in BC, as an expression of intra-tumor immunity, correlates with better response to systemic treatment, a lower recurrence rate, and better OS, regardless of BC subtype.40–44 However, whether the TILs reflect the antitumor immunity status of the patients is still to clarify. A correlation between peripheral indicators of immunity, such as NLR and PIV, and TILs in the microenvironment might be the next step to better define an immune signature of cN+ BC patients who will benefit the most from NAC.
Ideally, if these data are confirmed, a novel axillary immune-oncology algorithm might be designed for cN+ operable BC undergoing NAC to achieve a more precise definition of axillary surgery.
The limits of the study mainly consist of its retrospective nature. Another limitation is that different cutoffs for blood cell ratios are applied in different studies and different patients’ cohorts. Further prospective studies, as well as the definition of reliable and shared cutoff values, are needed to validate the role of inflammatory biomarkers in selecting those patients with a high probability of achieving N0 through NAC.
The strength of this study lies in its multicentric nature (11 major certified Breast Units) and the large sample size (1274 cN+ BC patients). Moreover, there are only a few studies reporting the role of inflammatory biomarkers in predicting axillary pCR, and the majority of literature reports consider a single biomarker and analyze small populations. This is the first study, so far, where two biomarkers were simultaneously evaluated for the prediction of axillary pCR, thus providing a more comprehensive overview of the role of systemic immune inflammation in nodal response to NAC.
Conclusion
In conclusion, our results document that low NLR and low PIV predict axillary pCR in cN+ BC patients undergoing NAC, and results were confirmed also in the sub-analysis on cN1 BC patients. Further prospective trials will be needed to validate the use of these systemic inflammatory markers as clinical indicators of axillary response in nodal-positive BC patients undergoing NAC, for better refinement of axillary surgery.
Supplemental Material
sj-docx-1-tam-10.1177_17588359231193732 – Supplemental material for Low neutrophil-to-lymphocyte ratio and pan-immune-inflammation-value predict nodal pathologic complete response in 1274 breast cancer patients treated with neoadjuvant chemotherapy: a multicenter analysis
Supplemental material, sj-docx-1-tam-10.1177_17588359231193732 for Low neutrophil-to-lymphocyte ratio and pan-immune-inflammation-value predict nodal pathologic complete response in 1274 breast cancer patients treated with neoadjuvant chemotherapy: a multicenter analysis by Maria Luisa Gasparri, Sara Albasini, Marta Truffi, Karin Favilla, Barbara Tagliaferri, Francesca Piccotti, Daniela Bossi, Giulia Armatura, Arianna Calcinotto, Corrado Chiappa, Francesca Combi, Annalisa Curcio, Angelica Della Valle, Guglielmo Ferrari, Secondo Folli, Matteo Ghilli, Chiara Listorti, Stefano Mancini, Peter Marinello, Simone Mele, Anna Pertusati, Manuela Roncella, Lorenzo Rossi, Francesca Rovera, Silvia Segattini, Adele Sgarella, Daniela Tognali and Fabio Corsi in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
The authors acknowledge the Biobank of ICS Maugeri ‘Bruno Boerci’ for support in the management of clinical samples and data.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.