
Abstract
Driver mutations in lung cancer have been generally considered mutually exclusive; however, multiple gene screenings have recently become mainstream. Therefore, it is not uncommon to identify two or more mutations at first diagnosis, making it difficult to determine which tyrosine kinase inhibitor to administer. A 69-year-old woman complaining of back pain was diagnosed with adenocarcinoma T4N3M1c, stage IVB. Although PCR mutation test detected exon21 L858R point mutation by bronchoscopic sample, the therapeutic effect of afatinib was poor. Subsequently, next-generation sequencing (NGS) panel test of a metastasized bone specimen confirmed BRAF V600E. Furthermore, high sensitivity NGS panel system found the gene mutation allele frequency was higher for BRAF V600E than EGFR exon21 L858R for both primary lung tissue and the metastasized specimen. Subsequent BRAF/MEK inhibitor administration showed a remarkable treatment effect. When two or more driver mutations are detected in lung cancer, confirming the allelic frequency of the mutant gene might be useful in selecting more effective agents for front-line treatment.
Introduction
In lung cancer, the presence of driver mutations is considered to be mutually exclusive. 1 However, molecular screening for driver mutations at first diagnosis is becoming more widespread. As a result, the existence of two or more driver mutations for lung adenocarcinoma is gradually becoming known. This is the first report where EGFR major mutation and BRAF V600E mutation were detected in the first diagnostic specimens for both primary and metastatic lesions. Moreover, we report the clinical effect using EGFR-TKI and sequential BRAF/MEK inhibitors, confirming a drastic therapeutic response for the latter agent.
Case report
A 69-year-old woman with a light smoking history was diagnosed with malignant lymphoma at the age of 35, which was successfully treated with chemoradiotherapy. However, an abnormal chest shadow was seen after her latest medical examination. Subsequently, she consulted an orthopedic surgeon due to back pain and was referred to our department on suspicion of bone metastasis from lung cancer. Chest computed tomography (CT) showed an obstruction at the right main bronchus and atelectasis at the lower right lobe (Figure 1(a)). Tumor progression was also seen at Th12 of the spinal canal (Figure 3(b)). Bronchoscopy revealed the right middle trunk was completely occluded by the tumor, which showed a white necrotic surface, and the surrounding bronchial epithelium was reddish, displaying cancerous lymphangiopathy (Figure 2(a) and (b)). A biopsy was performed by endobronchial ultrasonography using guide sheath obtaining sufficient samples. A sample of the metastasized bone was collected during subsequent fusion surgery due to a metastatic spinal tumor.
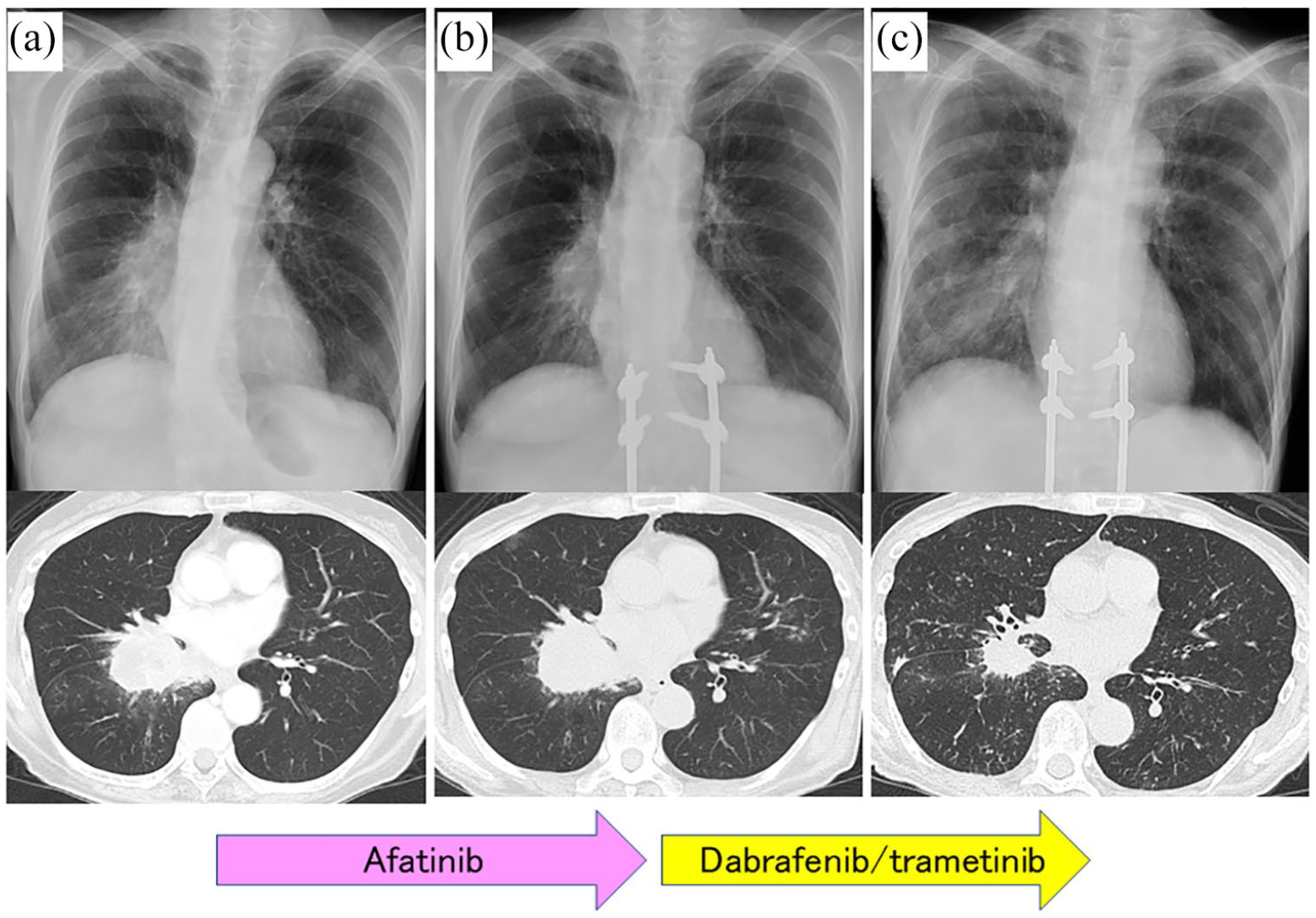
Chest X-ray and CT image before treatment (a), after administration of first-line treatment afatinib on Day 12 (b), and after administration of second-line treatment of dabrafenib and trametinib on Day 13 (c).
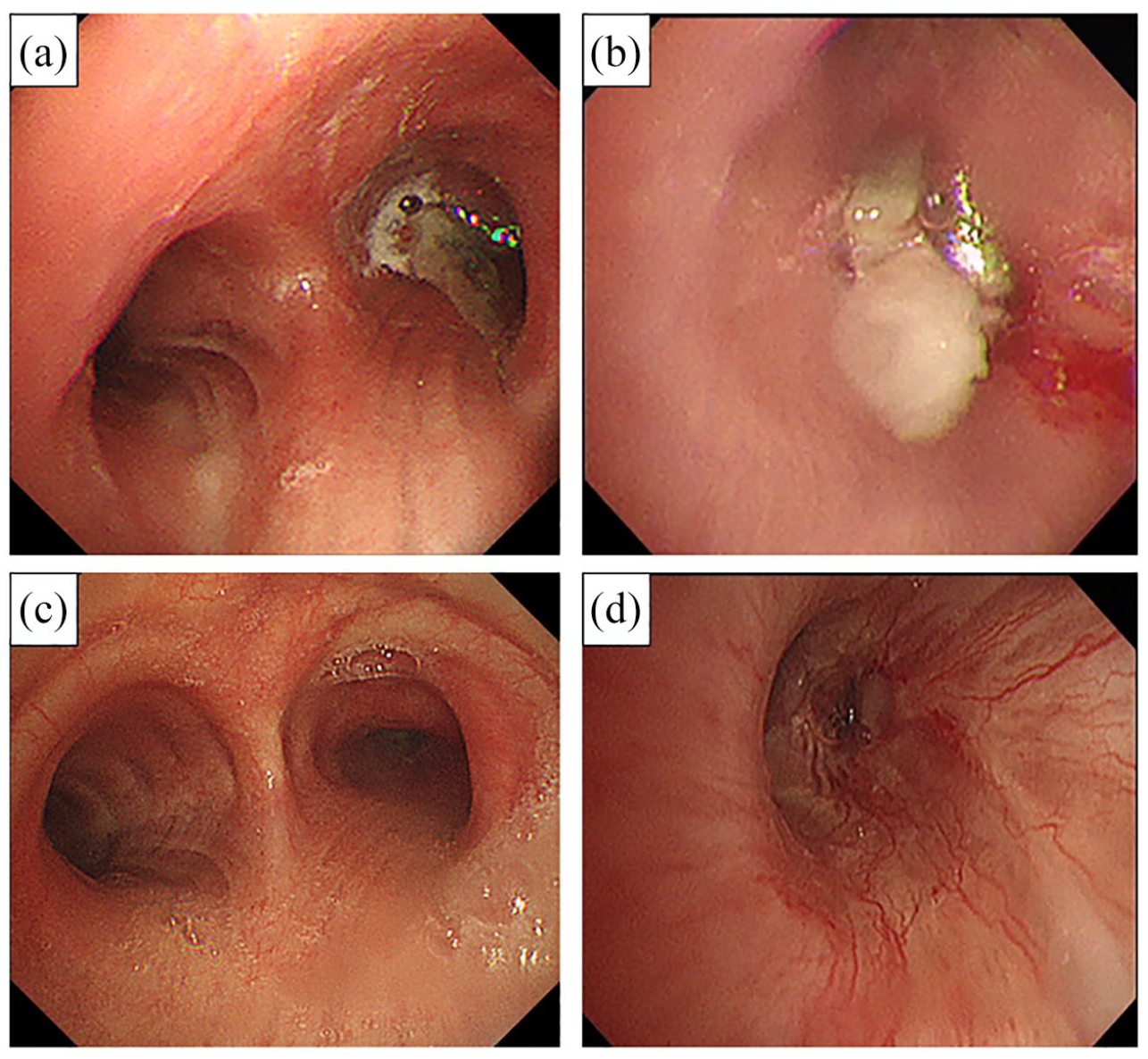
Bronchoscopic view of pretreatment tracheal bifurcation (a) and tumor-occluded right middle trunk (b). After administration of dabrafenib and trametinib on Day 23, endoscopic observation showed remarkable endobronchial treatment effect (c, d).
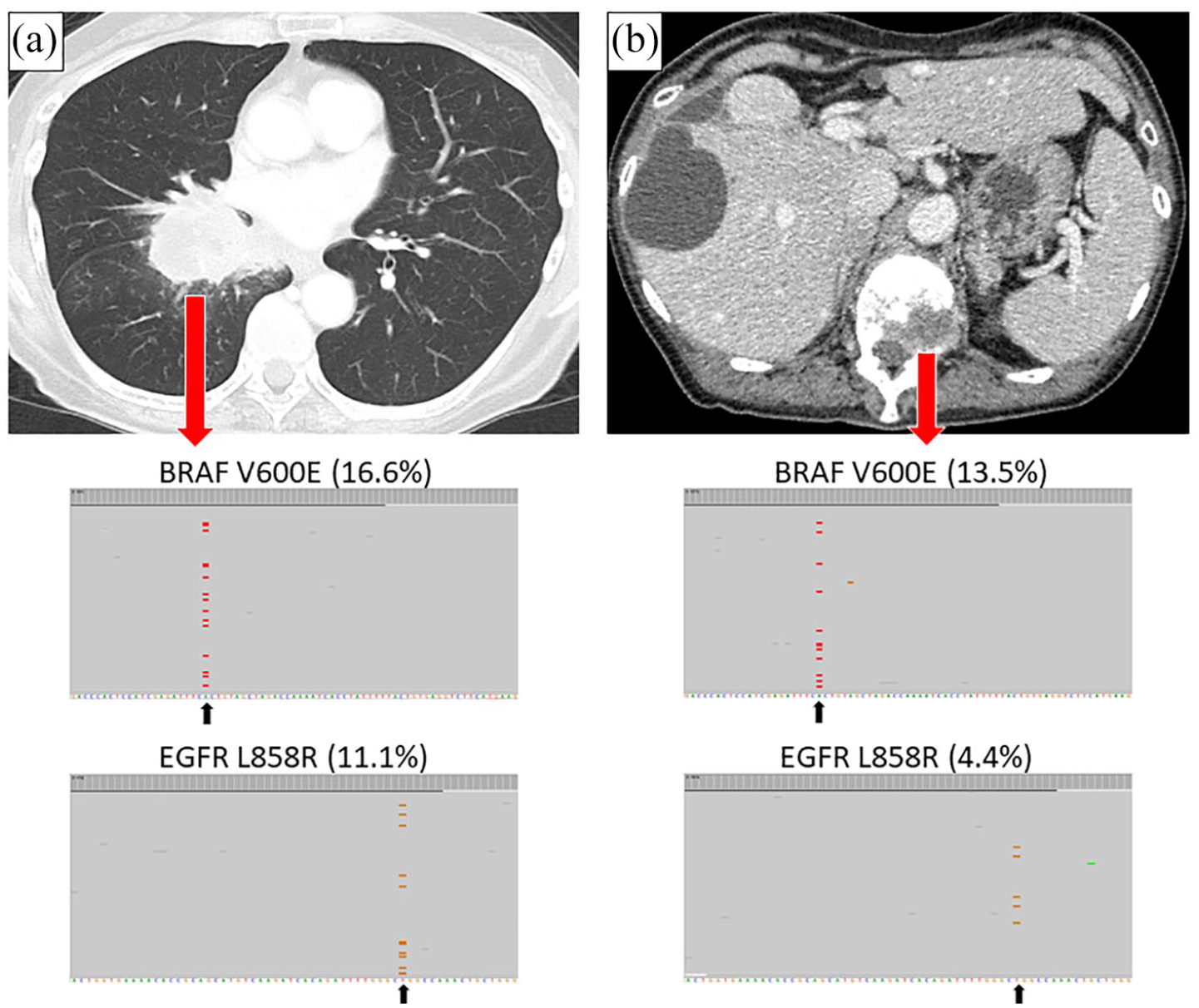
High sensitivity NGS panel system revealed the primary lung tissue consisted of 16.6% BRAF V600E and 11.1% EGFR exon21 L858R (a), while the bone specimen consisted of 13.5% BRAF V600E and 4.4% EGFR exon21 L858R for gene allele frequency (b).
Bronchoscopic examination revealed class V non-small-cell carcinoma by cytology, and immunostaining revealed TTF-1, p40, and CK5/6 were negative for non-small-cell carcinoma. Clinically, tumor necrosis factor (TNM) classification was T4 (tracheal carina invasion) N3M1c (OSS) stage IVB. Cobas® EGFR Mutation Test v2.0 was performed using cytological specimens, and exon21 L858R point mutation was detected. First-line treatment with afatinib 40 mg/day was introduced but discontinued due to slight regrowth of the primary tumor confirmed by CT on Day 12 (Figure 1(b)). On Day 14, the results of an Oncomine™ Dx Target Test using the bone specimen revealed EGFR mutation was “no call,” or undecidable, which is sometimes noted when allele frequency is below the sensitivity required to be reported. However, BRAF V600E mutation was positive. The following day, the patient received BRAF inhibitor, dabrafenib 300 mg and MEK inhibitor, trametinib 2 mg. The drugs were temporally suspended for several days due to Grade-2 fever and loss of appetite, but her symptoms gradually improved, and CT on Day 13 showed a patent airway at the right middle trunk (Figure 1(c)). Endoscopic observation on Day 22 confirmed a remarkable endobronchial treatment effect (Figure 2(c) and (d)). The therapeutic effect has also been confirmed with tumor markers. Carcinoembryonic antigen (CEA) value was within the normal range (2.0 ng/mL) before treatment and was not an indicator. However, SLX, CA19-9, CYFRA, NSE, and Pro GRP values were high before treatment (58.9 U/mL, 108.0 U/mL, 6.3 ng/mL, 16.7 ng/mL, 43.2 pg/mL, respectively), all increased after the first treatment (immediately before the introduction of the second-line treatment) (80.2 U/mL, 127.2 U/mL, 9.6 ng/mL, 19.5 ng/mL, 58.2 pg/mL, respectively), markedly decreased after second-line treatment (46.1 U/mL, 47.9 U/mL, 1.3 ng/mL, 10.6 ng/mL, 34.3 pg/mL, respectively).
High sensitivity next-generation sequencing (NGS) panel system revealed the primary lung tissue consisted of 16.6% BRAF V600E and 11.1% EGFR exon21 L858R (Figure 3(a)), while the bone specimen consisted of 13.5% BRAF V600E and 4.4% EGFR exon21 L858R for gene allele frequency (Figure 3(b)). After administration of BRAF/MEK inhibitor, we re-examined CT on Day 24 and confirmed partial response, the treatment was handed over to the referral hospital.
Discussion
To our knowledge, this is the first report describing both EGFR mutation and BRAF V600E mutation detected in primary and metastatic lesions before administration of molecular-targeted therapy, without an acquired resistance of EGFR-TKI. 2
We occasionally encounter cases with different driver genes detected at each lesion for double cancer. In addition, some cases have been reported where BRAF mutations emerge by sequential measurement after resistance to EGFR-TKI for EGFR-mutant adenocarcinoma.2,3 Although it is rare to find coexisting driver mutations in the primary diagnostic sample, we also detected these same driver mutations in the secondary metastatic lesion. From these findings, it might be easier to understand that lung adenocarcinoma originally having two driver mutations has metastasized to other organs, rather than considering a lung collision cancer with different driver mutations. However, the exact mechanism of onset or formative process of the primary lesion remains unclear. Although it has been reported that EGFR and BRAF genes were exclusive, 4 a recent report revealed a case of coexisting genes with V600G. 5
In this case, EGFR-TKI was ineffective but BRAF/MEK inhibitor showed a remarkable treatment effect. The poor therapeutic effect of EGFR-TKI is possibly due to the low allelic frequency of the EGFR mutation compared to BRAF mutation using high sensitivity NGS panel analysis. About this speculation, there is no literature that analyzes the relationship between the allele ratios of different driver genes and the therapeutic effect, but there is a report that the higher allele ratio of the T790M mutation of the EGFR mutation, the higher the therapeutic effect of osimertinib, which might be helpful to understand the course of treatment in this case. 6 When multiple driver mutations are detected at the primary diagnostic specimen, it might be necessary to consider a therapeutic agent with gene alleles frequency. Moreover, the usefulness of two types of molecular-targeted drugs in combination has also been reported, 2 but combination molecular-targeted therapy has not recognized in insurance medical treatment in our country. Among the EGFR-mutant lung cancers, it is speculated that there may be cases harboring double mutations when EGFR-TKI treatment is ineffective or judged early resistant. Although infrequent, interpretation and treatment strategies might become increasingly important when more than two gene mutations are detected.
Footnotes
Acknowledgements
The authors thank Mr. Jason Tonge from St. Marianna University School of Medicine for the linguistic review of this manuscript.
Author contributions
KM had full access to data in this case report and takes responsibility for the integrity and accuracy of data analysis. KM and YS contributed to bronchoscopic examination and interpretation. MI, HN, TI, and MM contributed to the scientific review and final approval of this manuscript. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research gene analysis of this case was conducted by DNA Chip Research Inc., Tokyo, Japan.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Joint research with DNA Chip Research Inc., Tokyo, Japan.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. The research gene analysis was with ethics approval (HREC ID 4814).