
Abstract
Introduction:
Given the metachronous and multifocal occurrence of hepatocellular carcinoma (HCC) and colorectal cancer metastases in the liver (CRLM), this study aimed to compare intrahepatic progression patterns after computed tomography (CT)-guided high dose-rate brachytherapy.
Patients and methods:
This retrospective analysis included 164 patients (114 HCC, 50 CRLM) treated with brachytherapy between January 2016 and January 2018. Patients received multiparametric magnetic resonance imaging (MRI) before, and about 8 weeks after brachytherapy, then every 3 months for the first, and every 6 months for the following years, until progression or death. MRI scans were assessed for local or distant intrahepatic tumor progression according to RECIST 1.1 and electronic medical records were reviewed prior to therapy. The primary endpoint was progression-free survival (PFS). Specifically, local and distant intra-hepatic PFS were assessed to determine differences between the intrahepatic progression patterns of HCC and CRLM. Secondary endpoints included the identification of predictors of PFS, time to progression (TTP), and overall survival (OS). Statistics included Kaplan–Meier analysis and univariate and multivariate Cox regression modeling.
Results:
PFS was longer in HCC [11.30 (1.33–35.37) months] than in CRLM patients [8.03 (0.73–19.80) months, p = 0.048], respectively. Specifically, local recurrence occurred later in HCC [PFS: 36.83 (1.33–40.27) months] than CRLM patients [PFS: 12.43 (0.73–21.90) months, p = 0.001]. In contrast, distant intrahepatic progression occurred earlier in HCC [PFS: 13.50 (1.33–27.80) months] than in CRLM patients [PFS: 19.80 (1.43–19.80) months, p = 0.456] but without statistical significance. Multivariate Cox regression confirmed tumor type and patient age as independent predictors for PFS.
Conclusion:
Brachytherapy proved to achieve better local tumor control and overall PFS in patients with unresectable HCC as compared to those with CRLM. However, distant progression preceded local recurrence in HCC. As a result, these findings may help design disease-specific surveillance strategies and personalized treatment planning that highlights the strengths of brachytherapy. They may also help elucidate the potential benefits of combinations with other loco-regional or systemic therapies.
Keywords
Introduction
Liver cancer is the sixth most commonly diagnosed cancer and the fourth leading cause of cancer death worldwide, with about 841,000 new cases and 782,000 deaths annually. 1 Hepatocellular carcinoma (HCC) represents more than 90% of primary liver cancers and is a major global health problem.2,3 Besides primary liver cancer, the liver is a common site for metastases of cancers that derive from other organs such as colorectal cancer liver metastases (CRLM). In 25% of patients, CRLM occur synchronously, while up to 60% of patients will develop them during the course of the disease. 4 Despite the availability of a multidisciplinary treatment armamentarium, the 5-year survival rate for patients with CRLM remains as poor as 10%. 5
Commonly used chemotherapeutic treatments for CRLM lead to a median life-prolonging effect of 2.3 months but bear the risk of systemic adverse events. 6 In liver-dominant disease, local, minimally-invasive therapies are effective alternatives, with a potentially reduced risk of side effects. 7 Thermal local ablation techniques lead to similar overall survival (OS) rates when compared with those for hepatic resection; however, the effect of treatment is limited by the heat-sink effect when lesions are located close to vessels or exceed a diameter of 5 cm. 8
Additionally, substantial evidence exists in support of non-thermal ablation with computed tomography (CT)-guided interstitial high-dose rate brachytherapy, which comprises the catheter-based, percutaneous internal radiation of the tumor with a gamma-emitting iridium-192 source that is temporarily applied and removed immediately after treatment. 9 Due to precise 3D radiation planning and the rapid dose drop outside the target tissue, brachytherapy allows for the ‘inside-out’ application of a very high radiation dose to the target volume in a single fraction (>100 Gy in central tumor parts), while sparing surrounding liver parenchyma. 10 The overall patient safety of the intervention is very high and local tumor control rates are encouraging. As a result, it represents an important option in treating patients with advanced hepatic tumors without a surgical alternative, especially when reduced liver function due to previous surgery or chronic liver disease is present. With this in mind, brachytherapy is also applied in patients with large (>5 cm) and multifocal unresectable HCC, where it demonstrates promising median OS of 28.9 and time-to-progression (TTP) of 11.7 months. 11
However, current monitoring strategies for patients who received brachytherapy do not consider the underlying tumor entity. Moreover, very little is known about its effect on tumor susceptibility to brachytherapy or tumor response. 12 Evidence exists supporting the theory that the majority of recurrences are limited to the liver and develop within the first year after treatment.13,14 Although this may seem intuitively right, it has not been previously reported for HCC and CRLM in the literature and no study exists that further investigated tumor-specific profiles of intrahepatic progression.
Given the metachronous and multifocal occurrence of HCC and CRLM possibly requiring personalized monitoring and treatment strategies, this study aimed to compare progression-free survival (PFS) and specifically local and distant intrahepatic progression patterns of HCC and CRLM after brachytherapy using longitudinal multiparametric magnetic resonance imaging (MRI).
Methods
Study cohort and endpoints
This retrospective, single-institution study was compliant with the Health Insurance Portability and Accountability Act (HIPAA) and approved by the institutional review board (EA4/089/17). Informed consent was waived, given the retrospective observational study design. All patients had been discussed in a multidisciplinary tumor board and had received a recommendation for tumor ablation. Consecutive patients with HCC and CRLM who received brachytherapy between January 2016 and January 2018 were included in this study. They had received at least one baseline MRI scan within 30 days prior to, and one follow-up MRI scan about 8 weeks after brachytherapy. All target lesions were naïve to loco-regional minimally invasive liver-directed therapies.
The primary endpoint was PFS. Specifically, local and distant intra-hepatic PFS were assessed to determine differences between the intrahepatic progression patterns of HCC and CRLM as further specified below. Secondary endpoints included the identification of predictors of PFS, TTP, and OS.
CT-guided high dose-rate brachytherapy
Technical brachytherapy protocol
Procedural standards of the brachytherapy were described in detail elsewhere.15,16 Briefly, patients were treated under conscious sedation (midazolam and fentanyl) and local anesthesia (xylocaine). The therapies were performed by two interventional radiologists with 12 and 8 years of experience in brachytherapy, respectively. Under CT-fluoroscopic guidance, a 6F angiographic sheath was inserted into the lesion. Through this sheath, the closed-ended 6F brachytherapy catheter (Primed, Halberstadt, Germany) was introduced. The array of the catheter in relation to the tumor was depicted on a contrast-enhanced CT scan (primary slice thickness 0.625 mm, reconstructed to a slice thickness of 5 mm), which was used for further treatment planning on a 3D radiation planning workstation (Brachyvision; Varian Medical Systems, Palo Alto, CA, USA). A portal venous contrast phase (45 seconds after injection) was chosen for CRLM and an arterial phase (15 seconds after injection) for HCC.
The clinical target volume was segmented manually on these planning CT scans and the general intention was to ablate each lesion with a tumor enclosing target dose of 20 Gy using the iridium-192 source (Gammamed 12; Varian Medical Systems). Adjacent structures at risk, such as the stomach or the duodenum, were marked and their dosage was calculated; if necessary, the overall dosage was modified according to Collettini et al. 17 After completion of the brachytherapy, the catheter was retracted and the puncture channels were sealed with resorbable, thrombogenic material (Gelfoam; Pfizer Inc., New York, NY, USA) to avoid bleeding.
Sequential brachytherapy treatments
A brachytherapy treatment was defined completed when all target lesions were completely irradiated with the target dose of 20 Gy. Target lesions were selected, and the treatment was planned at the discretion of the interventional radiologist. Sequential treatments were performed if the patient had multifocal or large tumors at baseline, where the radiation volume had to be split into sequential sessions to avoid adverse events from tumor lysis, or to reduce cumulative puncture risk. As a result, patients were included who had received up to 4 sequential brachytherapy sessions within 4–6 week-intervals to achieve completed brachytherapy.
If the patient developed new intrahepatic lesions during follow-up that were not present at baseline and were treated with brachytherapy in a new treatment cycle (at least 8 weeks after the first brachytherapy), these additional brachytherapy’s were considered separate treatments for the calculation of the TTP. However, for the calculation of the PFS, this event was considered tumor progression and follow-up was terminated.
Image acquisition and analysis
MRI protocol
MRI scans were acquired on a 1.5-T-device (Avanto, Siemens, Erlangen, Germany) using an eight-channel body phased-array coil. Hepatocyte-specific contrast agent (Primovist; Bayer, Leverkusen, Germany) was for dynamic contrast-enhanced sequences. A standard volume interpolated breath-hold examination sequence (VIBE) in the axial plane with a TR of 4.26 ms, a TE of 1.87 ms, a flip angle (FA) of 10°, a slice thickness of 3 mm, and a matrix size of 256 × 127 was acquired; this covered the entire liver with 60–72 slices and an adjusted field of view (FOV) of 255–300 × 340–400 mm. Images were evaluated with Merlin Phoenix version 5.8 (Pixmeo SARL, Bernex, Switzerland).
MRI schedule and tumor response assessment
Patients received multiparametric MRI before, and about 8 weeks after, brachytherapy, then every 3 months for the first, and every 6 months for the following years, respectively, until death or loss to follow-up.
Tumor response according to the response evaluation criteria in solid tumors (RECIST) 1.1 was assessed on the follow-up imaging datasets by two radiologists with 5 and 7 years of experience in abdominal imaging, who did not perform the brachytherapy. 18 The follow-up ended in June 2020, and all MRI or CT scans obtained until June 2020 were included in the analysis.
Kaplan–Meier survival analysis
Overall survival, progression-free survival, and time-to-progression
OS, PFS, and TTP were analyzed using Kaplan–Meier analysis and the log-rank test. OS was defined as the time between the first completed brachytherapy treatment and the date of death from any cause. Patients who were lost to follow-up or still alive at the time of the last follow-up without an event (progression or death) were censored at the respective timepoint.
PFS was defined as the time between the first completed brachytherapy treatment and death or the occurrence of intrahepatic or extrahepatic tumor progression, respectively. Patients who received additional loco-regional treatments of the target lesions were censored at the respective timepoint. Patients without progression of any kind or death until the end of follow-up were censored at the end of follow-up.
TTP was defined as the time between any completed brachytherapy treatment and the occurrence of intrahepatic or extrahepatic tumor progression. In contrast to PFS, TTP in this study was calculated for every completed brachytherapy treatment cycle (i.e., multiple completed brachytherapy treatments on different target lesions of the same patient).
Patterns of intrahepatic progression
In addition to the overall PFS and TTP, two specific progression patterns were separately assessed for subgroup analyses. These subtypes of progression were defined as local recurrence (PFSlocal or TTPlocal) and distant intrahepatic progression (PFSdistant or TTPdistant). Local recurrence was defined as an increase of the target lesion diameter >20% according to RECIST 1.1. While PFSlocal was assessed on the target lesions treated during the first completed brachytherapy, TTPlocal was always defined based on the target lesions treated during the respective brachytherapy cycle. Distant intrahepatic progression was defined as the occurrence of a new malignant hepatic lesion at a different site that had not been treated by brachytherapy before.
Cox regression model
In addition to the Kaplan–Meier analysis, a univariate Cox proportional hazard regression model was developed to evaluate the predictive value of each coverage factor (predictor variables). For the overall PFS, the PFSlocal and PFSdistant, statistically significant variables (p < 0.1) were selected to develop a multivariate Cox proportional hazard regression model to evaluate their predictive value for the overall PFS, the PFSlocal and PFSdistant, when taking into account multiple coverage factors. Covariates were selected, which had a previously reported effect on survival outcome.19–22 Besides imaging-based tumor characteristics (tumor type, target lesion diameter, number of target lesions), clinical and demographic parameters (age, gender) derived from electronic medical records prior to therapy were included in the regression model.
Statistics
Descriptive statistics were reported as the mean ± standard deviation (SD) and median and range, respectively. Statistical significance was defined as p < 0.05. Survival and Cox regression analyses were performed using SPSS software (IBM SPSS Statistics, version 26, 2019, IBM Corp, Armonk, NY, USA).
Results
Patient characteristics
In total, 156 HCC patients with 233 target tumors and 65 CRLM patients with 117 target tumors receiving brachytherapy were identified. Eleven patients who had no cross-sectional imaging 8 weeks after brachytherapy and 46 patients with combined loco-regional treatments to the target lesions [30 transarterial chemoembolization (TACE), 16 selective internal radiotherapy (SIRT)] were excluded. As a result, the total study population considered for the analysis consisted of 164 patients with 223 target lesions including 114 HCC patients with 142 target lesions and 50 CRLM patients with 81 target lesions, respectively. Of these 164 patients, 17 (14.9%) HCC and 6 (12.0%) CRLM patients received multiple completed brachytherapy treatments that were considered separately for the calculation of the TTP. As a result, in total, 131 and 56 completed brachytherapy treatments were performed in HCC and CRLM patients, respectively

Study workflow and exclusion criteria.
The mean age was 69.97 ± 10.75 and 66.30 ± 12.63 years in HCC and CRLM patients, and 78.9% and 72.0% were men, respectively. Patients with HCC presented with 1.24 ± 0.50 lesions at baseline and patients with CRLM with 1.62 ± 1.00, respectively. The target lesion diameter was 36.78 ± 23.00 mm in HCC and 40.00 ± 24.07 mm in CRLM. Patient demographics and tumor characteristics are summarized in Table 1.
Baseline patient, tumor, and other disease characteristics.

ALT, alanine aminotransferase; AP, alkaline phosphate; AST, aspartate aminotransferase; CRLM, colorectal cancer liver metastases; HCC, hepatocellular carcinoma; SD, standard deviation; TACE, transarterial chemoembolization.
Overall, major treatment-related complications (grade ⩾3 according to the Common Terminology Criteria for Adverse Events v5.1) following brachytherapy were rare. The rate of complications was <1%: comprising two bleedings that occurred in patients with hypervascularized HCC lesions.
Tumor response
In total, the 114 HCC patients included in this study received 3.11 ± 1.80 follow-up imaging scans and the 50 CRLM patients received 2.36 ± 1.64 scans, respectively, until an event (progression, death) was noted, or until they were censored, or until the end of follow-up. Results from the tumor response assessment according to RECIST 1.1 evaluated on the cross-sectional imaging 8 weeks and 3 months after completed brachytherapy are reported in Table 2. Follow-up imaging at 8 weeks was available for every complete treatment. However, follow-up imaging at 3 months was only available in 105 HCC and 30 CRLM cases due to progression, death, or loss of contact.
Tumor response after brachytherapy according to the response evaluation criteria in solid tumors (RECIST) 1.1.
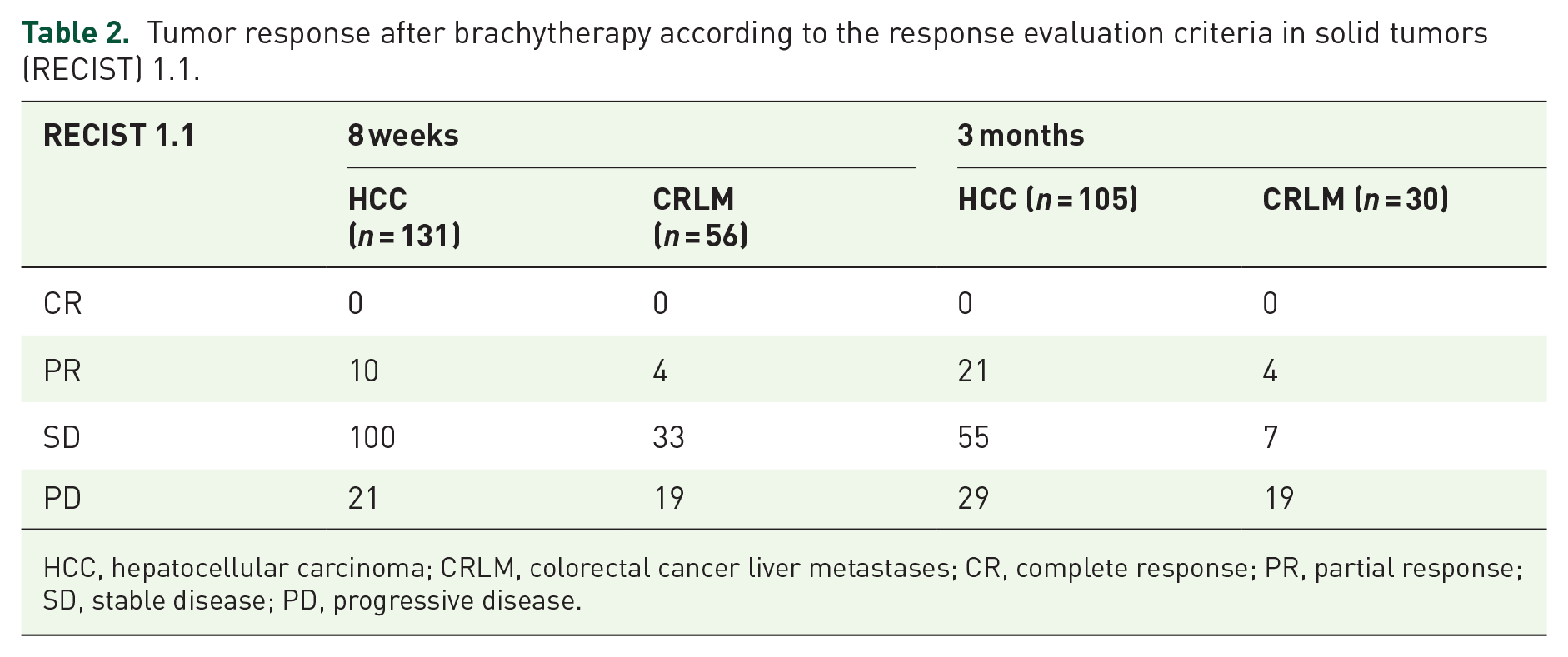
HCC, hepatocellular carcinoma; CRLM, colorectal cancer liver metastases; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease.
Overall survival
All OS, PFS, and TTP data are summarized in Table 3.
Survival data for patients with hepatocellular carcinoma (HCC) and colorectal cancer liver metastases (CRLM) undergoing CT-guided brachytherapy.

N/A, not assessable (the median overall survival for HCC was not reached); OS, overall survival; PFS, progression-free survival; PFSdistant/TTPdistant, distant intrahepatic progression; PFSlocal/TTPlocal, local recurrence; TTP, time to progression; bold p-values indicate statistical significance in the log-rank test (p < 0.05).
The median follow-up time was 24.03 (2.03–48.3) months for HCC and 13.80 (2.01–47.20) months for CRLM. During the follow-up period, 23 HCC and 9 CRLM patients had died, and 32 HCC and 7 CRLM patients were still alive at the end of follow-up without an event (progression or death), respectively. As for the OS, 91 HCC and 41 CRLM patients were censored. The median survival in HCC patients was not reached. For CRLM patients, the median OS was 47.20 months (p = 0.279). The OS rate was 92.9% at 6 months, 79.8% at 12 months, and 50.0% at 24 months in HCC patients, respectively. The OS rate was 78.0% at 6 months, 50.0% at 12 months, and 10.0% at 24 months of CRLM patients, respectively.
Progression-free survival
The median overall PFS was longer in HCC [11.30 (1.33–35.37) months] than in CRLM patients [8.03 (0.73–19.80) months; p = 0.048]. In particular, the local recurrence (PFSlocal) was longer in HCC [36.83 (1.33–40.27) months] than in CRLM patients [12.43 (0.73–21.90) months; p = 0.001] (Figure 2). However, the distant intrahepatic progression (PFSdistant) was longer in CRLM [19.80 (1.43–19.80) months] than in HCC patients [13.50 (1.33–27.80) months; p = 0.456] but without statistical significance (Figures 2 and 3). In addition, 7 HCC (6.1%) and 6 CRLM patients (12.0%) experienced extrahepatic metastases.

Patterns of intrahepatic progression following brachytherapy. (a, e) show representative axial MRI scans of an exemplary HCC (arterial phase) (a) and two CRLM (venous phase) (e) prior to treatment with brachytherapy. The patient shown in the upper row had a total of three HCC lesions that were treated with brachytherapy, one of which is displayed on the images (a–c). (b, f) show the brachytherapy planning on the peri-interventional CT scan. (c, g) show the first follow-up MRI approximately 8 weeks after brachytherapy. (d) and (h) show the first type of intrahepatic progression that was detected in these patients. The white arrow in (d) indicates a distant intrahepatic HCC lesion 11.1 months after brachytherapy. The arrowheads in (h) indicate the local recurrence of the CRLM at the margin of the treated lesion 12.9 months after brachytherapy.

Overall PFS, PFSlocal, and PFSdistant in HCC and CRLM following brachytherapy. (a) The median overall PFS was longer in HCC (11.30 months) compared to CRLM (8.03 months) (p = 0.048). Local recurrence of the target lesions occurred much earlier in CRLM (12.43 months) compared to HCC (36.83 months; p = 0.001). However, distant intrahepatic progression occurred earlier in HCC (13.50 months) than in CRLM patients (19.80 months; p = 0.456), but without statistical significance.
Time-to-progression
Median TTP was longer in HCC [11.17 (1.60–35.67) months] than CRLM patients [5.27 (0.73–19.80) months; p = 0.007]. In particular, the TTPlocal was detected to be much longer in HCC [50.13 (1.33–50.13) months] than in CRLM patients [9.90 (0.73–19.30) months; p < 0.001]. However, the TTPdistant was longer in CRLM [19.80 (1.43–19.80) months] than in HCC patients [13.50 (1.33–33.23) months; p = 0.535], but without statistical significance.
Predictors of progression-free survival after brachytherapy
In the entire study cohort, the univariate Cox regression model revealed that overall PFS was significantly reduced in patients with older age [confidence interval (CI), 1.005–1.041; hazard ratio (HR), 1.023; p = 0.013], larger tumor diameter (CI, 1.008–1.021; HR, 1.015; p = 0.001), or CRLM, as compared to HCC (CI, 0.497–1.032; HR, 0.711; p = 0.073). The multivariate Cox regression model confirmed the findings of the univariate Cox regression model and revealed that overall PFS was significantly reduced in patients with older age (CI, 1.016–1.054; HR, 1.035; p = 0.001) or CRLM, as compared to HCC (CI; 0.368–0.874; HR, 0.567; p = 0.01), which was also consistent with the findings from the Kaplan–Meier analysis.
In addition, the PFSlocal was significantly reduced in patients with older age (CI, 0.999–1.052; HR, 1.026; p = 0.056), larger target tumor diameter (CI, 1.033–1.023; HR, 1.013; p = 0.014), and particularly CRLM (CI, 1.202–3.095; HR, 1.929; p = 0.006). The multivariate Cox regression model confirmed the predictive value of the patients’ age (CI, 1.001–1.053; HR, 1.026; p = 0.044) for PFSlocal; it also revealed a strong trend for target tumor diameter (CI, 1.000–1.020; HR, 1.010; p = 0.057) and CRLM (CI, 0.963–3.254; HR, 1.770; p = 0.066), respectively.
By contrast, the only independent predictor for reduced PFSdistant was the patients’ age (CI, 1.008–1.048; HR, 1.028; p = 0.050), while the tumor type did not seem to have a significant effect on PFSdistant, which was consistent with the Kaplan–Meier analysis (Table 4).
Univariate and multivariate Cox regression hazard models for progression-free survival.

CI, confidence interval; HR, hazard ratio; PFS, progression-free survival; PFSdistant, distant intrahepatic progression; PFSlocal, local recurrence; bold p-values indicate statistical significance in the univariate (p < 0.1) and multivariate analysis (p < 0.05).
Discussion
The main finding of this study was that brachytherapy proved to achieve better tumor control of HCC than CRLM in terms of overall PFS [HCC: 11.30 (1.33–35.37) months; CRLM: 8.03 (0.73–19.80); p = 0.048] and especially local tumor recurrence [HCC: 36.83 (1.33–40.27); CRLM: 12.43 (0.73–21.90); p = 0.001]. By contrast, distant intrahepatic progression occurred earlier in HCC than in CRLM patients [13.50 (1.33–27.80) months; CRLM: 19.80 (1.43–19.80) months; p = 0.456] but without statistical significance. Patient age was the only independent risk factor for all types of intrahepatic progression.
Since HCC is less likely to develop extrahepatic metastases, local ablation techniques are often applied and guideline-approved, as they cause select maximum damage to the tumor while preserving organ function.23–25 Thermal ablation by radiofrequency (RFA) or microwave ablation (MWA) is recommended as a first-line treatment in very early-stage disease (BCLC 0, tumors < 2 cm diameter), where RFA has demonstrated similar outcomes to liver resection. 26 However, thermal ablations have several limitations, including an optimal tumor size not exceeding 3–3.5 cm, heat sink effects in the vicinity of large blood vessels, and the risk of causing injury to adjacent bile ducts. In contrast to thermal ablation, brachytherapy, which is considered an alternative to thermal ablations by the clinical practice guidelines of the European Society for Medical Oncology, has almost no restrictions with regards to the tumor size that can be treated, its therapeutic effect is not degraded by heat dissipation, and it can also be used to treat tumors in the vicinity of thermosensitive structures.12,26,27 Brachytherapy has proven effective, with tumor control rates >90% after 12 months in tumors of ⩽12 cm diameter in single-center studies with excellent safety profiles.12,28 Unlike conventional external beam radiotherapy and stereotactic body radiotherapy (SBRT), the therapeutic effect of brachytherapy is not endangered by patient movement or respiratory excursion since the applicator is anchored directly within the tumor.10,12 In addition, conventional percutaneous radiation of HCC is limited by the low radiation sensitivity of hepatocellular cancer cells, altered tissue structures in cirrhotic livers, and very radioresponsive organs surrounding the liver that adversely affect the dose of radiation used to target the tumor. 27
A retrospective study included 98 patients with 212 unresectable HCC with a mean tumor diameter of 5 cm (range, 1.8–12.0 cm). Eighteen of 212 (8.5%) tumors showed local, and 67 patients (68.4 %) experienced distant tumor progression, respectively. The median PFS was 15.2 months, and the median OS was 29.2 months with a 1-, 2-, and 3-year OS rate of 80, 62, and 46%, respectively. 28 Furthermore, a prospective phase II study of HCC showed a high survival benefit compared to best supportive care with a median OS of 23 months in the brachytherapy group versus 5 months in the control group for patients with a Cancer of the Liver Italian Program (CLIP) score of 2. Patients with CLIP scores ⩾ 3 demonstrated a median OS of 18 versus 4 months, respectively. 18 In a study evaluating brachytherapy for HCC as a bridge to liver transplant, the results showed a similar or even higher degree of necrosis and lower recurrence rates after liver transplant than TACE.27,28
For the treatment of large HCC up to 5 cm, ablation can be combined with TACE to decrease the risk of local recurrence.29,30 Positive results were obtained in patients with intermediate stage and large HCCs, which became the ideal setting for the combination of TACE and ablation. 31 In this setting, the superiority of brachytherapy has been reported over thermal ablation alone, or in combination with TACE, both of which are incapable of complete treatment of tumors larger than 3–5 cm leading to relatively high rates of local recurrence.12,29,30 Previous studies investigating brachytherapy in combination with conventional TACE demonstrated a promising median OS of 28.9 and TTP of 11.7 months in patients with large (>5 cm) and multifocal unresectable HCC. 30
In our study, distant intrahepatic progression [PFS: 13.50 (1.33–27.80); TTP: 13.50 (1.33–33.23) months] preceded local recurrence in HCC [PFS: 36.83 (1.33–40.27); TTP: 50.13 (1.33–50.13) months]. As HCC is characterized by this multicentric occurrence and oftentimes develops in chronic liver diseases that are hypothesized to generate a pro-inflammatory tumorigenic milieu, innovations in anti-cancer strategies focus on immunotherapeutic interventions that aim at lowering the barrier of immunosuppression and restoring the resources of the immune system against cancer cells.32,33 However, systemic approaches using such immunotherapies have largely failed to elicit meaningful survival benefits in HCC and no significant advantages have been made over standard treatment with sorafenib in more than a decade. 34 Just recently, the groundbreaking results of the IMbrave 150 trial showed that the combination of the immune checkpoint inhibitor atezolizumab with the anti-angiogenic agent bevacizumab was superior to sorafenib in the first-line treatment of advanced HCC and able to prolong PFS and OS. 35 However, overall response rates in the IMbrave 150 trial did not exceed 20% or 27%, according to RECIST and modified (m)RECIST, respectively, calling for further strategies to improve the tumor susceptibility. 36
This unmet clinical need could be addressed by strategies that exploit loco-regional therapies as conditioning tools to convert immune-resistant tumor habitats towards a more susceptible tumor microenvironment that can then be targeted with immunotherapies even in earlier disease stages. 37 The commonly cited rationale to utilize local ablation for this purpose is based on a variety of synergistic mechanisms; it proposes to exploit the presumably favorable effects of increased tumor-associated antigen exposure through tissue destruction.8,38 Recent data has further shown that radiation, as applied during brachytherapy, could re-program the tumor stroma and microenvironment against mechanisms of cancer immune evasion and convert the irradiated and gradually necrotic tumor into in situ vaccines to prime both the innate and adaptive immune system.39,40
In CRLM, surgical resection remains the standard of care for liver-only disease; retrospective studies have reported 5-year survival rates ranging from 25% to 47%.41,42 Comparing surgical resection alone for resectable disease with RFA for unresectable disease, RFA demonstrated inferior survival rates but significantly fewer complications. 43 However, many observational studies were confounded by the treatment indication, because thermal ablation was solely performed for unresectable disease. The more recent retrospective cohort using matched-pair or multivariate analysis reported comparable survival rates for thermal ablation alone versus surgery alone, while also decreasing perioperative morbidity and mortality, length of hospitalization, and accumulative costs with superior QoL.43–47 The results from the multicenter phase-III prospective randomized COLLISION trial (Clinicaltrial.gov identifier: NCT03088150) are awaited, which tests the hypothesis of non-inferiority of ablation compared to surgical resection in a large cohort of patients with small (⩽3 cm) CRLM. Additionally, the ongoing COLLISION XL trial (Clinicaltrial.gov identifier: NCT04081168) will compare SBRT and thermal ablation in patients with unresectable large CRLM (3–5 cm) with a 1-year local PFS being the primary endpoint.
Approximately 80% of patients with CRLM are initially not suitable for curative resection due to tumor location, multifocality, bilobar disease manifestation, or insufficient liver function. A total of about 65% develop intrahepatic recurrence within three years, even with adjuvant systemic chemotherapy. 48 In turn, image-guided ablation techniques may be suitable alternatives and particularly favorable options for elderly, vulnerable CRLM patients with high risks for surgery. 49 Major indications for thermal ablation include rather small (<3 cm), solitary unresectable hepatic metastases in patients with comorbidities, or poor performance status. A recent randomized prospective clinical trial revealed that local ablation can improve OS in unresectable CRLM. In particular, RFA (± surgical resection) and chemotherapy versus chemotherapy alone demonstrated a significantly prolonged 8-year OS of 35.9% versus 8.9%, respectively. 5 These results may also partially be transferable to brachytherapy.
With regards to brachytherapy, a prior retrospective analysis including 80 patients with 179 unresectable CRLM (mean diameter: 29 mm, range 8–107 mm) reported local recurrence in 23 (12.9 %) patients and systemic tumor progression in 50 patients (62.5 %), within a mean follow-up time of 16.9 months. The median OS was 18 months and TTP was 6 months. 28
In our study, the mean target tumor diameter of the CRLM was 40.00 ± 24.07mm, while the median time until local recurrence was 12.43 (0.73–21.90) months, which was significantly shorter than in HCC [36.83 (1.33–40.27); p = 0.001]. Unlike HCC, pathology reports de-monstrate that CRLMs have a more active peripheral tumor cell growth and abundant blood supply, whereas both primary and metachronous HCC foci are characterized by predominantly arterial neovascularization. 19 These features may also be assessable on MRI as subcapsular distribution and peritumoral enhancement, which are common findings in CRLM. 50
To address the limitations of brachytherapy alone in CRLM, a recent prospective study including 23 patients with 47 unresectable CRLMs (mean diameter: 62 ± 19 mm) proved the feasibility and safety of combined irinotecan chemoembolization and CT-guided brachytherapy with a median OS, PFS, and TTP of 8, 4, and 6 months, respectively. 51 However, randomized controlled trials to determine superiority of any of the approaches are warranted.
During the follow-up of the study, patients did not receive any specific or standardized treatment. Given that cancer patients usually receive a multidisciplinary treatment regimen, with several therapeutic approaches depending on their stage of disease, we did not censor patients with additional therapies that were not specifically directed to the previous target lesions (e.g., systemic therapies). It should be noted, however, that systemic (chemo)therapies were paused at least two weeks prior to brachytherapy and resumed two weeks after brachytherapy at the earliest.
Our study has several limitations. Due to the rerospective design, some clinical data could not be reported for all patients (i.e., performance score). In addition, a pathological diagnosis was not available for all HCCs and CRLMs but common MRI diagnostic criteria were used that allow for highly specific non-invasive diagnosis of HCCs and CRLMs, as recommended by practice guidelines.31,50 Tumor response was assessed by RECIST 1.1, which may not be entirely representative of the response of the tumor to brachytherapy that is indicated by gradual signal alterations rather than tumor shrinkage on MRI. However, RECIST 1.1 was applied, as it is the most widely-used criteria for solid tumors. It can also reliably detect tumor progression in terms of new lesions as well as an increase in size of the target lesion >20%, which is not typically expected after brachytherapy. Lastly, no median OS was reached in HCC, as many patients could not be traced to the endpoint of OS. However, PFS was the primary study endpoint; most patients presented with progression prior to death in both HCC and CRLM.
In conclusion, brachytherapy proved to achieve better tumor control of HCC than CRLM in terms of overall PFS and local tumor recurrence. With growing treatment possibilities for both HCC and CRLM, identifying the most beneficial therapeutic regimen for individual patients and disease stages becomes increasingly challenging. Our findings may help to design disease-specific surveillance strategies that highlight the efficacy and strengths of brachytherapy in primary and secondary liver cancer and elucidate the potential benefits of combination approaches with adjuvant loco-regional or immuno-oncological therapies.
Footnotes
Acknowledgements
H.X. and Y.H. are fellows of the Chinese Scholarship Council. L.J.S. is a fellow of the BIH Charité Junior Clinician Scientist Program funded by the Charité – Universitätsmedizin Berlin and the Berlin Institute of Health.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author to editors and referees at submission, and to readers upon reasonable request.