
Abstract
Pancreatic ductal adenocarcinoma (PDAC) remains one of the most aggressive solid tumours with an estimated 5-year overall survival rate of 7% for all stages combined. In this highly resistant disease that is located in the vicinity of many radiosensitive organs, the role of radiotherapy (RT) and indications for its use in this setting have been debated for a long time and are still under investigation. Although a survival benefit has yet to be clearly demonstrated for RT, it is the only technique, other than surgery, that has been demonstrated to lead to local control improvement. The adjuvant approach is now strongly challenged by neoadjuvant treatments that could spare patients with rapidly progressive systemic disease from unnecessary surgery and may increase free margin (R0) resection rates for those eligible for surgery. Recently developed dose-escalated RT treatments, designed either to maintain full-dose chemotherapy or to deliver a high biologically effective dose, particularly to areas of contact between the tumour and blood vessels, such as hypofractionated ablative RT (HFA-RT) or stereotactic body RT (SBRT), are progressively changing the treatment landscape. These modern strategies are currently being tested in prospective clinical trials with encouraging preliminary results, paving the way for more effective treatment combinations using novel targeted therapies. This review summarizes the current literature regarding the use of RT for the treatment of primary PDAC, describes the limitations of conventional RT, and discusses the emerging role of dose-escalated RT and heavy-particle RT.
Keywords
Introduction
Pancreatic ductal adenocarcinoma (PDAC) remains one of the most aggressive solid tumours with an estimated 5-year overall survival (OS) rate of 7% for all stages combined. 1 Most patients have asymptomatic early disease, a factor that contributes to the discovery of PDAC at a locally advanced or metastatic stage in more than 70% of cases. The remaining patients are diagnosed with potentially resectable disease, classified as either resectable (around 20% of cases) or borderline resectable (BR; up to 10% of cases); resectability status being determined by the tumour’s relationship with the surrounding vascular structures.1,2 The only potentially curative option is to obtain a complete surgical resection, but even in this case, the 5-year OS is only about 20%. 3 Currently, across the United States and Europe, with nearly 57,000 and 44,000 deaths per year, respectively, PDAC ranks fourth in number of cancer deaths and is expected to reach second place in this ranking by 2030.4–6 This situation is exacerbated by delays in the emergence of effective systemic treatments compared with many other cancers, highlighting the fact that new strategies are urgently needed. 6 In this treatment-resistant disease, located in the vicinity of many radiosensitive organs, the role of radiotherapy (RT) and indications for its use in this setting have been debated for some time and are still under investigation. The results of several important RT trials did not meet expectations and, thus, many have predicted that the use of RT in pancreatic cancer has ended.7–10 Although a survival benefit has yet to be clearly demonstrated for RT, it is the only technique, other than surgery, that has been demonstrated to lead to local control improvement. 10 The lack of survival benefit is likely hidden by poorly effective prior systemic therapies that do not allow sufficient survival for RT to play its role, with the exception of a minority of poorly identified long-term survivors.11–13 However, the integration of dose-escalated RT treatments, such as hypofractionated ablative RT (HFA-RT) and stereotactic body RT (SBRT), into innovative multidisciplinary neoadjuvant approaches has renewed interest in the use of RT in PDAC. These modern strategies, currently being tested in several single- and multi-centre trials with encouraging preliminary results but without level I evidence, are already changing the way radiation oncologists treat PDAC. These promising combinations, with more effective systemic therapies and progressive improvements in patient selection, are paving the way for RT to become relevant to survival outcomes. This review will summarize the current literature regarding the use of RT for the treatment of primary PDAC, describe the limitations of conventional RT in this setting, and highlight the emerging roles of dose-escalated RT and heavy-particle RT.
RT for primary pancreatic cancer
Non-stereotactic RT
For several decades, conventional RT has been used for the treatment of PDAC but the lack of high-level evidence of its added survival value has made the place of RT in the management of this disease uncertain, particularly for potentially resectable PDAC. 14 The introduction of intensity-modulated RT (IMRT) into the clinical routine a decade ago has limited the treatment-related toxicity of these procedures. 15 However, many issues have been, and are still being, encountered in RT trials for PDAC owing to the lack of consensus with regard to delineation, dose and fractionation to be used, leading to significant treatment variations between radiation oncologists with possible effects on survival. 16 Recently, efforts have been made to conduct PDAC studies using contemporary RT techniques and modern quality assurance.
Resected pancreatic cancer: adjuvant approach
Given the residual high risk of loco-regional failure (LF) in the resection bed and lymph nodes after surgery and standard adjuvant chemotherapy (CT), which was estimated to be as high as 53% in the recent ESPAC-4 trial, adjuvant RT strategies have been explored over the last 30 years. 17 Compared with surgery followed by observation, a phase III trial published in 1985 by the Gastrointestinal Study Group (GITSG) demonstrated that adjuvant chemoradiotherapy (CRT) offered an advantage in survival. 18 However, the three phase III studies that followed were not able to replicate the results of the GITSG trial and did not support a survival benefit of adjuvant CRT compared with observation.7–9,19 In comparison with adjuvant CT alone, prospective phase II/III studies and meta-analyses reported no advantage of adding RT8,9,20–22 except in subgroup analyses of patients with positive resection margins for which CRT might still have a role. 23 However, while a survival advantage has not been demonstrated, adjuvant CRT appears to reduce local recurrence rates at first progression, as suggested in a randomized phase II trial (11% versus 24% for CT alone). 20
It is important to note that the above-mentioned phase III trials have been strongly criticized for the use of an inadequate split-course scheme, the delivery of a total dose of 40 Gy that was likely to be insufficient for providing disease control, and inadequate RT quality control. In addition, two of these phase III studies included a large number of patients with other types of peri-ampullary cancers, known to be associated with a better prognosis than PDAC. 24 The ESPAC-1 phase III trial, which concluded that RT was detrimental to survival,8,9 was particularly criticized for an unexpectedly high local recurrence rate (62%), poor adherence to treatment (30% of patients did not receive the planned treatment) and no uniformity of treatment. Moreover, only 53% of the patients were included in the final analysis and modifications of the primary design resulted in three underpowered parallel studies rather than a real 2 × 2 randomization.25–27
In an attempt to close this debate, the ongoing RTOG 0848 phase III trial aims to demonstrate that modern adjuvant CRT [50.4 Gy in 28 fractions with concomitant 5-fluorouracil (5-FU)] with high-quality control can increase the survival of resected patients who remain free of disease after five cycles of adjuvant gemcitabine ± erlotinib.28,29 The results of the first randomization of 336 resected patients evaluating the addition of erlotinib to adjuvant gemcitabine were presented in 2017 and did not demonstrate any increase in OS. 29 We are now awaiting the results of the second randomization comparing adjuvant CT with or without concurrent RT.
However, this adjuvant approach is now being strongly challenged by more aggressive neoadjuvant treatments that could spare patients with rapidly progressive systemic disease from unnecessary invasive surgery and might increase free margin (R0) resection rates. 30
Potentially resectable pancreatic cancer: neoadjuvant approach
Resectable pancreatic adenocarcinoma
Less than 20% of PDACs are diagnosed as initially resectable due to the close vicinity of major arterial and venous trunks. However, even for these patients with relatively favourable disease, the risk of positive margin at surgery (R1) remains high (around 20–50%), especially at the retroperitoneal margin and due to underestimated contact between the tumour and blood vessels.31–33 Pathological margin status is a crucial prognostic factor and the survival rate of patients with direct involvement of a margin is similar to that of patients with locally advanced disease.34–37 When tumour within 1 mm of the resection margin is included in the definition of R1 margins, the rate of R1 resections increases dramatically up to 80% and this also correlates with poor survival.38–41 Consequently, we are now progressively moving toward developing clinical trials in resectable PDAC that investigate the role of neo-adjuvant therapies, including CRT with or without induction CT. These approaches offer several hypothetical advantages including tumour down-staging, maximizing CRT efficacy on well-oxygenated tissues, increasing R0 resection rates, eradicating micrometastases and selecting patients without rapidly progressive disease.42–44 The results of the randomized phase II/III Prep-02/JSAP05 trial have been recently presented at the American Society of Clinical Oncology (ASCO) meeting and are gradually changing the paradigm. The authors reported a statistically significant survival benefit for the CT arm (gemcitabine/S1) compared with upfront surgery for resectable PDAC (median OS 36.7 versus 26.6 months, p = 0.015). 45 Regarding RT, several single-arm studies and meta-analyses exploring neo-adjuvant CRT in this setting have demonstrated promising results with regard to R0 resection rates (84–100%) and OS,46–51 but results are still conflicting (Table 1).44,52–55 Nevertheless, upfront surgery followed by adjuvant CT remains the standard of care for resectable PDAC.17,56,57 Currently, upfront surgery followed by adjuvant CT [gemcitabine ± capecitabine and, more recently, FOLFIRINOX (oxaliplatin, irinotecan, leucovorin and fluorouracil) in fit patients] is still the standard option for resectable PDAC. However, National Comprehensive Cancer Network (NCCN) and ASCO guidelines do recommend that neoadjuvant treatment be considered in patients with high-risk features including: large primary tumours, very highly elevated CA19-9 levels, large regional lymph nodes, radiographic interface between tumour and mesenteric vasculature, excessive weight loss and extreme pain.58,59
Selected modern trials evaluating the role of non-stereotactic CRT in potentially resectable (R – BR) pancreatic adenocarcinoma.

#, number of fractions; 5-FU, 5-fluorouracil; AHPBA/SSO/SSAT, American Hepatopancreaticobiliary Association/Society of Surgical Oncology/Society for surgery of the Alimentary Tract; BR(-A/PV), borderline resectable (due to arterial abutment/due to exclusive involvement of the portal vein system); CRT, chemoradiotherapy; CT, chemotherapy; DPCG, Dutch Pancreatic Cancer Group; FOLFIRINOX, oxaliplatin, irinotecan, leucovorin and fluorouracil, Gy, Gray; I, induction; S, sensitizer; Gem, gemcitabine; IMRT, intensity-modulated radiation therapy; N, number of patients; NA, not applicable; NCCN, National Comprehensive Cancer Network; NR, not reported; R, resectable; RT, radiation therapy; S-1, combination Tegafur/gimeracil/oteracil; VMAT, volumetric modulated arc therapy.
Early termination due to efficacy.
Statistically positive results in favour of CRT arm.
Closed early due to poor accrual.
Results for BR population only.
Borderline resectable pancreatic adenocarcinoma
One of the main issues so far has been that the definition of resectability varies considerably from one study to another and that most trials include resectable, borderline resectable (BR) and even locally advanced pancreatic cancer (LAPC) patients. Theoretically, BR tumours can potentially be resected but contacts between the primary tumour and the surrounding vasculature are more extended, impeding a curative surgery. 67 The lack of standardization for this sub-population is of critical importance as various BR definitions have been used, sometimes with significant differences. For example, the MD Anderson group includes patients with poor performance status or severe comorbidities (BR type C) and patients with a suspicion of extra-pancreatic metastatic disease (BR type B).68,69 Therefore, cautious interpretation should be made when analysing and comparing trials that include patients with BR tumours. The neoadjuvant approach appears to be particularly beneficial for BR tumours since several non-randomized trials and meta-analyses have demonstrated promising results regarding R0 resection rates and survival (Table 1).48–56,62–66,68,69 However, the four published randomized phase II/III trials comparing primary surgery with neoadjuvant CRT in potentially resectable PDAC closed early and/or were largely underpowered due to poor accrual.57,61,65,70 Another example is a Korean phase II/III trial that aimed to compare initial surgery versus neoadjuvant CRT (54 Gy in 30 fractions with gemcitabine) for BR tumours only, defined according to 2012 NCCN guidelines. Results of the interim analysis were recently published: 50 patients were enrolled out of the 110 required and, in the intention-to-treat analysis, the experimental arm showed a significant improvement in R0 resection rates (51.8% versus 26.1%, p = 0.004) and median survival (21 versus 12 months, p = 0.028). Consequently, owing to these positive results, the study was prematurely discontinued based on efficacy. 61 In addition, the phase III PREOPANC-1 study completed inclusion of patients in July 2017 with 248 resectable and BR patients randomized between immediate surgery and preoperative hypofractionated CRT with modern quality assurance (36 Gy in 15 fractions; 3 cycles of gemcitabine 1 g/m2, concurrent during the second cycle).71,72 This particular hypofractionated RT scheme was chosen to maintain a full dose of gemcitabine during CRT and was determined according to preliminary phase I/II studies.73,74 The results demonstrated a higher R0 resection rate (40% versus 71%, p < 0.001), benefits in terms of median disease-free survival (DFS; 7.7 versus 8.1 months, p = 0.032) and median LF-free interval (LFFI; 13.4 months versus not reached, p = 0.003) and significantly lower rates of pathologic lymph nodes (78% versus 33%, p < 0.001) and perineural and venous invasion (73% versus 39%, p < 0.001 and 36 versus 19%, p = 0.024, respectively) in favour of the neoadjuvant CRT arm. However, median OS by intention-to-treat, the primary end point, including survival results of patients with metastatic lesions at diagnostic laparoscopy and unexpected LAPC, was not significantly improved for this arm (16 versus 14.3 months, p = 0.096). 60 A sub-group analysis of patients undergoing R0/R1 surgery after CRT and having started adjuvant CT was performed to allow for comparison with adjuvant trials and showed a large benefit in median OS (35.2 versus 19.2 months, if not resected, p = 0.029). When looking at the BR subgroup only, the median OS is also in favour of the preoperative CRT arm (17.6 versus 13.2 months, p = 0.029). 60 Once again, these results only suggest but do not definitively prove the superiority of the neoadjuvant CRT approach. Furthermore, beyond gemcitabine, new combined CT regimens, such as gemcitabine/nab-paclitaxel and, particularly, FOLFIRINOX, have shown promising improved outcomes in the metastatic and adjuvant settings but now also in the neoadjuvant approach.75–77 Recent studies and meta-analyses have shown neoadjuvant FOLFIRINOX to be the most effective, providing significantly better resection rates and OS compared with other CT regimens.43,78,79 In 2016, Katz et al. published a unique prospective series of 22 BR patients treated with induction CT with 4 cycles of modified FOLFIRINOX followed by CRT (50.4 Gy in 28 fractions with capecitabine). The authors reported a resection rate of 68% and an R0 resection rate of 93% with 13% complete pathological response. The median OS was 21.7 months, demonstrating that this neoadjuvant sequence was feasible despite significant toxicity associated with preoperative treatments (grade ⩾3: 64%). 64
Main ongoing trials
While upfront surgery seems to be less commonly recommended today, favouring the neoadjuvant approach for potentially resectable disease, high-level evidence is still needed and it remains unclear which modality or strategy is the most effective, CT only or CT followed by CRT. Results of randomized phase II/III trials are urgently required. The PREOPANC-2 phase III study from a Dutch group began in June 2018 with a goal of randomising 368 resectable or BR patients in order to compare 8 cycles of neoadjuvant FOLFIRINOX versus preoperative hypofractionated CRT (as previously described) followed by surgery and 4 cycles of adjuvant gemcitabine. 80 In addition, the randomized phase II PANDAS-PRODIGE 44 trial from a French group is recruiting BR patients who will be allocated to 6 cycles of neoadjuvant FOLFIRINOX ± classical CRT (50.4 Gy in 28 fractions with concurrent capecitabine) and will also contribute to answering that question. 81
Locally advanced (unresectable) pancreatic cancer
As we have described for potentially resectable tumours, the role of RT in the management of LAPC is not yet well defined and is an important topic of debate. While the two initial GITSG trials in the 1980s demonstrated a survival advantage for CRT over CT or RT alone,82,83 further randomized trials and meta-analyses have not confirmed these first results84–89 with the exception of the Eastern Cooperative Oncology Group (ECOG) E4201 study. 89 This randomized trial reported a significant improvement in median OS for treatment with CRT compared to gemcitabine alone (11.1 versus 9.2 months, p = 0.017). However, the results of the ECOG E4201 trial should be considered with great caution due to incomplete accrual, including 74 patients instead of the 316 planned. 89 Recent meta-analyses of available randomized trials were not able to demonstrate a statistically significant difference in OS between patients treated with neoadjuvant CT alone versus CRT, except on a subgroup analysis of consolidation CRT after an induction CT of at least 3 months.90,91 The largest phase III study to date to explore this question was the LAP07 trial from the Groupe Coopérateur Multidisciplinaire en Oncologie (GERCOR) that aimed to investigate the benefit of CRT after 4 months of induction CT with gemcitabine ± erlotinib. The trial did not meet its primary endpoint (median OS: 15.2 for CRT versus 16.5 months for CT alone, p = 0.830) despite the fact that CRT was associated with a statistically significant decrease in local progression (32% versus 46%, p = 0.030) and a trend toward improved median progression-free survival (PFS: 9.9 versus 8.4 months for CT alone, p = 0.060). 10 This study had several limitations due to the choice of CT regimen used and the quality of RT. For RT, 88% of patients treated with CRT were assessable for RT quality analysis and, of these, 50% and 18% presented with minor and major RT protocol deviations, respectively. For CT, the LAP07 trial was designed in 2005 before the advent of FOLFIRINOX and gemcitabine/nab-paclitaxel and, therefore, used a non-optimal gemcitabine regimen. In this trial, although loco-regional progression was decreased, the rate of metastatic progression was higher in the CRT arm (60% versus 44% for CT alone, p = 0.040). This implies that with the use of chemotherapies allowing for better control of distant disease, CRT could add more survival benefit. It should also be noted that in the LAP07 trial, the resection rate obtained either after CT alone or after CRT was very low (7% and 3%, respectively) because these treatments were delivered mainly in a conclusive manner with no intention of further surgical exploration except for the few cases where an important response was shown. 10
Interestingly, a meta-analysis by Gillen et al. in 2010 reported that one-third of patients initially classified as unresectable at diagnosis can be successfully resected after neoadjuvant treatment with an estimated median survival of 20.5 months, approximately equivalent to patients who underwent immediate resection. 46 However, given the evolution and high variability of the definitions of resectability of PDAC, some of these patients considered to be LAPC at the time of this trial could currently be classified as BR. More recent non-randomized studies exploring induction with modern combinations of CT over 4–8 cycles followed by CRT in LAPC have reported even more impressive results regarding resection rates (up to 89%), R0 resection rates (70–100%), and median survival (18.1–58 months) (Table 2).10,68,88,89,92,93,94,95,96 In 2018, a large French retrospective trial of highly selected patients with resected PDAC (106 BR and 97 LAPC) treated with induction FOLFIRINOX ± CRT (54 Gy in 30 fractions with concurrent 5-FU or capecitabine) was published. Significant differences were demonstrated in favour of neoadjuvant treatment with FOLFIRINOX+CRT, both in BR and LAPC populations with greatly improved median OS (57.8 versus 35.5 months; p = 0.007), R0 resection rates (89.2% versus 76.3%, p = 0.017), and ypN0 rates (76.2% versus 48.5%, p < 0.001). 62 This neoadjuvant approach, providing true R0 resection, tumour downstaging and downsizing and major pathological response in a selected number of “good” patients with better outcomes suggests that this represents a multi-step selective process for patient selection that could offer a way to improve the prognosis of pancreatic cancer.
Selected modern trials evaluating the role of CRT for locally advanced pancreatic adenocarcinoma (LAPC).
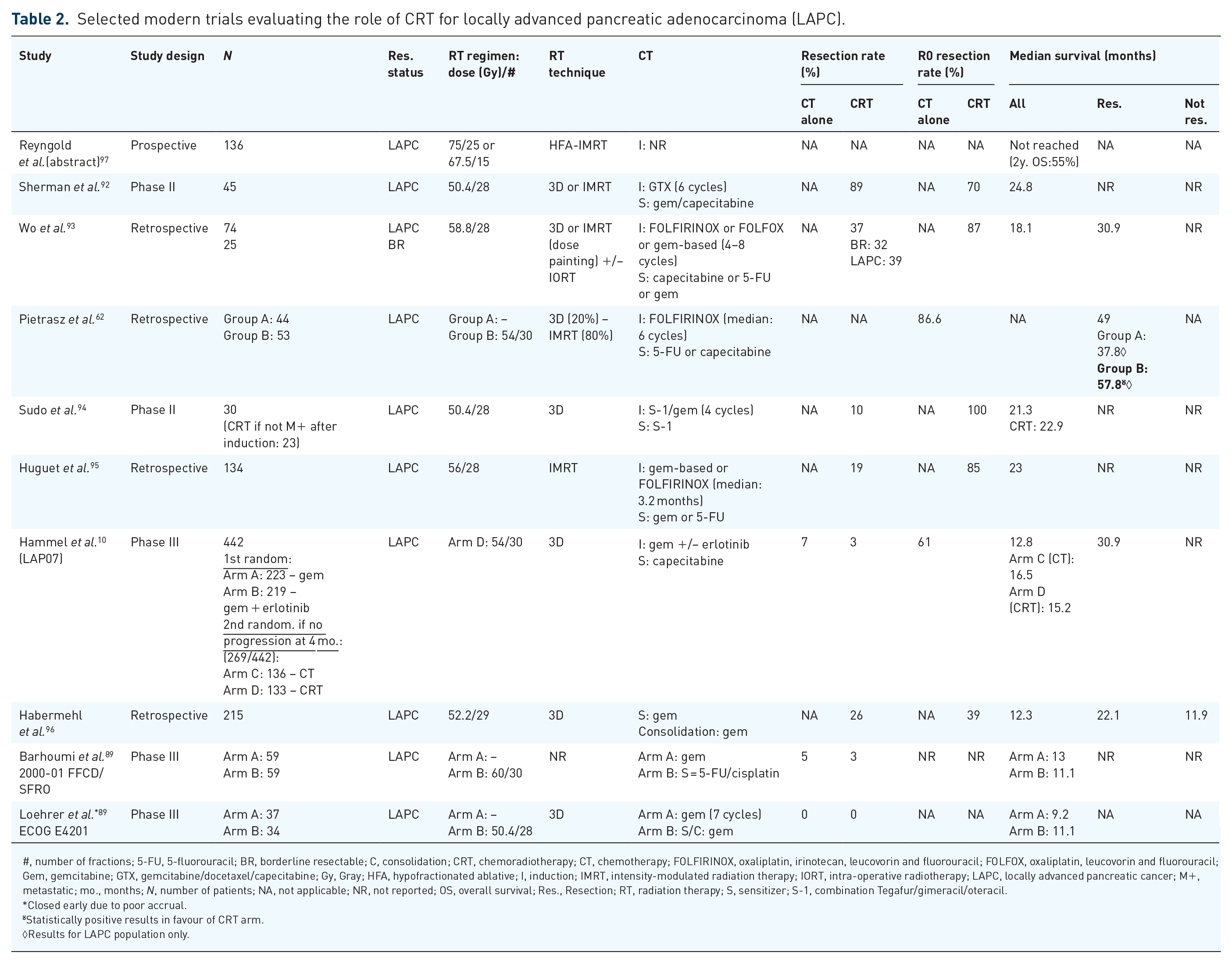
#, number of fractions; 5-FU, 5-fluorouracil; BR, borderline resectable; C, consolidation; CRT, chemoradiotherapy; CT, chemotherapy; FOLFIRINOX, oxaliplatin, irinotecan, leucovorin and fluorouracil; FOLFOX, oxaliplatin, leucovorin and fluorouracil; Gem, gemcitabine; GTX, gemcitabine/docetaxel/capecitabine; Gy, Gray; HFA, hypofractionated ablative; I, induction; IMRT, intensity-modulated radiation therapy; IORT, intra-operative radiotherapy; LAPC, locally advanced pancreatic cancer; M+, metastatic; mo., months; N, number of patients; NA, not applicable; NR, not reported; OS, overall survival; Res., Resection; RT, radiation therapy; S, sensitizer; S-1, combination Tegafur/gimeracil/oteracil.
Closed early due to poor accrual.
Statistically positive results in favour of CRT arm.
Results for LAPC population only.
The use of hypofractionated ablative (HFA)-RT for selected patients after induction CT is also an interesting approach. In a study by Krishnan et al., 200 LAPC patients were treated with induction CT followed by either conventional CRT (50.4 Gy in 28 fractions with concomitant CT) or HFA-IMRT [delivery of biologically effective doses (BED) > 70 Gy, mainly by using a simultaneous integrated boost technique (SIB) in 15 or 28 fractions]. Only 47 patients with tumours more than 1 cm from the closest gastrointestinal (GI) mucosa were treated with HFA-IMRT. The authors reported promising OS (median: 17.8 versus 15 months, p = 0.030; 3-year OS: 31% versus 9%) and local control (median local-regional recurrence-free survival: 10.2 versus 6.2 months, p = 0.050) for HFA-IMRT. Interestingly, no additional toxicity in the HFA-IMRT group was observed and delivery of high BED was the only predictor of improved OS on multivariate analysis. The authors also suggested that concomitant capecitabine could be better tolerated with dose escalation than gemcitabine, cisplatin/5-FU or 5-FU/mitomycin C. 98 Recently, the results of a prospective study from the Sloan Kettering group including 136 LAPC patients treated with definitive HFA-IMRT (BED ⩾ 100 Gy; 75 Gy in 25 fractions or 67.5 Gy in 15 fractions) were presented. With a median follow-up of 12 months, the median OS and freedom from local progression (FFLP) were not reached and the impressive 2-year OS and FFLP were 55% and 78%, respectively, with a safe toxicity profile. 97
Regarding these data, while (C)RT was initially only used as a definitive treatment to prevent or delay local progression, there is now a gradual shift for patients with LAPC toward a neoadjuvant approach followed by surgical exploration in cases of no progression. New RCTs are underway to evaluate the role of modern (HFA)-CRT after induction therapy with more active CT versus CT alone, such as the CONKO-007 trial using FOLFIRINOX, the SCALOP-2 trial using gemcitabine/nab-paclitaxel for induction, and the phase II MAIBE trial that is further exploring the role of HFA-RT (67.5 Gy in 15 fractions or 75 Gy in 25 fractions with concomitant capecitabine).99–101
SBRT
Background
SBRT allows precise delivery of high doses to the tumour in a few sessions (1–5), reducing the dose and toxicity to neighbouring organs at risk (OARs). 102 The SBRT technique is already successfully used, particularly for intracranial tumours and for the treatment of early-stage non-small cell lung cancer in patients who are inoperable or refuse surgery. 103 However, performing an SBRT treatment that targets a pancreatic lesion that may move during respiration in the middle of the upper abdomen is more challenging. Several useful tools and techniques have recently been developed, making SBRT possible for PDAC, including: modern planning methods [IMRT/volumetric modulated arc therapy (VMAT), four-dimensional computed tomography (4D-CT) to assess the amplitude and direction of tumour movement during the respiratory cycle, abdominal compression and breath-hold techniques to restrain tumour movement, endoscopic implantation of fiducial markers into the tumour, and the use of on-board cone-beam computed tomography (CBCT) for daily tumour position verification or tracking.104,105 All these innovations provide reductions in margin expansion and dose escalation to the target volume while safely limiting and controlling dose and toxicity to OARs. In contrast to conventional RT, the SBRT approach seeks to avoid irradiation of large volumes and, therefore, does not include prophylactic irradiation of neighbouring lymph node areas. Owing to the shorter duration of treatment compared to conventional RT (1 week versus 4–6 weeks), patients receiving SBRT can resume systemic therapy more quickly, reducing long interruptions of full-dose chemotherapy.103,104 Another goal of SBRT is to improve local control with the delivery of higher BED to the tumour, since up to 30% of PDAC patients die due to local progression only. 106 Therefore, SBRT has been tested in the treatment of PDAC since the early 2000s with interesting results in terms of feasibility, safety and efficacy, providing high local control, improved (R0-) resection rates and survival.
Clinical data in pancreatic cancer and challenges
History
The development of SBRT for PDAC took place in two main phases. During the first decade of the 2000s, studies explored pancreatic SBRT in different sequences (alone, with induction CT, as a boost after CRT) with very good local control rates (LCR, generally > 85% at 1 year) but with little or no impact on median survival. These early studies, usually using a single fraction with very high dose per fraction (15–25 Gy), reported unacceptably high rates of grade 3–4 GI toxicity up to 22.6%, leading to a new disappointment for radiation oncologists.107–113 Subsequently, during the second decade of the 2000s, further retrospective or phase II trials reported results on the use of fractionated SBRT (3–5 fractions) with softer hypofractionation (mainly 5–6.6 Gy per fraction), that attempted to respect strict GI constraints, particularly for the duodenum. These studies reported acceptable rates of acute and late grade ⩾3 GI toxicity, with risks generally between 0% and 10% and consisting mainly of GI bleeding, ulcers, stenosis, perforations or gastroparesis.114–128 Overall, fractionated SBRT treatments are well tolerated, showing less acute toxicity than IMRT-CRT and similar perioperative complication rates.129–132 The main studies that have reported the use of this approach in this setting are summarized in Table 3.
Selected historical and modern trials evaluating the role of SBRT for pancreatic adenocarcinoma.

#, number of fractions; BR, borderline resectable; C, consolidation; CRT, chemoradiotherapy; CT, chemotherapy; FOLFIRINOX, oxaliplatin, irinotecan, leucovorin and fluorouracil; FOLFOX, oxaliplatin, leucovorin, and fluorouracil; Gem, gemcitabine; GI, gastrointestinal; GTX, gemcitabine/docetaxel/capecitabine; Gy, Gray; I, induction; LAPC, locally advanced pancreatic cancer; LC, local control; Linac, linear accelerator; N, number of patients; NA, not applicable; NR, not reported; R, resectable; RT, radiation therapy; S, sensitizer; SBRT, stereotactic body radiation therapy; SIB, simultaneous-integrated boost; TVI, tumour–vessel interface.
Results concerns LAPC only even if other PDAC status were included in the studies, excepted if clearly mentioned in the table.
SBRT in the neoadjuvant PDAC setting
While the main indication for SBRT was initially the definitive treatment of LAPC, some trials have investigated the role of SBRT for potentially resectable PDAC and LAPC in a neoadjuvant setting and these are summarized in Table 3.113,114,123–127 The SBRT technique can be easily integrated into a neoadjuvant approach to target the tumour with a particular concern for the areas of contact between the tumour and blood vessels that are called the tumour–vessel interfaces (TVIs) where an integrated boost should be applied whenever possible. These TVIs are very important for limiting the possibility of curative resection outside the metastatic context and attempts to sterilize these areas could increase (R0) resection rates. 132 This hypothesis seems to be confirmed by the results of available phase I/II and retrospective studies showing very high rates of R0 resection for BR and LAPC patients treated with SBRT (84–97.5%) (Table 3).113,114,120–127 However, it is now well known that a major issue with the use of modern multi-agent CT and RT is the difficulty of predicting resectability after neoadjuvant treatment by imaging assessment.133,134 Indeed, few patients show an improvement in the number and degree of TVIs after neoadjuvant treatment due to insufficient differentiation of residual tumour versus desmoplasia, particularly at TVIs.66,133,134 For illustration, in the study by Kluger et al., 61 LAPC patients who failed to regress from >180° encasement of coeliac, superior mesenteric or hepatic arteries after receiving neoadjuvant therapy (induction CT principally gemcitabine-based or FOLFIRINOX followed by RT with IMRT or SBRT technique) were systematically surgically explored. While 8% were metastatic at laparoscopy, the remaining 56 patients were resected with an R0 resection rate of 80.4% (defined as no malignant cells within 1 mm of any margin) and an impressive median OS from the beginning of neoadjuvant therapy of 28.9 months. 135 New imaging modalities are currently being explored to improve appropriate selection of patients for surgery such as positron emission tomography (PET) or advanced diffusion-weighted imaging magnetic resonance imaging (DWI-MRI).136,137 It is now uniformly recommended to perform systematic surgical exploration in non-metastatic and non-locally progressive operable patients with localized PDAC, even if there is no evidence of radiographic down-staging after modern-era neoadjuvant strategies.
Clinical development and limitations of SBRT in PDAC
The only analysis that pooled 19 SBRT trials for LAPC patients demonstrated a median OS of 17 months (range 5.7–47 months), a 1-year OS rate of 51.6% and a 1-year LCR of 72.3%. Heterogeneity was high between studies and most of them were small retrospective series. 138 The dose and the number of fractions delivered were highly variable and an optimal scheme for pancreatic fractionated SBRT was not clearly established. However, reducing the dose too much to ensure safety, as is commonly done in current practice, is not a solution, as the fractionation schemes of 25–33 Gy in 5 fractions correspond to a maximal BED of 55 Gy, well below the ablative doses sought with SBRT. It is, therefore, not surprising that the survival benefit usually obtained with this low-BED SBRT is modest and that the local control is weaker than that observed with the first historical SBRT analyses of non-randomized studies available (Table 3).107–128 This modest survival benefit of SBRT over CRT seems to be confirmed by the results of three large retrospective studies using the National Cancer Center Database and one recent meta-analysis.117,139,140 To illustrate for LPAC, in the meta-analysis by Tchelebi et al., SBRT, defined as RT delivered at ⩾5 Gy per fraction, was associated with a modest benefit for 2-year OS (26.9 versus 13.7 months for CRT, p = 0.004) but OS differences were not statistically significant at 1 year (53.7% versus 49.3%, p = 0.630). 140 For resectable and BR PDAC, Jiang et al. retrospectively studied 5828 patients treated with different neoadjuvant treatments before pancreatectomy including 332 with CT followed by SBRT (defined as ⩾6 Gy per fraction). Although the SBRT group contained more stage cT3–T4 patients, a survival improvement was shown compared with CT alone or CT+conventional CRT and persisted after propensity score-matching with median OS of 32.1, 27.5 and 27.1 months (p = 0.013), respectively. The R0 resection rate was higher in the RT groups than with CT alone (p < 0.001) and the SBRT group was also associated with better T/N-stage downstaging (p < 0.001). 141 Substantial expectations were placed upon the randomized phase II Alliance A021501 trial designed to compare the outcomes of BR patients treated with induction with FOLFIRINOX alone or followed by SBRT (33 Gy in 5 fractions with SIB up to 40 Gy at TVI or 25 Gy in 5 fractions). 142 Initially this trial included three arms, but due to the results of the LAP07 trial, the FOLFIRINOX followed by conventional CRT arm was cancelled. 143 Unfortunately, the study was recently suspended following an interim analysis of 30 patients revealing crossing of the futility boundary for R0 resection rates for the SBRT arm.127,144 Taking into account all these data, and despite the lack of level I evidence, the NCCN, ASCO, ASTRO and the American College of Radiobiology (ACR) guidelines have already listed SBRT as an optional treatment for localized PDAC in experienced, high-volume centres.2,14,58,59,145
It is essential to continue to improve the pancreatic SBRT technique, in particular by trying to deliver very high BED to the target while maintaining a safe toxicity profile. Indeed, delivery of a BED10 ⩾60 Gy (α/β = 10) seems correlated with improved OS and PFS on multivariate analysis. 146 The progressive availability of magnetic resonance linear accelerator (MR-linac) systems in high-volume RT centres could be an elegant option for providing high-dose delivery. Using the stereotactic MR-guided adaptive RT (SMART) technique, Rudra et al. treated 44 BR or LAPC patients with different RT schemes including high-dose SBRT (BED ⩽70 Gy group: 40–55 Gy in 25–28 fractions or 30–35 Gy in 5 fractions; BED > 70 Gy group: 50–67.5 Gy in 10–15 fractions or 40–52 Gy in 5 fractions). The authors reported a 2-year OS of 49% versus 30% (p = 0.030) in favour of the high-dose group but only six patients underwent surgery after completion of RT and high-dose RT did not predict OS in multivariate analysis. 147 A prospective phase II multi-institutional trial opened in 2019 with the goal of investigating the SMART technique (50 Gy in 5 fractions) for BR and LAPC patients. 148
Another limitation of SBRT in this setting could be the failure of durable local control following low-BED SBRT owing to the limited irradiated volume. Dholakia et al. generated a map of local recurrences from 202 heterogeneously treated PDAC with or without RT. Forty-five per cent of these patients presented with an LF and 90% of these LFs could be covered using a method of asymmetric Boolean extension from the superior mesenteric artery (SMA) and coeliac trunk of 1–3 cm. 149 These perivascular tissues are not systematically covered by pancreatic SBRT and could explain the important rates of LF reported in some studies.127,150 A recent example is provided by the phase II study from Kharofa et al. in which 18 BR patients were treated with 3 cycles of multi-agent CT followed by SBRT (33 Gy in 5 fractions with an optional elective 25 Gy volume to the at-risk vasculature). Surgery was performed in 12 patients with 92% of R0 resections. The median OS and PFS were 21 and 11 months, respectively, with LF predominantly observed outside the planning target volume (PTV) 33 Gy. 127
Numerous studies are underway to further explore and evaluate the role of SBRT in PDAC, especially in the neoadjuvant setting. A randomized phase II study was recently opened for recruitment by the Medical College of Wisconsin, the SOFT Preop study, for resectable and BR patients who will be randomized between neoadjuvant SBRT versus CRT + CT. 151 For LAPC patients, a phase III trial from Stanford University is recruiting 172 patients randomized between induction with up to 4 cycles of FOLFIRINOX alone versus FOLFIRINOX + SBRT. 152
Future challenges
As distant and regional recurrence remains a problem for a majority of localized PDAC patients, even when they are treated with the best current standard of care, the emergence of new systemic innovative targeted therapies is awaited. Until now, results of trials using single- or dual-checkpoint immunotherapy in PDAC have not made the expected breakthrough as PDACs, except for a few patients with MSI, appear to be unresponsive.153–156 This failure is largely explained by the high capacity of immune escape owing to the complex tumour microenvironment of PDAC that contains abundant desmoplastic stroma and immunosuppressive cells. 157 Various combinations with checkpoint immunotherapy are currently under study, including: a/plus CT with some encouraging results, such as the recent phase Ib studying triple combination of gemcitabine/nab-paclitaxel with anti-CD40 and anti-PD-1 in a first-line metastatic setting 158 or the phase Ib study combining FOLFIRINOX with anti-CCR2 and additional neoadjuvant CRT at the discretion of the tumour board for BR and LAPC patients; 159 b/plus modulators of the stroma, such as pegvorhyaluronidase alfa (PEGPH20); 160 c/plus immunocytokines in an effort to boost anti-tumoural immunity;157,161 d/plus RT, particularly SBRT as an immune priming treatment. Modern, highly localized SBRT techniques can partly spare local lymphatics and have the potential to trigger immune responses through multiple pathways such as: induction of immune cell death, delivery of new antigens, activation of the cGAS-STING pathway, local recruitment of T cells and transient overexpression of specific receptors at the surface of tumour cells rendering them more vulnerable to cytotoxic T-cell killing.157,162,163 Although optimal dose, fractionation and timing between RT and immunotherapy are not well established and appear to vary widely depending on the context, a multitude of phase I/II trials are underway to explore these innovative immuno-SBRT combinations, including some for PDAC.162,164
Heavy-particle therapy: proton and carbon-ion therapy
Heavy-particle beam therapy takes advantage of a particular physical characteristic with an energy release inversely proportional to the square of its velocity. The result is a very conformal dose deposit, as the particle delivers a low dose at the entry and most of its energy to a peak called the ‘Bragg peak’ just before it stops. Therefore, particle therapy is expected to offer interesting perspectives in PDAC by limiting toxicity to the many surrounding OARs and allowing dose escalation at the tumour level. 165 Most of the heavy-particle centres in the world are equipped with proton therapy facilities but there are many other particles that can be exploited in RT, including carbon ions ( 12 C-ions). Compared with photon- or proton-based RT, 12C-ion therapy may also offer the advantage of better local control of radioresistant tumours through higher linear energy transfer, resulting in more effective DNA damage to cancer cells, reduced oxygen effect and less cell cycle-related radiosensitivity. 166 As 12C-ion facilities are increasing but still limited worldwide, studies exploring this technique for PDAC are rare. Results of the few published phase I/II and retrospective studies have demonstrated promising results with median OS up to 25.1 months for LAPC patients included in the higher-dose groups (Table 4).167–174 However, toxicity outcomes should be carefully considered as some trials have reported high GI toxicity following CRT with particle therapy. A dosimetric analysis between IMRT and proton plans in LAPC reported a decrease in low and intermediate doses at OAR volumes, but an increase in the high-dose region to the duodenum and stomach. 174 Another in silico analysis using fraction dose calculations on CBCT for PDAC with photon, proton and 12C-ion plans reported that photon plans were highly robust regarding interfractional anatomical changes in contrast to heavy-particle plans where severe adaptive reductions in target dose coverage were observed. 175 Similarly, a prospective study in which endoscopy was performed after proton-based CRT with concurrent gemcitabine demonstrated appearance of RT-induced ulcers in the stomach and duodenum in 49.4% of the 91 patients investigated, although no bleeding or perforations were described. 176 Therefore, particle therapy should be used with caution for moving GI targets, particularly for investigating dose escalation as this technique could deliver very high BED to OAR in cases of slight inter/intrafractional and set-up modifications of their position. Use of strict management of tumour and OAR motion with dedicated devices such as tracking or 4D treatment planning is, therefore, highly recommended and the development of new delivery techniques such as pencil-beam scanning intensity-modulated proton therapy (IMPT) could improve the dosimetric advantage of particle therapy over photon.177–179 Regarding outcomes, although a retrospective data-based model of CRT in LAPC predicted an advantage of hypofractionated particle therapy over standard photon RT for 1-year OS, there are still no available results from randomized trials comparing the efficacy and toxicity outcomes of photon versus proton or 12C-ion therapy. 180 A phase III trial comparing 12C-ion therapy with photon IMRT in LAPC followed by four cycles of gemcitabine/nab-paclitaxel has recently opened for recruitment. 181
Selected trials evaluating the role of heavy-particle therapy for pancreatic cancer.

#, number of fractions; C, consolidation; CRT, chemoradiotherapy; FOLFIRINOX, oxaliplatin, irinotecan, leucovorin and fluorouracil; Gem, gemcitabine; GI, gastrointestinal; GTX, gemcitabine/docetaxel/capecitabine; GyE, Gray equivalent; I, induction; IPMT, intensity proton modulated therapy; LAPC, locally advanced pancreatic cancer; LC, local control; N, number of patients; NR, not reported; R, resectable; RBE, radiobiological equivalent; S, sensitizer; S-1, combination Tegafur/gimeracil/oteracil.
Conclusions and perspectives
After decades of discussion and investigation, the role of RT in the treatment of primary PDAC has not yet been established. Currently, except for its well-proven benefit in local control, conventional RT treatment cannot be formally recommended in either adjuvant or neoadjuvant approaches as a result of the recently published randomized studies showing no survival benefit of adding RT to CT. However, the final results of ongoing phase III trials using modern high-dose RT techniques, which have already reported encouraging preliminary data, are eagerly awaited. These trials are summarized in Table 5 and a comparison between modern conventional CRT, SBRT and HFA-RT for the treatment of localized PDAC in the neoadjuvant setting is summarized in Table 6. In particular, the integration of hypofractionated SBRT or HFA-RT into modern neoadjuvant treatment regimens (FOLFIRINOX or gemcitabine/nab-paclitaxel) seems to be the most promising for resectable, BR and LAPC pancreatic cancer. These options for neoadjuvant sequence allow optimization of PDAC patient selection and are expected to demonstrate their superiority by improving resectability rates and clinical outcomes of PDAC patients with curative intent. Moreover, while LAPC patients were definitively treated with (R)CT several years ago, it has become clear that these patients can now also benefit from these modern neoadjuvant treatments with resection rates of up to about 40%. These resected LAPC patients now show increased survival times that were previously not considered for this category of patients. Well-designed trials should also focus on and integrate a strict definition of tumour (non-)resectability. In light of the above, the place of RT in the field of localized PDAC is an open question and the development of new techniques (SBRT, HFA-IMRT, heavy-particle therapy and combinations with immunotherapy) must be investigated further in good quality randomized studies.
Radiotherapeutic perspectives for potentially resectable (R & BR) and locally advanced pancreatic adenocarcinoma (LAPC).
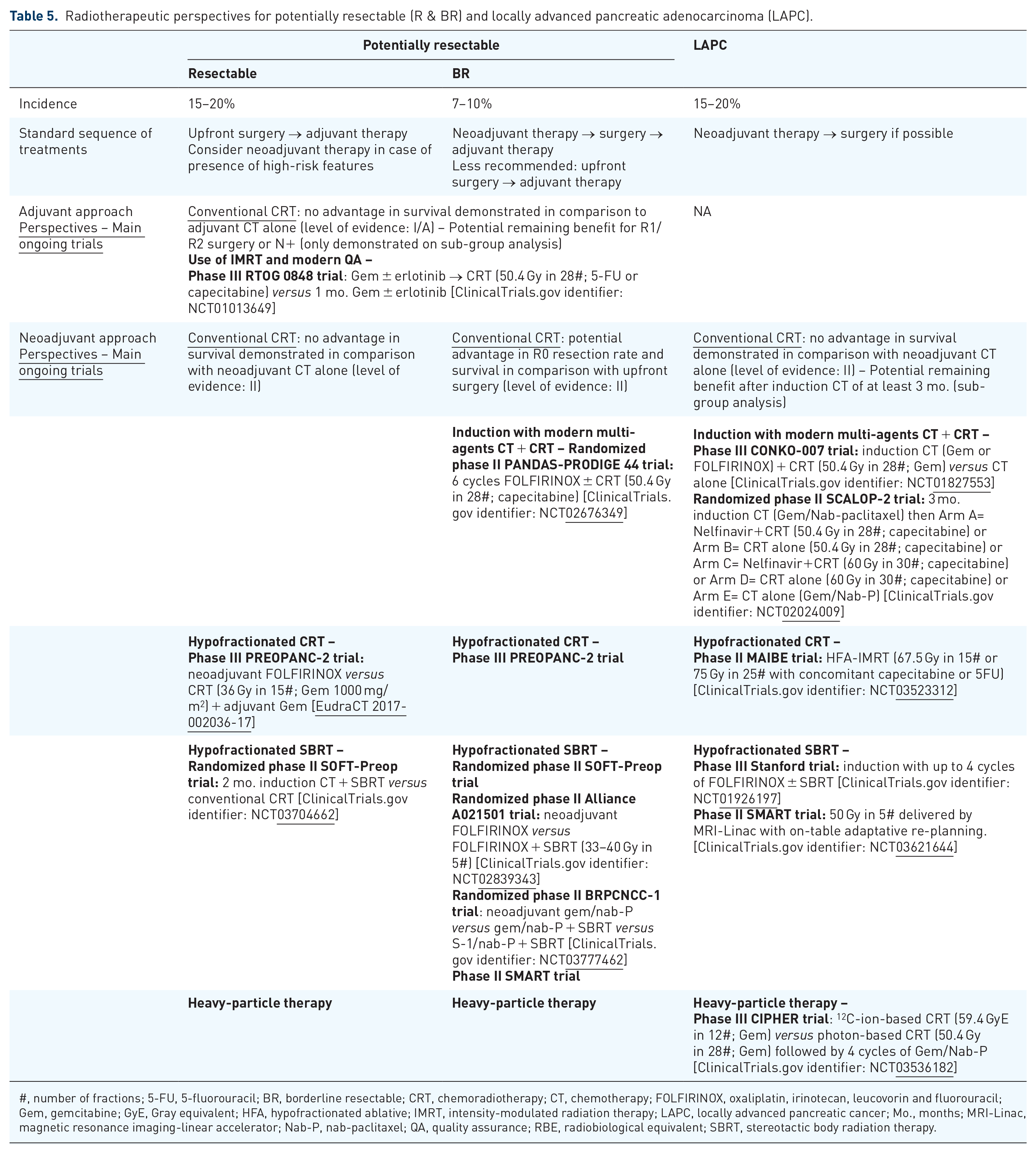
#, number of fractions; 5-FU, 5-fluorouracil; BR, borderline resectable; CRT, chemoradiotherapy; CT, chemotherapy; FOLFIRINOX, oxaliplatin, irinotecan, leucovorin and fluorouracil; Gem, gemcitabine; GyE, Gray equivalent; HFA, hypofractionated ablative; IMRT, intensity-modulated radiation therapy; LAPC, locally advanced pancreatic cancer; Mo., months; MRI-Linac, magnetic resonance imaging-linear accelerator; Nab-P, nab-paclitaxel; QA, quality assurance; RBE, radiobiological equivalent; SBRT, stereotactic body radiation therapy.
Global comparison between conventional chemoradiotherapy and emerging dose-escalated treatments for the neoadjuvant treatment of localized pancreatic adenocarcinoma.

#, fraction; 3D-CRT, 3-dimensional conformal radiotherapy; 4D-CT, four-dimensional computed tomography; BED, biological equivalent dose; BR, borderline resectable; CBCT, cone beam computed tomography; CRT, chemoradiotherapy; CT, chemotherapy; DIBH, deep inspiration breath hold; ENI, elective nodal irradiation; GI, gastrointestinal; Gy, Gray; IMRT, intensity-modulated radiation therapy; LAPC, locally advanced pancreatic cancer; Linac, linear accelerator; MRI, magnetic resonance; PDAC, pancreatic adenocarcinoma; RT, radiotherapy; SBRT, stereotactic body radiation therapy; SIB, simultaneous integrated boost; TVI, tumour–vessel interface; VMAT, volumetric modulated arc therapy.
Footnotes
Acknowledgements
The authors want to thank Tatjana Arsenijevic for her proofreading of the manuscript. The authors would like to acknowledge the contribution of a medical writer, Sandy Field, PhD, for language editing of this manuscript.
Author contributions
CB drafted and designed the manuscript; JN/JC/AH/DVG contributed to major review of the manuscript; LM/JLVL contributed to review and concept supervision of the manuscript; all authors reviewed and edited the manuscript, gave critical input and gave final approval for publication.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a doctoral grant from the ‘Amis de l’Institut Bordet’ [grant number: 2019-31] and by the ‘Fonds de la Recherche Scientifique – FNRS’ [grant number: FC 33593] (CB).