
Abstract
Poly(ADP-ribose)polymerase (PARP) inhibitors are targeted therapy for cancers with homologous repair deficiency (HRD). They were first approved for ovarian cancer and have changed current treatment strategies. They have also demonstrated efficacy in HER2-negative metastatic breast cancer and advanced prostate cancer with BRCA1/2 or ATM mutations. Patients with somatic and/or germline BRCA1/2 mutations benefit more from these treatments than other patients. Nowadays, the diagnosis of HRD is largely based on germline genetic testing, which is performed after an in-person genetic counseling session, even for patients without any family history of cancer. However, with the increasing number of PARP inhibitor indications across different tumor types, rapid access to oncogenetic consultations will become a challenge. To meet this demand, tumor genomic testing could be offered at initial diagnosis. Telephone counseling and other referral systems could replace in-person consultations for certain subgroups of patients deemed to have a low risk of harboring a germline mutation. This article reviews international guidelines for genetic counseling testing. We herein propose new care pathways for breast, prostate and ovarian cancers, including tumor genomic testing at initial diagnosis in order to help triage genetic counseling referrals.
Background
Anti-poly(ADP-ribose)polymerase (PARP) therapies have been developed for various solid tumors such as ovarian, breast and prostate cancers, mainly based on BRCA1/2 (Breast Cancer 1 or 2 genes) mutations. A BRCA-like phenotype, which has been described in ovarian cancer, is a tumor phenotype with high sensitivity to platinum-based chemotherapies and PARP inhibitors, and may be due to either an alteration of the genes involved in homologous repair or functional deficiency.1,2 Recent research has shown that the BRCA-like profile is also associated with non-BRCA1/2 mutations such as RAD51 and ATM mutations, widening the concept to a so-called homologous repair deficiency (HRD) profile. 3 Next-generation sequencing (NGS) is used in blood, saliva or tissue samples to sequence genes involved in homologous repair in order to detect germline mutations and in tumor tissue to detect somatic mutations. PARP inhibitors have shown some efficacy in ovarian, breast and prostate patients with deleterious BRCA1/2 mutations, but also in ovarian patients with a BRCA-like phenotype. Olaparib was the first PARP inhibitor to receive US Food and Drug Administration (FDA) approval for advanced ovarian cancer patients with a germline or somatic BRCA1/2 mutation who had received three or more prior lines of treatment.4,5 Altogether, somatic and/or germline BRCA1/2 mutations are present in only 20% of epithelial ovarian cancers.6,7 In the recurrent setting, for patients with a BRCA1/2 mutation, maintenance olaparib following response to platinum-based chemotherapy increased median progression-free survival (PFS) from 5.5 months in the placebo group to 19.1 months in the olaparib group. 4
PARP inhibitors have shown efficacy not only in ovarian cancer patients with BRCA1/2 mutations but also, to a lesser extent, in patients with other HRD and BRCA-like profiles. Coleman and colleagues demonstrated in the ARIEL3 study that rucaparib maintenance after platinum chemotherapy for recurrence significantly enhanced median PFS in patients with BRCA1/2 mutations by 16.6 months, and in those with the BRCA-like phenotype by 13.6 months. 8 The NOVA study also showed a significant difference in survival between BRCA1/2 mutated and non-mutated patients treated with niraparib, another PARP inhibitor, as maintenance therapy. 9 The best response to niraparib was for patients with germline BRCA1/2 mutations, with 21 months of median PFS versus 12.9 months for patients with a HRD mutation but without a BRCA1/2 germline mutation. Moreover, olaparib has shown 34% objective response rate as monotherapy in recurrences for patients with germline BRCA1/2 mutations and after at least three therapeutic lines. Recently, the efficacy of PARP inhibitors was confirmed in the SOLO1 study in a first-line setting for BRCA1/2 mutated patients with a 60.4% rate of freedom from disease progression at 3 years in the maintenance olaparib group after platinum chemotherapy, compared with 27% in the placebo maintenance group [hazard ratio (HR) for disease progression or death, 0.28; 95% confidence interval (CI): 0.20–0.39; p < 0.001]. 10
Olaparib and other PARP inhibitors have also been evaluated in other solid tumors based on a somatic or germline homologous recombination defect. In the OlympiAD trial, patients with HER2-negative metastatic breast cancer with a germline BRCA1/2 mutation received olaparib as first- or second-line treatment, with an increase in median PFS from 4.2 to 7 months. 11 Another PARP inhibitor, talazoparib, has also shown similar efficacy in HER2-negative metastatic or locally advanced breast cancer patients with a germline BRCA1/2 mutation with a median PFS of 8.6 months in the group treated with talazoparib versus 5.6 months in the control group, receiving physician’s choice of single-agent therapy. 12
Among patients with castration-resistant prostate cancer, Mateo and colleagues found that 88% of the patients with a somatic homologous recombination defect (BRCA2, ATM, etc.) responded to olaparib after one or two regimens of chemotherapy. 13 Recently, rucaparib also showed efficacy among patients with BRCA1/2-mutated prostate cancer (preliminary results of TRITON2 have been presented at ESMO 2018). 14
As a result, the US FDA has approved olaparib and talazoparib as a treatment for HER2-negative metastatic breast cancer with a BRCA1/2 germline mutation and given olaparib a Breakthrough Therapy Designation for the treatment of BRCA1/2 or ATM-mutated metastatic castration-resistant prostate cancer. Rucaparib has received a Breakthrough Therapy Designation for the treatment of BRCA1/2-mutated metastatic castration-resistant prostate cancer. In addition, PARP inhibitors are being tested in clinical trials in other settings such as pancreatic cancer, small cell lung cancer and gastric cancer (ClinicalTrials.gov identifiers: NCT02184195, NCT01082549, and NCT03427814).
Since the number of indications for PARP inhibitors is increasing, the number of patients requiring genetic counseling and testing is also likely to increase. However, not all these patients have a familial predisposition and/or germline genetic mutation. In ovarian cancer, the prevalence of BRCA1/2 mutations varies with age at diagnosis. After 70 years, fewer than 1–10% of patients without a family history present an inherited BRCA1/2 mutation versus 12–28% for younger patients.15–17 Previously, oncogenetic consultations focused on familial predisposition with a view to providing genetic counseling in cases in which a germline mutation was detected. Family history and pedigrees are obtained by oncogeneticists or genetic counselors. They explain genetic information to patients and obtain informed consent for DNA testing before samples can be taken. Patients are informed about genetic predispositions and their implications, for them and their families. Waiting periods to access an oncogenetic consultation can be long, exceeding 6 months in some countries. With the advent of PARP inhibitors for the treatment of many cancers, the aim of genetic counseling has changed. Consultations are not only dedicated to counseling patients about genetic predisposition, but are also needed to develop therapeutic strategies. Oncologists, oncogeneticists and molecular biology platforms have to continue to update their organization and protocols to include homologous repair gene testing.
This article reviews international guidelines on indications for oncogenetic counseling, considering family predisposition and therapeutic indications, and proposals for new referral systems in ovarian, breast and prostate cancer based on personal or familial history of cancer, type of tumor and PARP inhibitor indications.
Methods
This review was conducted in accordance with PRISMA guidelines. PubMed, Cochrane, Medline and Google Scholar were used to index medical guidelines and publications reporting prevalence of somatic and/or germline mutations in ovarian, breast and prostate cancer, using appropriate search terms. Papers published in either English or French were eligible. The literature search used variations and Boolean connectors of the key terms. An exploratory search was conducted with the various associations of the terms (MESH if possible) ‘genetic counselling’, ‘genetic testing’, ‘breast neoplasms’, ‘prostate neoplasms’, ‘BRCAness’, ‘BRCA1 genes’, ‘BRCA2 genes’, ‘breast cancer, prostate cancer, ovarian cancer, familial’, ‘guideline’, ‘recommendation’, ‘neoplastic syndromes, hereditary’, ‘multi-gene panel’. The websites of associations, colleges and learned societies listing the various recommendations were also examined.
For the selection of guidelines, we considered only the recent and national guidelines or recommendations for oncogenetic care and indications for genetic testing, published in English and/or French until September 2018. First, articles were screened on titles and publication dates, excluding duplicates, surgical, molecular, technical or psychological articles. The different steps are summarized in Figure 1.

Flow chart of the systematic review following PRISMA guidelines.
Results
Twenty-four recommendations for oncogenetic care and indications for genetic testing were examined (Figure 1). The indications for PARP inhibitors are summarized in Table 1.
Indications of PARP inhibitors.

BC, breast cancer; EMA, European Medical Agency; FDA, Food and Drug Administration; OC, ovarian cancer; PC, prostate cancer.
Ovarian cancer
Given the results confirming the efficacy of olaparib, the first FDA-approved PARP inhibitor, most guidelines have extended indications for germline genetic testing at diagnosis to all patients with high-grade serous non-mucinous epithelial ovarian cancer, whatever the patient’s age.4,6,15–28 Some guidelines even suggest extending this indication to other histology types (NICE, GECKO).26,27 These recommendations are reinforced by the SOLO2 results, as patients with endometrioid ovarian cancer were also included in this study. 5 The indications for germline genetic testing in ovarian cancer according to the different guidelines are summarized in Table 2.
Indications for addressing and/or genetic analyses in case of ovarian cancers.

ACOG, American College of Obstetricians and Gynecologists; AGO, Association of Gynecologic Oncology; BC, breast cancer; ESMO, European Society for Medical Oncology; GECKO, Genetics Education Canada – Knowledge Organization; INCA, Institut National du Cancer; NBCG, Norwegian Breast Cancer Group; NCCN, National Comprehensive Cancer Network; NICE, National Institute for Health; OC, ovarian cancer; SEOM, Sociedad Española de Oncología Medica.
1 including cancer of the peritoneum and fallopian tubes should be considered a part of the spectrum of the hereditary breast and OC syndrome.
2 indication for referral and not for testing.
4 close relative: defined as a first-degree relative (mother, sister, daughter) or second-degree relative (grandmother, granddaughter, aunt, niece).
Nowadays, a genetic consultation is recommended for all patients with high-grade non-mucinous epithelial ovarian cancer at initial diagnosis, in order to facilitate genetic testing for germline and somatic BRCA1/2 mutations, irrespective of the patient’s age or family history. In patients with recurrent ovarian cancer who have not previously undergone genetic testing and with no family history of cancer, some guidelines propose systematic referral for oncogenetic counseling.
In some countries such as France, for patients without prior oncogenetic testing and with a platinum-sensitive recurrence, rapid-access genetic testing pathways have been developed to decrease the time to consultation (<3 months) and have been validated by the French National Cancer Institute. 25 The indication for tumor testing has also been included in the guidelines in addition to germline testing. This somatic testing is done at the same time as the first germline genetic test, or can be prescribed for patients with prior negative germline genetic testing. For patients with platinum-sensitive recurrence and without prior germline screening, tumor and germline testing are recommended at the same time. For patients with germline-negative screening, tumor testing is mandatory. With the new results of the SOLO1 study confirming the efficacy of olaparib as first-line maintenance treatment among patients with BRCA1/2 mutations, care pathways will need to be streamlined. 10
Breast cancer
The recommendations are presented in Table 3.
Indications for addressing and/or genetic analyses in the case of breast cancers.

ACOG, American College of Obstetricians and Gynecologists; AGO, Association of Gynecologic Oncology; ASCO, American Society of Clinical Oncology; BC, breast cancer; BeSHG, Belgian Society for Human Genetics; ESMO, European Society for Medical Oncology; GECKO, Genetics Education Canada – Knowledge Organization; INCA, Institut National du Cancer; NBCG, Norwegian Breast Cancer Group; NCCN, National Comprehensive Cancer Network; NICE, National Institute for Health; OC, ovarian cancer; PC, prostate cancer; SEOM, Sociedad Española de Oncología Medica; SIGN, Scottish Intercollegiate Guidelines Network.
1 including cancer of the peritoneum and fallopian tubes should be considered a part of the spectrum of the hereditary breast and OC syndrome.
2 indication for referral and not for testing.
3 close blood relatives include first-, second-, and third-degree relatives on same side of family (NCCN).
4 close relative: defined as a first-degree relative (mother, sister, daughter) or second-degree relative (grandmother, granddaughter, aunt, niece).
There are some small differences between guidelines but they generally recommend genetic counseling for patients with breast cancer at an early age, or in the event of triple-negative synchronous or metachronous bilateral breast cancer, or combined with ovarian cancer, or a family history of breast cancer, male breast cancer, or ovarian cancer.18–20,23,26–30 In addition, Ashkenazi, Icelandic or French-Canadian heritage are also risk factors for BRCA1/2 mutations.19,20,23,26,27 Some guidelines propose complex predictive scores such as the BODICEA, BRCAPRO and Manchester scores to determine the level of risk. These scores estimate the risk of a person having a germline mutation according to their personal and familial history and determine the indication for genetic testing.19,20,26,27,31,32
Unlike ovarian cancer, there have been no recent modifications of the guidelines concerning the indications for oncogenetic counseling in association with indications for PARP inhibitors. However, the FDA has recently approved olaparib for patients with HER2-negative metastatic breast cancer and a BRCA1/2 germline mutation and talazoparib for HER2-negative metastatic or locally advanced breast cancer and a BRCA1/2 germline mutation (Table 1).11,12 Consequently, requests for clinical counseling are likely to increase considerably. For these patients, rapid access to genetic counseling is necessary, but delays are still very long in many countries. Moreover, the possibility for tumor testing of HRD genes has not been included in the guidelines for this group of patients, and access to classical genetic counseling could shortly become an acute problem.
Prostate cancer
Few guidelines are available regarding oncogenetic counseling for familial risks of prostate cancer (Table 4). Germline mutations affect fewer than 3% of prostate cancer patients. Only patients with early (<55 years) and/or aggressive prostate cancer (Gleason ⩾ 7), associated with an evocative familial history of breast cancer (early, triple-negative, bilateral, multiple), ovarian cancer or other Gleason ⩾ 7 prostate cancers are referred to oncogenetic counseling (especially in the USA and Australia).20,21,29,33
Indications of addressing and/or genetic analyses in case of prostate cancers.
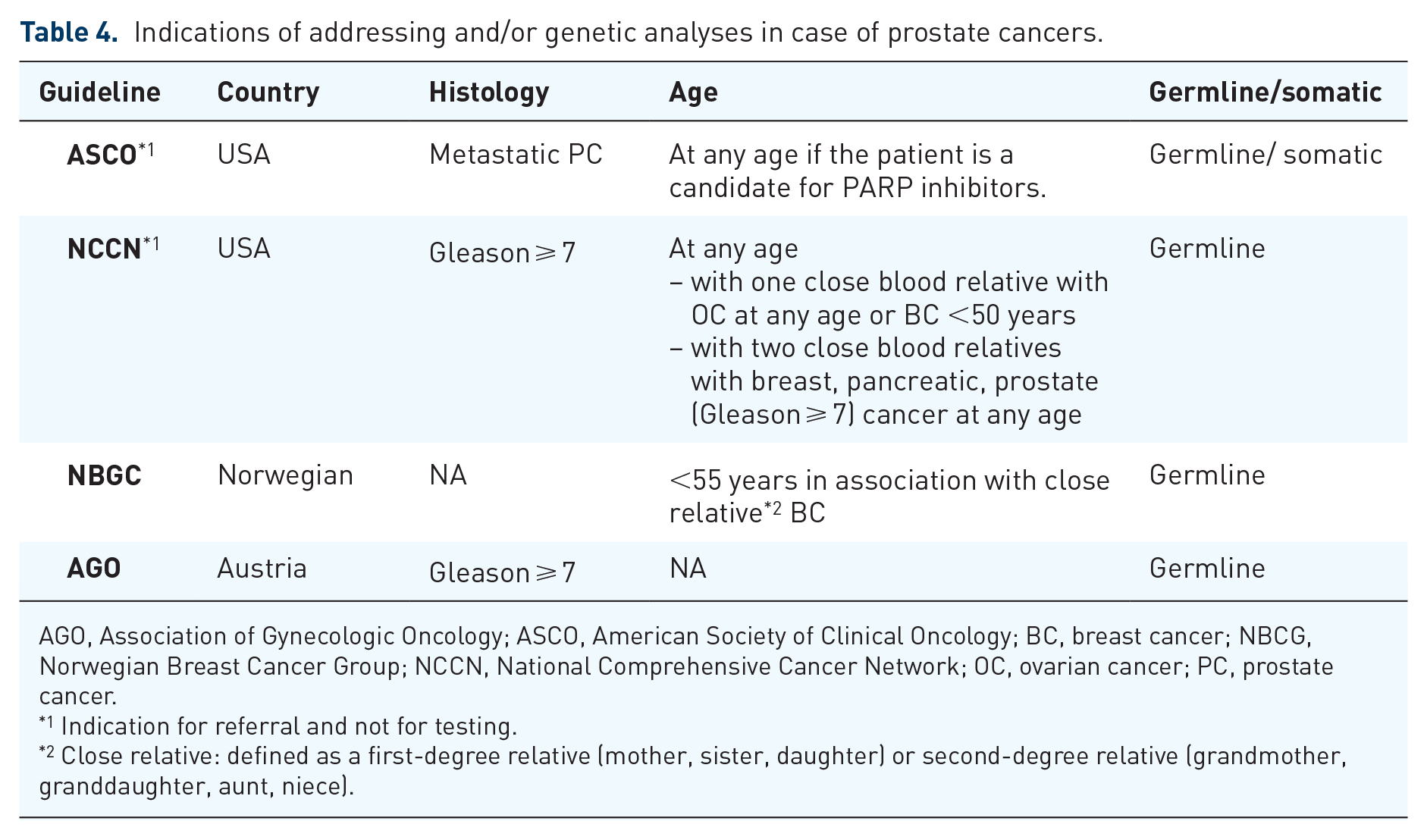
AGO, Association of Gynecologic Oncology; ASCO, American Society of Clinical Oncology; BC, breast cancer; NBCG, Norwegian Breast Cancer Group; NCCN, National Comprehensive Cancer Network; OC, ovarian cancer; PC, prostate cancer.
1 Indication for referral and not for testing.
2 Close relative: defined as a first-degree relative (mother, sister, daughter) or second-degree relative (grandmother, granddaughter, aunt, niece).
PARP inhibitors are showing very encouraging preliminary results in prostate cancer and phase III trials are ongoing.13,34 As in breast cancer, tumor tests have not been included in the current guidelines for genetic testing. Based on this efficacy data, the FDA has approved olaparib monotherapy for patients with metastatic castration-resistant prostate cancer (mCRPC) with germline or somatic BRCA1/2 or ATM mutations, after prior taxane-based chemotherapy and at least one newer hormonal agent (abiraterone or enzalutamide). More recently, the FDA gave a Breakthrough Therapy Designation to rucaparib for single-agent use in BRCA1/2-positive mCRPC following at least one androgen receptor-directed therapy and taxane-based chemotherapy. With these new indications, a large group of patients should be offered genetic counseling to explore whether they could be candidates for PARP inhibitors despite a very low risk of familial predisposition. In practice, it seems difficult to ensure easy access with reasonable delays to oncogenetic counseling, so new strategies are needed to meet the growing demand for genetic testing.
Discussion and proposals
With PARP inhibitors approved in ovarian, breast and prostate cancers, the classical care route consisting of an initial germline genetic test after genetic counseling is no longer efficient. New care pathways need to be developed with early tumor testing, based on predisposing risk factors, and a new approach to genetic counseling notably for patients without a family history of cancer. For patients with a family history, an initial genetic consultation before any germline testing remains mandatory.
In ovarian cancer, oncogenetic counseling is still recommended at diagnosis, whatever the patient’s age. Some oncology teams have specific care pathways for these patients with rapid-access genetic testing and pre-counseling telephone interviews, in order to have genetic test results at the time of recurrence. The limited number of patients and the high risk of family predisposition (around 15–25%) have made it possible to continue to refer patients for rapid-access genetic testing and an oncogenetic consultation if they require treatment promptly. 35 However, care pathways are evolving quickly. With the recent results of the SOLO1 study, underlining the potential benefit of maintenance olaparib after first-line platinum chemotherapy in BRCA1/2 -mutated patients, early testing before initiating chemotherapy will become essential. 10 These test results will influence treatment decisions, such as adding bevacizumab or olaparib to platinum chemotherapy. Thus, tumor testing should be prescribed by oncologists at diagnosis in order to prescribe olaparib in case of a BRCA1/2 mutation. They could provide the initial counseling about familial risks with the help of genetic counselors. Patients with a somatic mutation could benefit from a genetic consultation with an oncogeneticist or genetic counselor secondarily. For patients without a family history of cancer and with a negative tumor test, this could avoid an unnecessary oncogenetic consultation, provided that information about familial risks is given clearly by oncologists. This type of organization would be more efficient and time-saving. It will be developed in the GREAT project. This study will evaluate a new care pathway with initial tumor BRCA1/2 testing for patients with epithelial ovarian cancer, followed by an oncogenetic consultation in the event of a positive somatic result and/or family history. On this basis, a decision tree is proposed in Figure 2, for genetic testing in ovarian cancer.
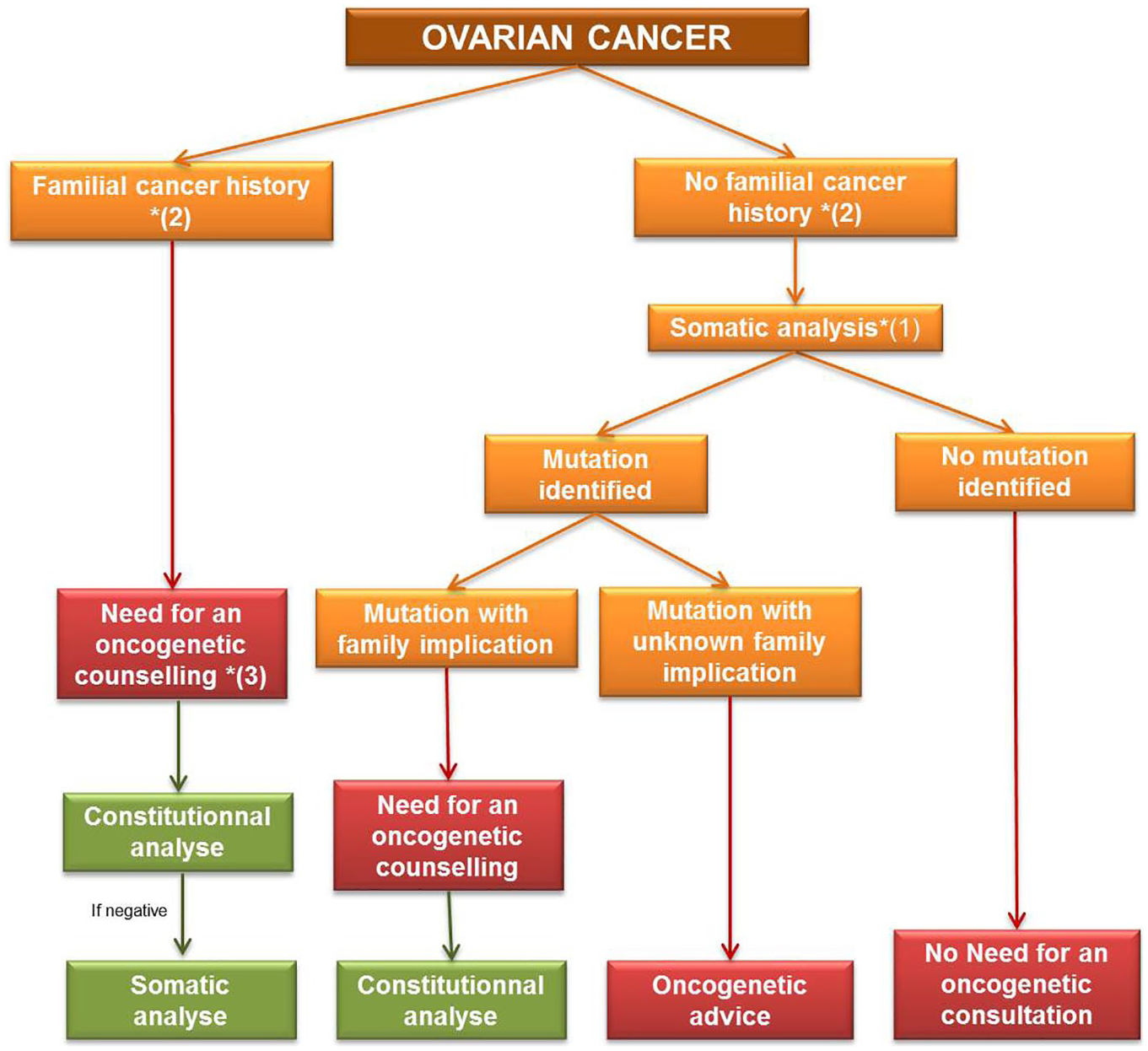
Proposal of care pathway for patients with ovarian cancers at initial diagnosis.
Breast and prostate cancer affect a larger number of patients, so PARP inhibitor indications in these types of tumors will concern more patients. These patients also present a lower risk of family predisposition than ovarian cancer patients. In fact, the risk of presenting a family predisposition is approximately 1–2% in prostate cancer and 5–7% in breast cancer.11,13 On the other hand, only 3% of breast cancer patients present only a somatic mutation of BRCA1/2.11,36 In addition, a significant number of patients have an uninformative family history: in a Swedish study, for example, 62% of patients who were mutation carriers were not identified by selective clinical screening. However, to access PARP inhibitors, genetic testing must be performed in these patients. New strategies are thus needed to meet the demand. As in ovarian cancer, different care pathways can be proposed for these pathologies. In the absence of a family history of cancer or specific age and/or tumor characteristics, tumor genetic testing at diagnosis could become the norm. This could help identify patients who require an oncogenetic consultation and may benefit from this innovative treatment. These proposals are illustrated in Figures 3 and 4.
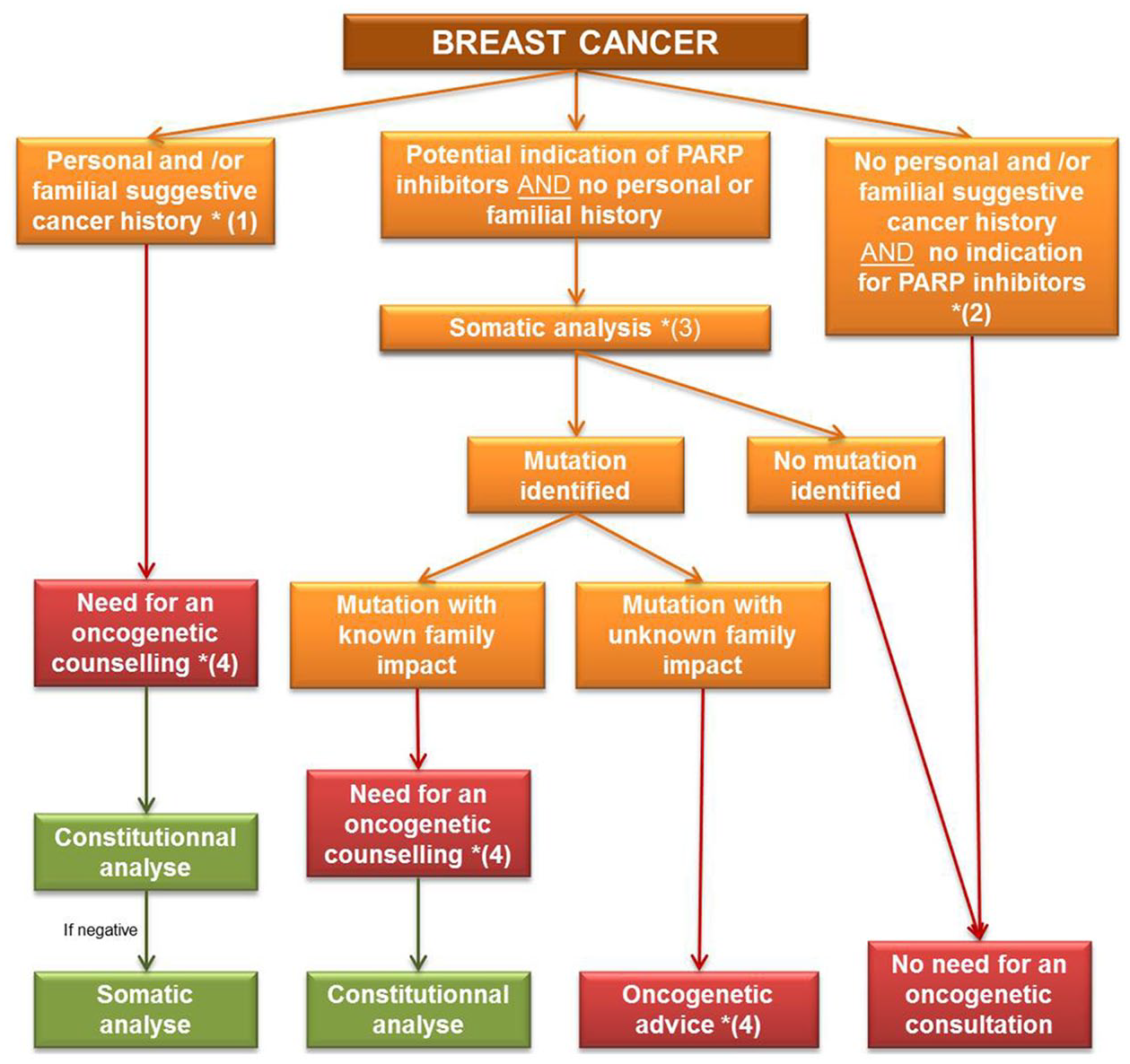
Proposal of care pathway for patients with breast cancers.

Proposal of care pathway for patients with prostatic cancers.
Although the indications for referral are being optimized, the number of oncogenetic consultations is likely to increase and some teams have already proposed training programs in which health professionals (oncologists, nurses, etc.) discuss how the indications for genetic testing and the turnaround time for consultations can be improved.15,37–39 As reported by George and colleagues, new genetic testing pathways have been proposed. 15 In this study, genetic counseling is performed by a trained oncologist prior to germline testing. This organization has shortened waiting times for results and reduced the required resources, with good feedback from patients and medical teams. Likewise, ENGAGE (Evaluating a Streamlined Onco-genetic BRCA Testing and Counselling Model among Patients with Ovarian Cancer) was an international, multicenter, prospective, observational study designed to evaluate the feasibility of a streamlined oncologist-led BRCAm testing model in patients diagnosed with epithelial ovarian, fallopian tube, or primary peritoneal cancer. After training, medical and paramedical partners improved the quality of the first session of genetic counseling. Thereafter, Colombo and colleagues showed that an oncologist-led germline BRCAm testing process is feasible in ovarian cancer. 38 It shortened turnaround times to 9.1 weeks, with high acceptance and satisfaction among both patients and clinical staff (oncologists, nurses, etc.). However, only half of the oncogeneticists were satisfied with the information given to the patients. Percival and colleagues reported, in another study, that the first genetic information could be given by a nurse. 39
Another emerging approach is telephone interviews or telemedicine before face-to-face genetic counseling and testing.37,40,41 Patients can be better selected for oncogenetic consultations and the initial information can be given to patients by trained caregivers during telephone interviews or face-to-face consultations. In a French study, a first telephone interview was conducted by genetic counselors and/or physicians to identify the familial risk requiring a complete genetic work-up. 37 The study showed that pre-counseling telephone interviews were cost-effective as they did not lead to consultations in 39% of cases due to the absence of a significant medical history or by designating a more appropriate index case. In a Swedish study, telephone interviews were conducted by a well-trained nurse and a physician to replace the initial part of face-to-face counseling sessions. 40 Participants reported a high satisfaction rate regardless of whether counseling was conducted by telephone or in person.
A US team offered telephone counseling instead of usual care to healthy women with a risk of a BRCA1/2 mutation above 10%. 41 Board-certified genetic counselors delivered standard BRCA1/2 genetic counseling and disclosed the results in person or by telephone. Telephone counseling cost less than in-person genetic counseling, shortened delays and did not have any detrimental psychological impact. The testing rate was lower with telephone counseling than with face-to-face consultations. Other studies are needed to determine the level of satisfaction of geneticists, long-term adherence to risk management guidelines and effective strategies. However, this approach may be complicated to apply to cancer patients. Replacing face-to-face consultations is difficult, but telephone interviews could improve patient selection and best index case identification. Further studies are needed with telemedicine, which makes an impersonal consultation more humane.
To save time and help oncogeneticists, genetic counselors can take on some of the physicians’ tasks and deliver genetic counseling.
Even if new care pathways need to be developed in this theranostic era, somatic testing still has limitations. Tumor samples have to be available and in sufficient quantity. There are other specific problems such as tumor heterogeneity and the characterization of driver or passenger mutations. There are also technical limitations, as with Formalin-Fixed Paraffin-Embedded (FFPE) samples, which can present altered DNA, or chemical pre-treatments which increase genomic instability. These limitations reinforce the need for a genetic consultation.
In this context, oncogenetic consultations are a key aspect of the healthcare system and are required for patients with germline and somatic mutations and/or a family history and/or unavailability for tumor testing. During these consultations, potential risks and benefits of genetic testing, the probability of finding a mutation, and the implications for the individual and the family are detailed. They also make it possible to explain variants of uncertain significance or a negative result. This requires time for genetic testing, expertise and follow up. Oncogenetic consultations allow results to be delivered within the family and to organize preventive family care. The disclosure of a deleterious mutation is a sensitive moment and requires medical and psychological follow up for patients and their families. These new proposed care pathways need to be evaluated in terms of efficiency and satisfaction of medical staff, patients and their families.
In conclusion, the advent of new cancer therapies such as PARP inhibitors is increasing the demand for genetic counseling. The emergence of this personalized medicine is leading to the systematic molecular characterization of advanced tumors for therapeutic purposes. Genetic testing and counseling pathways need to adapt to this theranostic purpose.
Footnotes
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Conflict of interest statement
Prof Joly’s COI are: TESARO GSK Roche Clovis and Astra Zeneca.