
Abstract
Background:
Preclinical evidence suggests that zoledronic acid (ZOL) works synergistically with chemotherapy by enhancing anti-tumor activity. ZOL blocks the mevalonate pathway and may indirectly interact with human epidermal growth factor receptor 2 (HER2) pathway activation. The clinical efficacy and biological rationale of chemotherapy plus anti-HER2 therapy and ZOL as a part of neoadjuvant therapy has not been previously tested.
Patients and methods:
We conducted a phase II clinical trial to evaluate the efficacy and safety of ZOL as part of a neoadjuvant treatment in patients with HER2-positive breast cancer (BC). The protocol consisted of four cycles of doxorubicin/cyclophosphamide with ZOL, followed by four cycles of docetaxel with trastuzumab and ZOL prior to surgery. The primary endpoint was the pathologic complete response (pCR) rate. Secondary endpoints were safety and the identification of clinicopathological characteristics associated with pCR.
Results:
A total of 71 patients with stage IIA to IIIB BC were included, with 60 eligible for the safety assessment and 58 for the efficacy analysis. Overall, the pCR rate was 42%, with higher rates in hormone receptor (HR)-positive tumors (40%), which contrasts with the results of pivotal trials. The most commonly observed grade 3 and 4 events were febrile neutropenia (grade 3, 20%; grade 4, 3%) and diarrhea (grade 3, 12%).
Conclusions:
The addition of ZOL as a repositioning drug in neoadjuvant treatment was an effective and well-tolerated therapy. This drug combination might overcome endocrine and anti-HER2 resistance. The higher pCR rates in the HR-positive subgroup deserve further translational investigation.
Keywords
Introduction
Neoadjuvant therapy is indicated for human epidermal growth factor receptor 2 (HER2)-positive breast cancer (BC) and is an option even for early tumors. Trastuzumab plus neoadjuvant chemotherapy increases the pathologic complete response (pCR) rate compared with chemotherapy alone in women with HER2-positive BC 1 and is correlated with longer survival. 2
New therapeutic strategies have been developed to broaden the benefit of trastuzumab while maintaining the focus on blocking the HER2 pathway, including the addition of pertuzumab with chemotherapy 3 and the use of neratinib following standard adjuvant treatment with trastuzumab. 4
The activated HER2 protein initiates several phosphorylation events, which leads to crosstalk of signaling pathways and constitutively stimulates tumor growth, invasiveness and cell survival. 5 These key pathways include the mitogen-activated RAS-RAF-protein kinase (MAPK), extracellular signal-regulated kinase (MEK)/ERK and the phosphatidylinositol 3-kinase (PI3K)/PTEN-AKT pathways. 6 For oncogenic activity, RAS proteins depend on interprotein interactions and post-translational processing by isoprenoid precursors produced in the mevalonate pathway that enable attachment to cellular membranes. 6
Bisphosphonates inhibit mevalonate metabolism and thus also inhibit prenylation of the RAS superfamily of GTPases, 7 which provides a molecular rational for a potential synergistic action with the HER2 pathway. Zoledronic acid (ZOL), a third-generation bisphosphonate, has been evaluated in adjuvant studies with variable results.8,9 Notably, survival improvement in BC was only demonstrated in the Early Breast Cancer Trialists’ Collaborative Group meta-analysis 10 for postmenopausal women with HR-positive/HER2-negative tumors. These trials largely excluded women with HER2-positive BC, so there is no information on this subgroup.8–10
In preclinical studies using HER2-negative cell lines, ZOL demonstrated inhibition of tumor cell proliferation, induction of apoptosis, inhibition of angiogenesis, reduction of tumor cell invasion and migration, activation of specific cellular anti-tumor immune responses and a synergistic/additive anti-tumor effect with anthracycline and paclitaxel. 11
However, the effectiveness of ZOL combined with chemotherapy and anti-HER2 therapy has not yet been analyzed. Thus, in our study we evaluated the effect of ZOL added to a neoadjuvant regime of doxorubicin/cyclophosphamide followed by docetaxel/trastuzumab in women with HER2-positive BC. The outcome was measured using the pCR rate as the primary endpoint. Secondarily, we evaluated safety and clinicopathological characteristics in order to identify predictive factors of pCR.
Patients and methods
Recruitment criteria
This was a neoadjuvant, prospective, single-center, open-label, phase II clinical trial conducted in patients with HER2-positive BC. This study was undertaken in accordance with the Declaration of Helsinki, following the guidelines and approval of the local Ethics Committee, the National Ethics Commission for Research Ethics and the National Health Surveillance Agency. All participants signed informed consent forms.
The inclusion criteria were age 18 years or older, HER2-positive, stage IIA to IIIB, and Eastern Cooperative Oncology Group performance status ⩽2. Patients were required to have adequate organ function, left ventricular ejection fraction (LVEF) >50%, a negative serum test for pregnancy and the ability to understand and adhere to treatment. Exclusion criteria were previous history of malignant neoplasm, active infection, peripheral neuropathy grade ⩾2, uncompensated comorbidity, bilateral BC or lactation. Distant metastases were excluded by thoraco-abdomin-pelvic tomography and bone scintigraphy. Cardiac function was monitored at baseline, after anthracycline, after taxane and every 3 months during adjuvant trastuzumab therapy. Fertile women were required to use nonhormonal contraceptives.
Procedure to assess efficacy
Clinical variables collected from patients included race, age, menopausal status, family history of cancer, clinical stage at diagnosis and histopathological and immunohistochemical tumor characteristics.
Core biopsies from the tumor and nontumoral areas were performed by guided ultrasonography. The decision between breast-conserving surgery and mastectomy or sentinel lymph node biopsy and axillary lymph node dissection was decided according to institutional guidelines. For both tissue samples, one part was paraffin-embedded for histological and immunohistochemistry (IHC) analysis, and the rest was frozen and stored at −80°C.
Histopathology and IHC analyses were performed pre (core biopsy) and post-chemotherapy (surgical part material) by two experienced and blinded BC pathologists from our institution. Definition of pCR was absence of infiltrating carcinoma in the breast and axilla.
For patients who did not obtain pCR, the residual breast cancer burden (RCB) was calculated and classified through the MD Anderson calculator (www3.mdanderson.org/app/medcalc/index.cfm?pagename=jsconvert3) according to the following scale: RCB 0 (pCR), I (minimal residual disease), II (moderate residual disease) and III (extensive residual disease). The optimal pathological response was considered to be RCB 0 and RCB I.
Histopathology evaluation was performed on hematoxylin and eosin stained slides to determine the histological classification, 12 histological tumor grade, 13 lymphovascular invasion (LVI), 13 necrosis, 13 and stromal lymphocytic infiltration (sTIL). 14
The results from LVI, sTIL and necrosis analyses were classified as present or absent.
For immunohistochemistry analysis, staining was performed on 3-μm-thick tissue sections prepared on polarized slides. Positive controls for each antibody were utilized according to the manufacturer’s instructions. Sections were incubated with estrogen receptor (ER), progesterone receptor (PgR), Ki-67 labeling index, p53, HER2, E-cadherin (E-CAD) or beta catenin (B-CAT) antibodies overnight at dilutions of 1:1600 ER (clone 1D5), 1:1600 PR (clone PR-636), 1:600 KI67 (clone MIB-1) and 1:200 P53 (clone DO-7) supplied by the DAKO Corporation® (Santa Clara, CA, USA). The 1:500 anti-HER2 (clone SP2) was supplied by Cell Marque™ (Rocklin, CA, USA). The 1:1200 E-CAD (clone SPM471) and 1:100 B-CAT (clone E-5) were supplied by Santa Cruz Biotechnology (Hortolândia, SP, Brazil). The staining was visualized using an optical microscope.
The cut-off value for ER and PgR positivity was 1% positive tumor cells with nuclear staining. 15 Ki-67 expression was considered high when ⩾20% of cells were stained. 16 HER2 status was defined according to the American Society of Clinical Oncology (ASCO) and the College of American Pathologists (CAP) guidelines from 2007 and 2013. 17
A positive nuclear staining visual score of 10% or greater for invasive cancer cells was considered p53-positive. 18
Immunopositivity to E-CAD was determined by comparing the labeling of tumor cells with adjacent normal epithelial cells. Strong tumor cell staining consistent with adjacent normal epithelial cells was considered positive, while negative epithelial cells had weak or no staining. 19
The staining intensity for B-CAT was determined by comparing the labeling of tumor cells with adjacent normal epithelial cells and classified as strong expression (>90%), moderate expression (⩾10% ⩽90%) or weak expression (<10%). 20
Therapeutic procedures
Patients received four 3-week cycles of 60 mg/m2 doxorubicin and 600 mg/m2 cyclophosphamide (AC) followed by four 3-week cycles of 100 mg/m2 docetaxel (DOC) with 6 mg/kg trastuzumab every 3 weeks (8 mg/kg as a loading dose). Overall, eight cycles of 4 mg/dose ZOL were given, the first cycle concomitant with AC and subsequent cycles 1 week after each chemotherapy’s cycle (AC × 4 + ZOL × 4 → DOC × 4 + trastuzumab × 4 + ZOL × 4) every 3 weeks, followed by surgery.
Granulocyte-colony stimulating factor was administered in cases of febrile or afebrile grade 3 or 4 neutropenia and then continued for each consecutive cycle. Cycle delays and 25% dose reduction of chemotherapy were permitted when toxicity was greater than grade 2. Patients could be discontinued from chemotherapy due to chemotoxicity and continue treatment with trastuzumab and ZOL or referred for surgery.
After surgery, radiotherapy was delivered according to institutional guidelines, and trastuzumab was continued as a single agent for 1 year or combined with adjuvant endocrine therapy when indicated.
Study endpoints
The primary endpoint was the pCR rate. Secondary endpoints evaluated safety, and an exploratory analysis was conducted to examine the correlation between clinicopathological features and pCR. For the safety evaluation, adverse events (AEs) were collected at each visit and graded according to the Common Terminology Criteria for Adverse Events version 4.0. Patients who underwent breast surgery were included in the efficacy analysis and those who received at least one course of chemotherapy were included in the safety analysis.
Statistical analysis
Statistical analyses were performed using SPSS version 18 (SPSS, Chicago, IL, USA). With a significance level of 0.1% and 80% power using a one-stage Fleming method, a total of 56 patients were needed to detect a pCR rate between 0.22 and 0.35. Responses were calculated as percentages of all patients who underwent surgery after neoadjuvant treatment. Baseline patient characteristics and AEs are presented as percentages, medians and ranges. Associations between clinicopathological features and pCR were calculated by Pearson’s Chi-squared test or Fisher’s exact test according to the statistical assumptions.
Results
Patient characteristics
From November 2012 to July 2016, 71 patients with HER2-positive BC stage IIA–IIIB signed the informed consent form (ICF), and 60 were eligible and treated in NCI-Brazil. The two patients who had a complete clinical response refused to undergo surgery at the end of neoadjuvant treatment and were excluded from the efficacy analysis.
Baseline characteristics of the patients are summarized in Table 1. The median age was 54 years with a range of 26–74 years, and the tumors were large with a median size of 61 mm. A total of 38 patients (63%) were postmenopausal. Most patients had stage IIB (37%), tumor grade 2 (52%) and were ER or PgR-positive (73%). A total of 31 patients had a family history of breast/ovarian cancer and 42% were white.
Patients and disease characteristics at baseline.
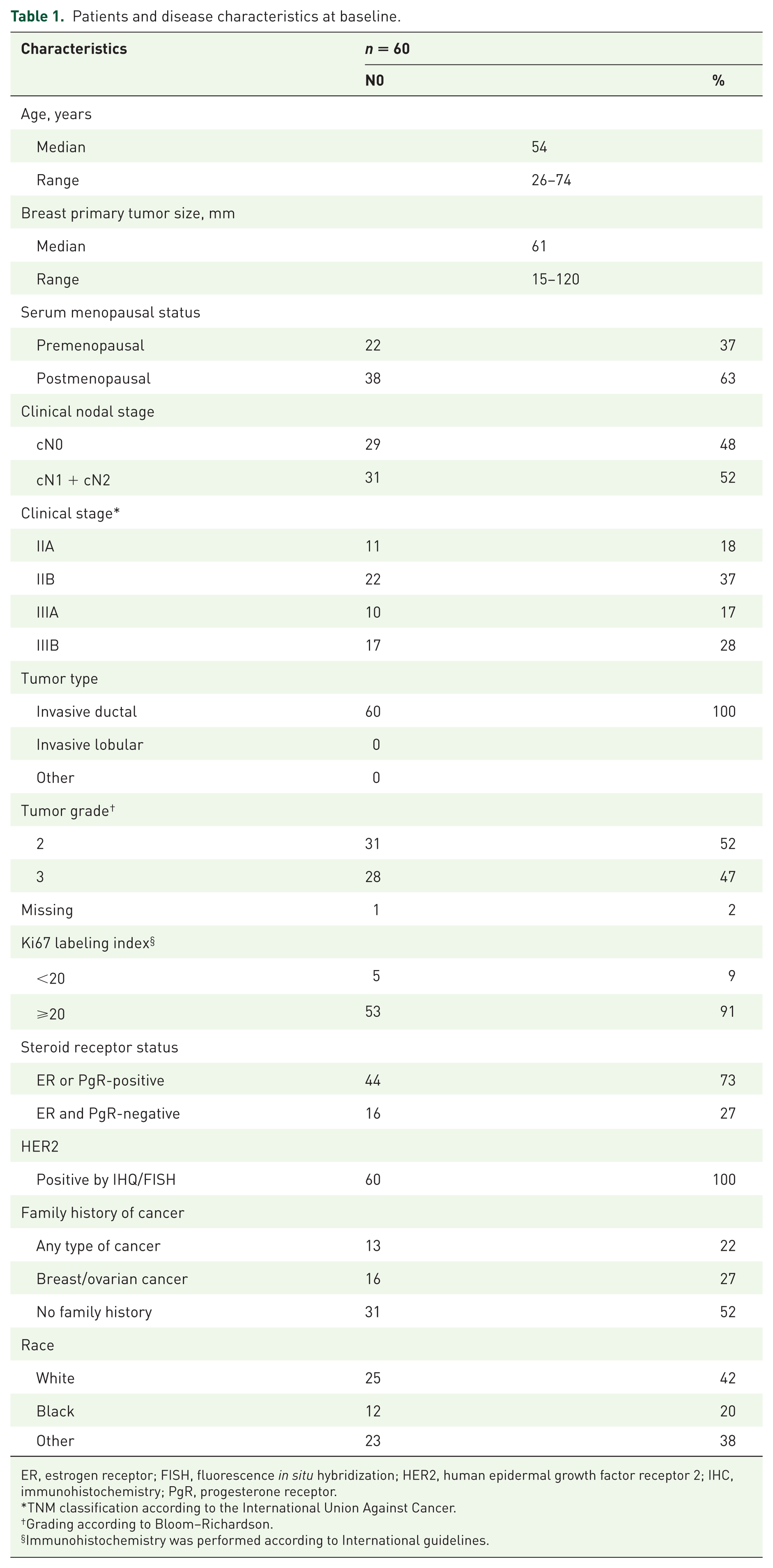
ER, estrogen receptor; FISH, fluorescence in situ hybridization; HER2, human epidermal growth factor receptor 2; IHC, immunohistochemistry; PgR, progesterone receptor.
TNM classification according to the International Union Against Cancer.
Grading according to Bloom–Richardson.
Immunohistochemistry was performed according to International guidelines.
Efficacy data
All the patients who accepted the breast operation, after the treatment, were able to undergo surgery. pCR (RCB 0) was achieved in 24 (42%) and minimal residual disease (RCB I) was achieved in 15%, generating an optimal pathological response (RCB 0 plus RCB I) of 57%. We explored the pCR in different subgroups as shown in Table 2.
Pathological response rate.

IS, in situ; RCB, residual cancer burden.
There was a significantly higher pCR rate in patients with nuclei/cytoplasmic β-catenin expression (p = 0.030). None of the other clinicopathological variables evaluated in the study showed an association with pCR (Table 3). Although numerically higher, pCR in HR-negative = 0.44 [0.31; 0.56] was not statistically significant compared with HR-positive = 0.40 [0.27; 0.52] BC.
Association between pathological response and baseline clinicopathological features.

ER, estrogen receptor; PgR, progesterone receptor; pCR, pathological complete response; RCB, residual cancer burden.
TNM classification according to the International Union Against Cancer, †Grading according to Bloom–Richardson, §Immunohistochemistry was performed according to local practice.
n = 56 because the material was consumed in two patients.
Safety data
For the safety evaluation, 60 patients were included, as shown in Table 4. The most frequent AEs were gastrointestinal grade 1 and 2. A total of 17 (28%) patients had possible ZOL-related AEs; 29% had grade 1 myalgia (3) and fever (2) and 71% had grade 2 myalgia (6), arthralgia (4), and fever (2). No cardiac dysfunction or osteonecrosis of the jaw was reported as a grade 5 adverse event. Overall, 3 patients (5%) had grade 4 events and 39 (65%) had grade 3 events.
Most common adverse events* (reported in ⩾20% of patients).

Evaluated in 60 patients.
Gastrointestinal events included nausea, mucositis, vomiting, diarrhea, constipation, stomach pain and abdominal pain.
Skin and subcutaneous tissue disorders included erythema, pruritus, acne, and nail changes.
Respiratory and thoracic disorders included bronchial asthma, definite dry cough, sore throat and allergic rhinitis.
Infections and inflammations included infections and inflammations of skin or teeth (without jaw osteonecrosis), urinary infection, pneumonia, tonsillitis and upper respiratory infection.
Incidence <20%, but adverse events of special interest.
Discussion
The current trial is the first to our knowledge to evaluate the in vivo benefit of ZOL in a neoadjuvant setting, combined with chemotherapy and HER2-targeted therapy for women with HER2-positive tumors and high tumor burden (median tumor size of 61 mm). This study met its primary endpoint of therapeutic efficacy, with an overall pCR rate of 42% and showed that pCR rates according to HR status were similar between HR-positive and HR-negative subgroups (40% versus 44%).
HER2-positive BC is a heterogeneous disease; some studies even report that almost two-thirds are HR-positive. There is preclinical and clinical evidence to suggest bidirectional crosstalk between the HER2 and ER pathways, which can lead to endocrine and anti-HER2 therapy resistance. 21 This evidence is supported by the significantly lower pCR rate of HR-positive/HER2-positive BC compared with HR-negative/HER2-positive BC demonstrated in the neoadjuvant trials22–26 (Table 5). Although direct comparisons with other trials are not appropriate, the pCR rates in our trial for HR-positive tumors were higher than seen in some studies22–26 (Table 5). These results seem to provide clinical evidence that ZOL might have a role in reverting resistance of anti-HER2 agents in HR-positive/HER2-positive tumors.
Pathological complete response rates (ypT0/ypTis ypN0 or ypT0/ypTis) in neoadjuvant breast cancer trials with anti-HER2 blockade, according to the expression of the hormone receptors breast cancer.

Weekly paclitaxel.
Paclitaxel every 3 weeks.
pCR only in breast (ypT0/ypTis).
pCR in breast and axilla (ypT0/ypTis ypN0).
AC, adriamicin/cyclophosphamide; Carb, carboplatin; Doc, docetaxel; EC, epirubicin/cyclophosphamide; FEC, fluorouracil/epirubicin/cyclophosphamide; L, lapatinib; P, pertuzumab; Pac, paclitaxel; pCR, pathological complete response; T, trastuzumab; ZOL, zoledronic acid.
ZOL inhibits farnesyl pyrophosphate synthase, a crucial enzyme for mevalonate pathway integrity, which promotes a post-translational modification of GTPases, such as RAS, RHO and RAC, which integrate with the HER2 pathway. These molecules are involved in cellular proliferation, cell survival, formation of intracytoplasmic vesicles and plasma membrane rearrangement, 6 thus molecularly supporting the interaction between HER2 blockade therapy and ZOL.
The synergistic effect of chemotherapy and ZOL has been explored in clinical trials. In the AZURE adjuvant study, an exploratory, retrospective analysis among the subgroups of patients who underwent neoadjuvant chemotherapy with or without ZOL showed that patients who received the combination had lower residual disease (median of 15.5 mm and 27.4 mm respectively) and higher pCR rate (17.7% and 6.9%, respectively). 27 In 2016, a meta-analysis of four trials (NEOZOTAC, AZURE, JONIE and Aft and colleagues) 28 was published and revealed the absence of impact in pCR when ZOL was combined with chemotherapy, despite some benefit in postmenopausal patients. There were more than 750 patients included in this meta-analysis, with only 58 (7.7%) being HER2-positive. Therefore, no conclusions were reported in the HER2-positive population. 28
Most studies that have attempted to identify predictive factors of complete pathological response in HER2-positive BC patients are retrospective. 29 In our prospective study, only nuclei/cytoplasmic β-catenin expression was associated with a higher rate of pCR after neoadjuvant treatment with ZOL (Table 3). This finding is different from the findings of Elsamany and colleagues in 2016; their retrospective study found that membrane β-catenin expression was associated with higher rate of pCR. 30 Because our study included only a few tumors harboring nuclei/cytoplasmic β-catenin expression, these data need to be validated in a larger cohort of patients.
β-catenin is a multifunctional protein which has been evaluated as a predictor of pathological response in BC. It was originally identified as a component of cell–cell adhesion machinery. The protein β-catenin is an essential integral structural component of cadherin-based adherens junctions, and the key nuclear effector of canonical Wnt signaling in the nucleus. Imbalance in the structural and signaling properties of β-catenin often results in disease and deregulated growth connected to cancer and metastasis. In HER2-positive BC the RAS/RAF/MEK/MAPK and the PI3K/AKT/mTOR pathway are highly deregulated and Akt represents a central hub in the Wnt/β-catenin and PI3K signaling pathways 31 which in turn plays a role in resistance mediation to anti-HER2 therapies. 32
Safety was an important outcome. The concurrent use of anthracycline and taxane with trastuzumab and ZOL in neoadjuvant therapy is well tolerated, and no grade 3 or higher AEs were found to be related to ZOL.
The findings of this study have to be seen in light of some limitations. It was performed in a single center due to resources limitations. The sample size was calculated based on a pCR rate in literature, however since this was a proof-of-concept study, it was feasible not having a randomized-comparative arm. Additionally, prior research about prospectively neoadjuvant chemotherapy plus ZOL in the HER2-positive population is lacking and we had to develop an entirely new research typology. Finally, results must be relativized to possible underpowered associations between study variables.
Conclusion
The current trial results support a feasible, effective, affordable and well-tolerated alternative for neoadjuvant treatment in HER2-positive BC. ZOL should be encouraged as a possible repositioning drug in clinical trials. The better evaluation of its potential role in overcoming endocrine and anti-HER2 resistance deserves attention.
Footnotes
Acknowledgements
The study was conducted in accordance with the Declaration of Helsinki, following the guidelines of the local Ethics Committee. It was approved by the National Cancer Institute Ethics Committee (CEP-INCA no 154/10, ClinicalTrials.gov identifier: NCT01472146), by the National Health Surveillance Agency (ANVISA) and by National Commission for Ethics Research (CONEP– no 16488). All participants signed informed consent forms.
We would like to thank all patients for the trust in the Zo-NAnTax team and their time invested. Additionally, a special compliment is reserved for Dr Ian Tannock for his guidance and critical review.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.