
Abstract
Background:
Novel prognostic markers and therapeutic targets for advanced cancer are urgently needed. This report with trial sequential analysis (TSA) was first conducted to provide robust estimates of the correlation between aldehyde dehydrogenase 1 (ALDH1) and Nestin and clinical outcomes of advanced cancer patients.
Methods:
Hazard ratios (HRs) with 95% confidence intervals (CIs) were summarized for overall survival (OS), disease-free survival (DFS), progression-free survival (PFS), cancer-specific survival (CSS), relapse/recurrence-free survival (RFS), and metastasis-free survival (MFS) from multivariable analysis. TSA was performed to control for random errors.
Results:
A total of 20 studies with 2050 patients (ALDH1: 15 studies with 1557 patients and Nestin: 5 studies with 493 patients) were identified. ALDH1 (HR = 2.28, p < 0.001) and Nestin (HR = 2.39, p < 0.001) were associated with a worse OS, as confirmed by TSA. Nestin positivity was linked to a poor PFS (HR = 2.08, p < 0.001), but ALDH1 was not linked to DFS, RFS, MFS, or PFS, and TSA showed that more studies were needed. Subgroup analysis by tumor type indicated that ALDH1 positivity may be associated with shorter OS in breast, head and neck cancers, but there was no association with colorectal cancer. Subgroup analysis by study source showed that ALDH1 positivity was correlated with a worse OS for Japanese (HR = 1.94, p = 0.002) and European patients (HR = 4.15, p < 0.001), but there was no association for Chinese patients. Subgroup analysis by survival rate showed that ALDH1 positivity correlated with poor OS at ⩾ 5 years (HR = 2.33, p < 0.001) or 10 years (HR = 1.76, p = 0.038).
Conclusions:
ALDH1 may be more valuable as an effective therapeutic target than Nestin for improving the long-term survival rate of advanced cancer. Additional prospective clinical trials are needed across different cancer types.
Introduction
Cancer is still one of the most threatening diseases in the world, with high morbidity and mortality rates. 1 Although the therapeutic strategies (surgery, chemotherapy, radiotherapy, targeted molecular therapy, and immunotherapy) have greatly improved in recent years, effective therapeutic opportunities are still limited. Therefore, the 5-year survival rate of patients with liver, lung or lymph node metastases (advanced stage) remains disappointing.2–5 The addition of prognostic markers to better prognostic models could improve the outcomes of advanced or metastatic cancer patients and aid in the appropriate selection of treatment strategies as potential novel therapeutic targets.
Cancer stem cells (CSCs), a small subset of cancer cells, are responsible for the capability of self-renewal, uncontrolled proliferation and differentiation, tumor progression, and resistance to traditional therapy.6,7 CSCs have been identified in many tumors, for example, lung, breast, colorectal and cervical cancer.8–10 Nestin, namely, neural stem cell protein, a member of the class VI intermediate filament (IF) family, was first discovered as a neural stem and progenitor cells marker. 11 Subsequent reports suggested that Nestin is observed in nonneural tissues 12 and may play a role in CSC phenotypes. 13 Nestin is involved in tumor angiogenesis, growth and cellular processes such as cell adhesion, proliferation, migration, and invasion.14–16 The aldehyde dehydrogenase 1 (ALDH1) gene has been mapped to chromosome 12q24.2 and is responsible for oxidation and detoxification functions. 17 ALDH1 is involved in cellular differentiation and proliferation and in resistance to alkylating chemotherapeutic agents.18,19 ALDH1 has been identified in some tumors and acts as a promoter, inducing an epithelial-mesenchymal transition (EMT) in tumor cells.20,21 ALDH1 and Nestin are expressed in some malignant tumors.22–25 However, there are some uncertain conclusions for ALDH1 and Nestin in advanced cancer; for example, Dong and colleagues reported that ALDH1-positive expression was not correlated with overall survival (OS) in multivariable analysis in advanced breast cancer. 26 However, ALDH1-positive expression was associated with worse overall survival in multivariable analysis in advanced breast cancer by Alamgeer and colleagues. 27 Thus, further analysis is needed to elucidate the significance of ALDH1 and Nestin in advanced cancer.
To better understand the prognostic mechanisms of ALDH1 and Nestin in advanced or metastatic cancer, we first performed a systematic meta-analysis to evaluate the benefits of ALDH1 and Nestin using multivariable survival analysis. We also conducted trial sequential analysis (TSA) to correct for the increased risk of random errors and to determine if additional studies were needed. Our study’s results could assist in the selection of appropriate treatment strategies, suggest novel therapeutic targets for advanced cancer patients, and help stratify patients in future prospective clinical trials.
Materials and methods
Search strategy
This meta-analysis was performed based on the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement. 28 We systematically searched the PubMed, EMBASE, EBSCO, Web of Science, and Cochrane Library databases for relevant studies published prior to April 2018. The search strategy was on the basis of the following key words and search terms: ‘aldehyde dehydrogenase 1 OR ALDH1 OR Nestin’, ‘metastatic OR advanced OR metastasized OR recurrent’, ‘cancer OR tumor OR carcinoma OR neoplasm’, ‘survival OR outcome OR prognosis’ (Table S1). The reference lists of all eligible articles were also manually reviewed to identify additional studies. Overall, three authors (SH, TH, and FH) independently assessed the publications, and discrepancies were resolved by consensus.
Eligibility criteria
Articles that met the following inclusion criteria were selected: (1) patients were diagnosed with advanced, metastatic, or recurrent cancer; (2) prospective or retrospective clinical studies that reported sufficient information for the prognostic estimation of ALDH1 and Nestin positivity; (3) studies reported available data regarding hazard ratio (HR) and 95% confidence interval (CI) using multivariable survival analysis for prognostic indicators of OS, disease-free survival (DFS), progression-free survival (PFS), cancer-specific survival (CSS), relapse/recurrence-free survival (RFS), or metastasis-free survival (MFS); (4) if studies did not record sufficient data on HR with 95% CI, HR and 95% CI values were calculated on the basis of the described method if possible,29,30 or we emailed the corresponding author to request useful information; (5) the eligible studies were limited to the English language. If the authors published multiple papers using overlapping sample data, only the study with the latest information or the largest number of patients was extracted to avoid repeated data. Studies that did not meet the above-described inclusion criteria were excluded.
Data extraction and study assessment
Methodological assessment was performed based on the Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK) guidelines. 31 REMARK criteria include 20 items (introduction: 1 item, materials and methods: 10 items, results: 7 items, and discussion: 2 items), having a maximum possible score of 40. An item had the following possible values: 2 if the item was clearly described, 1 if the item was incompletely described, and 0 if the item was not applicable or not fully defined. Additionally, multivariable survival analysis adjusted factors was considered more valuable than a study using univariable survival analysis. Thus, the meta-analysis only included the prognostic data from multivariable analyses. The REMARK scores are listed in Table S2. The following data were extracted from the eligible full-text papers: the surname of the first author, publication year, number of patients, demographic data (median or mean age), study source, median or mean follow-up time, cancer type, study design, testing method, therapy regimes, sample type, cut-off value, survival rate, adjusted variables, and clinical outcomes of multivariable analysis. Any disagreements were resolved by discussion until consensus was achieved.
Statistical analysis
Data with an HR >1 indicated worse survival, whereas an HR <1 indicated favorable survival. Pooled HR and 95% CI were calculated to evaluate the prognostic effect of ALDH1 and Nestin positivity using multivariable analysis for advanced cancer (OS, DFS, PFS, CSS, RFS, or MFS). Heterogeneity among the eligible studies was measured using the Cochran’s Q statistic and I2 test. 32 According to the der Simonian–Laird method, the random-effects model was applied in the meta-analysis.33,34 Both I2 < 50% and p > 0.1 were considered as signifying low-level heterogeneity. For the results (> seven studies) with obvious heterogeneity, subgroup analyses by cancer type, study source, survival rate, age (years), detection method, and study center design, etc. were conducted to explain the possible sources of heterogeneity and the strength of the correlation among different subgroups. Sensitivity analyses were also performed to estimate the effect of each individual study on the HR value by removing one study from the analysis at a time. Publication bias was detected using Egger’s and Begg’s funnel plots.35,36 If the meta-analysis included a small sample size, random errors may cause spurious findings.37,38 TSA was performed to evaluate the required sample information. 39 Alpha (type I error) and beta (type II error) levels of significance of 5% and 20% were used, respectively, and the optimal a priori anticipated information size (APIS) method was set. Monitoring boundaries were constructed to decide whether a study could be terminated early. When the cumulative Z-curve crossed the trial sequential monitoring boundary or required information size boundary, the evidence was considered to be conclusive, and further studies were deemed unlikely to change the results; otherwise, additional clinical studies were necessary. Meta-analysis was performed with Stata software, version 12.0 (Stata Corp., College Station, TX, USA) and R software, version 3.4.2 (The R Foundation for Statistical Computing, Vienna, Austria).
Results
Study characteristics
A flow diagram of the literature search procedure is presented in Figure 1. After applying the eligibility criteria, a total of 20 studies published from 2010 to 2018 were included in the meta-analysis,26,27,40–56 including 2050 patients with advanced cancer. These studies were evaluated against the REMARK criteria, with a mean REMARK score of 20. A total of nine studies were conducted in Europe, two in the USA, four in China, four in Japan, and the remaining one in Korea. Among the included studies, 15 studies involving 1557 advanced cancer patients evaluated the association between ALDH1 positivity and the prognosis using multivariable analysis for CSS, OS, DFS, RFS, MFS, and PFS.26,27,41,43,45–52,54,56 Overall, five studies involving 493 advanced cancer patients assessed the correlation between Nestin positivity and the prognosis using multivariable analysis for OS and PFS.40,42,44,53,55 The characteristics of the included studies are listed in Table 1 and Table S3.

PRISMA diagram/flow chart.
Main characteristics of the eligible studies.

Note: the studies from Charafe-Jauffret 2010 to Ning 2018 were of ALDH1 and the studies from Fusi 2011 to Onisim 2016 were of Nestin.
stands for the mixed population.
CSS, cancer-specific survival; DFS, disease-free survival; FC, flow cytometry; IHC, immunohistochemistry; MFS, metastasis-free survival; N, number of cases; NA, not applicable; OS, overall survival; PFS, progression-free survival; qRT-PCR, real-time quantitative PCR; RFS, relapse/recurrence-free survival.
Association between ALDH1 positivity and the prognosis
CSS was only available in one study with 77 cases that showed that ALDH1 positivity was correlated with a poor CSS (5-year CSS: HR = 2.7, 95% CI = 1.48–4.93; Figure 2). There was no statistically significant correlation with DFS (n = four studies with 333 cases, HR = 0.95, 95% CI = 0.38–2.36, p = 0.907), RFS (n = three studies with 344 cases, HR = 0.90, 95% CI = 0.41–1.99, p = 0.797), MFS (n = two studies with 112 cases, HR = 1.04, 95% CI = 0.16–6.70, p = 0.97), or PFS (n = two studies with 168 cases, HR = 1.32, 95% CI = 0.65–2.68, p = 0.445; Figure 2). Data from 10 studies indicated that ALDH1 positivity was significantly correlated with a negative effect on OS with an HR of 2.28 (95% CI: 1.59–3.27, p < 0.001, n = 1070 cases; Figure 3). Additionally, three studies did not report information about the use of adjuvant therapy, so we recalculated the OS results of the remaining seven studies using adjuvant therapy and found that ALDH1 positivity was still correlated with a worse OS (HR = 1.84, 95% CI = 1.29–2.62, p = 0.001; Figure 3).
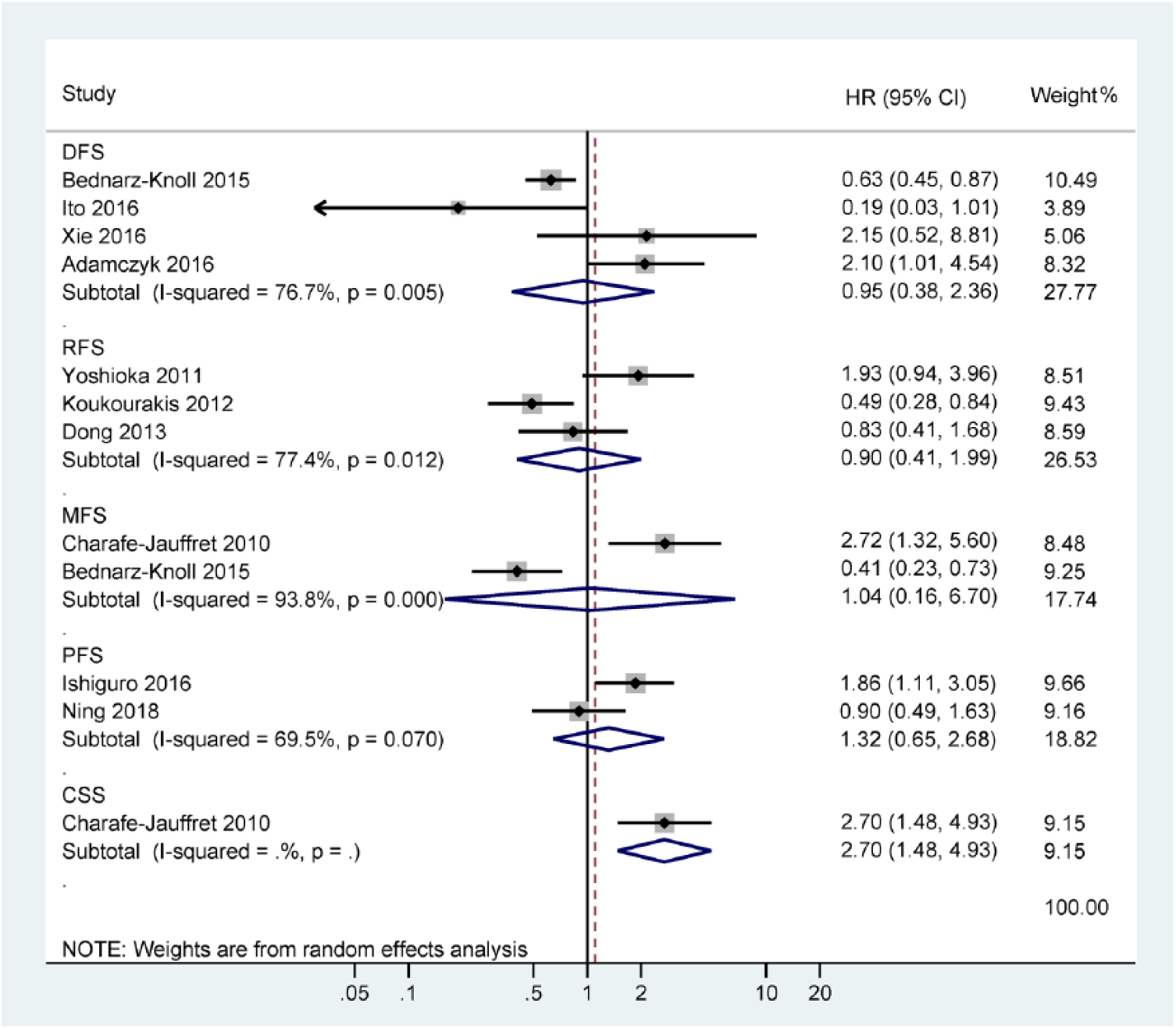
Forest plot of the association between ALDH1 positivity and DFS, RFS, MFS, PFS, and CSS.

Forest plot of the association between ALDH1 positivity and OS.
Subgroup and sensitivity analyses of ALDH1 positivity in OS
The results of subgroup analyses by the possible sources of heterogeneity for the OS results are listed in Table 2. Most subgroups were not significantly changed by the study factors for heterogeneity. The testing method and treatment regimens could reduce the level of statistical heterogeneity (testing method: blind, I2 = 72.2% and p = 0.013; NA, I2 = 30.3% and p = 0.208; treatment regimens: surgery with adjuvant therapy, I2 = 32.9% and p = 0.202; others, I2 = 68.0% and p = 0.014). In addition, the strength of the association among different subgroups was evaluated and there was a significant association for patients with head and neck carcinoma (n = 122 case, HR = 3.99, p < 0.001), cervical cancer (n = 52 case, HR = 3.51, p = 0.034), and ovarian carcinoma (n = 90 case, HR = 2.51, p = 0.003). Data from four studies with 707 cases showed a trend towards poor OS in breast cancer patients (HR = 1.67, 95% CI = 0.97–2.87, p = 0.062), but no association was found for colorectal cancer (two studies with 99 cases: HR = 2.30, 95% CI = 0.79–6.70, p = 0.129). Subgroup analysis by study source showed that ALDH1 positivity was linked to a shorter OS in Japanese (three studies with 517 cases: HR = 1.94, 95% CI = 1.28–2.92, p = 0.002) and Europeans (four studies with 262 cases: HR = 4.15, 95% CI = 2.46–7.03, p < 0.001), but not in Chinese (two studies with 213 cases: HR = 1.61, 95% CI = 0.40–6.53, p = 0.506). Stratified analysis based on survival rate indicated that ALDH1 positivity was correlated with a poor prognosis in terms of ⩾5-year OS (eight studies with 971 cases: HR = 2.33, 95% CI = 1.54–3.53, p < 0.001), and further pooled HR from two studies with 427 cases resulted in a decreased OS at 10 years (HR = 1.76, 95% CI = 1.03–3.00, p = 0.038),43,54 but no association at <5-year OS (two studies with 99 cases: HR = 2.30, 95% CI = 0.79–6.70, p = 0.129). Significant associations were noted between other subgroup analyses (testing method, study center design, and treatment regimens).
Summary of ALDH1 by subgroup analyses in OS.

ALDH1, aldehyde dehydrogenase 1; CI, confidence interval; HR, hazard ratio; NA, not applicable; OS, overall survival; TSA, trial sequential analysis.
Sensitivity analysis was conducted based on the omission of one study at a time, and when the studies of Dong and colleagues 26 or Miyoshi and colleagues 43 were removed, heterogeneity was lacking (I2 = 0.0% and p = 0.442), but the HR was not significantly changed (HR = 2.75, 95% CI = 2.03–3.73, p < 0.001).
Association between Nestin positivity and the prognosis
Data from four studies with 460 cases demonstrated that Nestin-positive expression was associated with significantly poorer OS (HR = 2.39, 95% CI = 1.86–3.05, p < 0.001, I2 = 0.0%; Figure 4) and Nestin-positive expression was also significantly linked to a worse PFS (three studies with 338 cases: HR = 2.08, 95% CI = 1.58–2.73, p < 0.001, I2 = 0.0%; Figure 4).

Forest plot for the association between Nestin positivity and OS and PFS.
Publication bias
The funnel plots showed that a slight publication bias existed regarding OS and ALDH1 (Egger’s test: p = 0.037 < 0.05), but no publication bias existed regarding OS (Begg’s test: p = 0.074; Figure S1).
TSA
The relative risk reduction of 20%, type I error α (5%), and type II error β (20%; power of 80%) were used. The TSA showed that the cumulative Z-curve crossed the trial sequential monitoring boundary regarding OS of ALDH1 and Nestin positivity (Figures S2 and 3) and the subgroup of ALDH1 at ⩾5-year OS (Table 2), suggesting that further studies are unlikely to change these results. However, for most subgroups of ALDH1 (Table 2), the results of Nestin positivity for PFS (Figure S4), and the results of ALDH1 for DFS, RFS, MFS, or PFS (Table S4), showed that the cumulative Z-curve did not cross the trial sequential monitoring boundary, suggesting that additional studies are needed. For the above results from the sensitivity analysis, further TSA still showed that the cumulative Z-curve was more than the trial sequential monitoring boundary (Figure S5), further suggesting that additional studies are not needed.
Discussion
Epithelial tumors are generally heterogeneous cell populations with highly variable abilities of survival, growth, and metastasis. 57 Emerging evidence suggests that the top of the cellular hierarchy is a CSC population that can self-renew, proliferate and differentiate into progeny cells, thus causing the cellular and functional heterogeneity within epithelial tumors.58,59 CSCs have been reported in many tumors, such as breast, lung, melanoma, and colorectal cancers. 60 Wu and colleagues reported that Nestin-positive expression was correlated with worse survival in glioma. 24 Shan and colleagues found that weak Nestin expression was associated with favorable survival in ampullary adenocarcinoma. 61 Some studies reported that ALDH1-positive expression was linked to decreased survival outcomes in lung, bladder, and breast cancers,62–64 while other studies reported that loss of ALDH1 was correlated with shortened survival in pancreatic and lung cancers.65,66 However, the prognostic effect of ALDH1 and Nestin in patients with advanced or metastatic cancer remains unclear and the present meta-analysis was conducted to better clarify the characteristics of CSCs expressing ALDH1 and Nestin. This information added to the current prognostic models could guide the development of new therapeutic strategies for advanced or metastatic cancer by identifying them as effective therapeutic and prognostic targets in clinical practice.
Conventional chemotherapy and radiation therapy are two common useful strategies to eliminate cancer cells and shrink tumors. However, chemotherapy/radiotherapy resistance and disease recurrence are major challenges for the long-term survival of cancer patients.67–69 Thus, understanding the mechanisms of chemoresistance and radioresistance are important for improving chemotherapy and radiation therapy. The reasons for cancer drug resistance are very complex and affected by many factors, which also affect therapy efficacy.70–72 Importantly, recent studies have suggested that CSCs are resistant to traditional chemotherapy and radiotherapy.73,74 Some mechanisms, such as important signaling pathways (e.g. PI3K/Akt/mammalian target of rapamycin, vascular endothelial growth factor, Notch, and Wnt/β-catenin pathways) are closely correlated with CSCs. 75 Therefore, targeting CSCs may be a promising approach to curing cancer patients. 76 Based on the recommended adjustment of survival analysis for known prognostic factors, a comprehensive analysis of published studies (ALDH1: 15 studies with 1557 cases and Nestin: 5 studies with 493 patients with advanced cancer who received adjuvant chemotherapy/radiotherapy) was performed. We found that ALDH1 positivity was significantly associated with a shorter OS (HR = 2.28, p < 0.001) but was not linked to DFS, RFS, MFS, or PFS. Additionally, evidence from some previously published studies is consistent with our analyses, where ALDH1 positivity was found to be correlated with worse OS in advanced cancers.27,46,48,50,51,54 A possible explanation for the results for the other outcomes might be different definitions of the various non-OS outcome measures.77,78 OS is almost always defined as the time from study enrollment to the date of death from any cause or the last follow up. OS is the most common standard endpoint because it is easy to measure and interpret and it is completely objective and unbiased. 79 We also found that the sample sizes in our analyses regarding the other outcome measurements (DFS, RFS, MFS, and PFS) were small (<350 patients per outcome measurement), which was confirmed by TSA. Further analysis of only the seven studies with 927 advanced cancer patients treated with adjuvant therapy also showed a significant association between ALDH1 positivity and poor OS (HR = 1.84, p = 0.001). Nestin-positive expression was also correlated with a significantly shorter OS (HR = 2.39, p < 0.001) and PFS (HR = 2.08, p < 0.001). These findings were verified by TSA and the results suggested that additional clinical studies are not needed to confirm these conclusions regarding OS of ALDH1 and Nestin. Our analyses suggest that ALDH1 and Nestin may be effective therapeutic targets to eliminate the subpopulation of CSCs and this may improve the treatment outcome of patients with advanced cancer.
Stratified analysis by cancer type suggested that ALDH1 positivity may be correlated with inferior OS in breast (HR = 1.67, p = 0.062), head and neck (HR = 3.99, p < 0.001), cervical (HR = 3.51, p = 0.034), and ovarian carcinomas (HR = 2.51, p = 0.003) but was not associated with OS in colorectal cancer (p = 0.129), suggesting that ALDH1 may play different roles in different cancer types and could become a potential target for the treatment of advanced breast, head and neck, cervical, and ovarian cancers. Moreover, evidence from some of the previously published studies on these specific tumor types is consistent with ours, such as colorectal cancer, 41 breast cancer,27,54 and head and neck carcinoma. 51 Stratified analysis by study source indicated that ALDH1 positivity was associated with a shorter OS for Japanese (HR = 1.94, p = 0.002) and Europeans (HR = 4.15, p < 0.001), but there was no association for Chinese (p = 0.506), which suggested that ALDH1 might only play a role in Japanese and European patients with advanced cancer and this may have potential implications to help stratify patients for treatment and prognostication. It is also possible that early detection, treatment schedules, and cancer-related lifestyles might to some extent differ in China compared with the rest of the world,80,81 which might have contributed to the lack of an association of the ALDH1 marker with the OS of Chinese patients. Stratified analysis by survival rate demonstrated that ALDH1 positivity was linked to an unfavorable OS at ⩾5 years (HR = 2.33, p < 0.001), and further analysis showed a reduced long-term OS rate at 10 years (HR = 1.76, p = 0.038). However, the eligible studies did not report long-term follow-up results, such as 10 years in terms of Nestin. According to the present analyses, ALDH1 might be a more important and meaningful marker than Nestin in advanced cancer. The above results of the subgroups were further confirmed by TSA, which suggested that more clinical studies were necessary to confirm these conclusions except for the subgroup of ⩾5-year OS.
Some limitations should be acknowledged. First, although we systematically searched the relevant databases as completely as possible, a slight publication bias was noted for the OS of ALDH1 data. Potential explanations for this are: (1) only final eligible studies published in English were selected. Studies of other types, such as unpublished papers or conference abstracts, were excluded because of incomplete information; (2) papers with positive results are more easily published than papers with negative results found in survival analyses, which are therefore lacking. Second, although the results were confirmed by TSA, and TSA suggested that only the results for OS were firm, most of these studies were retrospective in design. Third, the testing method and treatment regimens may impact the current findings of the subgroup analyses in this meta-analysis. Cancer is a heterogeneous disease and different cancer types may impact overall effect estimates; however, we did not find this factor to be a potential source of heterogeneity, possibly because the number of the eligible cancer types was relatively small. Fourth, we found that most eligible studies did not report that the assessors of the Nestin and ALDH1 tests were blinded to clinical findings. Finally, the REMARK guidelines only evaluate the reporting aspect of each study and they are not a tool for study quality assessment, because reporting quality and study quality are not necessarily interchangeable. For example, a prospective study design is more valuable and more easily achieved in a clinic in the future than any retrospective study design.
To conclude, our meta-analysis and TSA indicated that ALDH1 and Nestin were associated with shorter OS, and these two results were reliable. Nestin positivity may be correlated with a worse PFS, but ALDH1 positivity was not linked to DFS, RFS, MFS, or PFS. Subgroup analysis by cancer type showed that ALDH1 positivity may be correlated with poor OS in breast, head and neck, cervical, and ovarian cancers, but there was no association in colorectal cancer. Subgroup analysis by study source showed that ALDH1 positivity was linked to a worse OS for Japanese and European patients, but there was no correlation for Chinese patients. Subgroup analysis by survival rate demonstrated that ALDH1 positivity was associated with an unfavorable OS at 10 years. ALDH1 may be valuable as a potential effective therapeutic target for the improvement of treatment of advanced cancer in clinical practice. Additional high-quality, prospective, randomized clinical trials are needed to provide more conclusive evidence in different types of advanced cancer.
Supplemental Material
Supplementary_file_(1) – Supplemental material for Prognostic value of ALDH1 and Nestin in advanced cancer: a systematic meta-analysis with trial sequential analysis
Supplemental material, Supplementary_file_(1) for Prognostic value of ALDH1 and Nestin in advanced cancer: a systematic meta-analysis with trial sequential analysis by Susu Han, Tao Huang, Xing Wu, Xiyu Wang, Wen Li, Shanshan Liu, Wei Yang, Qi Shi, Hongjia Li, Kunhe Shi and Fenggang Hou in Therapeutic Advances in Medical Oncology
Footnotes
Author Contributions
Susu Han, Tao Huang, Fenggang Hou, and Kunhe Shi contributed to the conception and design of this research. Susu Han, Wen Li, Shanshan Liu, Wei Yang, Qi Shi, Hongjia Li, Xing Wu, and Xiyu Wang contributed to the drafting of the article and final approval of the submitted version. Susu Han, Tao Huang, Xing Wu, Xiyu Wang, Wen Li, Shanshan Liu, Wei Yang, Qi Shi, Hongjia Li, Kunhe Shi, and Fenggang Hou contributed to data analyses and interpretation and completion of the figures and tables. All authors read and approved the final manuscript.
Funding
This research was supported by grants from Shanghai Science and Technology Innovation Action Plan Project (NO. 16401970500-3). The sponsor had no role in the study design, data collection, data analysis, data interpretation, or writing of the report.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.