
Abstract
Background:
It is difficult to collect peripheral lung cancer samples. This study analyzed the applicability of endobronchial ultrasonography with a guide sheath (EBUS-GS) and computed tomography-guided transthoracic needle aspiration (CT-TTNA) for the diagnosis of peripheral lung cancer.
Methods:
A prospective analysis of peripheral lung cancer patients was performed. The study included 150 cases in the EBUS-GS group and 177 cases in the CT-TTNA group. The diagnostic rate, pathological type, genetic status and complications were analyzed.
Results:
The diagnosis rates were 64.0% and 97.7% in the EBUS-GS and CT-TTNA groups, respectively. The EBUS-GS group had undergone the most operations of the upper lobes of both lungs, while there was no significant difference in the operation distribution among the lobes in the CT-TTNA group. Adenocarcinoma (64 cases versus 51 cases) was most commonly observed in both groups, followed by squamous cell carcinoma. The detection rates of patients who were given a genetic test were 96.1% and 98.9% in the EBUS-GS and CT-TTNA groups, respectively. The incidence of complications in the EBUS-GS group was significantly less than that in the CT-TTNA group.
Conclusions:
EBUS-GS and CT-TTNA both had operational limitations. The diagnostic rate of EBUS-GS was lower than that of CT-TTNA, but there were fewer complications. CT-TTNA had better tolerance. According to the specific location of the lesion, we recommend EBUS-GS for lesions with a diameter ⩽30 mm and CT-TTNA for lesions with a diameter >30 mm. CT-TTNA specimens were advantageous for genetic testing.
Keywords
Introduction
Currently there are many diagnostic methods for primary lung cancer. Sputum examination, lung biopsy, 1 bronchoscopy, lymph node biopsy, surgical biopsy, etc., can all be used to collect tissue samples for cytology or histopathological examination and diagnosis. Primary diagnosis is more difficult in lung cancer patients with peripheral lung lesions compared to other patients. For patients whose specimens cannot be obtained by conventional bronchoscopy, both endobronchial ultrasonography with a guide sheath (EBUS-GS) 2 and computed tomography-guided transthoracic needle aspiration (CT-TTNA) 3 can be used as the diagnosis method. In this study, patients with peripheral pulmonary lesions (PPLs) who were considered to be possibly positive for lung cancer during primary diagnosis were selected to take part in a prospective study. The indication, significance and complications for the diagnosis of disease using EBUS-GS and CT-TTNA were analyzed.
Materials and methods
Recruitment criteria
This prospective study was conducted at the Shanghai Pulmonary Hospital, Tongji University School of Medicine, China. This study was approved by the Ethics Committee of Shanghai Pulmonary Hospital, Tongji University School of Medicine (ethics approval no. K17-143). All patients provided written informed consent for inclusion in this study. The study started in January 2014 and ended in April 2017. Recruitment criteria included: PPL confirmed by chest-enhanced CT; no definite diagnosis; no significant mediastinal lymph node enlargement of newly diagnosed patients; considered possible lung cancer by imaging diagnosis; tissue not obtainable through conventional bronchoscopy or EBUS-TBNA for pathological diagnosis; cancer cells not observable by sputum examination; Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0–2 points; normal electrocardiogram, blood routine and blood coagulation indicators; absence of organic diseases that could affect the operation; ability to tolerate local or general anesthesia; and no progressive hemoptysis (patients with a small amount of sputum blood can be used for examination). Patients with lung function who could not tolerate general anesthesia were excluded.
Patient grouping
This study recruited patients with PPL who were considered to potentially have lung cancer based on imaging, excluding patients who had been diagnosed by conventional bronchoscopy or EBUS-TBNA. The distance of lesions to the chest wall was >80 mm in the EBUS-GS group and ⩽80 mm in the CT-TTNA group. Patients whose distance between the lesions and the chest wall was ⩽80 mm but whose lesions were located beside the heart, large blood vessels and connected bronchioles were assigned to the EBUS-GS group. Patients whose distance between the lesions and the chest wall was >80 mm but ⩽100 mm and whose lesions did not contact bronchioles were assigned to the CT-TTNA group.
Instruments and methods
EBUS-GS was performed using a dedicated endobronchial ultrasonography instrument [Xenon light source: CLV-260SL; endoscopic ultrasound system: EU-ME1; cavity ultrasound probe: UM-S20-17S; UM-S20-20R, Olympus (Olympus Sales Service Co., Ltd., Beijin, China)] after 8 h of fasting. Patients were routinely given glottic local anesthesia with 2% lidocaine. 4 General anesthesia was performed for patients who could not tolerate local anesthesia. 5 An endoscope was inserted through the nasal cavity or mouth. When lesions were detected, tissues were collected by negative pressure suction (the 20 ml volume negative pressure syringe tube was attached to the back end of the guide sheaths and tissues were collected by negative pressure). CT-TTNA was performed with a SIEMENS 64-slice spiral CT [SOMATOM Definition AS, Siemens Co., Ltd. (Beijing, China)]. Patients received a subcutaneous injection of 2% lidocaine as local anesthesia. After locating the lesions with CT, tissues were obtained via core needle biopsy under negative pressure. Patients in the CT-TTNA group were routinely biopsied with an 80 mm needle; if the lesion from the chest wall was >80 mm but ⩽100 mm, a 100 mm needle was used for biopsy operation.
Observational indicators
The collected tissues were examined by smear, HE staining and liquid-based cytology for pathological analysis. If sufficient tissues were obtained, they were embedded in paraffin, sliced and subjected to pathological diagnosis. If the pathological diagnosis revealed lung cancer, we issued a clear diagnosis. If the pathology diagnosis was not clear, then we used additional methods to confirm the diagnosis, such as surgical biopsy. The location, size and sampling method of the lesions were recorded before the examination. After the examination, pathological results, complications and other findings were recorded.
Statistical analysis
After data collection, statistical analysis of the data was performed using a statistical software package [(SPSS for Windows, version 21.0; SPSS Inc. (IBM SPSS, Chicago, USA)]. Descriptive statistics was used for the baseline clinical characteristics. Enumeration data were described by percentage or rate. Chi-square test was used to compare the rates. p < 0.05 was considered statistically significant.
Results
Patient characteristics
A total of 339 patients were screened, of which four were biopsied directly because EBUS-GS or CT-TTNA examination could not be conducted due to the location of the lesions. A total of 335 cases were included in the study. There were 158 cases in the EBUS-GS group, which consisted of 86 (54.4%) males and 72 (45.6%) females. The ages ranged from 23 years to 81 years, with an average age of 59.5 ± 1.3 years (Table 1). Biopsy was not successful in eight cases (5.1%); the biopsy success rate was 94.9%. There were 177 cases in the CT-TTNA group, which consisted of 123 males (69.5%) and 54 females (30.5%). The ages ranged from 24 years to 93 years, with an average age of 63.0 ± 1.3 years. CT-TTNA biopsy success rate was 100%. For all patients, the ECOG PS was mostly 0–1 points. More PS2 patients had CT-TTNA than EBUS-GS (19.2% versus 5.7%) (p = 0.016). Table 2 presents the CT characteristics of the lung lesions before diagnosis.
Clinical characteristics of the patients.

CT characteristics of the lung lesions before diagnosis.

Biopsy results
Biopsy was successful in 150 cases (94.9%) in the EBUS-GS group. Two patients underwent EBUS-GS twice, and eight cases were unsuccessful, including six cases whose biopsy could not be performed due to undetectable lesions by ultrasound examination and two cases whose examinations were canceled due to uncontrollable preoperative hypertension. Biopsy was successful in 177 cases in the CT-TTNA group, of which biopsy was performed twice in 32 cases (18.1%) and three times in eight cases (4.5%). The success rate was 100%. The most biopsied area in the EBUS-GS group was in the right upper lobe [46 cases (30.6%)], followed by the left upper lobe [34 cases (22.7%)] and right lower lobe [33 cases (22.0%)]. Biopsy in the right middle lobe [13 cases (8.7%)] was the least prevalent. There was no significant difference in the frequency of biopsy area among different lobes in the CT-TTNA group (p = 0.742). Two groups of patients were mostly newly diagnosed cases (88.0% versus 78.5%). Thirty-eight cases (21.5%) in the CT-TTNA group with a disease course >3 months had large lesions. In the EBUS-GS group, 55 cases (36.7%) had lesions of 20–30 mm, followed by 10–20 mm [37 cases (24.7%)] and 30–40 mm [39 cases (26.0%)] (Figure 1). In the CT-TTNA group, 132 cases (74.6%) had lesions >30 mm (Figure 2). Twenty cases (11.3%) in the CT-TTNA group were biopsied using a 100 mm needle, all with one operation; there were no additional biopsies in these patients.
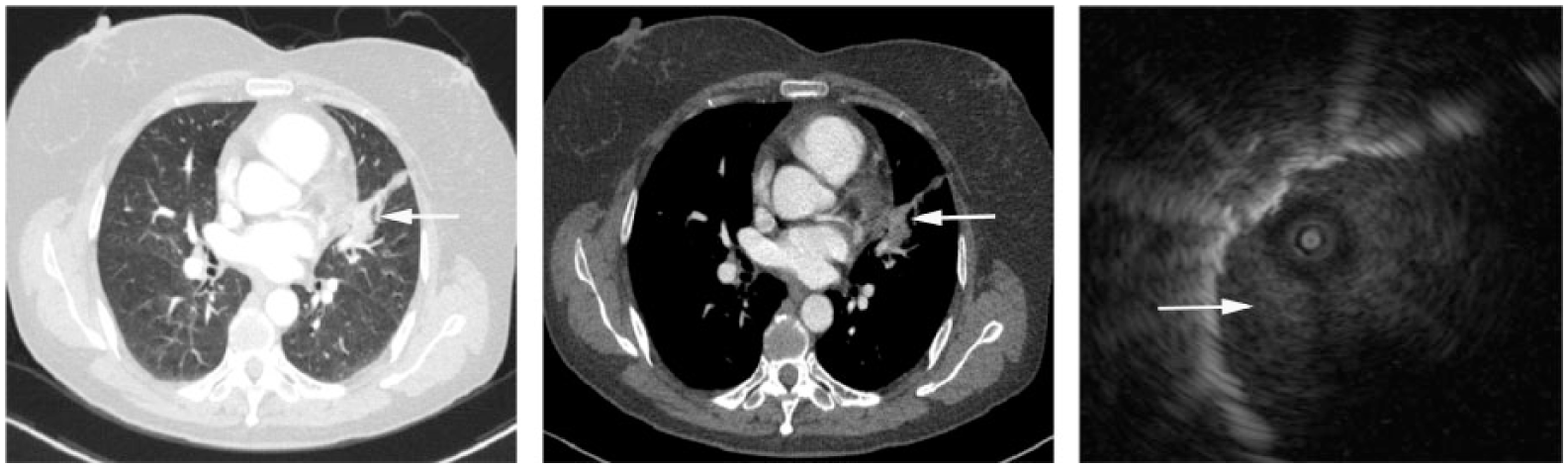
The distance from the lesions to the chest wall was 96 mm for this patient. The lesions were close to the heart. After EBUS-GS, the diagnosis was confirmed as adenocarcinoma by pathology. The mutation was identified as an EGFR 21 exon mutation (arrows point to the location of the lesion).

The lesions were located behind the ribs of this patient. The lesions were far away from the bronchioles, and thus EBUS-GS could not be performed. The biopsy point was 91 mm from the chest wall. CT-TTNA was performed with a 100 mm biopsy needle, and the diagnosis of adenocarcinoma was confirmed. The lesion was EGFR negative (arrows point to the biopsy needle).
Pathological results
Pathological examination was performed for the lesions obtained from the patients of the EBUS-GS and CT-TTNA groups. A clear diagnosis was issued for patients with direct diagnosis of lung cancer. For patients whose cancer tissue could not initially be obtained, tissues were collected during follow-up clinical examination for further diagnosis. The diagnosis rate of the EBUS-GS group was 64.0% (Table 3), and the diagnosis rate of the CT-TTNA group was 97.7% (Table 4), which was higher than that of the EBUS-GS group (p = 0.001). Among confirmed cases of the two groups, adenocarcinoma was the most common (64 cases versus 51 cases), followed by squamous cell carcinoma (10 cases versus 39 cases). Genetic testing was performed to direct the follow-up therapy for patients with confirmed adenocarcinoma, non-small cell lung cancer (NSCLC) or idioblast cells with tendency of NSCLC (Table 5). Diagnosis was confirmed in 29 cases of the CT-TTNA group with a second biopsy, and six cases were confirmed by a third biopsy. EBUS-GS examination was performed twice in two cases; the results were both negative.
Diagnosis results of EBUS-GS.

Abnormal cells (suspected lung cancer): final classifications: adenocarcinoma in four cases, squamous cell carcinoma in two cases, non-small cell lung cancer in two cases and malignant cells (not classified) in three cases.
Diagnosis results of CT-TTNA.

Abnormal cells (suspected lung cancer): final classifications: adenocarcinoma in three cases, squamous cell carcinoma in five cases, non-small cell lung cancer in one case and mesothelioma in one case.
Gene mutation results of positive cases in EBUS-GS and CT-TTNA examinations.

ALK, anaplasticlymphoma kinase; EGFR, epidermal growth factor receptor; ROS1, c-ros oncogene 1 receptor tyrosine kinase.
Operational complications
The most common postoperative complications of the EBUS-GS group were fever [16 cases (10.6%)] and a small amount of sputum (⩽30 ml/day) [14 cases (9.3%)]; 74.7% of patients did not have any complications (Table 6). The most common postoperative complications in the CT-TTNA group were pneumothorax [67 cases (37.9%)] and intrapulmonary hemorrhage [37 cases (20.9%)]. The EBUS-GS group was associated with significantly less risk than the CT-TTNA group (p = 0.001). Only one case had pneumothorax in the EBUS-GS group. The incidence of pneumothorax was 32.5% in 157 cases of the CT-TTNA group whose biopsies were performed using an 80 mm needle. The incidence of pneumothorax was 80% for 20 cases in which a 100 mm needle was used. One case of pneumothorax improved 2 weeks after closed thoracic drainage, and the remaining pneumothorax patients improved a few days after treatment. There were no irreversible complications in either group.
Postoperative complications of EBUS-GS and CT-TTNA examinations.

Genetic testing
For patients directly diagnosed with lung cancer in the EBUS-GS group and the CT-TTNA group, genetic testing was performed if their pathological results showed adenocarcinoma or NSCLC (including idioblast cells with NSCLC tendency). Genetic testing was performed in a small number of patients with squamous cell carcinoma. Among 77 cases of non-squamous cell carcinoma in the EBUS-GS group, genetic testing was not performed in three cases due to specimen issues; the detection rate was 96.1%. Genetic testing was not performed in only one case among 88 patients with non-squamous cell carcinoma in the CT-TTNA group, and the detection rate was 98.9%. This result may be related to better specimens obtained in the CT-TTNA group (the inner diameter of the 80 mm biopsy needle was 0.6 and 0.4 mm in the CT-TTNA group and the EBUS-GS group, respectively).
Discussion
It is difficult to collect specimens for peripheral lung cancer, especially in patients with small lesions. In the EBUS-GS group, the size of PPLs in 62.7% patients were <30 mm, conventional bronchoscopy could not see cancer tissue in the bronchial tube and the tissue could not be obtained through transbronchial biopsy. Therefore, the PPL must be punctured by EBUS-GS. EBUS-TBNA examination can be performed for patients with mediastinal lymphadenopathy. 6 EBUS-GS can only be considered when there is no lymphadenopathy. EBUS-GS technology is relatively new, while CT-TTNA is mature, but the two technologies have different applications. Slavova-Azmanova and colleagues 7 suggested that the use of EBUS-GS resulted in a decrease in CT-TTNA operation, but we thought both had limitations in operation and that EBUS-GS cannot completely replace CT-TTNA. EBUS-GS cannot obtain specimens in patients whose lesions are close to the chest wall and far from the bronchiole. It is difficult to obtain specimens for CT-TTNA in patients whose lesions are >100 mm from the chest wall and close to the heart blood vessels and the back of the scapula. Our hospital has 150 mm biopsy needles, but the needle body is too long and soft, and biopsy accuracy cannot be guaranteed for biopsy over a long distance. Therefore, the clinical use of this needle is very limited. For cases whose specimens cannot be obtained by either method, bronchoscopic transparenchymal nodule access (BTPNA) 8 can be attempted, but this technique is not yet fully mature and the diagnostic rate remains to be ascertained. In this study, the tolerance of EBUS-GS was slightly worse than CT-TTNA. The oldest patient in the CT-TTNA group was 93 years old, and this patient was diagnosed with adenocarcinoma and no postoperative complication was observed. In the EBUS-GS group, six patients had no lesions detected by ultrasound, and the preoperative CT showed that the lesions were close to the bronchioles. This may occur because the EBUS-GS probe was unable to access the lesions located in smaller bronchi. In this study, EBUS-GS was relatively easy to operate for lesions in both upper lobes, and CT-TTNA had no obvious specificity for the location of the lesion. In the EBUS-GS group we used two kinds of guide sheaths: one was 2.0 mm and the other was 2.6 mm. The decision of which of these tools to use depended on the location of the lesions and the relationship between the airway and lesions. The diagnostic rate of the small guide sheath was lower than the larger guide sheath because of the small tools and inadequate specimen. If we could use rapid on-site evaluation (ROSE) or other tools, just like brush needle, to perform the biopsy we believed we would achieve a higher diagnostic rate. Performing TBNA was a good idea in the EBUS-GS procedure, but we thought that not every lesion was appropriate for performing TBNA. Also, we needed x-ray to confirm the security of TBNA, and the x-ray could harm patients and doctors. As such, we opted not to follow this route. Lesions with diameters ⩽30 mm were suitable for EBUS-GS; for larger lesions, especially those with diameter >30 mm, CT-TTNA examination is more suitable. For patients with larger lesions and negative results in the primary biopsy, there were greater chances for two or three biopsy samplings. We recommend EBUS-GS for lesions with diameters ⩽30 mm and recommend CT-TTNA for lesions with diameters >30 mm. For 20 mm PPLs, EBUS-GS combined with virtual bronchoscopic navigation can have a diagnostic rate of 69%. 9 In addition, if PPL has high [ 18 F]-fluoro-2-deoxy-d-glucose ( 18 F-FDG) uptake, combination with EBUS-GS can improve the diagnostic rate. 10
In this study, the diagnosis rate of the EBUS-GS group was 64.0%, which was significantly lower than that of the CT-TTNA group (97.7%) (p = 0.001). In Wang and colleagues’ study, 11 the malignancy diagnosis rate of EBUS-GS was 79%, which is higher than that shown here. This may be related to the high number of cases in this study. The diagnostic rate of the CT-TTNA group was similar to that of Wang and colleagues’ study (93%). In the CT-TTNA group, 29 cases had two biopsies and six cases had three biopsies to confirm the diagnosis. The results were both negative for two cases that underwent EBUS-GS examination twice, which might be related to the fact that multiple CT-TTNA operations could improve the diagnostic rate, whereas multiple EBUS-GS examinations had no obvious significance. The primary negative results of CT-TTNA might be false negatives, 12 so in this study some patients had two or three operations. Computed tomography-guided transthoracic needle biopsy (CT-TTNB) 13 had a higher diagnosis rate of malignant disease than did CT-TTNA, but the small PPLs in this study were not suitable for CT-TTNB. For lesions around 20 mm, electromagnetic navigation bronchoscopy (ENB) can be considered if neither method can obtain the specimens. 14 However, ENB cannot be carried out extensively due to the high cost. Among the cases with clear diagnosis, adenocarcinoma accounted for the majority, with 64 and 51 cases in the EBUS-GS group and CT-TTNA group, respectively. Among EBUS-GS patients without clear diagnosis, adenocarcinoma was still the majority established through follow-up diagnosis. The CT-TTNA group had slightly better quality specimens than the EBUS-GS group for subsequent genetic testing, which may be associated with a higher quantity of specimens in the CT-TTNA group. As the inner diameter of the biopsy needle was 0.6 and 0.4 mm in the CT-TTNA group and the EBUS-GS group, respectively, we could obtain more tissue through CT-TTNA than EBUS-GS for genetic testing. In the CT-TTNA group, for example, we did genetic testing in 51 adenocarcinoma patients, among them 44 (86.3%) patients underwent epidermal growth factor receptor (EGFR), anaplasticlymphoma kinase (ALK) and c-ros oncogene 1 receptor tyrosine kinase (ROS1) testing, and 7 (13.7%) patients only underwent EGFR testing. In the EBUS-GS group, 42 (67.7%) patients underwent EGFR, ALK and ROS1 testing, and 20 (32.3%) patients only underwent EGFR testing. CT-TTNA is still advantageous if better tissue specimens are needed for genetic testing (p = 0.001). There were 25 and 31 patients with EGFR mutations in the EBUS-GS group and CT-TTNA group, respectively. The probability of mutations of ALK and ROS1 is extremely low. CT-TTNB is more suitable if more accurate genetic analysis is needed or for the diagnosis of metastatic lung cancer. 15 Sakamoto and colleagues 16 suggested that bronchial lavage fluid can be used for EGFR testing during EBUS-GS examinations, but we still recommend genetic testing using pathological specimens.
This study showed that patients without postoperative complications comprised 74.7% and 23.7% in the EBUS-GS group and CT-TTNA group, respectively. EBUS-GS was significantly safer (p = 0.001), but EBUS-GS had a higher selection standard for patients before the operation due to patient tolerance. Heerink and colleagues’ 17 meta-analysis suggested that the complication rate was 24.0% for CT-TTNA. There were more complications in this study, which may be associated with the greater number of patients with small lesions enrolled in this study. After EBUS-GS, complications of small amounts of sputum [14 cases (9.3%)] and fever [16 cases (10.6%)] can be improved via short-term treatment. In Oki and colleagues’ 18 multi-center study, the incidence of pneumothorax and bleeding was 5% during EBUS-GS. Therefore, operations should still be performed with caution. In the study by Xu and colleagues, 19 pneumothorax and hemoptysis were not observed during EBUS-GS, which may be associated with small lesions in our study. The most common complication after CT-TTNA was pneumothorax [67 cases (37.9%)], especially for a 100 mm biopsy needle, and the incidence of pneumothorax was 80.0%; therefore, 100 mm needles should be used carefully. We recommend chest CT immediately after the completion of biopsy to determine whether there is pneumothorax. Pneumothorax should be treated immediately. The guide wire technique provides a novel method with CT-TTNA to reduce the incidence of complications. 20 Intrapulmonary hemorrhage [37 cases (20.9%)] consisted of a small amount of bleeding in the needle channel after CT-TTNA biopsy. Small amounts of bleeding can self-absorb and generally do not need special treatment. For patients with pulmonary hypertension, the probability of complicated bleeding is 26% after CT-TTNA, 21 which can be accompanied by hemothorax; thus, indications need to be considered before the operation.
The study began in January 2014. The number of cases collected by the end of the study was still low. More cases and longer follow-up times are needed to increase the accuracy of the data.
Conclusion
For peripheral lung cancer, EBUS-GS and CT-TTNA each had operational limitations. The diagnostic rate of EBUS-GS was lower than that of CT-TTNA, but EBUS-GS had fewer complications. CT-TTNA had good tolerance but required attention for postoperative pneumothorax and intrapulmonary hemorrhage. Additionally, 100 mm biopsy needles should be used with caution. According to the specific location of the lesion, we recommend EBUS-GS for lesions with diameters ⩽30 mm and recommend CT-TTNA for lesions with diameters >30 mm. CT-TTNA is still advantageous if better tissue specimens are needed for genetic testing.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.