
Abstract
Background:
The anti-programmed cell death-1 (PD-1) and anti-programmed cell death ligand-1 (PD-L1) immunotherapies have shown exceptional activity in many cancers. However, these immunotherapies can also result in diverse adverse cutaneous eruptions that need to be better characterized for ongoing management. The objective was to provide clinical and histopathologic descriptions of the variety of cutaneous adverse events seen in patients who received anti-PD-1/PD-L1 treatment and discuss their management.
Methods:
Patients with advanced cancers in clinical trials at University of California Los Angeles (UCLA), receiving anti-PD-1/PD-L1 treatment between 2012 and 2016 who developed cutaneous eruptions and were evaluated in the dermatology clinic were included in this retrospective case series study. A total of 16 patients were included in this study; of these, five were treated with pembrolizumab alone, two with avelumab alone, eight with nivolumab plus ipilimumab and one with nivolumab plus T-Vec. Of these 16 patients, eight had received systemic chemotherapy, six had received radiotherapy, and one had received trememlimumab prior to the immunotherapies described in this study.
Results:
Cutaneous eruptions occurred at variable times, from week 1 to 88, with a median of 11.5 weeks; the morphologies included lichenoid, bullous, psoriasiform, macular, morbiliform appearances, and alopecia which were confirmed histopathologically in several of the cases. All cutaneous immune-related adverse events were either grade 1 or 2. Ten patients were treated with topical corticosteroids, and one also received NBUVB. Four patients eventually required systemic steroids. Three required discontinuation of their anti-PD-1/PD-L1 therapy secondary to the cutaneous eruptions.
Conclusions:
There are several different types of adverse cutaneous morphologies that may be seen with administration of PD-1 and PD-L1 inhibitors. Identifying the patterns of eruption may assist in prompt treatment. Most eruptions could be managed with topical corticosteroids and without discontinuation of the systemic treatment.
Keywords
Introduction
The immune response to cancer involves a complex network of cellular and molecular interactions. Many advanced cancers have adopted methods to evade immune detection and clearance; one pathway involves overexpression of programmed cell death ligand-1 (PD-L1). PD-L1 binds to PD-1 on T-cells and suppresses their activity. 1 By blocking this interaction, the host immune response can be improved, potentially augmenting the anti-tumor response. PD-1 modulation has been found to be important in numerous cancers, including renal cell carcinoma, head and neck squamous cell carcinoma, melanoma, and non-small cell lung cancer, with activity against other tumor types being tested. Although only a minority of patients have clinical responses, those that do often have a durable response.1–5
Blockade of PD-1 has proven to be particularly efficacious, with fewer side effects than prior immunomodulatory therapies. Nivolumab and pembrolizumab are IgG4 antagonist antibodies against PD-1, while avelumab, atezolizumab and durvalumab are IgG1 antibodies against PD-L1. All these agents have shown good activity in lung cancer and other solid tumors. These inhibitors are generally well tolerated, though some of the most common immune-related adverse events (irAE) are cutaneous rash or pruritus. Up to 40% of patients in recent clinical trials experienced some type of cutaneous manifestation.6–10
As more of these immunotherapies are utilized in trials and general practice, the incidence of observed dermatologic side effects will continue to rise. Many of these agents have only recently received approval or currently remain in trials; thus their toxicity profiles are still being fully defined. The breadth of cutaneous manifestations of immune checkpoint inhibitors have yet to be fully understood. Here we present the course, description, biopsy results and management of differing rashes in several patients with a variety of malignancies, undergoing treatment with checkpoint inhibitors, either as a single agent or in combination with another immunomodulatory agent. Our goal was to describe the spectrum of cutaneous toxicities that developed during administration of these agents as well as highlight the clinical course and discuss potential management strategies.
Methods
Cases were collected based on patients seen by the authors in the oncology and dermatology clinics. All patients were initially part of clinical trials testing the efficacy of novel immunotherapies in malignancy, approved by the UCLA Institutional Review Board (#16-000790). Written informed consent was obtained at the initial clinic visit and the IRB approval and informed consent also covered this case series. Data were collected retrospectively. Patients were included if they were receiving treatment with an anti-PD-1 or anti-PD-L1 agent alone or in combination with another immunotherapy (primarily ipilimumab). Data for patients evaluated between 2012 and 2016 were collected and included demographic information, treatment regimen, morphology and distribution of skin lesions, histopathologic information (if skin biopsy was performed), treatments utilized and overall tumor response. Overall tumor response was determined by the treating oncologist and classified using RECIST (Response Evaluation Criteria in Solid Tumors). Time to progression was determined based on start date of immunotherapy until disease progression as documented by imaging.
Results
A total of 16 patients were included (11 men and 5 women). Of these, five were treated with pembrolizumab alone, two with avelumab alone (one of these patients later was treated with another PD-1 inhibitor, REGN2810 with recurrence of rash), eight with nivolumab plus ipilimumab, and one with nivolumab plus T-Vec. Of these patients, eight had received prior systemic therapy for their cancer, and six had received radiotherapy. One had received a prior immune checkpoint inhibitor (tremelimumab); a summary of patient characteristics is provided in Table 1.
Clinical and histopathological information of 16 patients with cutaneous adverse eruptions while receiving anti-PD-1 or anti-PD-L1 treatment.

Cutaneous eruptions manifested at various time points in treatment, ranging from as early as the first week to as late as week 88, with a median of 11.5 weeks. The morphologies were variable and included lichenoid, eczematous, bullous, urticarial, psoriasiform, macular, and morbiliform appearances (Figure 1), and one case of non-scarring alopecia. Many of the eruptions occurred on the arms, trunk and lower extremities, though one was exclusively facial (malar distribution). None developed mucosal lesions. All but three patients noted pruritus with the lesions. All eruptions were either grade 1 or grade 2.
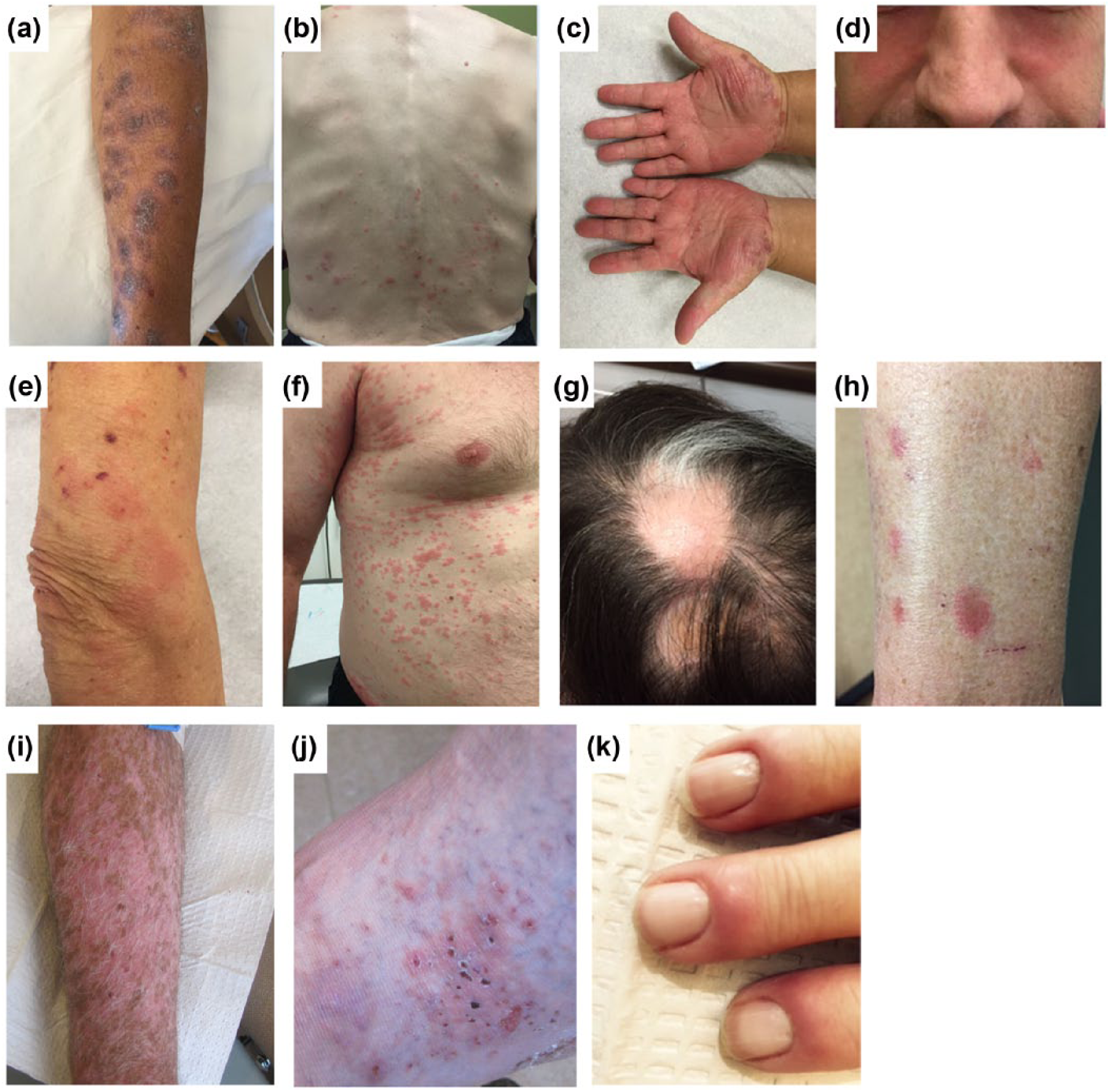
Clinical photographs of diverse eruptions due to anti-PD-1 or anti-PD-L1 therapy. (a) Erythematous and hyperpigmented papules and plaques (lichenoid eruption in photodistributed pattern; patient 1). (b) Erythematous papules and plaques on back (urticarial eruption, patient 2, second eruption). (c) Erythematous scaly papules and plaques on palmar surface of hands (psoriasiform eruption, patient 6). (d) Erythematous patches in malar distribution (patient 7). (e) Erythematous papules and plaques on arm (eczematous eruption, patient 8). (f) Erythematous macules and papules (morbiliform eruption, patient 9). (g) Non-scarring alopecia (alopecia areata, with regrowth of white hair; patient 10). (h) Erythematous macules (eczematous eruption; patient 11). (i) Hypopigmented and depigmented macules (vitiligo reaction; patient 13). (j) Eroded vesicles and urticarial plaques (bullous pemphigoid; patient 14). (k) Periungual erythema (10-finger paronychia; patient 15).
The most common treatment was topical steroids, followed by systemic antihistamines. Four patients eventually received systemic steroids for resolution of the cutaneous eruptions, while one received NBUVB (narrow band ultraviolet B) treatment in combination with topical steroids. Four patients elected not to receive treatment.
Tumor response, time to progression, grade of cutaneous irAE and development of any other irAEs were also assessed (Table 1). One patient with a prior history of psoriasis experienced a psoriasis flare. Histopathologic analysis was available for seven of the 16 patients and showed patterns consistent with the clinically described morphologies (Figure 2; Table 1). All patients eventually had resolution of their cutaneous irAEs. Of the 16 patients in this study, four required permanent discontinuation of their immunotherapy treatment for any irAE, with two requiring permanent discontinuation for cutaneous irAEs (patients 14 and 16).
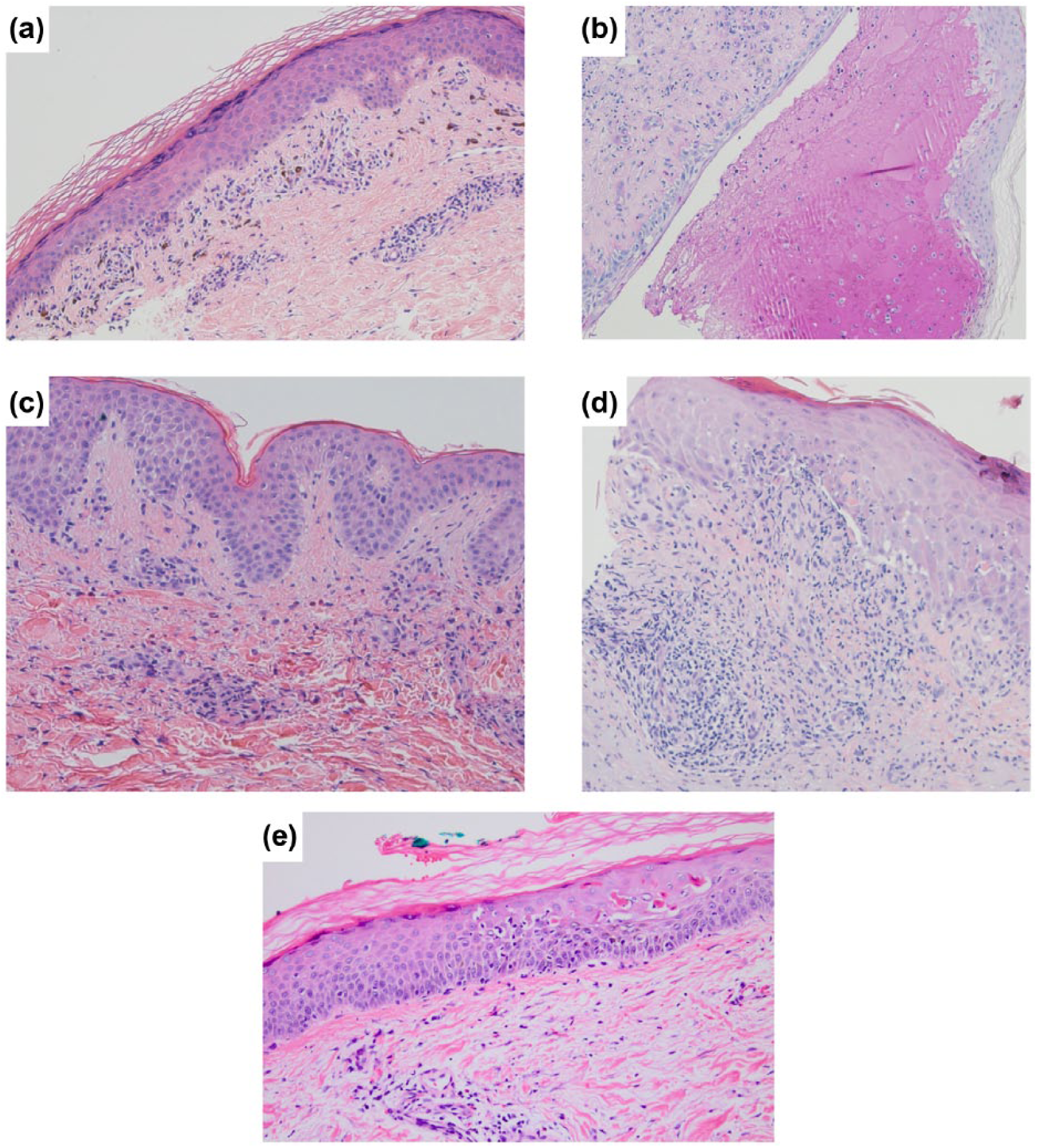
Photomicrographs of biopsy specimens. (a) Superficial perivascular lymphocyte inflammatory infiltrate (patient 1); hematoxylin and eosin (H&E) staining, 10× magnification. (b) Epidermal spongiosis and intraepidermal neutrophilic and eosinophilic pustules (patient 2; first eruption); periodic acid-Schiff (PAS) staining, 10× magnification. (c) Eosinophilic spongiosis with focal subepidermal clefting (patient 2, second eruption); H&E staining, 10× magnification. (d) Spongiotic psoriasiform and interface dermatitis with necrotic keratinocytes (patient 5); H&E staining, 10× magnification. (e) Epidermal spongiosis with patchy necrotic keratinocytes and dermal lymphocyte predominant perivascular infiltrate (patient 11); H&E staining, 10× magnification.
Discussion
Cutaneous side effects have been reported to occur in up to 40% of patients on immunotherapies.6–10 While the initial studies often described the cutaneous manifestations as a ‘rash’, 1 more recent studies have begun to delineate the variety of eruptions that may occur as a result of immunotherapies.9–12 Our study aimed to further characterize the spectrum of cutaneous adverse effects. The clinical morphologies varied significantly among patients, and histopathology was consistent when performed.
Most of the cutaneous adverse effects were mild and could be adequately managed with topical corticosteroids, with only a minority requiring systemic steroid treatment and, importantly, few requiring permanent discontinuation of immunotherapy. Other case series have reported lichenoid and bullous eruptions secondary to PD-1 inhibition, with similar treatment courses and resolution with topical treatment.9,12 These eruptions may appear similar to idiopathic dermatitis, including lichen planus, psoriasis, or bullous pemphigoid, though the molecular mechanisms are different and the cutaneous irAEs usually resolve with discontinuation of the inciting agent, rather than waxing and waning as idiopathic dermatitis often does.
Eight of the 16 patients included were treated with anti-PD-1 antibody concomitant with anti-CTLA4 blockade (ipilimumab). Ipilimumab itself may cause a cutaneous eruption which often appears as erythematous papules and plaques (morbiliform).4,13 Other morphologies have not yet been reported due to ipilimumab alone, suggesting that eruptions observed in this study are more likely due to anti-PD1 alone or potentiated by the combination. 4
The mechanism by which cutaneous eruptions occur through PD-1/PD-L1 inhibition is unknown. It is thought they may occur due to aberrant targeting of dermal antigens by reactivated T-cells, which generates inflammation after cross-reaction with normal skin.8,9 For bullous eruptions, some of the autoantigens are suspected to be either hemidesmosomal structural proteins, BP180, or BP230.12,14 However, specific self-antigens that may recruit such T-cells have not yet been identified. One possibility is that the immunotherapy may unmask or amplify a pre-existing response. Since PD-1 modulation is not specific to cancer antigens, it is possible that autoreactive T-cells may be unmasked. Further study of these particular T-cells, including efforts to identify the specificity of T-cell receptors, may provide additional insight into the mechanism underlying these eruptions and may identify strategies to mitigate them.
Conclusion
There is a wide range of adverse cutaneous morphologies seen with PD-1/PD-L1 inhibitors. Elucidating the patterns of eruptions may assist clinicians in identifying suspected cutaneous adverse events and initiating timely treatment. The morphologies have included papular/morbiliform, eczematous, urticarial, bullous, hypopigmented, lichenoid or psoriasiform eruptions or non-scarring alopecia. In most cases, the eruptions are relatively mild and can be treated with topical corticosteroids with the possible addition of systemic antihistamines for pruritus. More severe eruptions may be treated with systemic corticosteroids, with or without temporarily discontinuing immunotherapy. This case series provides a sampling of the diverse cutaneous eruptions that may be seen with PD-1/PD-L1 inhibition. Further monitoring of patients and analysis of existing data may help to determine whether cutaneous eruptions are associated with clinical responses or improved outcomes, and additional research may help to design strategies to better mitigate such adverse eruptions while still maintaining efficacious anti-tumor response.