
Abstract
Hyponatremia is the most common electrolyte disorder in lung cancer patients. This condition may be related to many causes including incidental medications, concurrent diseases and side effects of antineoplastic treatments or the disease itself. Although not frequently life-threatening, it is usually associated with prolonged hospitalization, delays in scheduled chemotherapy, worsening of patient performance status and quality of life and may also negatively affect treatment response and survival. Most of the available data focus on thoracic tumors, especially small-cell lung cancer (SCLC), where hyponatremia is frequently related to the syndrome of inappropriate secretion of antidiuretic hormone (SIADH). Few studies specifically focus on non-small cell lung cancer (NSCLC) patients. Hyponatremia treatment needs to be personalized based on severity and duration of sodium serum reduction, extracellular fluid volume and etiology. However, literature data highlight the importance of early correction of the serum concentration levels. To achieve this the main options are fluid restriction, hypertonic saline, loop diuretics, isotonic saline, tolvaptan and urea. The aim of this review is to analyze the role of hyponatremia in lung cancer patients, evaluating causes, diagnosis, management and clinical implications.
Introduction
Electrolytic disorders are common in cancer patients and may worsen patient prognosis. Among these disorders, hyponatremia is the most common although its prevalence is not well known.
Several guidelines suggest that hyponatremia is defined as serum sodium concentration (Na+) lower than 135 mmol/l, 1 with different degrees of severity (mild 130–134 mEq/l, moderate 125–129 mEq/l and severe <125 mEq/l). 1 However different cutoffs have been used to classify patients based on their hyponatremia levels. 2 Several factors might lead a cancer patient to hyponatremia, such as incidental medications, concurrent diseases, side effects of antineoplastic treatments or the cancer itself. Although not frequently life-threatening, it usually causes prolonged hospitalization, delay in scheduled chemotherapy and worsening of patient performance status and quality of life.3,4 Out of different types of cancer, lung cancer is the one most frequently associated with hyponatremia; retrospective studies showed an incidence of about 20–44% in this setting.2,5–7 According to Hermes and colleagues the incidence of hyponatremia in small-cell lung cancer (SCLC) is 18.9% and correlates with disease stage at diagnosis; 24% in patients with extensive disease compared with 11% in those with limited disease. 8 In metastatic patients, those with liver and pleural metastases are more likely to develop hyponatremia, according to Hansen and colleagues. 5 Few studies have specifically focused on non-small cell lung cancer (NSCLC) patients.2,9–12 The estimated incidence of the syndrome of inappropriate secretion of antidiuretic hormone (SIADH) in this subgroup of patients is about 2–4%. 9
The aim of this review is to analyze the role of hyponatremia in lung cancer patients, evaluating causes, diagnosis, management and clinical implications.
Methods
We extensively reviewed the available scientific literature, searching studies on hyponatremia published between 1982 and April 2017, using PubMed and MEDLINE databases. The search was limited to English language publications. The search terms included hyponatremia, lung cancer, chemotherapy, survival and syndrome of SIADH. Full articles were obtained and we checked for additional appropriate references. Where results were reported or updated in more than one publication, only the most recent one was used.
Etiology
Sodium homeostasis is regulated through an integrated system involving antidiuretic hormone (ADH, also known as vasopressin or AVP) and kidney excretion of water and sodium. In normal conditions, ADH is secreted by the posterior pituitary in response to increased plasma osmolality or decreased blood volume and pressure. The same causes arise in renin production by the kidney with activation of angiotensin II and the aldosterone system. ADH production inhibits aldosterone secretion.13,14 The aim of this mechanism is to regulate the levels of serum osmolality and Na+ content within the normal ranges of 275–295 mOsm/kg and 135–145 mmol/l, respectively.15,16
Classification of hyponatremia depends on serum osmolality levels: isotonic (275–295 mOsm/kg), hypertonic (>295 mOsm/kg) and hypotonic (<275 mOsm/kg). Pseudohyponatremia is a laboratory artifact related to marked elevations of either proteins or lipids in serum. This condition must be considered for differential diagnosis of hyponatremia but it does not need any action.
Isotonic and hypertonic hyponatremia occur where there is an increase in osmotically active solutes in the extracellular fluid and, consequently, a water efflux from the intracellular to the extracellular space. These conditions occur, for example, in cases of hyperglycemia.17–19
Out of the two, hypotonic hyponatremia is the most frequent subtype in cancer patients and it can be classified as euvolemic, hypervolemic or hypovolemic based on the extracellular fluid (ECF) volume (Table 1).20,21 Hypovolemic hyponatremia can be caused by renal fluid and solute losses, vomiting, diarrhea, adrenal insufficiency (i.e. Addison’s disease and adrenal gland destruction), nephropathy and cerebral salt wasting. Hypervolemic hyponatremia occurs when there is an excess of total body water, a typical symptom of several edematous states such as cirrhosis, nephrotic syndrome and congestive heart failure.22,23 Euvolemic hyponatremia shows normal ECF levels because the increase of total water is predominantly occurring in the intracellular space. The most frequent cause of this subtype of hyponatremia in cancer patients is SIADH, but also endocrinopathies such as pure glucocorticoid deficiency or hypothyroidism and polydipsia and beer potomania should be considered. 2 SIADH is due to increased secretion from the pituitary gland or to ectopic production of ADH by tumor cells. High levels of ADH cause a reduction of renal free water excretion, which leads to serum hypoosmolality and hyponatremia.24,25
Causes of hypotonic hyponatremia.
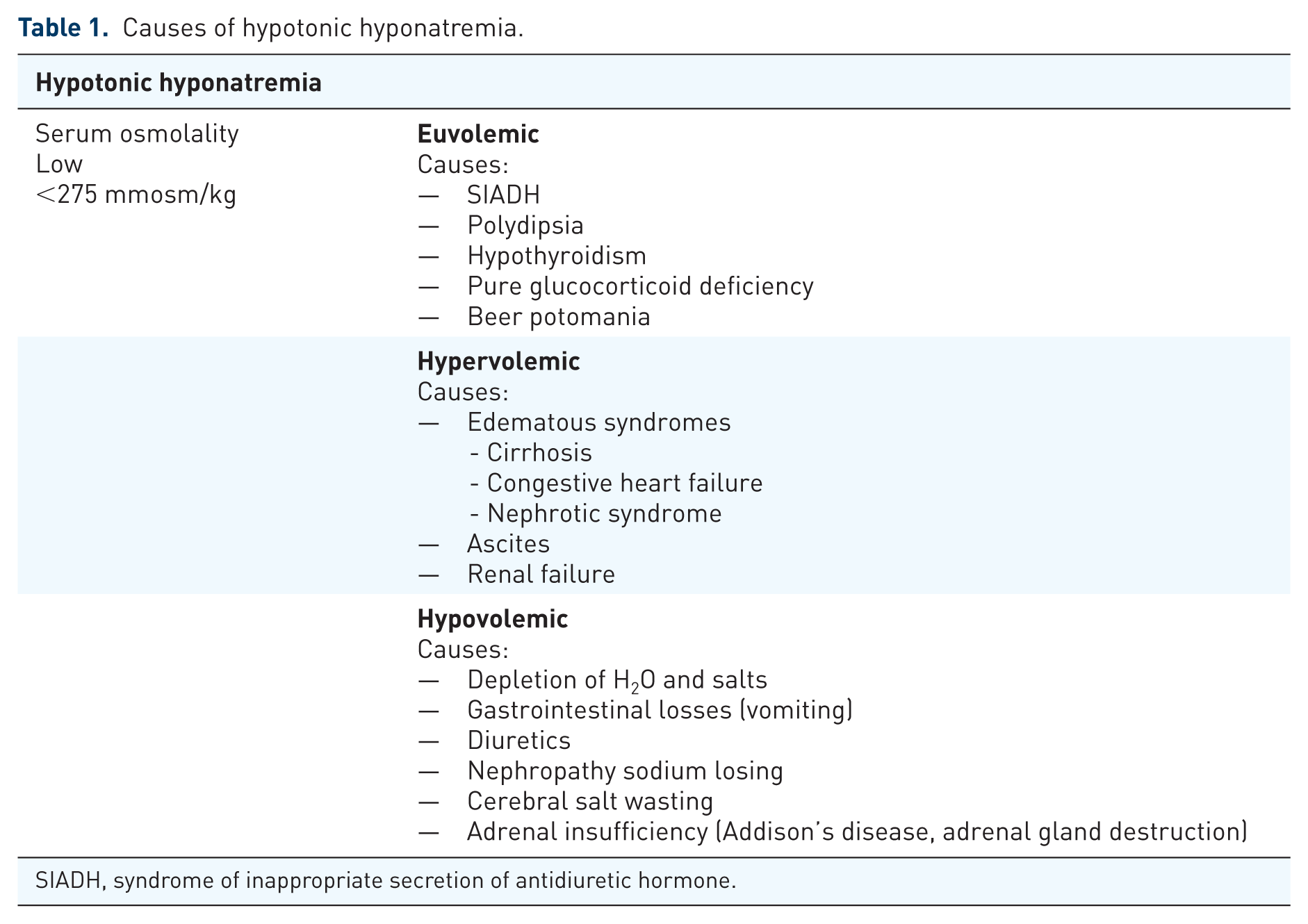
SIADH, syndrome of inappropriate secretion of antidiuretic hormone.
SIADH has been identified in different solid tumors, although the incidence is higher in SCLC.26–28
In lung cancer patients, other pulmonary disorders such as asthma, chronic obstructive pulmonary disease, acute respiratory failure or positive-pressure ventilation are responsible for SIADH. 14
Furthermore, anticancer therapies or other concomitant treatments can cause hyponatremia through different mechanisms (Table 2). 29
Drugs inducing hyponatremia and their mechanism of action.

ADH, antidiuretic hormone.
Prabhash and colleagues confirmed the role of anticancer drugs in producing this electrolyte disorder. In particular, their retrospective study showed an association between platinum drugs, alkylating agents, vinca alkaloids, epidermal growth factors receptor monoclonal antibody inhibitors, tyrosine kinase inhibitors and the occurrence of hyponatremia. 30 Case reports had already demonstrated that patients treated with the chemotherapy regimen vinorelbine, cyclophosphamide or methotrexate are more likely to develop hyponatremia.31–33 In a recent study focused on the use of carboplatin in NSCLC, Ma and colleagues found that its use was significantly associated with occurrence of hyponatremia. 34 The mechanism of action could be explained by excessive water ingestion and decreased serum electrolyte concentrations.
The association between pemetrexed and hyponatremia was analyzed by Gota and colleagues in 46 patients with advanced NSCLC. 35 A total of 16 patients (35%) receiving pemetrexed experienced at least one episode of grade 3 hyponatremia (<130–120 mmol/l) according to the Common Terminology Criteria for Adverse Events 4.03 (CTCAE). Patients affected by severe hyponatremia (⩽124 mEq/l) had a lower pemetrexed clearance compared with patients with normal sodium concentration (p = 0.001).
Diagnosis and clinical presentation
Hyponatremia can be diagnosed by chance in asymptomatic patients during routine laboratory tests or it can be suspected in cancer patients who develop suggestive (mostly neurological) symptoms. 13
When hyponatremia has been detected, additional laboratory investigations are needed for a correct differential diagnosis and appropriate therapy choice (Figure 1).13,36 Euvolemic hyponatremia in lung cancer patients, especially SCLC, should suggest the diagnostic hypothesis of paraneoplastic SIADH.
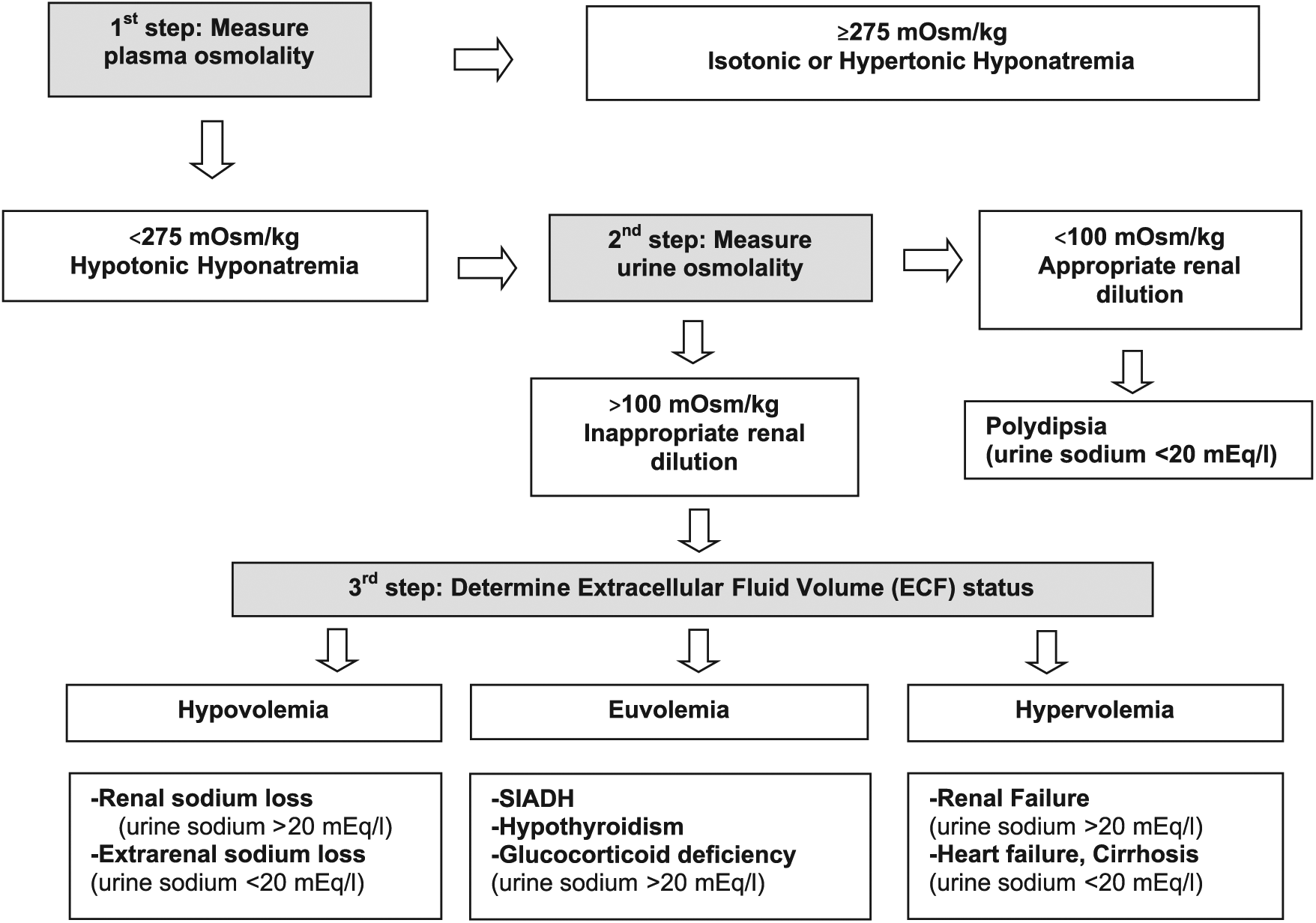
Algorithm for first diagnostic approach to hyponatremia.
The main diagnostic criteria for SIADH are: reduced plasma osmolality <275 mOsm/kg, increased urine osmolality >100 mOsm/kg, euvolemic status, increased urinary sodium >30 mEq/l, normal kidney, thyroid and adrenal function. Additional diagnostic criteria are: no use of diuretics, reduced blood uric acid <4 mg/dl, reduced blood urea nitrogen (BUN) <10 mg/dl, increased sodium renal excretion fraction >1%, and increased urea excretion fraction >55%. 37 The severity of clinical presentation depends on the magnitude of the hyponatremia as well as on the speed of decline in serum sodium concentration. In fact, hyponatremia can be classified as acute, if it develops within 48 h, and chronic, if it develops over 48 h, a timeframe that allows the brain to initiate adaptive mechanisms. Patients with acute hyponatremia present different alterations that can vary from unspecific symptoms such as headache, nausea, vomiting and muscle cramps, to life-threatening conditions such as bradycardia, hypertension, impaired regulation of body temperature, cerebral herniation, convulsions and coma.38–41 Chronic hyponatremia is usually an asymptomatic condition or, at worst, results in weakness, nausea, vomiting and loss of appetite. Recent studies have shown long-term side effects even for mild-to-moderate hyponatremia such as deficits in gait and attention, falls, bone losses and fractures.42–44
Treatment
Hyponatremia treatment needs to be personalized depending on the severity and duration of sodium serum reduction, ECF volume and etiology. 45 In the last few years, several international and national expert panels have published guidelines for detecting and managing this electrolyte disorder in cancer patients, although with differences in recommendations.13,46,47 Firstly, it is recommended to detect the cause of reduced sodium concentration, although the increase in sodium concentration levels is likely to be the main issue in life-threatening hyponatremia.
Sodium correction needs to be managed with care, to avoid an overcorrection causing a neurological side effect described as central pontine myelinolysis. Chronic hyponatremia induces the brain’s adaptation to hyposmolality of extracellular space by the secretion of osmotically active solutes. When the extracellular sodium concentration increases too rapidly, cells are not able to adapt, leading to blood–brain barrier damage, influx and activation of complement that leads to osmotic demyelination. In this case, after an initial clinical benefit due to a rapid rise in sodium levels, patients experience progressive neurological impairment, which can result in irreversible damage.41,48 Risk of osmotic demyelination syndrome is high in patients with chronic and severe hyponatremia (⩽105 mmol/l), hypokalemia, as well as in those with history of alcoholism, malnutrition or liver failure. The limit of correction is 4–6 mmol/l in the first 24 h. Serum sodium concentration and urine volume must be closely monitored until Na+ >125 mmol/l. In case of hypercorrection (>8 mmol/l/24 h), re-lowering is recommended. For patients without high risk factors, the limit of hyponatremia correction is an increase in sodium concentration of <10–12 mmol/l in 24 h and of <18 mmol/l in 48 h.46,48
The importance of early correction is generally acknowledged. Even if most patients with mild chronic serum sodium reduction are usually asymptomatic, they may have a higher risk of complications such as gait instability, falls or fractures. Clinical effects of hyponatremia are enhanced in hospitalized cancer patients.49–51
In cases of isotonic and hypertonic hyponatremia, physicians have to correct the underlying issues, except for pseudohyponatremia that does not need any action, as mentioned earlier. For hypotonic hyponatremia, treatment options depend on symptoms and total body water amount. In cases of hypervolemic conditions and absent or mild symptoms, it is suggested to decrease fluid intake and increase renal water excretion by loop diuretics such as furosemide. If patients appear symptomatic, serum sodium (Na+) must be recovered by hypertonic saline. Patients with hypovolemic hyponatremia need to be treated with isotonic or hypertonic saline on the basis of the severity of clinical features, as for hypotonic hyponatremia. Mild symptoms due to euvolemic hyponatremia can benefit from fluid restriction, but if the patient experiences severe or acute reduction of serum sodium concentrations it is important to administer hypertonic saline with or without furosemide. Moreover, pure glucocorticoid deficiency and hypothyroidism need specific hormone replacement. For patients affected by SIADH, vaptans represent a new class of drug antagonizing the V2 receptor on renal tubular cells. To date, two molecules are approved: conivaptan and tolvaptan. The prescription of conivaptan (intravenous use) has been authorized for euvolemic hyponatremia due to SIADH by the United States (US) Food and Drug Administration (FDA) but not by the European Medicines Agency (EMA); it has also been evaluated in patients with hypervolemic hyponatremia (mainly in patients with congestive heart failure (CHF)) but safety has not been established. 52 Oral tolvaptan is approved by the US FDA and the EMA for use in euvolemic hyponatremia due to SIADH with mild or moderate symptoms. The dose range varies from 15 to 60 mg/day and dosage changes need to be carefully evaluated by sodium concentration and plasma volume, at 24-h intervals. Patients should be monitored at recovery to avoid the risk of overcorrection. The drug must be discontinued if the serum sodium rises up to 135 mmol/l or the increase has been >5 mmol/l in the previous 24 h.9,53 Recent retrospective studies highlighted the role of tolvaptan in lung cancer patients with SIADH diagnosis. Petereit and colleagues, in a small monocentric study in SCLC patients, demonstrated its efficacy in increasing sodium concentration and consequently in performance status improvement and better chemotherapy adherence. 54 Tolvaptan treatment needs to be continued throughout the clinical management of lung cancer, due to the reversible effect of this drug when stopped. However, in some cases, SIADH resolves with tumor response to chemotherapy and with resolution of concomitant causes. Few literature data, deriving from case reports and retrospective studies, support the efficacy of urea for SIADH treatment, but its use is allowed in several guidelines37,46 and it is recommended as a second-line treatment in European guidelines.
Urea is an osmotic solute that induces renal fluid loss and decrease in urinary sodium excretion.46,55,56
Focus on hyponatremia in lung cancer patients
Hyponatremia is a well-known prognostic and predictive factor in cancer patients and it has a negative influence on performance status and hospitalization.6,15,17,25,27,29
In fact, Doshi and colleagues demonstrated a significant difference in length of hospital stay between cancer patients with hyponatremia (defined as <135 mEq/l; median of 10.2 days) and patients with eunatremia (median of 5.6 days; p < 0.01). 4 Similarly to Doshi and colleagues, our previous study conducted on 105 consecutive hospitalized cancer patients (28.6% lung adenocarcinoma) showed that hyponatremia (defined as ⩽134 mEq/l) increased the length (p = 0.0001) and the cost of hospitalization. In particular, the median number of days of hospitalization was different in moderate hyponatremia and severe hyponatremia (9 versus 21 days). 3
Furthermore, Abu Zeinah and colleagues showed a correlation between hyponatremia grade and risk of in-hospital mortality: considering 130 mEq/l as a cutoff, patients with moderate-to-severe hyponatremia had a 4.28-times higher risk of death than those with normal-to-mild hyponatremia (p < 0.05). 57
Moreover, hyponatremia affects performance status in different disease settings, including the palliative care one. 58
Most available data concern thoracic tumors, especially SCLC, in relation to high the frequency of SIADH.
In a recent prospective single-center study conducted by Wang and colleagues, the incidence of SIADH was 9.1% (35 patients of 385). 59 Hyponatremia was mainly severe (<125 mmol/l, 29/35 patients). They observed a significant difference in median progression-free survival (PFS) [6.7 versus 9.2 months, hazard ratio (HR): 0.610, p = 0.007] and median OS (11.6 versus 19.2 months, HR: 0.464, p = 0.000) between the SIADH group and control group. A further analysis regarding SIADH patients that recovered to normal serum sodium showed a median PFS similar to the control group.
In a retrospective study on 395 SCLC patients by Hermes and colleagues, the hyponatremia (<135 mmol/l) subgroup showed shorter median survival (9.0 versus 13.0 months, p < 0.001), although reduction in patients with extensive disease was not significant (9.0 versus 10.0 months, p = 0.135). 8
Castillo and colleagues analyzed 405 patients with NSCLC during chemotherapy treatment, 75.8% with ⩾1 hyponatremia episode (cutoff < 135 mEq/l), with significantly increased likelihood of death [HR 2.8, 95% confidence interval (CI) 2.0–3.9; p < 0.01]. 60
The prognostic role of hyponatremia has also been recognized in patients treated with targeted therapies. Svaton and colleagues showed a better response rate to erlotinib in NSCLC patients with normal serum sodium compared with patients with low serum sodium concentrations.61,62
In a retrospective surgical analysis assessing 386 patients with NSCLC, hyponatremia was found in 59.7% of patients (cutoff ⩽139 mEq/l). The study showed a significant prognostic role of low serum sodium concentration (p = 0.002). 63
Normalizing sodium concentration seems to improve survival in SCLC and NSCLC patients.
Petereit and colleagues, in a monocentric study with 2145 lung cancer patients, showed that median 2-year survival was 13.32 months in patients with correction of plasma sodium (>138 mmol/l) versus 5.16 months in patients with Na+ ⩽138 mmol/l (p = 0.007). 28
Patients with SIADH diagnosis improved their serum sodium concentrations if treated with tolvaptan but there are not enough available data about its effect on increasing survival.13,54,64
Therefore, sodium is considered an important factor for prognosis and survival in cancer patients.3,65
In our retrospective experience on a large series of NSCLC patients, the normalization of sodium concentration improved overall survival (OS) and PFS. 45
Similarly, Hansen and colleagues showed that normalizing hyponatremia has an impact on outcome in SCLC. 5
Conclusion
Hyponatremia is an emerging issue in cancer patients, especially those affected by lung cancer. Among different causes of hyponatremia, SIADH plays a central role due to its frequency especially in SCLC, but it should be suspected also in other tumors, such as NSCLC. In conclusion, this review pointed out the need to start the specific diagnostic-therapeutic algorithm early, to improve patients’ quality of life and compliance to anticancer treatments.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
Rossana Berardi has received consulting fees or honoraria from Otsuka (Otsuka Pharmaceutical Co., Japan).
The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.