
Abstract
Background:
More than one-third of hepatocellular carcinoma (HCC) patients are diagnosed at advanced stage with portal vein tumor thrombosis (PVTT) or extrahepatic metastasis. However, the outcomes of current therapeutic approaches are unsatisfactory. As a novel therapeutic strategy for unresectable HCC with PVTT, we analyzed the outcomes of transarterial infusion of epirubicin and cisplatin combined with systemic infusion of 5-fluorouracil (TAC-ECF) and compared its therapeutic effects and toxicity with transarterial chemoembolization (TACE) using doxorubicin (DOX).
Methods:
A total of 540 consecutive HCC patients who received TACE at the Catholic Medical Center between January 2007 and November 2013 were enrolled. Of these patients, we retrospectively analyzed 129 Barcelona clinic liver cancer stage C HCC patients with PVTT who received either TAC-ECF or TACE using DOX.
Results:
The objective tumor response rate was higher in the TAC-ECF group, with 31.3% objective response rate after TAC-ECF compared to 10% after DOX treatment (p = 0.004). Median follow-up period was 7 months (range, 1–57 months). The overall survival rate was also significantly higher in the TAC-ECF group compared to the DOX group (median 9.3 versus 4.6 months, p < 0.0001). Multivariate analysis revealed that TAC-ECF and extrahepatic metastasis were independent predictive factors for overall survival (p < 0.0001 and p = 0.002 respectively). No serious adverse effects developed in both groups.
Conclusions:
TAC-ECF therapy was tolerable and showed higher overall survival rate and tumor response compared to the conventional TACE DOX in advanced stage HCC patients with PVTT. Therefore, TAC-ECF may be considered as an effective treatment option for patients with unresectable HCC.
Introduction
Hepatocellular carcinoma (HCC) is a major health problem worldwide and is the sixth most common cancer and the third highest cause of cancer-related death. 1 The treatment options and prognosis of HCC have been mainly determined according to the tumor stage, liver dysfunction and performance status. Although several staging systems in different countries have been proposed for HCC, the Barcelona clinic liver cancer (BCLC) staging system has been generally accepted as a standard staging system for HCC. 2 Despite the surveillance programs that are performed in populations at high risk for HCC, many patients are still diagnosed at unresectable and advanced stages. 3 The patients who present with cancer symptoms and/or vascular invasion or extrahepatic spread are referred to as the advanced stage of HCC. 4 The prognosis of the patients who have advanced HCC with portal vein tumor thrombosis (PVTT) remains extremely poor, with a median survival of only 3 months if they are not treated.5,6 Furthermore, the presence of a tumor thrombus in the first branch (Vp3) or the main trunk (Vp4) of the portal vein can cause portal hypertension, which often leads to life-threatening complications including variceal bleeding, ascites and hepatic encephalopathy.7,8
As no standard therapeutic modality has been established for advanced HCC with PVTT, various therapeutic approaches have been proposed in an attempt to prolong survival of HCC patients with PVTT. They include transarterial chemoembolization (TACE), hepatic arterial infusion chemotherapy (HAIC), systemic chemotherapy and interdisciplinary treatment modality. 9 However, the results from previous studies are not strongly evident due to confounding factors and bias in retrospective cohort studies, as well as the limited number of enrolled patients. More recently, a phase II study of patients treated with yttrium-90 radioembolization (Y90RE) demonstrated that Y90RE is a safe and effective treatment in intermediate to advanced HCC, particularly in the case of PVTT. 10 However, as this trial included only a small number of patients with PVTT, larger prospective clinical trials to compare Y90RE with conventional treatments for advanced HCC with PVTT are warranted. Also, two phase III randomized clinical trials have demonstrated that sorafenib, an oral multikinase inhibitor that inhibits tumor cell proliferation and angiogenesis, 11 improves median overall survival in patients with advanced HCC.12,13 Based on these results, sorafenib has been widely accepted as a standard treatment for advanced HCC (BCLC stage C). However, in a recent phase II study, sorafenib did not show a survival benefit in hepatitis B-endemic Asian patients with HCC and PVTT. 14
TACE was not considered as an effective treatment modality for HCC patients until two recently conducted randomized controlled studies reported that TACE improved survival in patients with unresectable HCC.15,16 TACE is usually recommended for intermediate stage HCC according to the BCLC staging system, but in real-life clinical practice TACE is applied at various stages. Currently, for HCC patients with PVTT who have Child-Pugh A or B cirrhosis, the American Association for the Study of Liver Diseases (AASLD) 4 and the European Association for the Study of the Liver (EASL) guidelines 17 recommend sorafenib administration but not TACE, whereas the Asian Pacific Association for the Study of the Liver (APASL) guideline 18 suggests that TACE can be recommended for those patients. 19 However, TACE alone has not been sufficient to control unresectable HCC up to now.
To maximize the therapeutic efficacy of TACE for unresectable HCC, various approaches using different anti-cancer drugs or delivery systems have been conducted, which resulted in clinically favorable outcomes.20,21 We have previously reported that transarterial infusion of epirubicin and cisplatin combined with systemic infusion of 5-fluorouracil (5-FU) (TAC-ECF) was safe and effective for unresectable HCC. 22 However, there has been no report on the long-term follow-up results of this therapeutic approach for unresectable HCC with PVTT.
The present retrospective analysis of HCC patients with PVTT was done to evaluate the therapeutic efficacy of transarterial infusion of epirubicin and cisplatin combined with systemic infusion of 5-FU in comparison with conventional TACE using doxorubicin (DOX). We report here the survival rate and the prognostic factors of survival as well as the adverse effects of each regimen.
Materials and methods
Patients
A total of 540 consecutive HCC patients who received TACE at the Catholic Medical Center between January 2007 and November 2013 were enrolled. Patients without PVTT, those who were lost to follow up, patients with other tumor entities and those with missing data were excluded. A total of 129 (TAC-ECF, n = 67; DOX, n = 62) BCLC stage C HCC patients with PVTT were analyzed (Figure 1). All patients presented with Eastern Co-operative Group performance status (ECOG) 0–2 and the Child-Pugh score ⩽7. The treatment allocation was made at the patient’s request after the multidisciplinary team at our institution, which consists of four physicians and two intervention radiologists, agreed to perform TACE. Informed consent was obtained before the procedure for the inclusion in this study. The diagnosis of HCC was based on the histologic confirmation or typical radiologic findings on the dynamic computed tomography (CT) scan or magnetic resonance imaging (MRI) scan. Portal vein tumor thrombosis was defined as a low attenuation intraluminal filling defect in the portal vein that extended from the primary hepatic tumor on enhanced CT scan or MRI scan. This clinical study (KC15RISI0441) was approved by the institutional review board of the Catholic University of Korea.

Flow diagram for the patient selection process.
Therapeutic procedures
In both treatment groups, the catheter was inserted through the femoral artery. Hepatic arteriography was performed to detect the feeding arteries of the HCC and then the microcatheter was advanced into the feeding artery to selectively deliver the chemotherapeutic agents. In the DOX group, doxorubicin (50 mg) mixed with 2–10 ml of Lipiodol (Guerbet, Aulnay-sous-Bois, France) was transarterially infused followed by Gelfoam (Spongostan, Johnson & Johnson Medical, Gargrave, UK) embolization. Transcatheter arterial chemo-lipiodolization (TACL) without Gelfoam embolization was performed in cases of main portal vein tumor thrombosis. In the TAC-ECF group, the mixture of epirubicin (50 mg/m2), cisplatin (60 mg/m2) and 2–10 ml Lipiodol were transarterially infused. After TACL, 5-FU (200 mg/m2) was systemically infused for 12 h. The assessment of treatment response was done 1–2 months after each treatment with dynamic CT or MRI. The decision for additional treatment was made with the consideration of the size and the number of the remnant tumor, liver function and the patient’s general condition. When the decision was made for the patients to perform additional TACE, identical chemotherapeutic agents were used in both groups.
Treatment-related toxicities and dose modification of the chemotherapeutic agents
Treatment-related toxicities were assessed using the Common Terminology Criteria for Adverse Events (CTCAE, version 4.0). Also, the post-treatment deterioration of liver function was assessed by calculating the albumin-bilirubin (ALBI) grade before and after the procedure. 23 The toxicities were assessed for 1 week after each treatment and when the patient was admitted for subsequent treatment. The doses of the chemotherapeutic agents were reduced when treatment-related adverse events of more than G3 were encountered.
Assessment of treatment response
The tumor response was assessed by dynamic MRI scans, or dynamic CT scans when MRI was not available, 1–2 months after each treatment. Overall tumor response was defined as the best response since the first TAC-ECF or TACE DOX according to the modified Response Evaluation Criteria in Solid Tumors (mRECIST) criteria. 24 In terms of target lesion response, a complete response (CR) was defined as the disappearance of any intratumoral arterial enhancement in all target lesions. A partial response (PR) was defined as at least a 30% decrease in the sum of diameters of viable (enhancement in the arterial phase) target lesions. Progressive disease (PD) was defined as an increase of at least 20% in the sum of the diameters of viable (enhancing) target lesions. Stable disease (SD) was defined as any cases that do not qualify for either PR or PD. The objective response was defined as the sum of CR and PR.
Statistical analysis
Overall survival (OS) was estimated from the date of the first TAC-ECF or TACE DOX treatment to the date of death or last follow up. For the baseline characteristics analyses, the chi-square and Fisher’s exact tests were used for the comparison of categorical variables and Student’s t test for the continuous variables. Logistic regression analysis was used for the assessment of predictors for tumor response. The cumulative survival rates were calculated using the Kaplan–Meier method and the differences were analyzed using the log-rank test. The Cox proportional hazard model was used for the assessment of predictors for OS. Variables with p < 0.05 by univariate analysis were included for multivariate analysis and a p < 0.05 was considered statistically significant. All analyses described above were performed using SPSS version 18.0 software (SPSS Inc., Chicago, IL, USA).
Results
Baseline characteristics
Baseline characteristics of the patients are summarized in Table 1. There were 67 patients in the TAC-ECF group and 62 patients in the DOX group. The median follow-up period was 7 months (range, 1–57 months). The mean age of the patients was 56 ± 10.8 years; 81% were male and 85% had chronic hepatitis B. The mean diameter of the largest tumor was 10.9 ± 4.3 cm and 28% had extrahepatic metastasis at initial presentation. In terms of the degree of portal vein invasion, 12.4% of the patients showed main portal vein invasion, 57.4% first-order branch invasion and 30.2% second or third branch invasion. There was no difference in the age, sex, etiology, tumor size, number of tumors, degree of portal vein invasion, extrahepatic metastasis and alpha-fetoprotein (AFP) between the two groups.
Baseline characteristics.

Data are expressed as the number of patients, with percentages in parentheses.
AFP, alpha-fetoprotein; HBV, hepatitis B virus; HCV, hepatitis C virus; PV, portal vein.
Tumor response
Overall tumor response was defined as the best response since the first TAC-ECF or DOX. In the TAC-ECF group, CR was achieved in six patients (8.9%), PR in 15 patients (22.4%), SD in 27 patients (40.3%) and PD in 19 patients (28.4%). In the DOX group, CR was achieved in three patients (4.8%), PR in three patients (4.8%), SD in 23 patients (37.1%) and PD in 33 patients (53.2%). The objective response rate was significantly higher in the TAC-ECF group compared to the DOX group (31.3% versus 10.0%, p = 0.004) (Figure 2).
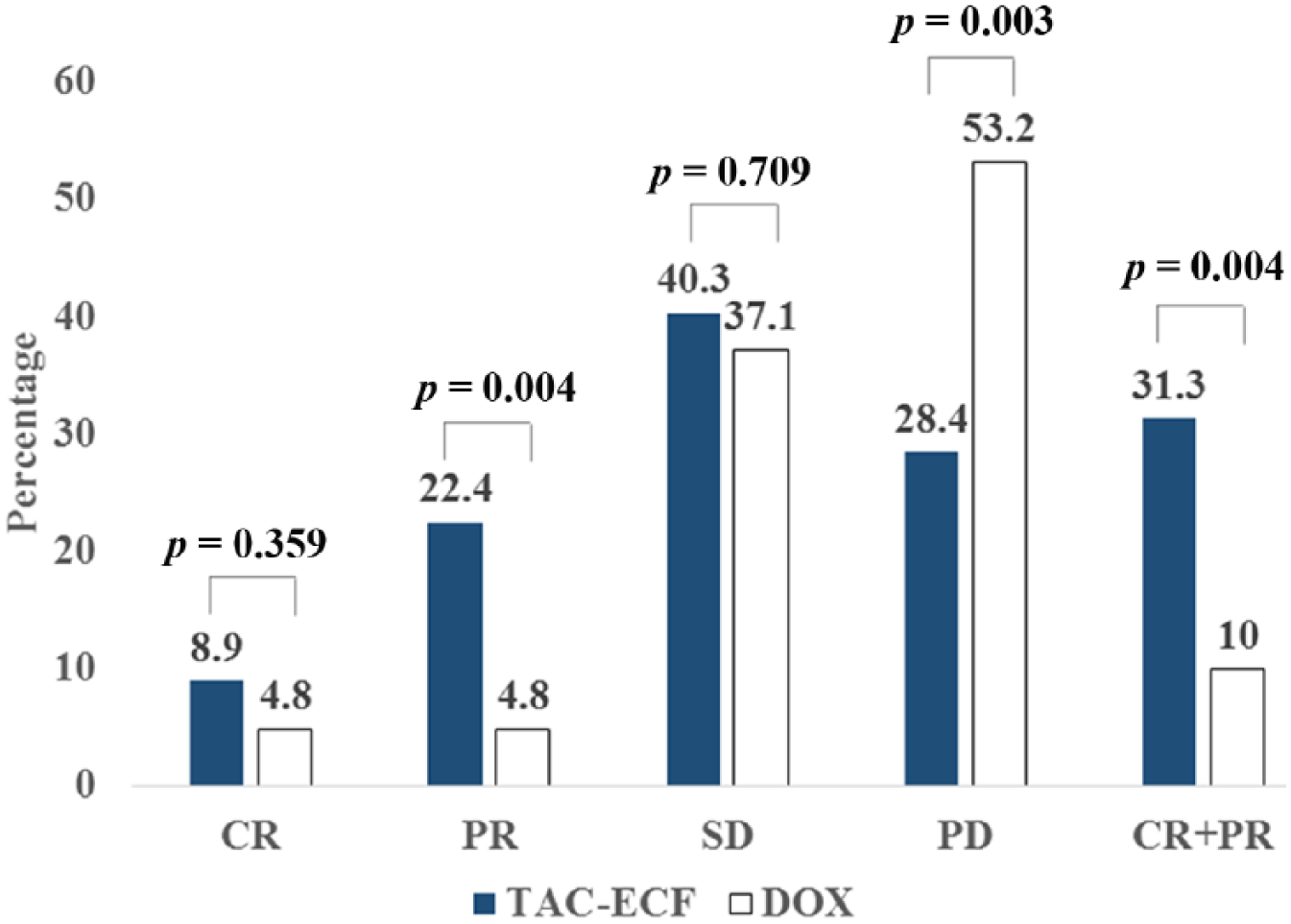
Tumor response. Treatment response was evaluated according to the mRECIST criteria. The objective tumor response rate, defined as the sum of complete and partial response, was significantly higher in the TAC-ECF group compared to the DOX group (p = 0.004).
Survival analysis and prognostic factors for survival
The OS rate was significantly higher in the TAC-ECF group compared to the DOX group (median 9.3 versus 4.6 months, p < 0.0001; Figure 3). The cumulative survival rates at 6, 12, 18 and 24 months was 69.7%, 38.7%, 29.4% and 24.6% in the TAC-ECF group and 39.7%, 16.8%, 12.6% and 2.1% in the DOX group, respectively. Univariate analysis showed that TAC-ECF [p < 0.0001, hazard ratio (HR) 2.383 (95% confidence interval (CI) 1.606–3.536)], tumor size [p = 0.032, HR 0.502 (95% CI 0.268–0.942)] and extrahepatic metastasis [p = 0.01, HR 1.703 (95% CI 1.136–2.553)] were the factors that influenced OS. Multivariate analysis revealed that TAC-ECF [p < 0.0001, HR 2.554 (95% CI 1.695–3.849)] and extrahepatic metastasis [p = 0.002, HR 1.948 (95% CI 1.277–2.972)] were the independent prognostic factors for OS (Table 2).

Overall survival rates. The median survival times in the TAC-ECF and DOX groups were 9.3 and 4.6 months, respectively. The overall survival rate was significantly higher in the TAC-ECF group compared to the DOX group (p < 0.0001).
Univariate and multivariate analysis of prognostic factors for survival.

Boldface values are statistically significant.
AFP, alpha-fetoprotein; CI, confidence interval; HBV, hepatitis B virus; HR, hazard ratio.
Treatment-related toxicity
The treatment-related toxicities of CTCAE grade ⩾2 are summarized in Table 3. The most common acute toxicities were liver enzyme elevations in both groups, with 30–40% of the patients experiencing more than a three-fold increase above the upper normal limit of aspartate aminotransferase (AST) or alanine aminotransferase (ALT). Post-embolization syndrome such as nausea, vomiting, abdominal pain and fever were frequently observed, but those exceeding grade 2 developed in fewer than 10% of the patients. There was no difference in the frequency of adverse events between the two groups. All treatment-related toxicities were either controllable with symptomatic management or regressed spontaneously. In the TAC-ECF group, treatment discontinuation developed in three patients before the infusion of 5-FU due to abdominal pain and liver enzyme elevation after the TACL. In these patients, doses of the chemotherapeutic agents were reduced in subsequent treatments and no serious treatment-related toxicity developed that required repeated interruption in the treatment. The post-treatment deterioration of liver function was also assessed by calculating the albumin-bilirubin (ALBI) grade before and after the procedure. The aggravation in the ALBI grade was observed in 13 patients (19.4%) in the TAC-ECF group and 13 patients (21.0%) in the DOX group, with no significant difference between the two groups (p = 0.460) (Table 4). No treatment-related death was observed in either group.
Treatment-related toxicity.
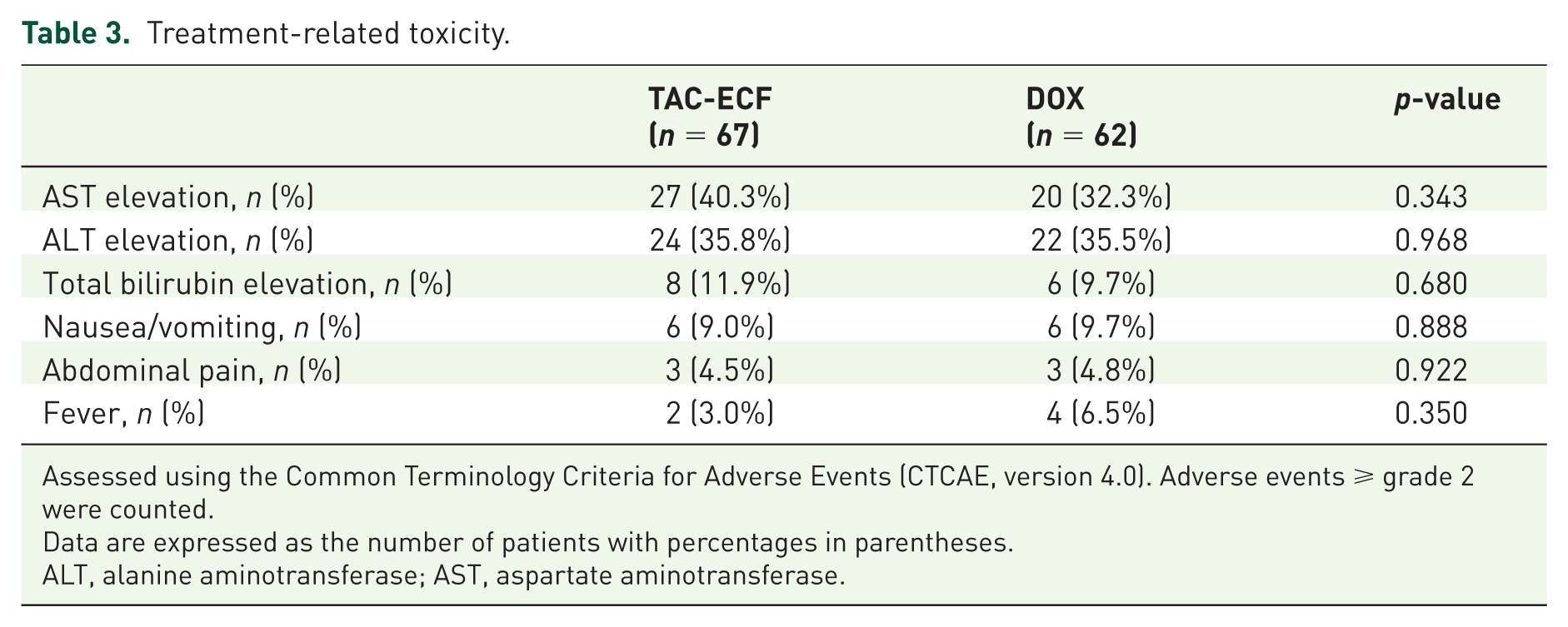
Assessed using the Common Terminology Criteria for Adverse Events (CTCAE, version 4.0). Adverse events ⩾ grade 2 were counted.
Data are expressed as the number of patients with percentages in parentheses.
ALT, alanine aminotransferase; AST, aspartate aminotransferase.
ALBI grades before and after treatments.
(a) ALBI grade before treatment.

(b) ALBI grade after treatment.

(c) Changes in the ALBI grade before and after treatment.

Abbreviations: ALBI, albumin-bilirubin.
Subsequent anti-cancer therapy
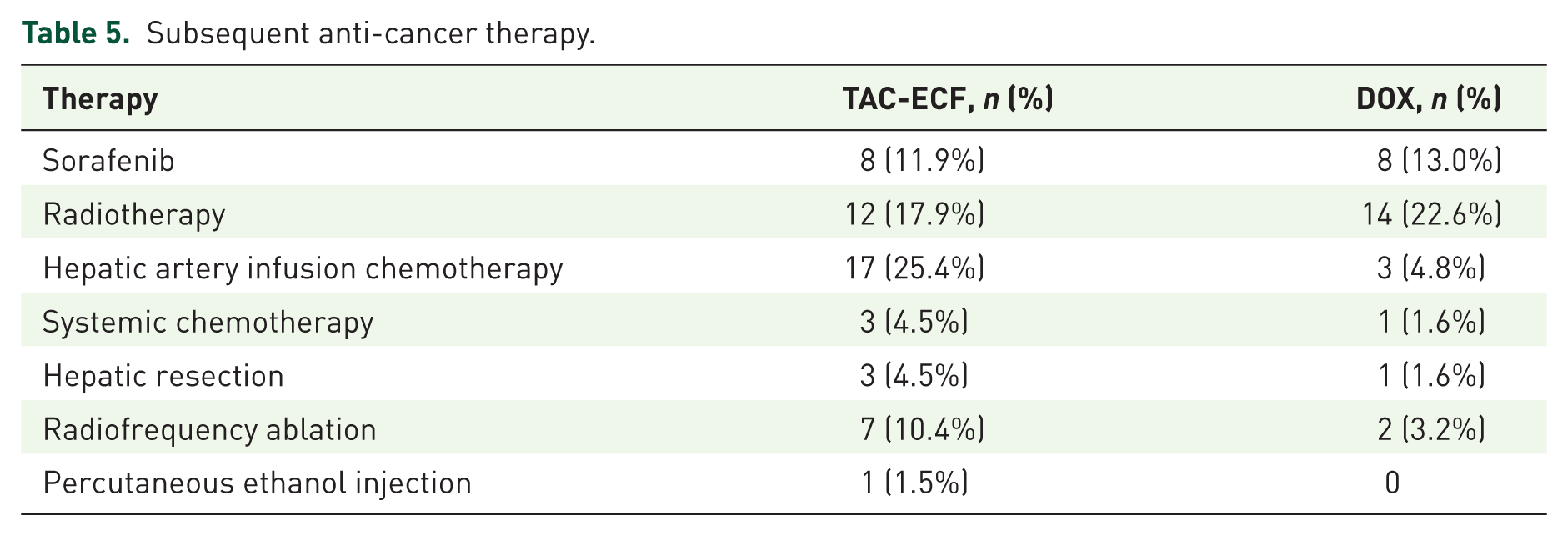
Thirty-seven patients (55.2%) in the TAC-ECF group and 28 patients (45.2%) in the DOX group received subsequent anti-cancer treatments (Table 5). In the TAC-ECF group, eight patients (11.9%) received sorafenib, 12 patients (17.9%) radiotherapy, 17 patients (25.4%) HAIC, three patients (4.5%) systemic chemotherapy, three patients (4.5%) hepatic resection, seven patients (10.4%) radiofrequency ablation (RFA) and one patient (1.5%) percutaneous ethanol injection (PEI). In the DOX group, eight patients (12.9%) received sorafenib, 14 patients (22.6%) radiotherapy, three patients (4.8%) HAIC, one patient (1.6%) systemic chemotherapy, one patient (1.6%) hepatic resection and two patients (3.2%) RFA.
Subsequent anti-cancer therapy.
Discussion
More than one-third of the HCC patients are diagnosed at advanced stage with PVTT or extrahepatic metastasis. 25 The BCLC guidelines recommend sorafenib for patients with advanced HCC, with approximately 3 months survival benefit shown in a multicenter randomized phase III trial.13,26 However, a recently reported multiregional cohort study with 18,031 patients from 14 countries worldwide revealed that TACE was the first recorded treatment in nearly 50% of the patients diagnosed as BCLC stage C in real clinical practice. 25 Therefore, the standard therapeutic option is yet to be established for HCC with PVTT in real clinical settings. Also, even in patients with extrahepatic metastasis, the importance of intrahepatic tumor control has been emphasized for prolonging survival when the intrahepatic tumor burden largely outweighs the extent of extrahepatic metastasis.27,28 In our data, the median survival of the 17 patients in the TAC-ECF group with extrahepatic metastasis was 9.3 months, which is identical to the OS time of the whole TAC-ECF group. This result may indicate the importance of intrahepatic tumor control and its influence on survival time in advanced HCC patients with PVTT, even in selected patients who present with extrahepatic metastasis.
The rationale for TACE in selected cases with PVTT is that the formation of collateral vessels around the portal vein and good liver function enable the patient to tolerate the treatment. 29 However, therapeutic approach with TACE for HCC with PVTT is challenging as the deterioration of the liver function after the treatment is more evident in cases of advanced tumors. 22 In addition, the presence of PVTT may aggravate portal hypertension, and complications such as ascites, variceal bleeding and hepatic encephalopathy are more likely to develop following embolization. The prognosis of patients diagnosed with advanced HCC is still very poor due to these limitations in treatment. Therefore, as a novel therapeutic approach for unresectable HCC with PVTT we performed and analyzed the effects and toxicity of TAC-ECF, a sequential TACL followed by systemic chemotherapy.
The combination regimen using epirubicin, cisplatin and 5-FU has shown clinical benefits in gastric, 30 biliary 31 and pancreatic cancers, 32 and the synergistic effects of cisplatin and 5-FU have been reported in animal models. 33 Also, the efficacy of epirubicin and cisplatin in TACE has been chronicled.34–37 We have previously reported the efficacy and safety of the TAC-ECF in large, extensive HCC with PVTT, which showed a 5.2 months survival benefit in comparison with conservative management 38 and the efficacy of TAC-ECF combined with PEI in unresectable HCC, which showed a survival benefit of 3 months compared to TACE using DOX. 22 However, there has been no report on the long-term follow-up results of this combination regimen versus conventional TACE using DOX for unresectable HCC with PVTT.
In our data, higher objective tumor response rate was observed in the TAC-ECF group compared to the DOX group. Although direct comparison of the tumor response was difficult due to the different baseline characteristics of each study, the objective tumor response of 31.3% after TAC-ECF was superior to that of sorafenib, which produced modest objective tumor response rates of 2–5% in two randomized trials and one large prospective study with unresectable HCC and PVTT.12,26,39 In the survival analysis, TAC-ECF showed median OS of 9.3 months, which was superior to the 4.6 months after conventional TACE using DOX. The OS of 9.3 months is comparable with the results from previous studies that compared TACE with other treatment modalities for HCC with PVTT. Pinter and colleagues 40 reported an OS of 9.2 months after TACE compared to 7.4 months after sorafenib, and Luo and colleagues 41 reported on OS of 7.1 months after TACE compared to 4.1 months after conservative care. Also, recently reported studies for the treatment of HCC with PVTT have suggested the median OS of 5.5–10.2 months after HAIC, sorafenib, Y90RE, surgery and HAIC combined with three-dimensional conformal radiotherapy.12,42–46 Multivariate analysis of our data revealed that TAC-ECF was the significant independent prognostic factor for patient survival and objective tumor response. From these results, TAC-ECF may be considered as an effective treatment option for unresectable HCC with PVTT.
The tumor response rate was low in the DOX group. We speculated that low response was observed because 72.6% of the patients presented with PVTT of either Vp3 or Vp4. In these patients, only the superselective TACE should be performed with caution by a very experienced interventional radiologist as nonselective embolization could result in a significant deterioration of liver function or even hepatic failure. In a previous study of TACE for primary HCC at high risk, patients with nonselective lobar embolization had a much higher mortality (16.6%; p = 0.03) than patients who underwent selective segmental TACE. 47 However, in patients with large, multiple tumors and major PVTT, like in this study with 93.5% of the patients with tumor size >5 cm and 67.7% of the patients with multiple tumors in the DOX group, it is often difficult to perform multiple superselective embolizations sufficient to achieve an objective response. In this regard, recently published articles have reported objective response rates of 0% to ~10.5% after TACE in HCC patients with PVTT.48,49 The TAC-ECF regimen in our study was a novel therapeutic attempt to reduce the aggravation of liver function due to vigorous embolization but to maintain a substantial embolic effect with lipiodolization in patients with PVTT. Also, the relative preservation of liver function after TAC-ECF enabled the patient to receive higher chemotherapeutic doses compared to the DOX group which may have resulted in more clinical benefits.
Toxicities were tolerable in most patients, without treatment-related deaths. Treatment discontinuation developed in three patients in the TAC-ECF group after TACL, but after dose reduction of the chemotherapeutic agents no serious treatment-related toxicity developed in subsequent treatments that required discontinuation. The most common acute toxicities were liver enzyme elevations, which developed in 30–40% of the patients in the TAC-ECF group but without significant difference between the two groups. The relatively higher rate of liver enzyme elevations compared to other adverse events in this study may have been related to the advanced nature of the tumors. Taking into account that the deterioration of the liver function may develop more frequently in advanced tumors 22 and that embolization may incur greater ischemic injury, it is our opinion that in advanced HCC with PVTT, it may be safer to perform transarterial therapy only in patients with preserved liver function and without embolization.
We also analyzed post-treatment complications in the 16 patients who presented with main PVTT. Liver failure or treatment-related death were not observed in any cases. However, seven patients (43.8%; four in the TAC-ECF group and three in the DOX group) experienced an increase in the serum bilirubin level exceeding 1.5 times the upper normal limit. Such elevation in bilirubin developed in a greater proportion of patients with main PVTT compared to the patients without (43.8% versus 6.2%). Therefore the deterioration of liver function was greater in the patients with main PVTT but without decompensation.
The additional advantages of the TAC-ECF compared to other therapeutic modalities for advanced HCC are that, unlike HAIC, there is no need to keep an implanted port that poses the risk of infection, and that there is not much difference in the treatment cost compared to conventional TACE, not to mention the high-priced yttrium-90 or sorafenib.
The limitation of this study was that it was a retrospective study without randomization. There may have been potential selection bias. However, the baseline characteristics of the patients in the two groups showed no significant difference. Also, there was no comparison between the treatment group with the best supportive care group, but in our previous report we showed survival benefit of the TAC-ECF in large, extensive HCCs with PVTT in comparison with conservative management. 38
In conclusion, TAC-ECF was tolerable and showed higher OS rate and tumor response compared to TACE using doxorubicin in advanced stage HCC patients with PVTT. Therefore, TAC-ECF may be considered as an effective treatment option for patients with unresectable HCC and PVTT. Future large-scale randomized controlled study in comparison with therapeutic strategies such as HAIC, sorafenib and Y90RE in advanced HCC is required to properly evaluate the efficacy of the TAC-ECF.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.