
Abstract
Purpose:
To investigate the association between metabolic syndrome and prostate cancer risk in Turkish men.
Methods:
We examined data from 220 patients with prostate cancer and 234 men in a control group with benign biopsy results, who had a serum prostate-specific antigen (PSA) level ⩾ 4 ng/ml, or an abnormal digital rectal examination finding and who underwent transrectal ultrasound-guided prostate biopsy at two main training and research hospitals between February 2009 and April 2013. Metabolic syndrome was diagnosed according to The Society of Endocrinology and Metabolism of Turkey metabolic-syndrome criteria. Age, total PSA, waist circumference, body mass index, lipid profiles, fasting blood sugar level, blood pressure level and metabolic syndrome were considered for analysis.
Results:
A total of 454 patients were enrolled: 85 cases in group 1 (38.6% of 220 prostate cancer cases) and 104 control subjects in group 2 (40.4% of 234 controls) were diagnosed with metabolic syndrome. Higher ages and lower high-density lipoprotein-cholesterol were two parameters that were significant only in the prostate cancer group with metabolic syndrome. There was no significant predictor factor for prostate cancer alone; however, higher triglycerides (odds ratio [OR], 1.286; 95% confidence interval [CI] 1.09–1.82 and 1.142; 95% CI 1.06–1.62) and fasting glucose levels (OR, 1.222; 95% CI 1.08–1.61 and 1.024; 95% CI 1.07–1.82) were significant predictors in both the prostate cancer group and control group.
Conclusions:
We found little evidence to support the hypothesis that increased incidence of metabolic syndrome (or its components) contributes to increased incidence of prostate cancer. A larger, prospective, multicentre investigation is mandatory to confirm if there is any relationship between metabolic syndrome and prostate cancer.
Introduction
Prostate cancer is one of the most commonly diagnosed malignancies in men and the second leading cause of cancer-related death worldwide. In Europe 2.6 million new cases are diagnosed each year and prostate cancer accounts for 9% of all cancer deaths among men within European countries [Mistry et al. 2007]. The first epidemiological study in Turkey was conducted in İzmir and colleagues reported that prostate cancer is the fifth most common cancer after lung, colon, bladder and nonmelanoma skin cancers [Zorlu et al. 2004]. However, the Prostate Cancer Incidence Study, conducted between July 2008 and June 2009, in 12 provinces in Turkey gives the most up-to-date information. Preliminary results showed that prostate cancer has increased significantly and was ranked in second place after lung cancer [Zorlu, 2009]. An aging population and westernization of diet (such as higher intakes of dietary fat, meat and excessive calories) are contributing factors for prostate cancer [Kheterpal et al. 2013].
Metabolic syndrome includes glucose intolerance, dyslipidaemia, hypertension and obesity [Kassi et al. 2011]. Its incidence is increasing in Turkey as it is all around the world [Onat and Sansoy, 2002]. Although there is a hypothesis for a role of metabolic syndrome in the etiology of prostate cancer, the epidemiological evidence is insufficient to confirm this [Laukkanen et al. 2004]. There are few studies that contain all components of metabolic syndrome. Most previous studies on the relationship between metabolic syndrome and prostate cancer were conducted in multiracial groups or non-Turkish populations. In this study, we investigated whether or not there is a relationship between metabolic syndrome and prostate cancer in Turkish men.
Patients and methods
We reviewed the records of 502 patients who were admitted to outpatient clinics with a serum prostate-specific antigen (PSA) level ⩾ 4 ng/ml, or an abnormal digital rectal examination finding, and who underwent transrectal ultrasound-guided prostate biopsy at two main training and research hospitals between February 2009 and April 2013. Patients taking 5-alpha reductase inhibitors, those with a history of prostate cancer or prostatic surgery, or whose data were insufficient for analysis were excluded. There were 202 patients with prostate cancer (allocated to group 1, prostate cancer patients) and 234 men with benign biopsy results (group 2, control group). All patients received a physical examination including measurement of height, weight and waist circumference (2 cm above the umbilicus). Body mass index (BMI) was computed according to the Quetelet index: weight/height2 (kg/m2). The indicator of metabolic syndrome was defined according to The Society of Endocrinology and Metabolism of Turkey metabolic-syndrome diagnostic criteria (2005) as the presence of at least one component from among the following: diabetes mellitus or impaired glucose tolerance or glucose resistance and at least two components from among following: high blood pressure (130/85 mmHg) or use of antihypertensive drugs, dyslipidaemia (triglyceridemia [1.7 mmol/L] or reduced high-density lipoprotein (HDL)-cholesterol [< 1.0 mmol/L]), or abdominal obesity (abdomen circumference > 94 cm or BMI > 30 kg/m2) [Arslan et al. 2009]. Patients and controls were subdivided into two groups according to the presence of metabolic syndrome. The study was approved by institutional review board and ethics committee.
Statistical analysis
All statistical analyses were performed using SPSS version 16.5 (Statistical Package for Social Sciences for Windows 16.5 Inc., Chicago, II, USA). All values were expressed as mean ± standard error. The variables were investigated using visual (histograms probability plots) and analytical methods (Kolmogorov–Smirnov test) to determine whether or not they were normally distributed. Descriptive statistics were reported as the mean or median with standard deviation. Unpaired student’s t-tests were performed for data with normal distribution. For parameters that did not show normal distribution, the nonparametric Mann–Whitney U test was used to compare them. Between-groups analyses were performed using the chi-square test. Cox regression analysis was used in the analysis of time-to-event variable and the 95% confidence interval (CI) was selected; a p value of 0.05 was set for statistical significance.
Results
Table 1 shows 85 cases in group 1 (prostate cancer cases) and 104 controls in group 2 were diagnosed with metabolic syndrome according to the metabolic-syndrome diagnostic criteria. Baseline characteristics of the prostate cancer cases and controls are presented in Table 2. The mean age for metabolic-syndrome patients was 70.25 ± 7.02 years and for metabolic- syndrome controls 69.73 ± 7.20 years. The total PSA (tPSA) for metabolic-syndrome patients was 43.32 ± 97.40 ng/ml versus 8.25 ± 11.25 ng/ml in the metabolic-syndrome control group. Waist circumference was 101.67 ± 4.80 cm in group 1 metabolic-syndrome patients versus 102.09 ± 4.38 cm in group 2 metabolic-syndrome controls. BMI was 27.77 ± 2.85 kg/m2 in group 1 metabolic-syndrome patient versus 28.04 ± 2.82 kg/m2 in group 2 with metabolic syndrome. There was no significant difference in tPSA, low-density lipoprotein (LDL)-cholesterol and total cholesterol in group 1 and age, tPSA, LDL-cholesterol, HDL-cholesterol and total cholesterol in group 2 between the groups with and without metabolic syndrome. Group 1 patients and group 2 controls with metabolic syndrome had higher fasting glucose, triglyceride, hypertension (or use of antihypertensive), BMI and waist circumference than the patients/controls without metabolic syndrome. Higher ages and lower HDL-cholesterol were two parameters that were significant only in group 1 patients with metabolic syndrome. In the logistic regression analysis, higher triglycerides (odds ratio [OR], 1.286; 95% CI 1.09–1.82 and 1.142; 95% CI 1.06–1.62) and fasting glucose (OR, 1.222; 95% CI 1.08–1.61 and 1.024; 95% CI 1.07–1.82) were significant predictors both in prostate cancer and control groups. There was no significant predictor factor for prostate cancer to differentiate it from the control group. However age, the presence of metabolic syndrome, BMI, hypertension and low-HDL were not significantly related to increasing prostate cancer risk (Table 3).
Patients and controls with presence of metabolic syndrome.

Characteristics of 220 prostate cancer patients and 234 controls according to the presence of metabolic syndrome.
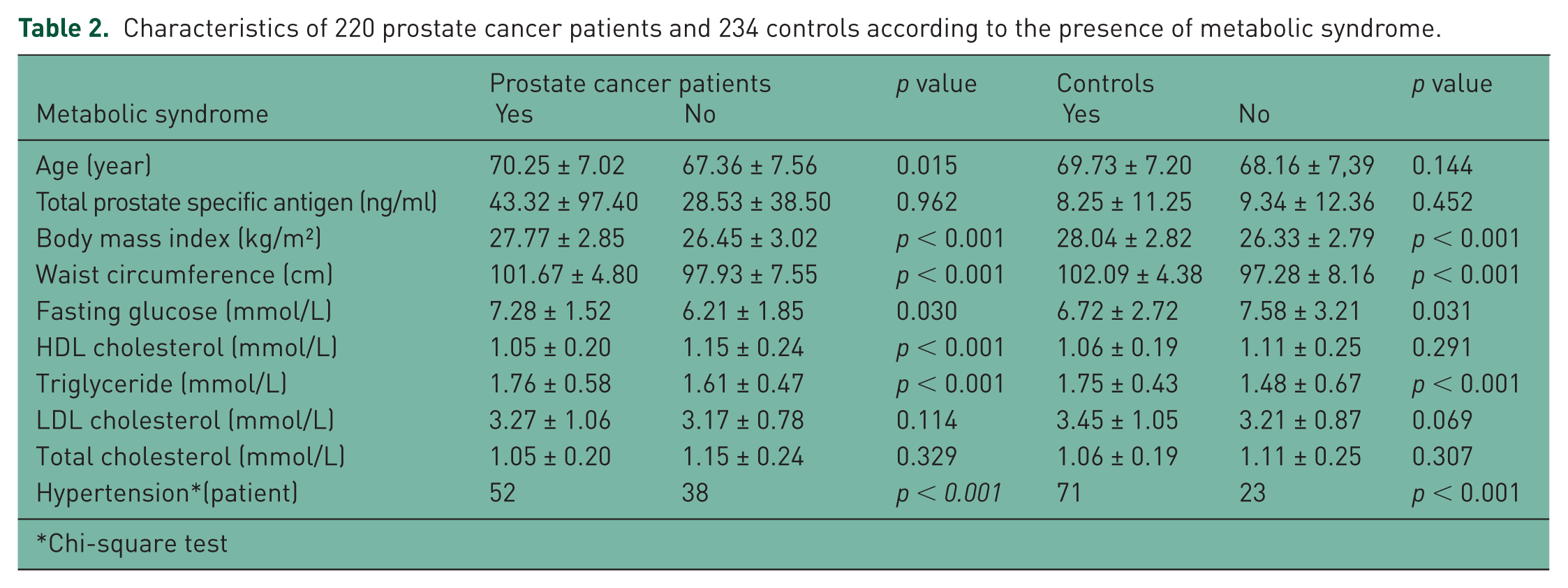
Chi-square test
Odds ratio and 95% confidence intervals for prostate cancer patients and controls with specific features of metabolic syndrome.
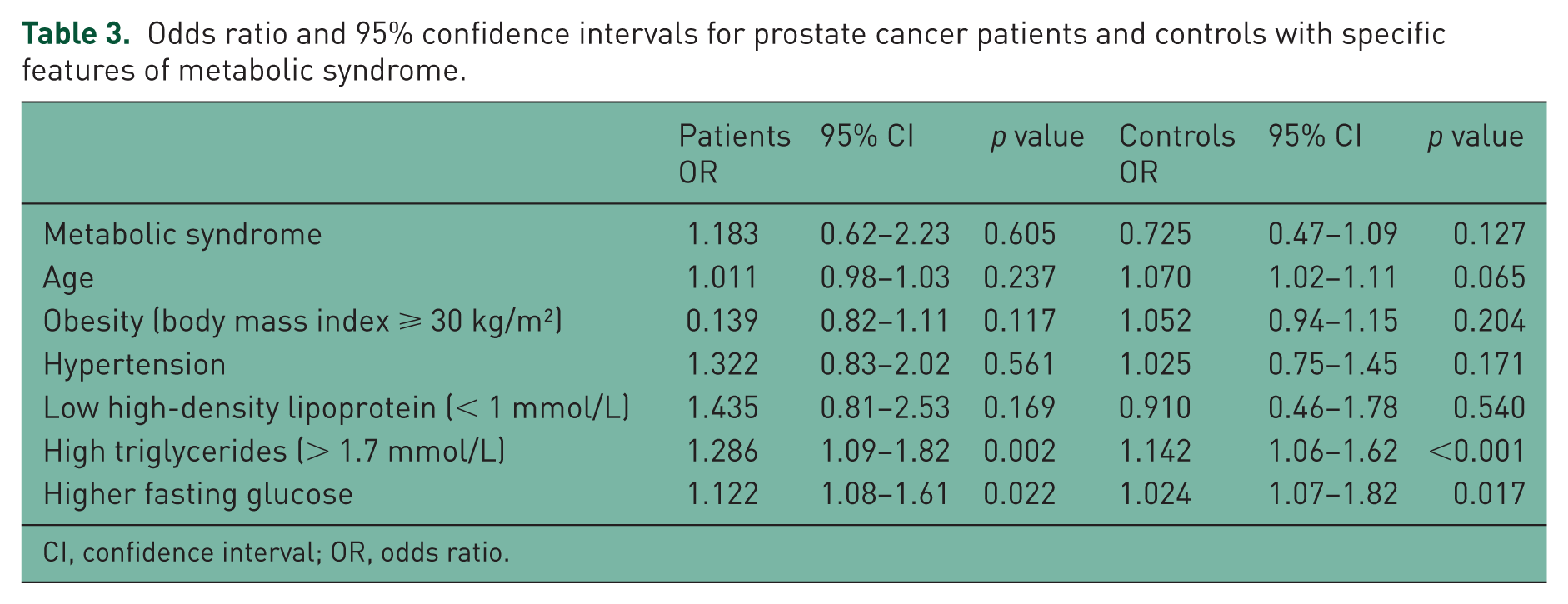
CI, confidence interval; OR, odds ratio.
Discussion
Metabolic syndrome is related to cardiovascular disease or type II diabetes; however, the relationship between metabolic syndrome and malignancy is unclear. It has been reported that incidence and mortality rates of colon cancer, endometrial cancer and breast cancer are associated with components of metabolic syndrome such as obesity and insulin resistance [Kassi et al. 2011]. In this study, we evaluated the association between metabolic syndrome parameters and blood-lipid profiles in patients with prostate cancer and controls. We found that prostate cancer patients with metabolic syndrome have higher age and lower HDL-cholesterol. Higher fasting glucose, triglyceride, hypertension (or use of an antihypertensive drug), BMI and waist circumference were higher in metabolic-syndrome patients – both in the prostate cancer group and the control group than in patients and controls without metabolic syndrome. tPSA, LDL-cholesterol and total cholesterol were not significant in both groups with metabolic syndrome and without metabolic syndrome. Similar findings were presented by Farwell and colleagues, who described a statistically significant association between HDL-cholesterol and low-grade prostate cancer, whereas for high-grade prostate cancer the association did not reach statistical difference [Farwell et al. 2011]. Hammarsten and Högstedt evaluated features of metabolic syndrome among 299 patients recently diagnosed with prostate cancer. Subjects with poorly differentiated prostate cancer had lower HDL-cholesterol levels and higher triglyceride levels compared with those with well-differentiated disease [Hammersten and Högstedt, 2004]. A hospital-based, case-control study found a statistically significant association between low levels of HDL-cholesterol and total prostate cancer risk. Large prospective studies, however, did not confirm an association between HDL-cholesterol and localized, advanced and total prostate cancer risk [Martin et al. 2009; Ahn et al. 2009; De Nunzio et al. 2012]. On the contrary, Tande and colleagues reported an inverse association. In their study in a large cohort of the Atherosclerosis Risk in Communities Study, men with metabolic syndrome showed a 23% reduction in risk of prostate cancer. They hypothesized that this finding reflects a decrease in bioavailable testosterone with metabolic syndrome and a concomitant reduction in prostate cancer risk [Tande et al. 2006; McGrowder et al. 2012].
Our results for BMI are in keeping with previous findings in large studies, and support the hypothesis that a high BMI is not related to prostate cancer risk [Häggström et al. 2012]. For blood pressure, the findings of what to our knowledge is the largest previous study indicated a nonsignificant association with prostate cancer death, whereas smaller studies reported a null association [Jeon et al. 2012]. No association with risk was found for high levels of glucose, cholesterol and triglycerides, which is in keeping with the majority of previous reports, with the exception of some studies. Similar to our study, Van Hemelrijck and colleagues found a positive association between high levels of triglycerides and pCa risk in men with high glucose levels, other investigators have found no relation between high triglycerides and pCa risk [Hemelrijck et al. 2011]. However in our study, higher triglycerides and fasting glucose were significant predictors in both in the prostate cancer group and the control group. In an Italian study, the number of factors contributing to metabolic syndrome was significantly associated with the development of prostate cancer and men with metabolic syndrome had a 66% higher risk compared with those without metabolic syndrome [Pelucchi et al. 2011]. Some studies have shown an association of metabolic syndrome with a higher risk of prostate cancer, the results are still inconclusive [Zadra et al. 2010]. However, there is clear evidence that tumours detected in men with metabolic syndrome are more aggressive than those detected in men without metabolic syndrome [Morote et al. 2013]. In our study, one of the main limitations was that we did not evaluate the presence of an association between higher grade/stage and more aggressive disease in metabolic-syndrome patients.
In addition, our study did not permit extensive analyses because of the relatively small number of controls with unreachable lack of information, which is the major limitation of a retrospective review. Another limitation of our study was that details of the specific diabetic medications were not collected from the participants. This could be an important confounding variable, since metformin has been associated with a lower risk of cancer [Libby et al. 2009; Noto et al. 2012]. We were unable to assess the effect of such use of diabetic medications, which could be an important aspect of evaluating metabolic syndrome and cancer risk in future studies to confirm the exact role of cholesterol and other blood lipids in the development and progression of prostate cancer.
In conclusion, we found little evidence to support the hypothesis that metabolic syndrome or its components can explain any association between metabolic syndrome and prostate cancer. Furthermore, our results suggest that different fractions of cholesterol are involved in metabolic-syndrome patients both in the prostate cancer group and controls. The association between the different fractions of cholesterol and prostate cancer needs to be confirmed in larger, prospective studies.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.