
Abstract
The intravenous nitrogen-containing bisphosphonate zoledronic acid has been shown to block multiple steps in tumor metastasis (e.g. angiogenesis, invasion, adhesion, proliferation) in preclinical and translational studies. Moreover, clinical data from the ABCSG-12 and ZO-FAST trials demonstrate significantly improved disease-free survival with zoledronic acid in the adjuvant breast cancer setting. In contrast to these two trials, recent interim results from the AZURE trial do not show a benefit from adding zoledronic acid to adjuvant therapy in the overall patient population. However, subset analyses of AZURE data show that zoledronic acid significantly improved overall survival in women who were more than 5 years postmenopausal or older than 60 years at baseline. Similarly, subset analyses of the ABCSG-12 trial data demonstrate greater benefits from zoledronic acid treatment in patients who theoretically would have achieved more complete ovarian suppression. These observations, together with the AZURE postmenopausal data, suggest that the endocrine environment may affect the potential anticancer activity of zoledronic acid. Indeed, current data support the possibility that zoledronic acid might be most effective for improving disease-free survival in the adjuvant breast cancer setting in women who are postmenopausal or have endocrine therapy-induced menopause.
Introduction
Breast cancer is the leading cause of cancer deaths and the most common cancer in women, with an estimated 1.4 million new cases diagnosed each year [American Cancer Society, 2011]. Indeed, in some Western countries (e.g. USA and UK) as many as one in eight women are at risk of developing breast cancer during their lifetime [Coleman, 2009]. Locoregional or distant relapse remains a challenge, even in patients with no evidence of residual disease after surgical resection and adjuvant therapy. Bone is a common site of recurrence in patients with breast cancer, up to 80% of patients with metastatic disease developing bone lesions [Coleman, 2009]. The bone marrow is highly vascularized and a source of numerous growth factors, cytokines, and other signaling molecules that support the hematopoietic niche. This environment, together with specialized cell–cell interactions designed to protect pluripotent hematopoietic stem cells against immune activity or other attacks, can function as an inadvertent sanctuary for cancer cells. Consequently, the bone microenvironment may act as a shield against chemotherapeutic agents, thereby promoting cancer cell survival and tumor growth [Meads et al. 2008; Shiozawa et al. 2008].
Bone integrity is maintained by the balanced and coupled processes of osteolysis and osteogenesis, which are regulated by a variety of local and systemic factors. Osteolysis results in the release of bone matrix-bound growth factors that can support cancer cell growth in the bone. Active bone remodeling also can release growth factors, enzymes, and other signaling molecules that support cancer cell proliferation and metastasis [Mundy, 2002]. In addition to seeding skeletal metastases, cancer cells surviving in the bone microenvironment can travel in the circulation to seed metastases at other distant sites, as well as serve as a source of local recurrences (a phenomenon termed ‘tumor self-seeding’) [Kim et al. 2009; Norton and Massague, 2006; Mundy, 2002].
The general consensus for the treatment of early breast cancer is surgical resection and systemic therapy, which includes chemotherapy, radiation therapy, and targeted treatment as appropriate, together with long-term endocrine therapy for hormone-responsive breast cancer [Goldhirsch et al. 2009]. Most adjuvant therapies for breast cancer, which have led to an increase in disease-free survival (DFS), directly or indirectly decrease estrogen levels. For example, chemotherapy can cause ovarian failure and early menopause [Shapiro et al. 2001], and ovarian suppression with a luteinizing hormone-releasing hormone (LHRH) agonist (e.g. goserelin, used in premenopausal patients with breast cancer) results in rapid decrease in circulating estrogens to postmenopausal levels for the duration of treatment [Goldhirsch et al. 2009]. In postmenopausal women with hormone-responsive breast cancer, aromatase inhibitors are established as the treatment of choice [Goldhirsch et al. 2009]. By inhibiting the aromatization of estradiol precursors in peripheral tissues, aromatase inhibitors reduce circulating estrogens to levels substantially lower than those observed after natural menopause [Dixon et al. 2008]. Thus, both chemotherapy and endocrine therapy can substantially reduce estrogen levels in women with breast cancer.
Because of the integral role estrogen plays in maintaining skeletal homeostasis, these decreased estrogen levels are associated with elevated rates of osteolysis and the resulting bone loss. It is important to note that these elevations in osteolysis are more rapid and profound than those during physiologic processes (e.g. normal aging and menopause) [Hadji, 2009]. In addition, changes in cytokines and hormones other than estrogen also affect bone physiology and lead to bone loss during menopause [Nicks et al. 2010; Pino et al. 2010; Perrien et al. 2006; Bismar et al. 1995]. Some of these factors (e.g. cytokines such as tumor necrosis factor-α and interleukin-6, and hormones such as inhibins) [Nicks et al. 2010; Pino et al. 2010; Perrien et al. 2006; Bismar et al. 1995] also might have an impact on breast cancer metastasis to bone. Indeed, correlative studies suggest that women with breast cancer and elevated rates of osteolysis are at higher risk of bone metastases compared with women with normal levels of osteolysis [Lipton et al. 2009]. A bone-targeted antiresorptive agent may therefore be of use as a potential anticancer agent in the adjuvant breast cancer setting. A wealth of preclinical data and clinical evidence, combined with its targeting to and storage in bone, make the antiresorptive agent zoledronic acid an attractive agent for investigation in this setting. Indeed, preclinical, translational, and clinical studies with zoledronic acid have demonstrated potential anticancer activity and improved outcomes in patients with early breast cancer [Green and Guenther, 2011; Gnant et al. 2011a; de Boer et al. 2010; Coleman et al. 2010a; Winter et al. 2008].
Zoledronic acid
Bisphosphonates are antiresorptive agents that inhibit osteoclast-mediated bone resorption [Russell, 2007; Mundy, 2002]. As a class, bisphosphonates attach to the mineralized bone matrix and are ingested by osteoclasts during osteolysis, thereby inhibiting osteoclast-mediated bone resorption. Being a nitrogen-containing bisphosphonate, zoledronic acid also inhibits the activity of farnesyl diphosphate synthase, a key enzyme in the mevalonate pathway [Russell, 2007; Kavanagh et al. 2006], resulting in reduced cellular activity, proliferation, and viability of cells that ingest this agent (e.g. osteoclasts actively resorbing bone, and cancer cells) [Winter et al. 2008; Russell, 2007].
The potential anticancer activity of zoledronic acid may be mediated through its effects on the bone marrow microenvironment. It has been postulated that zoledronic acid may impede the development of bone metastases by rendering the bone microenvironment less conducive to cancer cell survival and proliferation [Green and Guenther, 2011; Winter et al. 2008]. In addition to the effects of zoledronic acid on the bone microenvironment, preclinical evidence suggests that zoledronic acid treatment also may interfere directly or indirectly with other processes in cancer progression and tumor growth [Benzaid et al. 2011; Gallo et al. 2011; Green and Guenther, 2011; Stresing et al. 2011; Winter et al. 2008]. Indirect mechanisms of zoledronic acid-mediated anticancer activity include activating anticancer immune responses, inhibiting angiogenesis, and inhibiting interactions with mesenchymal stem cells [Benzaid et al. 2011; Gallo et al. 2011; Stresing et al. 2011]. These activities can have ramifications that extend beyond the development of bone metastases. For example, inhibiting the interaction between mesenchymal stem cells and cancer cells can have profound inhibitory effects on cancer cell invasion and migration [Liu et al. 2011; Suzuki et al. 2011], which might inhibit metastasis at skeletal and extraskeletal sites.
Direct anticancer effects of zoledronic acid include inhibiting cancer cell growth and survival and potential synergy with anticancer therapies [Green and Guenther, 2011; Neville-Webbe et al. 2010; Ottewell et al. 2010, 2008; Winter et al. 2008]. Furthermore, translational studies have shown that zoledronic acid can induce an anticancer immune response, decrease the persistence and number of disseminated tumor cells in bone marrow, and reduce the circulating levels of angiogenic growth factors [Aft et al. 2010; Rack et al. 2010; Santini et al. 2009; Lin et al. 2008; Solomayer et al. 2008; Santini et al. 2007]. Given the complexity of the process of metastasis from solid tumors, it is likely that a variety of the anticancer mechanisms of action demonstrated in preclinical and translational studies may contribute to the observed clinical anticancer benefits of zoledronic acid both in and outside of bone.
Is the potential anticancer activity of zoledronic acid greatest in a low-estrogen environment?
Zoledronic acid in three large phase III clinical trials in patients receiving adjuvant therapy for early breast cancer.
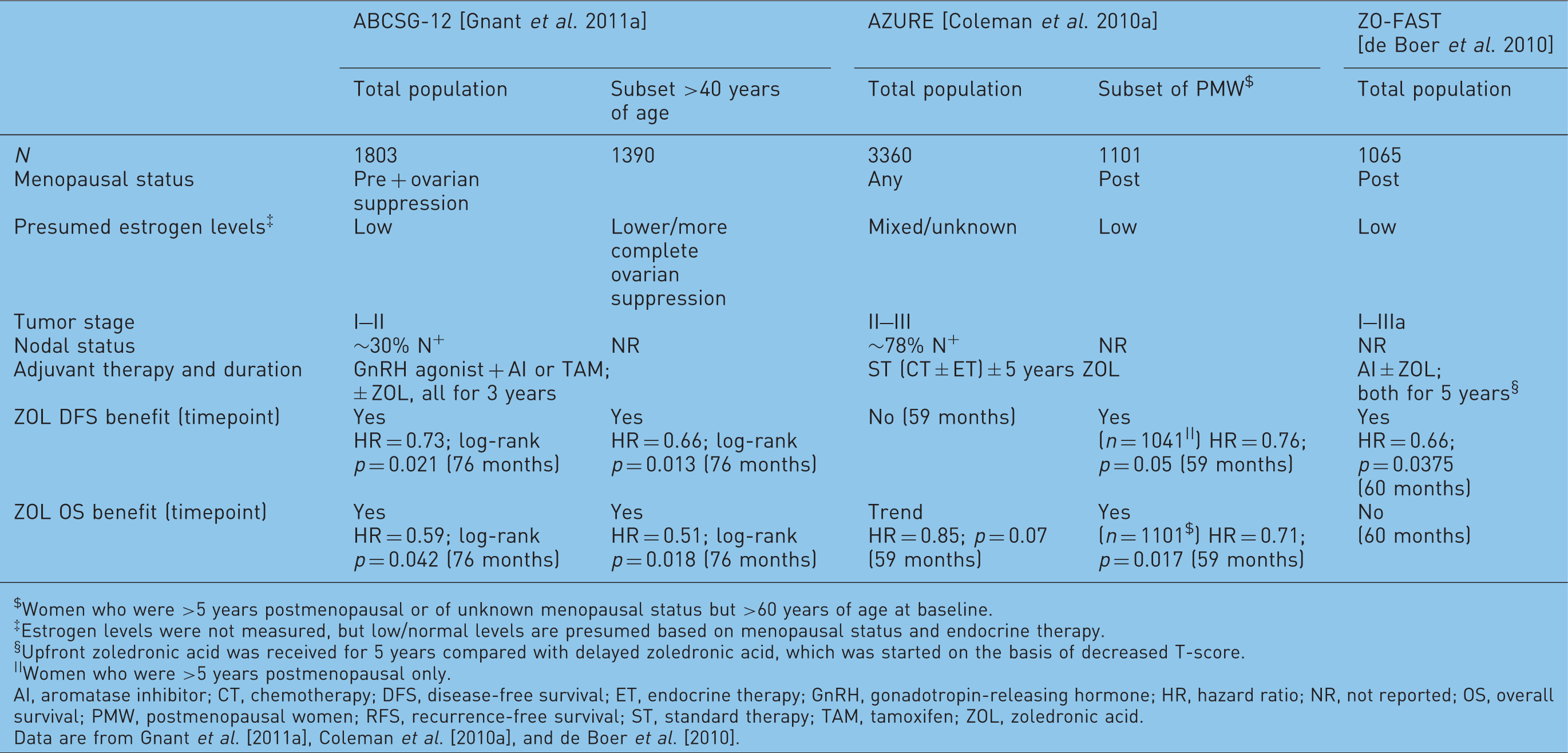
Women who were >5 years postmenopausal or of unknown menopausal status but >60 years of age at baseline.
Estrogen levels were not measured, but low/normal levels are presumed based on menopausal status and endocrine therapy.
Upfront zoledronic acid was received for 5 years compared with delayed zoledronic acid, which was started on the basis of decreased T-score.
Women who were >5 years postmenopausal only.
AI, aromatase inhibitor; CT, chemotherapy; DFS, disease-free survival; ET, endocrine therapy; GnRH, gonadotropin-releasing hormone; HR, hazard ratio; NR, not reported; OS, overall survival; PMW, postmenopausal women; RFS, recurrence-free survival; ST, standard therapy; TAM, tamoxifen; ZOL, zoledronic acid.
Data are from Gnant et al. [2011a], Coleman et al. [2010a], and de Boer et al. [2010].
AZURE trial
The AZURE trial evaluated the anticancer effects of zoledronic acid combined with adjuvant chemotherapy as well as endocrine therapy in pre- and postmenopausal women. In this study, women with stage II/III breast cancer (N = 3360) received standard therapy (i.e. chemotherapy or endocrine therapy) alone (control) or in combination with a tapered dosing schedule of zoledronic acid (4 mg every 3–4 weeks × 6; 4 mg every 3 months × 8; 4 mg every 6 months × 5). Notably, an early exploratory subset analysis of patients in this trial who received neoadjuvant chemotherapy (n = 205) showed that adding zoledronic acid reduced mean residual invasive tumor size by approximately 43.4% compared with chemotherapy alone (15.5 compared with 27.4 mm; p = 0.006) [Coleman et al. 2010b], suggesting potential anticancer benefit from combining zoledronic acid with cytotoxic chemotherapy in this setting.
Despite the potential anticancer activity of zoledronic acid suggested by the neoadjuvant subset analysis, adjuvant use of zoledronic acid did not improve the primary endpoint of DFS in the overall patient population (hazard ratio [HR] = 0.98; p = 0.79) [Coleman et al. 2010a]. However, there was a trend toward improved overall survival for zoledronic acid compared with control in the overall population (HR = 0.85; p = 0.07) [Coleman et al. 2010a]. It is likely that this trend was driven by the effects of zoledronic acid in some subsets of patients that have yet to be fully defined. Protocol-defined secondary endpoints in the AZURE trial included analyses of the zoledronic acid effect in patient subsets defined by minimization criteria, and showed that baseline menopausal status was the only factor that significantly influenced the effect of zoledronic acid on DFS [Coleman et al. 2010a]. Prospective subgroup analyses showed that zoledronic acid significantly improved DFS (HR = 0.76; p < 0.05) in women who were at least 5 years past menopause at study entry (n = 1041). Moreover, zoledronic acid was found to significantly improve overall survival (HR = 0.71; p = 0.017; n = 1101 including women of unknown postmenopausal status but age greater than 60 years). In addition, zoledronic acid reduced each type of DFS event and reduced recurrences both in and outside of bone (HR and p value were not reported) compared with control in this subset [Coleman et al. 2010a]. These data suggest that zoledronic acid has the greatest potential for anticancer benefits in a low-estrogen environment. Notably, estrogen levels decline rapidly before stabilizing approximately 2–3 years after menopause [Rannevik et al. 2008; Sowers et al. 2008]. Patients who were more than 5 years postmenopausal at baseline in the AZURE study were therefore likely to have had low estrogen levels.
Z-FAST, ZO-FAST, and E-ZO-FAST companion trials
Three companion studies, Z-FAST (N = 602), ZO-FAST (N = 1,065), and E-ZO-FAST (N = 527), were designed to evaluate the activity of zoledronic acid [upfront or delayed-start zoledronic acid (4 mg intravenously every 6 months for up to 5 years)] for preventing aromatase inhibitor-associated bone loss (AIBL) in postmenopausal women receiving adjuvant letrozole therapy for stage I–III breast cancer [Eidtmann et al. 2010; Llombart et al. 2009; Brufsky et al. 2008, 2009a]. Although these three bone health companion studies were not designed as anticancer trials, they assessed disease recurrence and DFS as secondary endpoints. The largest of the three trials (ZO-FAST, N = 1065) showed that adding upfront zoledronic acid to aromatase inhibitor therapy was associated with a 34% reduction in the risk of DFS events (disease recurrence or death) compared with delayed zoledronic acid (HR = 0.66; p = 0.0375) after a median follow up of 60 months [de Boer et al. 2010], despite approximately 25% of patients initiating zoledronic acid in the delayed group [Coleman et al. 2009]. Complete 60-month follow-up results from this study are expected this year.
In contrast with the ZO-FAST study, there were no significant differences in DFS for upfront compared with delayed zoledronic acid in the two smaller trials, Z-FAST (N = 602) and E-ZO-FAST (N = 527) [Coleman et al. 2009]. However, the lower event rates in Z-FAST (37 disease recurrences) and E-ZO-FAST (29 disease recurrences) preclude robust analyses of DFS compared with the larger ZO-FAST trial (87 disease recurrences and 104 DFS events) and the AZURE trial in patients at higher risk of recurrence (interim analysis conducted after 752 DFS events had occurred; 940 DFS events needed for final analysis) [de Boer et al. 2010; Coleman et al. 2010a].
ABCSG-12 trial
Like the AZURE study, DFS was the primary endpoint for the ABCSG-12 trial (N = 1803) [Gnant et al. 2009]. This trial is a randomized, phase III trial comparing the efficacy of tamoxifen (20 mg/day orally) with that of anastrozole (1 mg/day orally), with or without zoledronic acid (4 mg every 6 months) in premenopausal women with early stage, hormone-responsive breast cancer undergoing ovarian suppression with goserelin (3.6 mg subcutaneously every 28 days) for 3 years [Gnant et al. 2009]. Adding zoledronic acid to adjuvant endocrine therapy produced significant durable DFS benefits (HR = 0.64; p = 0.01 after a median follow up of 48 months; and HR = 0.68; log-rank p = 0.009 after a median follow up of 62 months) and a trend toward improved overall survival (HR = 0.67; log-rank p = 0.09) compared with endocrine therapy alone [Gnant et al. 2011b, 2009]. Furthermore, the trend for improved overall survival reached statistical significance at a median follow up of 76 months (HR = 0.59; log-rank p = 0.042) [Gnant et al. 2011a]. These benefits from adding zoledronic acid to adjuvant endocrine therapy were maintained more than 2 years after therapy completion, suggesting potential long-term carryover benefits from nitrogen-containing bisphosphonate therapy in early breast cancer.
Discussion
At first glance, the AZURE trial results appear inconsistent with those of the ABCSG-12 trial, which showed significant DFS benefits (that have proven consistent over time) from adding zoledronic acid to adjuvant therapy in premenopausal women with breast cancer. However, ovarian ablation with goserelin therapy resulted in amenorrhea in all patients in ABCSG-12, and residual estrogen levels in these patients were probably similar to the levels in postmenopausal women [Gnant et al. 2009]. In contrast, premenopausal women in the AZURE study likely received only chemotherapy (according to local treatment practices), resulting in heterogeneity in hormonal status. Furthermore, a preplanned subgroup analysis of the ABCSG-12 data suggested that the DFS and survival benefits with adjuvant zoledronic acid found in the overall population may be greatest in the patients most likely to achieve a low-estrogen environment [Gnant et al. 2011a]. In analyses of subgroups defined by age, no significant DFS (HR = 0.91; log-rank p = 0.707) or overall survival (HR = 1.01; log-rank p = 0.982) benefits were observed with zoledronic acid therapy in women 40 years of age or younger (n = 413). However, adding zoledronic acid to adjuvant endocrine therapy significantly reduced the risk of DFS events by 34% (HR = 0.66; log-rank p = 0.013) and reduced the risk of death by 49% (HR = 0.51; log-rank p = 0.018) for women older than 40 years (n = 1390) [Gnant et al. 2011a].
These data are consistent with the AZURE subgroup analyses in which significant DFS and overall survival benefits were observed in the postmenopausal patient population, suggesting that adjuvant zoledronic acid may have anticancer activity in patients with low estrogen levels. Although these trials did not measure estrogen levels, hormonal status can be assumed on the basis of the type of adjuvant endocrine therapy received, age, and menopausal status. Indeed, the subset of patients in ABCSG-12 who were older than 40 years at baseline may have achieved more complete estrogen suppression than younger patients. Case reports of pregnancies or resumed menses during suppression of ovarian function with an LHRH analogue in very young premenopausal women with breast cancer suggest the potential for incomplete ablation of circulating estrogen levels in this population [Jimenez-Gordo et al. 2000; Uncu et al. 1996]. Furthermore, chemotherapy-induced amenorrhea has been reported to occur less frequently in women younger than 40 compared with those older than 40 years [Gnant, 2009; Del Mastro et al. 1997], indicating that age markedly influences ovarian function during cancer therapy. Consequently, women more than 40 years of age in the ABCSG-12 trial presumably had more complete suppression of ovarian function compared with women 40 years of age or younger.
The findings of the AZURE and ABCSG-12 subset analyses suggest that effects of estrogen on the bone microenvironment may play a substantial role in determining who may benefit most from adjuvant zoledronic acid therapy. Ongoing analyses of the ZO-FAST trial database may offer additional insights into the possible relationship between menopausal status (established compared with newly menopausal) and improved disease outcomes with zoledronic acid. Overall, current clinical data suggest that both estrogen deprivation and reduction of bone turnover-derived growth factors in the bone marrow microenvironment are needed for sufficient suppression of dormant micrometastases in patients with early stage, hormone-receptor-positive breast cancer.
Footnotes
Acknowledgements
I thank Duprane Pedaci Young PhD, of ProEd Communications, Inc., for her medical editorial assistance with this manuscript.
Funding
Financial support for medical editorial assistance was provided by Novartis Pharmaceuticals.
Conflict of interest statement
Dr Gnant has received research support from and has served as a consultant for AstraZeneca, Novartis, and Pfizer, and has received lecture fees and honoraria for participation on advisory boards from AstraZeneca, Novartis, Sanofi-Aventis, Roche, Schering, Amgen, and Pfizer.