
Abstract
Ixabepilone demonstrates marked synergistic activity in combination with capecitabine, which served as the rationale for the evaluation of this combination in the clinic. Ixabepilone plus capecitabine is currently approved for patients with locally advanced or metastatic breast cancer (MBC) progressing after treatment with an anthracycline and a taxane; approval was based on the results of two phase III trials comparing the combination with capecitabine monotherapy. An array of preclinical studies in multiple solid tumor types show that ixabepilone demonstrates therapeutic synergy with targeted therapies including trastuzumab, bevacizumab, brivanib, and cetuximab; with immune-modulating agents such as anti-CTLA-4 antibody; and with other chemotherapy drugs such as irinotecan and epirubicin. Notably, experiments in several xenograft models show that ixabepilone provides greater antitumor synergism when combined with bevacizumab than either paclitaxel or nab-paclitaxel combined with bevacizumab. These preclinical findings provide a foundation for ongoing phase II clinical trials using ixabepilone in combination with trastuzumab or lapatinib in HER2-positive breast cancer; with bevacizumab in breast cancer, endometrial cancer, renal cancer, and non-small cell lung cancer (NSCLC); with cetuximab in breast cancer, NSCLC, and pancreatic cancer; and with brivanib, dasatinib, sorafinib, sunitinib, or vorinostat in MBC. Preliminary results from several of these trials suggest that ixabepilone-based combinations have promising anticancer activity.
Keywords
Introduction
Epothilones and taxanes bind to the same site on β-tubulin, but epothilones bind in a different manner [Rivera et al. 2008; Bode et al. 2002], which may explain why epothilones have reduced susceptibility to tumor resistance and retain activity against the tumor survival factor βIII tubulin. The natural epothilones have potent antineoplastic activity in vitro against a wide range of tumor cell lines [Bollag et al. 1995]. However, epothilones A and B proved less effective in vivo due to poor metabolic stability and unfavorable pharmacokinetic properties in rodent models [Lee et al. 2008a]. As a result, a series of semisynthetic analogs were produced and evaluated at Bristol-Myers Squibb in order to identify an agent that retained the antimicrotubule activity and reduced susceptibility to tumor resistance factors seen with epothilone B, but with improved pharmaceutical properties and in vivo efficacy.
The Bristol-Myers Squibb epothilone drug-discovery program created ixabepilone [Lee et al. 2008a]. Preclinical evaluation showed that ixabepilone was active in a wide range of tumor cells in vitro and tumor xenograft models in vivo, including those with chemoresistance to taxanes, anthracyclines, and other drug classes [Lee et al. 2009b, 2001]. Ixabepilone was selected for development because of its potent tubulin-polymerizing activity and in vivo efficacy, metabolic stability and low protein binding activity profile in high βIII-expressing/taxane-refractory tumor models, and low susceptibility to MDR-transport proteins [Lee et al. 2008a].
Preclinical findings with ixabepilone have translated to clinical studies. Phase II clinical trials show that ixabepilone is active in patients with a broad range of advanced solid malignancies, including breast cancer [Denduluri et al. 2007a, 2007b; Perez et al. 2007; Roché et al. 2007; Thomas et al. 2007a, 2007b; Low et al., 2005], pancreatic cancer [Whitehead et al. 2006], hormone-refractory prostate cancer [Galsky et al. 2005; Hussain et al. 2005], non-small cell lung cancer (NSCLC) [Vansteenkiste et al. 2007], endometrial carcinoma [Dizon et al. 2009], ovarian cancer [De Geest et al. 2010], and gastric cancer [Ajani et al. 2006]. In a phase III trial, ixabepilone plus capecitabine significantly extended progression-free survival (PFS) compared with capecitabine alone in women with locally advanced or metastatic breast cancer (MBC) who progressed after anthracycline and taxane treatment [Thomas et al. 2007a]. These clinical results led to approval of ixabepilone by the US Food and Drug Administration in October 2007, for the treatment of locally advanced or MBC in combination with capecitabine after failure of anthracycline and taxane therapy, and as monotherapy after failure of an anthracycline, a taxane, and capecitabine [Lechleider et al. 2008]. A second phase III trial in MBC patients pretreated with taxanes and anthracyclines confirmed the initial trial results, demonstrating the PFS benefit of ixabepilone plus capecitabine [Sparano et al. 2010; Hortobagyi et al. 2008].
Combination therapy is a mainstay of anticancer treatment, with optimal combinations producing synergistic antitumor responses, achieved by combining agents with nonoverlapping mechanisms of action and safety profiles. A number of targeted agents have demonstrated improvements in patient outcomes when used in combination with chemotherapy or as monotherapy depending on the treatment setting and tumor type [Nielsen et al. 2009; Di Costanzo et al. 2008; Blick and Scott, 2007; Press and Lenz, 2007]. For most clinical applications, targeted agents need to be combined with chemotherapy (often antimicrotubule agents) to achieve maximum efficacy. Currently, there are no definitive clinical data defining the optimal antimicrotubule agent for use in combination with targeted agents. In this paper, we review the preclinical and clinical evidence that ixabepilone has synergistic antitumor activity with key targeted agents and other chemotherapeutics in three solid tumor types: NSCLC, breast cancer, and colon cancer.
Methods
In vitro studies
The in vitro cytotoxicity of ixabepilone was evaluated against three tissue-specific tumor-cell panels, including 35 human breast cancer cell lines, 20 human colon cancer cell lines, and 23 human lung cancer cell lines [Lee et al. 2009b]. Most of the cell lines were obtained from American Type Culture Collection (Manassas, VA), and were maintained in RPMI 1640 culture medium and 10% fetal bovine serum. A tetrazolium-based colorimetric assay was used to assess cytotoxicity, based on the metabolic conversion of MTS (3-[4,5-dimethylthiazol-2-yl]-5-[3-carboxymethoxyphenyl]-2-[4-sulphenyl]-2H-tetrazolium, inner salt) to a reduced form that absorbs light at 492 nm. Tumor cells were incubated with serially diluted concentrations of ixabepilone at 37°C for 72 hours. MTS was added to the cells in combination with the electron-coupling agent phenazine methosulfate, incubated for 3 hours, and the absorbency of the medium was measured spectrophotometrically (492 nm) to obtain the number of surviving cells relative to control cell populations not exposed to ixabepilone.
In vivo models
The in vivo antitumor activity of ixabepilone, either alone or in combination with other anticancer agents, was evaluated in a series of human xenograft models as described previously [Lee et al. 2009b]. Human NSCLC (L2987), breast cancer (KPL4 and Pat-21), and colon cancer xenografts (GEO and HCTVM46) were used in the studies of ixabepilone in combination. Briefly, the tumors were maintained in nu/nu mice or Beige severe combined immunodeficient (SCID) mice, and propagated as subcutaneous transplants in the appropriate murine strain using tumor fragments obtained from donor mice. The anticancer agents were administered and evaluated at the maximum tolerated dose (MTD), defined as the dose level immediately below that which caused excessive toxicity (i.e. more than one death), as single-agent or combination therapy. Tumor response was determined by measuring tumors with calipers twice weekly until the tumors reached a predetermined target size of 500 or 1000 mg. Tumor weight (in milligrams) was estimated by multiplying the tumor length by the square of the tumor width, and then dividing by two. The tumor response endpoint was expressed in terms of tumor growth delay (T–C value), calculated as the difference in time (days) between the treated (T) and control (C) groups for the tumor to reach a predetermined target size.
Different tumor types can have different exponential growth rates, so delays in tumor growth were normalized by converting them into log cell kill (LCK) values. The LCK was calculated by dividing the T–C value by the tumor volume doubling time (TVDT) multiplied by the exponential function 3.32. Sensitivity to the treatment regimen was achieved when LCK was >1. Where indicated, tumor response was also characterized as partial regression (PR), complete regression (CR) or cure. PR was defined by a decrease in tumor volume >50%; CR by the disappearance of any visible or palpable tumor mass for two consecutive tumor measurements; and cure by the disappearance of any visible or palpable tumor mass for a period >10 times TVDT.
The in vivo antitumor activity of ixabepilone has also been evaluated in combination with a mouse anti-CTLA-4 monoclonal antibody (clone 4F10-UC10), a murine homolog of ipilimumab. Ipilimumab is a fully human anti-CTLA-4 monoclonal antibody in advanced clinical development. Lung cancer (M109), mammary carcinoma (EMT-6), and colon cancer (CT-26) murine models were used to evaluate the activity of this combination, and in some models, activity was compared with that of the ipilimumab mouse homolog, combined with paclitaxel. In addition, mice with M109 xenografts with complete tumor regression after initial tumor implantation and treatment with ixabepilone, with or without the ipilimumab mouse homolog, were rechallenged on day 98 with a lethal dose of tumor cells to determine the level of immune protection [Jure-Kunkel et al. 2008].
Clinical trial designs
Design of clinical trials evaluating ixabepilone in combination with other anticancer agents.
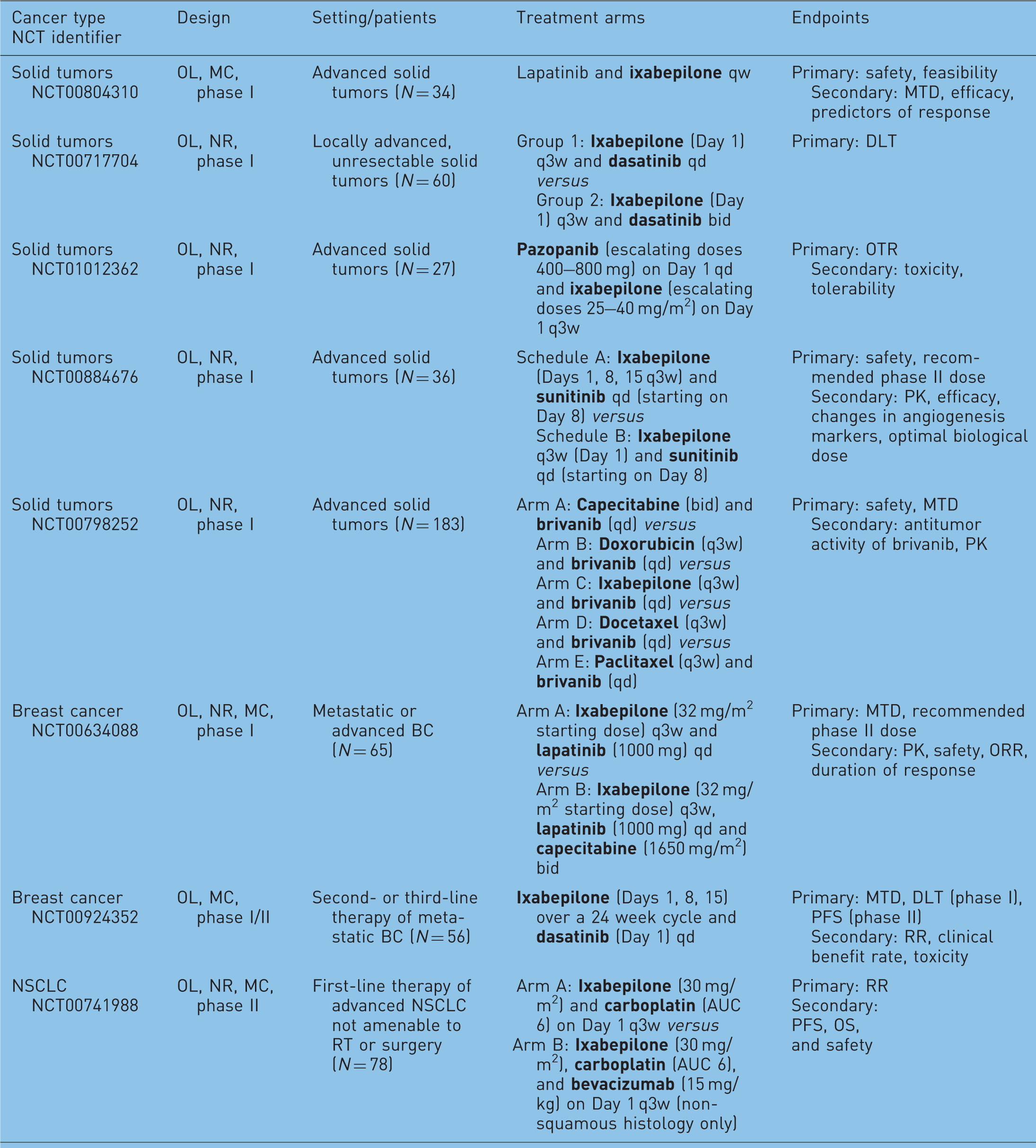
BC, breast cancer; CR, complete response; DFS, disease-free survival; DLT, dose-limiting toxicities; MC, multicenter; MTD, maximum tolerated dose; NR, nonrandomized; OL, open-label; ORR, objective response rate; OS, overall survival; OTR, optimum tolerated regimen; PFS, progression-free survival; PK, pharmacokinetics; R, randomized; RR, response rate; RT, radiotherapy; TTF, time to treatment failure; TTP, time to progression.
Results
Overview of preclinical studies of ixabepilone monotherapy
Preclinical studies of ixabepilone monotherapy [Lee et al. 2009b].

An IC50 value of >100 nM indicates ixabeplione resistance.
The antitumor activity of ixabepilone monotherapy was evident in human xenograft models. Ixabepilone demonstrated significant antitumor activity in 33 of 35 human cancer xenografts including all four NSCLC tumors, all four colon cancer tumors, and seven of eight breast cancer tumors [Lee et al. 2009b]. Significant antitumor activity was seen against ovarian, pancreatic, prostate, small cell lung, and gastric tumors, and a squamous cell carcinoma. In these xenografts, the activity of single-agent ixabepilone was shown by prolonged tumor growth delay ≥1 LCK, generally accompanied by significant tumor regression rates, and occasionally by long-term absence of measurable disease [Lee et al. 2009b; Lee, 2005].
Evidence for synergy with ixabepilone in lung cancer
Ixabepilone plus bevacizumab
Preclinical evidence of synergy between ixabepilone and targeted therapies in L2987 human lung cancer xenografts [Lee, 2005].
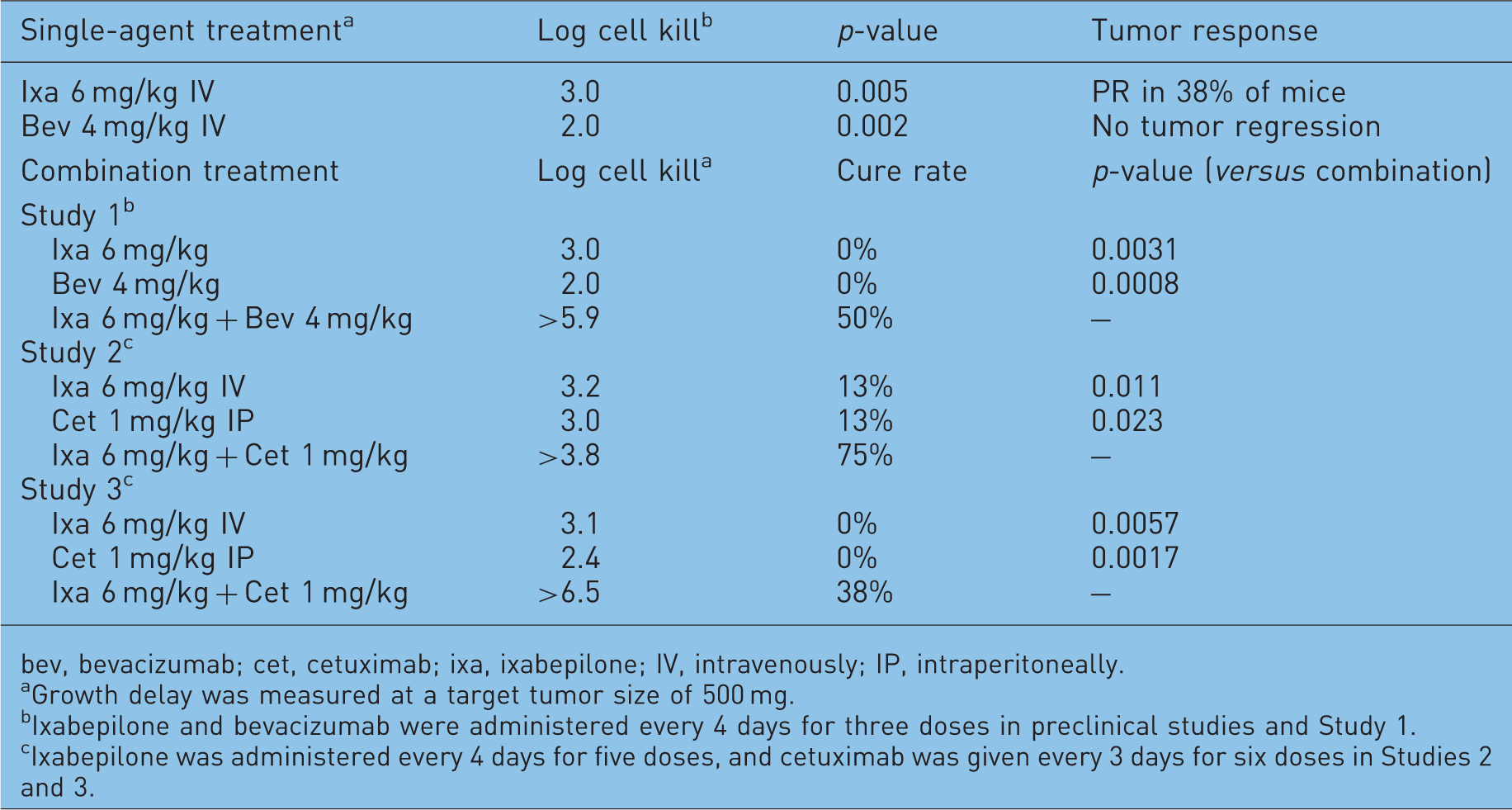
bev, bevacizumab; cet, cetuximab; ixa, ixabepilone; IV, intravenously; IP, intraperitoneally.
Growth delay was measured at a target tumor size of 500 mg.
Ixabepilone and bevacizumab were administered every 4 days for three doses in preclinical studies and Study 1.
Ixabepilone was administered every 4 days for five doses, and cetuximab was given every 3 days for six doses in Studies 2 and 3.
The demonstration of therapeutic synergism between ixabepilone and bevacizumab in vivo supported evaluation of these agents in combination in advanced NSCLC patients. In an ongoing, open-label, nonrandomized, multicenter, phase II trial [NCT00741988], newly diagnosed patients with advanced NSCLC that is not amenable to radiation therapy or surgery were treated with ixabepilone and carboplatin with or without bevacizumab. In order to ensure safe use of bevacizumab, patients with a squamous cell NSCLC histology were not eligible for the triple-therapy arm nor were patients receiving thrombolytic therapy or those with evidence of bleeding diathesis, coagulopathy, or a history of hemoptysis. The primary objective of this study was to evaluate the overall response rate (ORR) with each treatment regimen, whereas secondary objectives included evaluation of PFS, overall survival (OS), and safety. Results of this study were presented at ASCO 2010 [Shipley et al. 2010]. Eighty two patients were enrolled in the trial, and 66 patients were included in this analysis. Median follow up was 7 months (range 3.6–12.5), and the median number of cycles for arms A (ixabepilone plus carboplatin) and B (ixabepilone, carboplatin and bevacizumab) was two and three, respectively. The ORRs for arms A and B were 28% (95% CI 15–44%) and 46% (CI 27–67%), respectively. Stable disease was reported in 40% of patients in arm A and 28% of patients in arm B. Grade 3/4 adverse events included anemia, neutropenia, thrombocytopenia, hypersensitivity reaction, diarrhea, dyspnea, and neuropathy. These results confirm that these ixabepilone-based regimens are active in the first-line treatment of NSCLC.
Ixabepilone plus brivanib
Ixabepilone has also been evaluated in combination with the anti-angiogenic agent, brivanib (BMS-582664), a dual VEGF receptor (VEGFR) and fibroblast growth factor receptor (FGFR) tyrosine kinase inhibitor in clinical development. Mice with L2987 human lung cancer xenografts received ixabepilone at doses of 6, 10, or 13 mg/kg IV every 4 days for three doses in combination with brivanib at 100 mg/kg orally every day for 30 days [Lee et al. 2009a]. The MTD of ixabepilone was 13 mg/kg, the highest dose tested. Treatment efficacy was determined by the delay in time to achieve a target tumor size of 500 mm3. The combination of ixabepilone 6 mg/kg plus brivanib extended the time to target tumor size by 43 days compared with vehicle control; this was longer than the delay achieved with ixabepilone 6 mg/kg alone (7 days) or brivanib alone (26 days). Overall, combination therapy delayed tumor growth by 23% relative to the sum of the effects of the two drugs alone (i.e. 43 versus 33 days). Moreover, the combination produced a longer tumor growth delay than the 26 days achieved at the ixabepilone MTD. These findings support the continued evaluation of this novel drug combination.
A phase I trial of ixabepilone in combination with brivanib is currently ongoing [NCT00798252]. In this nonrandomized, open-label, multi-arm, dose escalation study of brivanib combined with several chemotherapy regimens, patients with advanced or metastatic solid tumors with no more than four previous chemotherapy regimens are being treated with ixabepilone and brivanib. The primary objective is to determine the safety and MTD of brivanib in combination with other chemotherapy agents. Secondary objectives include antitumor activity and pharmacokinetics. Planned accrual is 183 patients and the estimated study completion date is December 2011.
Ixabepilone plus cetuximab
Additional studies in L2987 human lung cancer xenografts showed that ixabepilone produces synergistic antitumor activity with cetuximab, a monoclonal antibody directed against the epidermal growth factor receptor (EGFR) [Lee et al. 2006]. In two separate independent studies, cetuximab at its MTD of 6 mg/kg IV produced LCK values of 3.2 and 3.1, respectively, whereas cetuximab at its OD of 1 mg/kg every 4 days for five doses produced LCK values of 3.0 and 2.4, respectively. Both single agents produced cures in 13% of animals in the first study, but none in the second study. However, in both studies, the combination of ixabepilone plus cetuximab was superior to ixabepilone alone (p = 0.011 and p = 0.006, respectively) and cetuximab alone (p = 0.023 and p = 0.002, respectively). In the first study, the LCK with the combination was >3.8 with 75% of the animals achieving cures, whereas in the second study, the LCK was >6.5 and the cure rate was 38%. Weight changes with the ixabepilone plus cetuximab were similar to those with ixabepilone alone. These findings indicate that ixabepilone produces therapeutic synergism with cetuximab [Lee, 2005].
Ixabepilone plus ipilimumab mouse homolog
The rationale for combining ixabepilone and the ipilimumab mouse homolog (murine anti-CTLA-4 monoclonal antibody) is based on their complimentary mechanisms of action. Ixabepilone induces tumor cell necrosis thereby releasing tumor antigens and changing tumor architecture to facilitate T-cell priming and infiltration, and blocking CTLA-4 promotes expansion and infiltration of tumor-primed cytolytic T cells. A synergistic and durable antitumor effect was observed with the combination in lung (M109) and other cancer models. In the M109 lung model, 80% of mice that received the combination were tumor free after initial tumor implantation, compared with 50% of mice that received ixabepilone alone and none that received the ipilimumab mouse homolog alone. This model was also used to evaluate the effect of combination therapy on inducing a protective memory immune response. On day 98, tumor-free mice were rechallenged with a lethal dose of live tumor cells. Most mice (75%) previously treated with combination rejected the tumor rechallenge, remaining tumor free, compared with only 20% of the mice originally treated with ixabepilone alone.
Additional experiments also showed that ixabepilone was a much more effective combination partner for the ipilimumab mouse homolog than paclitaxel. In the M109 tumor model, paclitaxel given alone at its OD of 24 mg/kg IP on days 3, 7, and 11 did not result in any complete tumor regressions, and when combined with the ipilimumab mouse homolog, only 20% of the mice were tumor free (compared with 80% with the ixabepilone and ipilimumab mouse homolog combination). These experiments demonstrate that combination treatment with ixabepilone and the ipilimumab mouse homolog is effective, producing durable antitumor effects, and warrants clinical investigation [Jure-Kunkel et al. 2008].
Evidence for synergy with ixabepilone in breast cancer
Therapeutic synergism between ixabepilone and capecitabine was shown in preclinical xenograft models [Lee et al. 2006] and in a phase III clinical trial in patients with MBC who had failed previous therapy with an anthracycline and a taxane [Thomas et al. 2007a]. The potential synergism between ixabepilone and other agents has been explored in breast cancer xenografts and clinical trials.
Ixabepilone plus trastuzumab
Preclinical evidence of synergy between ixabepilone and targeted therapies in human breast cancer xenografts [Lee et al. 2008b; Lee, 2005].

Bev, bevacizumab; CR, complete regression; Ixa, ixabepilone; IV, intravenously; PR, partial regression; T, trastuzumab.
Growth delay was measured at a target tumor size of 500 mg.
Ixabepilone and trastuzumab were administered every 4 days for five doses.
Ixabepilone and trastuzumab were administered every 4 days for three doses.
The combination of ixabepilone and trastuzumab is being evaluated in four phase II trials. In the first Eastern Cooperative Oncology Group trial (E2103), patients with HER2-positive MBC received first-line therapy with ixabepilone and carboplatin (on days 1, 8, and 15 of a 4-week cycle) plus weekly trastuzumab for six cycles. Maintenance trastuzumab was administered every 3 weeks until disease progression [Moulder et al. 2010]. Among 59 patients evaluable for response, the three-drug combination produced an ORR of 44%, including complete responses in three patients (5%) and partial responses in 23 patients (39%). Median PFS was 8 months. The regimen had an acceptable toxicity profile with neutropenia (48%), thrombocytopenia (14%), and anemia (12%) being the most common grade III/IV adverse events. The second trial involves an ixabepilone–carboplatin–trastuzumab combination (on day 1 every 3 weeks for up to six cycles, with trastuzumab continued for 1 year after surgery) in the neoadjuvant setting in women with HER2-positive locally advanced disease [NCT00821886]. The primary objective is to determine the pathologic complete response rate (RR) of neoadjuvant therapy. This study is currently recruiting patients, with planned accrual of 60 patients and an estimated study completion of January 2011.
In the other two studies, ixabepilone is being evaluated in combination with trastuzumab alone. One is an ongoing phase II, nonrandomized, multicenter, National Cancer Institute sponsored trial with two cohorts of patients with HER2-positive MBC: cohort 1 received no prior chemotherapy or trastuzumab for metastatic disease, and cohort 2 received one or two prior trastuzumab-containing regimens for metastatic disease [NCT00079326]. Patients in both cohorts received ixabepilone 40 mg/m2 as a 3-hour continuous infusion on day 1 of a 21-day cycle plus trastuzumab once every 21 days. The initial trastuzumab infusion was 8 mg/kg, and 6 mg/kg for subsequent infusions. Treatment was continued until disease progression or unacceptable toxicity. The primary endpoint was the RR in each cohort. Preliminary results have been reported for 39 patients, including 15 patients in cohort 1 and 24 in cohort 2 [Tolaney et al. 2008]. The ORR for the entire study population was 51.3%, with a substantially higher rate in cohort 1 compared with cohort 2 (80.0% versus 33.3%). When stable disease lasting ≥24 weeks was included, clinical benefit was achieved by 56.4% of patients; 80.0% in cohort 1 and 41.7% in cohort 2. The median time to treatment failure was 5.6 months in cohort 1 and 4.6 months in cohort 2. The combination regimen had an acceptable safety profile, although 56% of patients had grade II or higher sensory neuropathy.
In the final study, ixabepilone plus trastuzumab is being compared with a docetaxel–trastuzumab combination in patients with locally advanced or MBC. Patients who received prior chemotherapy or trastuzumab in the metastatic disease setting are not eligible, nor are patients who relapsed within 1 year after receiving adjuvant or neoadjuvant taxane or trastuzumab therapy. In both arms, the combination regimen is being administered every 3 weeks up to an estimated 10 cycles, with subsequent continuation of maintenance trastuzumab. Planned enrollment is 80 patients, with an estimated study completion of November 2012.
Ixabepilone plus lapatinib
The therapeutic potential of ixabepilone, lapatinib, paclitaxel, and trastuzumab was compared in three breast cancer cell lines: MCF-7 (control; non-HER2 amplified), SK-BR3, and BT-474 (HER2 amplified) [Mainwaring et al. 2009]. Dose response curves were clearly evident for all combinations; ixabepilone plus lapatinib significantly reduced proliferation (p < 0.001) at 120 hours. Of note, cell proliferation was reduced earlier and at lower drug concentrations with lapatinib combinations than with trastuzumab combinations.
An international, multicenter, nonrandomized, open-label phase I trial of ixabepilone in combination with lapatinib ± capecitabine has since commenced in patients with HER2-positive taxane and trastuzumab resistant advanced breast cancer [NCT00634088; Mainwaring et al. 2009]. Sixty five patients received ixabepilone plus lapatinib (Arm A) or ixabepilone plus lapatinib and capecitabine (Arm B). The primary outcome measures are MTD and recommended phase II dose for the two treatment arms. Study completion is estimated at September 2010.
Ixabepilone plus bevacizumab
Ixabepilone has also been evaluated in combination with bevacizumab in KPL4 and Pat-21 human breast cancer xenografts [Lee et al. 2009b, 2008b]. The Pat-21 model was sensitive to single-agent ixabepilone (LCK = 1.6) but resistant to single-agent bevacizumab (LCK = 0.3), whereas the converse was found in the KPL4 model (LCK = 0.5 and 2.2, respectively; Table 4). The combination of ixabepilone plus bevacizumab produced significantly greater antitumor activity than either agent alone in both KPL4 and Pat-21 xenografts, with LCK values of 2.3 and >3.2, respectively. Tumor regression was seen in all animals receiving the ixabepilone–bevacizumab combination.
The combination of ixabepilone plus bevacizumab is being compared with paclitaxel plus bevacizumab in a randomized, open-label, phase II trial of first-line therapy of locally recurrent or MBC [NCT00370552]. A total of 123 women were randomly allocated in a 3 : 3 : 2 ratio to receive ixabepilone on days 1, 8, and 15 of a 4-week cycle plus bevacizumab every 2 weeks (Arm A), ixabepilone and bevacizumab every 3 weeks (Arm B), or paclitaxel on days 1, 8, and 15 of a 4-week cycle plus bevacizumab every 2 weeks (Arm C). The final results of this study were presented recently [Rugo et al. 2010]. The ixabepilone–bevacizumab combination administered weekly or every 3 weeks demonstrated encouraging clinical activity compared with paclitaxel plus bevacizumab: objective RRs were 48%, 71%, and 63%, respectively. Median PFS was 9.6, 11.9, and 13.5 months, respectively. The safety profiles of the three regimens were generally comparable, with grade III peripheral neuropathy reported by 18%, 24%, and 25%, respectively. Grade III/IV neutropenia was more common with the every 3-week regimen than with either weekly regimen. These results support ongoing clinical trials of ixabepilone in first-line MBC, and in combination with bevacizumab.
The ixabepilone–bevacizumab combination is being compared with combinations of paclitaxel plus bevacizumab and nanoparticle albumin-bound paclitaxel (nab-paclitaxel) plus bevacizumab in the Cancer and Leukemia Group B (CALGB) 40502 trial [NCT00785291]. This randomized, three-arm, phase III trial is open to women with stage IIIB/IV breast cancer that is not amenable to local therapy. Patients with HER2-positive disease are eligible if previously treated with trastuzumab or lapatinib. Previous taxane therapy in the adjuvant or neoadjuvant setting is allowed providing it was completed at least 12 months before disease recurrence. To ensure the treatment groups are balanced, the patients are stratified according to taxane use in the adjuvant setting and estrogen receptor/progesterone receptor status. In each treatment arm, the chemotherapy will be administered on days 1, 8, and 15 of a 4-week cycle, whereas bevacizumab will be given on days 1 and 15. PFS is the primary outcome measure. Patients are currently being enrolled into the study and the target accrual is 900.
Ixabepilone plus cetuximab
Triple-negative breast cancer is a disease subset associated with an aggressive clinical course and poor outcomes [Rakha and Ellis, 2009]. In an ongoing phase II trial, ixabepilone plus cetuximab is being compared with single-agent ixabepilone as first-line therapy for patients with triple-negative locally advanced nonresectable or MBC [NCT00633464]. Ixabepilone 40 mg/m2 is being administered every 3 weeks, whereas cetuximab is being given at its standard dose of 250 mg/m2 weekly following a 400 mg/m2 loading dose. The study plans to enroll 80 patients and has an estimated completion date of January 2012.
Ixabepilone plus ipilimumab mouse homolog
The combination of ixabepilone plus the ipilimumab mouse homolog (anti-CTLA-4 monoclonal antibody) was evaluated in EMT-6 mammary carcinoma xenografts. In these studies, ixabepilone was administered at 8 mg/kg intraperitoneally (IP) on days 3, 7, and 11, and the ipilimumab mouse homolog at 20 mg/kg IP on days 4, 8, and 12. Ixabepilone alone produced complete regressions in 20% of mice, and the ipilimumab mouse homolog alone produced regressions in 40% of mice. However, combining the agents had a synergistic therapeutic effect, inducing complete regressions in all treated mice. Furthermore, ixabepilone was a more effective combination partner than paclitaxel, as paclitaxel and the ipilimumab mouse homolog induced regressions in only 40% of mice, essentially comparable with the effect of the antibody alone [Jure-Kunkel et al. 2008].
Preclinical evidence for synergy with ixabepilone in colon cancer
Ixabepilone plus cetuximab
Preclinical evidence of synergy between ixabepilone and other anticancer agents in human colon cancer xenografts [Lee et al. 2008b; Lee, 2005].
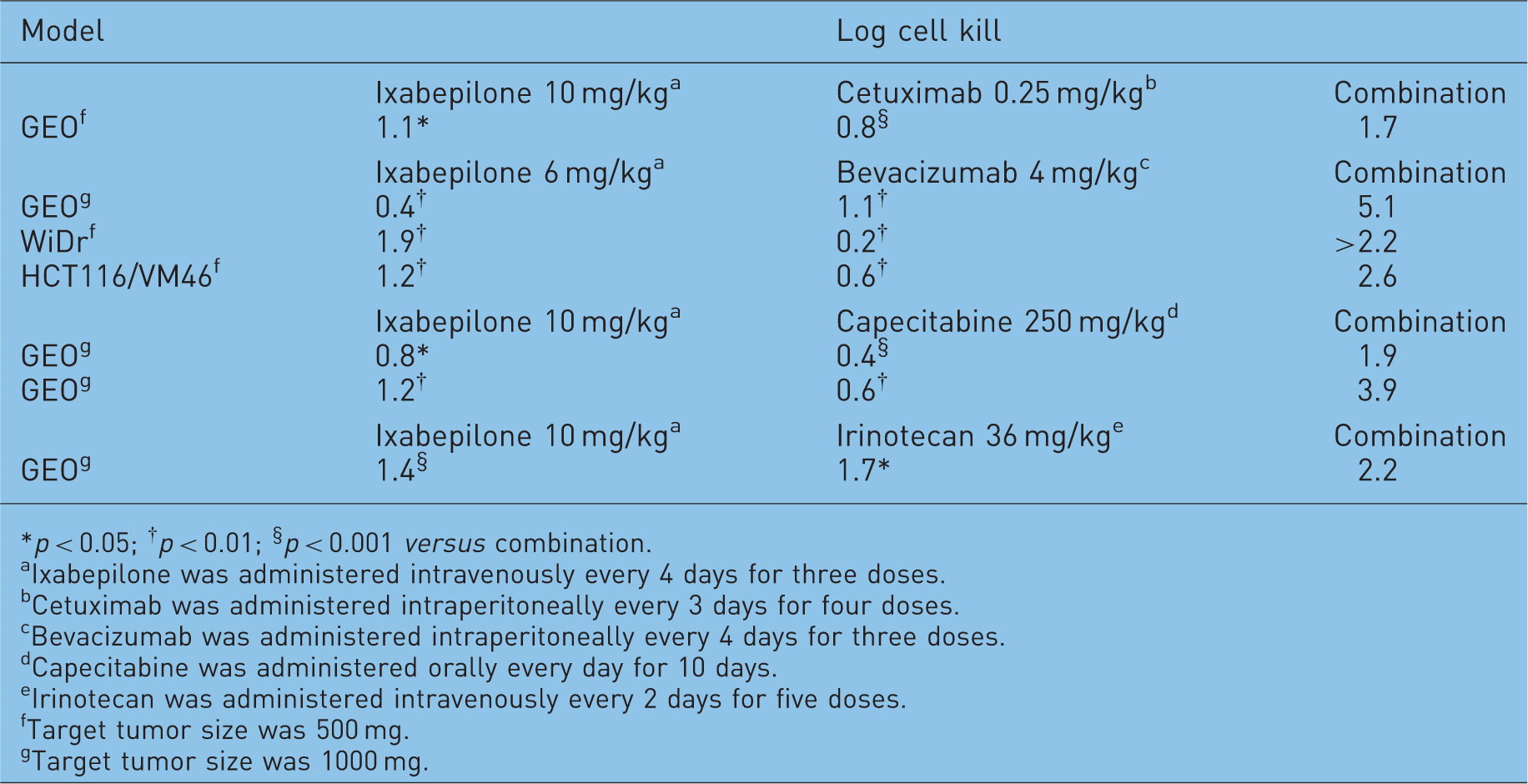
*p < 0.05; † p < 0.01; § p < 0.001 versus combination.
Ixabepilone was administered intravenously every 4 days for three doses.
Cetuximab was administered intraperitoneally every 3 days for four doses.
Bevacizumab was administered intraperitoneally every 4 days for three doses.
Capecitabine was administered orally every day for 10 days.
Irinotecan was administered intravenously every 2 days for five doses.
Target tumor size was 500 mg.
Target tumor size was 1000 mg.
Ixabepilone plus bevacizumab
Three different human colon cancer xenografts (GEO, WiDr, and the multidrug-resistant HCT116/VM46) were used to evaluate ixabepilone in combination with bevacizumab [Lee et al. 2008b]. Single-agent ixabepilone exhibited greater antitumor activity against the WiDr and HCT116/VM46 xenografts than the GEO xenografts (Table 5). Conversely, bevacizumab was active in the GEO model but not in the other two models. In each model, the ixabepilone–bevacizumab combination produced significantly greater antitumor activity than either agent alone, with LCK values of 5.1, >2.2, and 2.6 against the GEO, WiDr, and HCT116/VM46 xenografts, respectively (all p < 0.01) (Table 5). The ixabepilone–bevacizumab combination produced tumor regression in all mice with WiDr xenografts and in 88% of mice with multidrug-resistant HCT116/VM46 xenografts, but not in the GEO model, including CR rates of 63% and 25%, respectively. Single-agent ixabepilone produced lower rates of tumor regression: 38% in WiDr xenografts and 25% in HCT116/VM46 xenografts (including 13% with CR). Tumor regression was not seen in any mice treated with single-agent bevacizumab.
Ixabepilone produces greater therapeutic synergism with bevacizumab compared with paclitaxel in human colon cancer xenografts [Lee et al. 2008b].
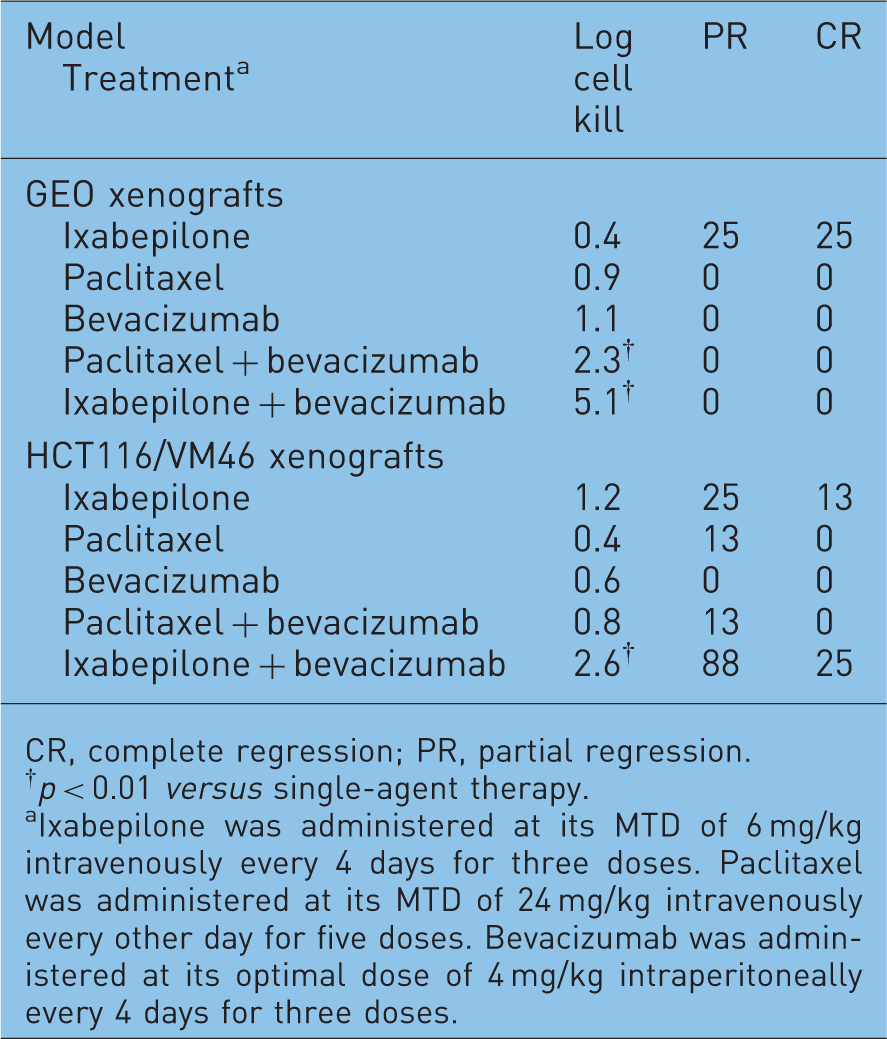
CR, complete regression; PR, partial regression.
p < 0.01 versus single-agent therapy.
Ixabepilone was administered at its MTD of 6 mg/kg intravenously every 4 days for three doses. Paclitaxel was administered at its MTD of 24 mg/kg intravenously every other day for five doses. Bevacizumab was administered at its optimal dose of 4 mg/kg intraperitoneally every 4 days for three doses.
Ixabepilone plus capecitabine
The antitumor activity of ixabepilone in combination with capecitabine was evaluated in the GEO model in two independent studies. In the first study, single-agent ixabepilone exhibited only modest activity with an LCK of 0.8 [Lee et al. 2006], and capecitabine was not active with an LCK of 0.4. However, the combination of these agents produced therapeutic synergism with an LCK of 1.9, which was superior to the activity of ixabepilone (p = 0.035) and capecitabine (p = 0.004) administered alone. Similar results were found in the second study: the LCK values were 1.2 with single-agent ixabepilone, 0.6 with single-agent capecitabine, and 3.9 with the combination (Table 5) [Lee et al. 2006].
Ixabepilone plus irinotecan
At their respective MTD, single-agent ixabepilone or irinotecan produced similar antitumor activity in the GEO xenografts with LCK values of 1.4 and 1.7, respectively (Table 5). The combination of ixabepilone and irinotecan produced significantly greater antitumor activity (LCK of 2.2) than either agent alone (p = 0.0004 versus ixabepilone and p = 0.0272 versus irinotecan) [Lee, 2005].
Discussion
Ixabepilone is the first epothilone to be approved for the treatment of patients with locally advanced or MBC. In vitro cytotoxicity studies in a broad panel of human tumor cell lines derived from breast cancer, NSCLC, and colon cancer demonstrate that ixabepilone has a broad spectrum of antineoplastic activity [Lee et al. 2009b, 2001]. This in vitro activity is paralleled by an equally broad spectrum of antitumor activity in human tumor xenograft models including breast, lung, colon, ovarian, prostate, pancreatic cancer, and gastric cancers. Notably, ixabepilone often produced significant tumor regression in these models, which in some cases led to the long-term absence of measurable disease. The antitumor activity of ixabepilone was evident in xenografts with various resistance mechanisms, including overexpression of the tumor survival and taxane resistance factor βIII-tubulin (e.g. Pat-21 and DU4475 breast lines, H1155, and LX-1 NSCLC lines) and overexpression of drug efflux pumps such as P-glycoprotein (e.g. HCT116/VM46 and Pat-7). These preclinical findings led to clinical evaluation of ixabepilone in a variety of human tumor types such as breast, pancreatic, prostate, endometrial, and NSCLC. Indeed, ixabepilone demonstrated clinical activity against a wide range of tumor types, including heavily pretreated and drug-resistant tumors.
The preclinical demonstration of synergism between ixabepilone and capecitabine led to clinical evaluation of this combination in MBC. A phase I/II study demonstrated the feasibility of combining ixabepilone and capecitabine [Bunnell et al. 2008], and two phase III studies demonstrated that the combination offers superior efficacy compared with capecitabine alone in patients with MBC who progressed after treatment with an anthracycline and a taxane [Thomas et al. 2007a].
Preclinical studies have driven the development of ixabepilone in breast cancer. Preclinical studies using xenograft models of multiple tumor types, including NSCLC, breast cancer, and colon cancer, indicate that ixabepilone has the potential for producing synergistic antitumor activity, while maintaining an acceptable safety profile, when combined with other approved anticancer agents, including monoclonal antibodies (trastuzumab, bevacizumab, and cetuximab) and chemotherapeutic agents (capecitabine and irinotecan). Clinical studies established that targeted agents provide greater clinical benefit when combined with a chemotherapeutic agent. Preclinical combination studies suggest that ixabepilone may be an optimal chemotherapy backbone for combination with targeted agents, as compared with paclitaxel. Preclinical data have provided the rationale for numerous ongoing or completed phase I/II clinical trials using ixabepilone in combination with trastuzumab or lapatinib in HER2-positive breast cancer [NCT00077376; NCT00079326; NCT00490646; NCT00821886]; bevacizumab, brivanib, dasatinib, sorafinib, sunitinib, vorinostat, or cetuximab in breast cancer [NCT00370552; NCT00633464; NCT00785291]; bevacizumab in endometrial cancer, renal cancer [NCT00820209; NCT00923130], ovarian cancer, and NSCLC [NCT00741988]; and cetuximab in pancreatic cancer [NCT00383149].
Overall, these data demonstrate that although ixabepilone has preclinical and clinical efficacy as a single agent, its greatest antineoplastic activity may be achieved in combination with other therapies. Moreover, current evidence suggests that ixabepilone-based combination therapy may provide clinical benefit versus several primary tumors. The ongoing clinical trial program will provide a more robust assessment of the synergy that is possible with ixabepilone combination therapies in the clinic.
Footnotes
Acknowledgments
The authors take full responsibility for the content of this publication and confirm that it reflects their viewpoints and scientific expertise. They also wish to acknowledge StemScientific, funded by Bristol-Myers Squibb, for providing writing and editorial support.