
Abstract
Background
In patients with symptomatic rotator cuff tears, arthroscopic rotator cuff repair (ARCR) is typically recommended when conservative management fails to provide symptom relief. Chronic post-surgical pain (CPSP) following ARCR is not uncommon and significantly reduces function and quality of life. This study aimed to develop a clinical prediction model for CPSP after ARCR.
Methods
This prospective analysis included 103 participants who underwent ARCR between August 2022 and November 2024. Potential predictor outcome variables were recorded preoperatively, and postoperative pain was assessed at 6 weeks, 3 months, and 6 months. The primary outcome was CPSP at rest and on shoulder movements, which was measured at the 6-month follow-up.
Results
Prediction models were developed using binomial logistic regression analysis and bootstrapping techniques for internal validation. Key independent predictors included scores on measures of Pain Catastrophizing Scale, Depression, Anxiety, Stress Scale 21, and Central Sensitization Inventory, as well as the pressure pain threshold over the middle deltoid muscle on the affected side.
Conclusion
Prediction models have been developed to forecast the occurrence of CPSP of the shoulder at 6 months post-ARCR. This represents a foundational step towards providing tailored risk evaluation, which can guide decisions regarding surgical management and therapeutic interventions for patients undergoing ARCR.
Introduction
Rotator cuff-related shoulder pain is a primary cause of shoulder pain and dysfunction. Rotator cuff (RC) tears occur in 13% to 37% of the general population, and the prevalence of RC tears increases with age.1,2 The initial guideline-driven approach for managing patients with RC tears consists of conservative measures, such as rest, ice, physical therapy, and anti-inflammatory medications. 3 Surgical repair is recommended when conservative management fails to provide the desired results of pain relief and functional improvement. 4 Arthroscopic rotator cuff repair (ARCR) is the standard surgical procedure for treating patients with RC tears who have not responded favourably to conservative care. 5 The rate of ARCR has constantly risen over time, and this procedure aims to reduce shoulder pain, restore function, and improve joint stability. 6 However, a subgroup of patients can develop chronic post-surgical pain (CPSP) after the ARCR procedure.7,8 In 2019, the International Association of the Study of Pain redefined CPSP as pain that develops or increases in intensity after a surgical procedure, persists for at least 3 months, and is localized to the surgical field or related innervation territory 9 CPSP often disrupts daily activities and negatively impacts quality of life and emotional and physical well-being. 10 Among the various shoulder arthroscopy procedures, ARCR is recognized as the most painful intervention. 11 Thus, CPSP can negatively affect a patient's function and overall quality of life. 12 Most of the time, CPSP has no bearing on the surgical intervention's success or failure, the tear's size, or the repair technique used. The literature suggests that various biopsychosocial factors contribute to the development of CPSP following the surgical procedure. 13 Following ARCR, several modifiable and non-modifiable predictors of CPSP have been identified. Some modifiable factors include greater preoperative pain, worse shoulder function, higher C-reactive protein levels, and longer symptom duration.7,14 The development of CPSP can also be predicted by several structurally linked non-modifiable factors, including tendon retraction and fatty infiltration of the RC muscles. 8 Psychological factors, like depression, anxiety, and pain catastrophizing, have shown a significant contribution to the development of CPSP following ARCR.15,16 Those with higher levels of measured psychological distress show heightened sensitivity to pain and a higher incidence of transitioning to chronic pain. Preoperative strategies to mitigate the adverse effects of psychological distress on surgical and rehabilitation outcomes have been highlighted in recent literature. 17 Additionally, recent studies indicate that preexisting altered pain processing significantly contributes to the persistent pain in various orthopedic surgeries.18,19 Emerging cohort data underscore the importance of psychosocial factors in shoulder pain outcomes. For example, in a large, multicentre cohort study of people referred for physiotherapy, Chester et al. found that psychological measures such as expectations of recovery, pain self-efficacy, and pain at rest were among the most consistent predictors of clinical outcome at 6 months, outperforming traditional clinical examination findings and structural diagnosis. These findings support a shift toward a comprehensive assessment and the need for risk-stratification tools when managing patients with RC tears. 20
Implementing high-quality clinical prediction models could enhance shared decision-making, leading to more efficient resource allocation and effective postoperative pain management, and reduce the number of patients developing CPSP.21,22 Therefore, clinical prediction models could prove essential for identifying patients at risk of developing CPSP and supporting preoperative and postoperative clinical decision-making based on individual patient risk profiles. While developing this prediction model, we focused on the modifiable factors that can be addressed before the surgical procedure to lower the risk of developing CPSP. This study aimed to develop preoperative clinical prediction models for the occurrence of CPSP of the shoulder in patients undergoing ARCR.
Materials and methods
Study design and participants
This prospective cohort study was conducted at the Department of Physiotherapy, Kasturba Hospital, Manipal, India. Patients who underwent ARCR for degenerative or traumatic RC tears between August 2022 and November 2024 at a single institution were included in the study. The Institutional Ethics Committee approved the study protocol (IEC:40/2020), and the study was registered in the clinical trials registry of India (CTRI/2021/04/032929). Participants were selected using purposive sampling to include individuals meeting the specific inclusion criteria relevant to this study. All participants received participant information sheets, and written informed consent was obtained prospectively. Participants were recruited from the hospital, and data were collected either the day before or on the day of ARCR surgery. This study was conducted as an unblinded investigation due to the nature of the clinical assessments and interventions, where blinding of participants and assessors was not feasible. While this may introduce risk of bias, all analyses were conducted with methodological rigor to minimize its impact. This study adhered to the Declaration of Helsinki.
Inclusion and exclusion criteria
The study included participants diagnosed with RC tears using diagnostic ultrasound and/or magnetic resonance imaging following clinical and radiological criteria. The inclusion criteria were age between 18 and 70 years, with unilateral RC tears undergoing primary ARCR surgery. The exclusion criteria included participants with fractures around the shoulder or upper quarter, previous diagnosis of chronic pain conditions, open or mini-open RC repair, trauma to the head or neck, language barrier, revision repair, cervical radiculopathy, neurological disorders, systemic inflammatory conditions, diagnosis of psychological conditions on medications, consumption of antidepressants or anticonvulsants, and malignancy.
Data collection and outcome measures
Preoperative data collection
Demographic and clinical data were obtained using data collection forms and electronic medical records. Preoperative patient characteristics included age, sex, height, weight, occupation, marital status, level of education, hand dominance, affected side, duration of symptoms, information on the nature of RC tears (i.e., traumatic or degenerative), and comorbidities such as diabetes mellitus, hypothyroidism, asthma, and hypertension. Electronic medical records were referenced to determine the number of tendon tears, tear size, and ultrasound and magnetic resonance imaging findings when available.
Pain, physical, and psychological assessments were performed at baseline (Table 1). Potential predictors for CPSP were selected based on a thorough review of the published literature,15,18,23,24 clinical expertise from professionals, including orthopedic surgeons and physical therapists, and potential modifiable factors considered for future clinical applications. Ten potential modifiable predictor outcome variables, broadly categorised as clinical, psychological and pain characteristics were recorded. Predictors identified a priori included (a) Pain characteristics: pain intensity measured using the Numerical Pain Rating Scale (NRS), assessments were made with the subject at rest and during active movement of the affected shoulder in the scaption plane; the temporal summation (TS) of pain to mechanical stimulus was recorded at the dorsal aspect of uninvolved forearm; pressure pain threshold (PPT) was measured over the middle deltoid, upper trapezius, infraspinatus, levator scapulae, and tibialis anterior muscles; Central Sensitization Inventory (CSI); (b) Clinical characteristics: Western Ontario Rotator Cuff Index (WORC); Quick Disability of Arm, Shoulder, and Hand Scale (Quick DASH); grip strength on the affected side; (c) Psychological factors: Pain Catastrophizing Scale (PCS); and Depression Anxiety Stress Scale 21 (DASS-21). The scales were implemented in English and the local language, Kannada. To translate the scales (CSI, WORC, DASS-21), we followed the following steps: forward translation, comparison of the two translated versions, blind back translation, comparison of the two back-translated versions, and pilot testing of the pre-final version in the Kannada language by eight participants. Bilingual experts assessed the content validity of the translated questionnaires before implementation. Ten predictor variables were recorded for each patient.
List of prognostic variables and the timelines of measurement.
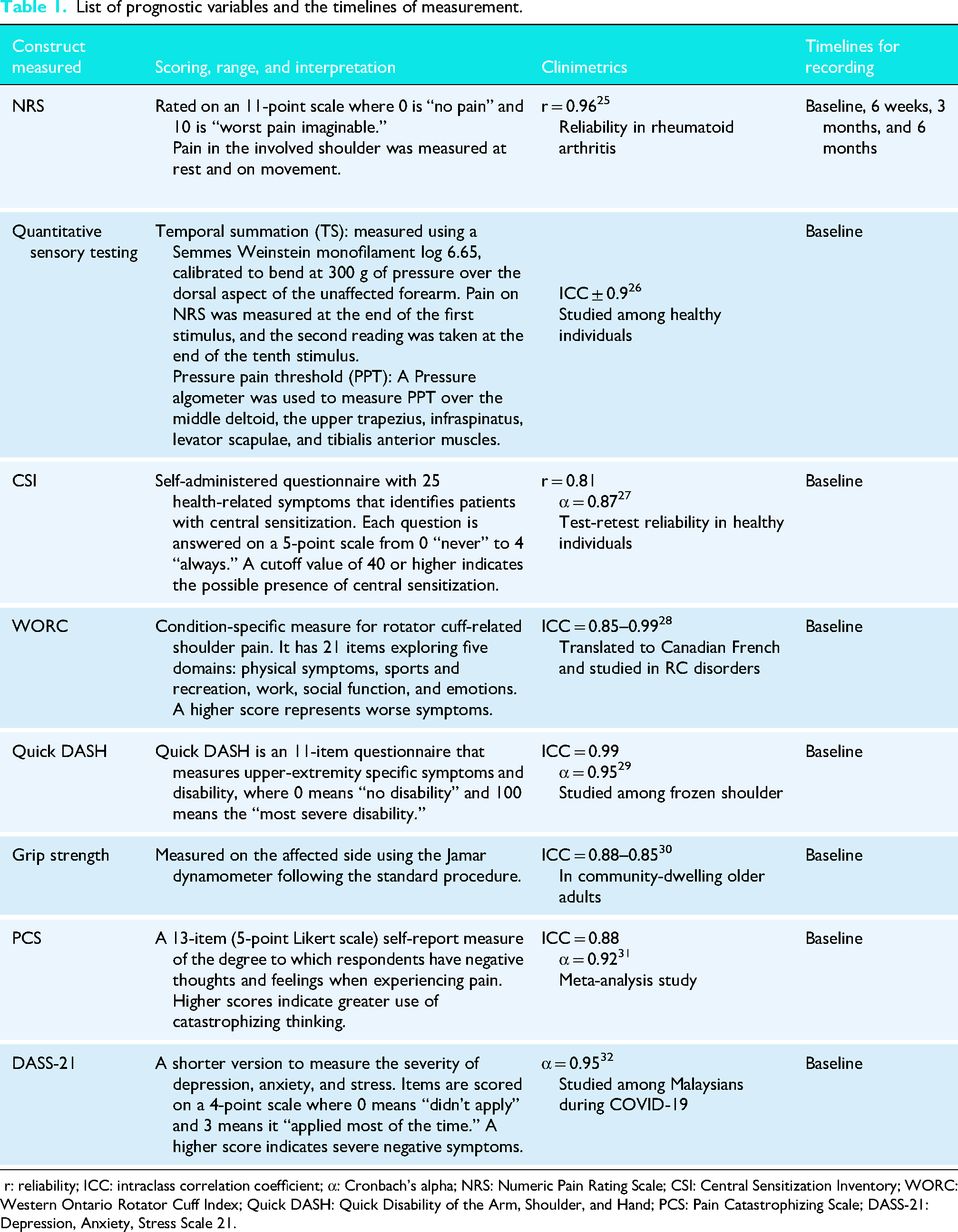
r: reliability; ICC: intraclass correlation coefficient; α: Cronbach's alpha; NRS: Numeric Pain Rating Scale; CSI: Central Sensitization Inventory; WORC: Western Ontario Rotator Cuff Index; Quick DASH: Quick Disability of the Arm, Shoulder, and Hand; PCS: Pain Catastrophizing Scale; DASS-21: Depression, Anxiety, Stress Scale 21.
Surgical procedure and rehabilitation
ARCR was performed by a single surgeon (VP) according to established clinical and international guidelines, with patients positioned in the beach chair position under general anesthesia. Following diagnostic arthroscopy, biceps tenotomy was selectively performed as needed. The ruptured tendons were mobilized and repositioned at their original footprint with minimal tension. A knotless suture bridge fixation technique was employed, utilizing two medial and two lateral screws and/or resorbable push-in anchors for supraspinatus tendon fixation. In a minority of cases, metal screws or non-resorbable push-in anchors were used. Additionally, medial anchors were applied to the subscapularis and infraspinatus tendons when required. Multi-strand, ultra-high molecular-weight polyethylene wires and/or tape sutures were utilized. RC integrity was confirmed intraoperatively, and surgical details were documented immediately post-surgery.
A standard rehabilitation protocol was implemented, and the physical therapy program was implemented across the three phases at the rehabilitation center of the same hospital. Phase 1: protection with a shoulder sling for 6 weeks with active elbow, wrist, and hand movements, and passive initial range of shoulder movements in the direction of flexion, abduction, minimal external rotation, and cervical spine isometrics. Phase 2: Active and active-assisted mobilization of the shoulder and coordination training. Phase 3: Progressive resistance exercises.33,34 Exercises were tailored to patients’ needs when required.
Measurement of CPSP
The NRS is widely used to measure CPSP across various populations. 35 We utilized the NRS to assess the intensity of shoulder pain. At every time point, shoulder pain was recorded at rest and during movement, i.e., on active shoulder elevation in the scaption plane. Post-surgical pain was recorded three times: 6 weeks, 3 months, and 6 months after the procedure, as depicted in Figure 1. We used follow-up data collected 6 months postoperatively because this timing was the most appropriate for reporting CPSP. CPSP was defined as a pain rating of ≥3 on NRS at rest or movement at 6 months after the surgical procedure. 36 Recovery from ARCR can take up to 3 months; therefore, we chose to assess pain ratings at 6 months for CPSP in this study.

Timelines for data collection and follow-up in the prospective cohort study.
Sample size calculation
To ensure the accuracy and generalizability of our prediction model, we determined the required sample size based on the events per variable (EPV) approach. 37 This method requires a minimum of 10 EPVs for each variable included in the model to ensure precision in the parameter estimates. This approach helps mitigate the risk of overfitting and improves the stability of the model's predictive performance. 38 Considering a 10% drop-out rate. We estimated that at least 110 participants would be needed to achieve enough events for 10 or fewer predictors, ensuring that our model is both robust and generalizable.
Statistical analysis
Statistical analyses were conducted using Jamovi 2.4.8 software. Normality was assessed using the Kolmogorov-Smirnov test. Based on this assessment, we performed parametric and nonparametric tests for this study. Descriptive statistics were used to summarize demographic data. Normally distributed data are expressed as mean ± standard deviation, while non-normally distributed data are presented as median and interquartile range. Categorical variables are reported as frequencies and percentages.
The presence of CPSP at the 6-month follow-up was defined as a binary variable; specifically, it indicated the presence of shoulder pain at rest and/or during movement, as reported by the patient. We developed two prediction models using logistic regression for the occurrence of CPSP based on available information regarding pain at rest and pain during movement for 6 months post-ARCR. Potential predictors identified a priori included pain on the NRS, temporal summation of pain to mechanical stimuli, PPT, CSI, WORC, QuickDASH, grip strength on the affected side, PCS, and DASS-21. Regarding missing data, no potential predictor had a missingness rate exceeding 20%. The WORC exhibited a missing data rate of 14% in the domain related to sports and recreation, which did not apply to 15 participants.
Mann-Whitney U-test was performed to compare between pain and non-pain groups. Binomial logistic regression was employed to examine the association between factors related to pain and no pain, based on pain at rest and pain during movement at 6 months. The association between all candidate predictors and CPSP was examined using bivariate logistic regression. A parsimonious set of final predictor variables was formed by discarding candidate variables with a p > 0.2 from the bivariate analysis. The remaining potential predictors were included in a binomial model, from which any variables that did not maintain significance at the p > 0.2 threshold were eliminated. We opted for a significance threshold of 0.2 instead of the traditional 0.05 found in explanatory models to enhance statistical power and prevent underfitting a model with an insufficient number of variables. Our model for predicting CPSP at 6 months was constructed using a stepwise selection approach. We computed the apparent and optimism-corrected c-statistic areas under the curve (AUC) to assess model discrimination. The apparent c-statistic quantifies the prediction model's accuracy within the study sample, while the optimism-corrected c-statistic estimates the model's performance in a new sample. We designed the confusion matrix to determine the sensitivity, specificity, positive, and negative predictive value of our findings. We conducted internal validation of the prediction models by repeating these assessments using bootstrapped resampling with the replacement method, performing 100 iterations for each imputed and complete data set, and calculating the overfitting percentage.
Results
Patient demographic characteristics
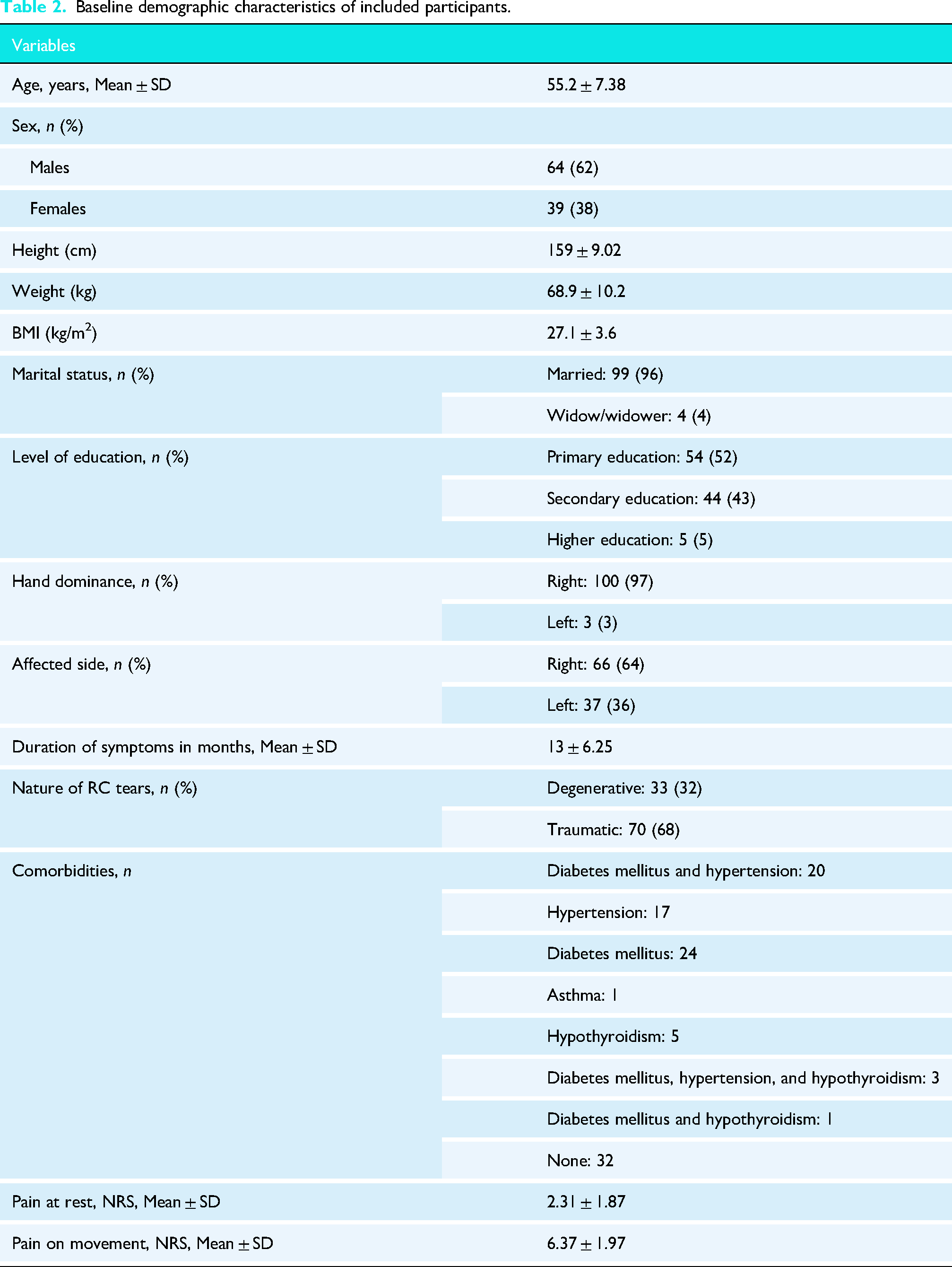
A total of 170 participants were screened based on the inclusion and exclusion criteria; 103 participants completed the study. The patient recruitment and follow-up details are shown in Figure 2. The baseline demographic characteristics of the participants are shown in Table 2. The mean age of our participants was 55 years, with the majority being male and predominantly exhibiting right-hand dominance. Many patients had associated comorbidities, including diabetes mellitus, hypertension, hypothyroidism, and asthma. In total, seven participants experienced CPSP at rest at the 6-month follow-up, while 18 participants reported pain during movement during the same follow-up period.
The comparison between participants with and without pain was examined using the Mann-Whitney U test, and the findings are reported in Table 3. At the six-month follow-up, seven participants reported CPSP at rest. Variables with a p-value of less than 0.20 were carried forward into the binomial model. These included the PPT over the Levator Scapulae, PCS, CSI, QuickDASH, and DASS-21. Eighteen participants reported CPSP in shoulder movements at the six-month follow-up. The variables considered as potential predictors included temporal summation, PPT over the Middle Deltoid and Levator Scapulae, as well as WORC, PCS, CSI, and DASS-21.
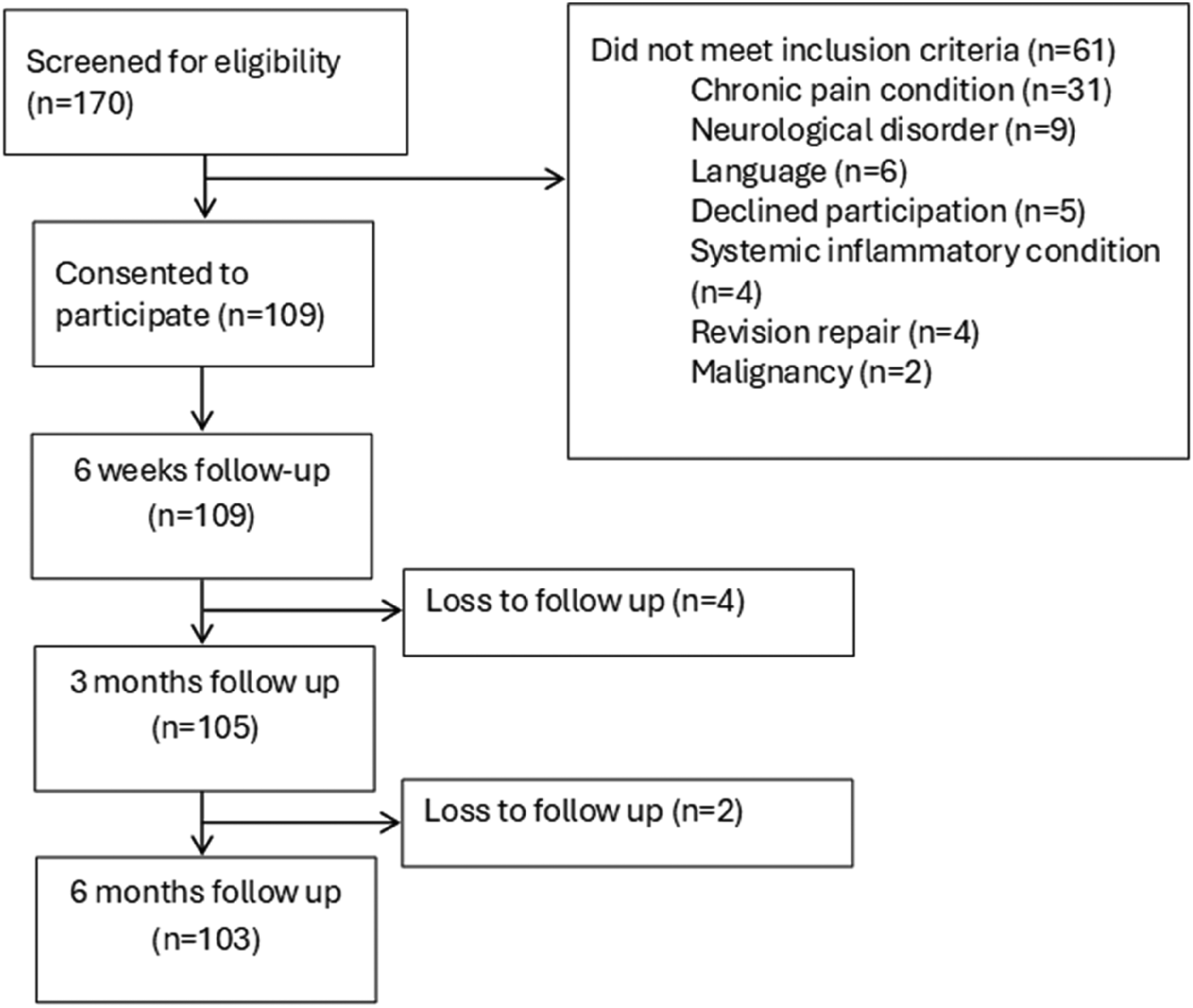
Flow of participants in the study.
Baseline demographic characteristics of included participants.
Univariate analysis of predictors of pain at 6-month follow-up in participants with and without CPSP.
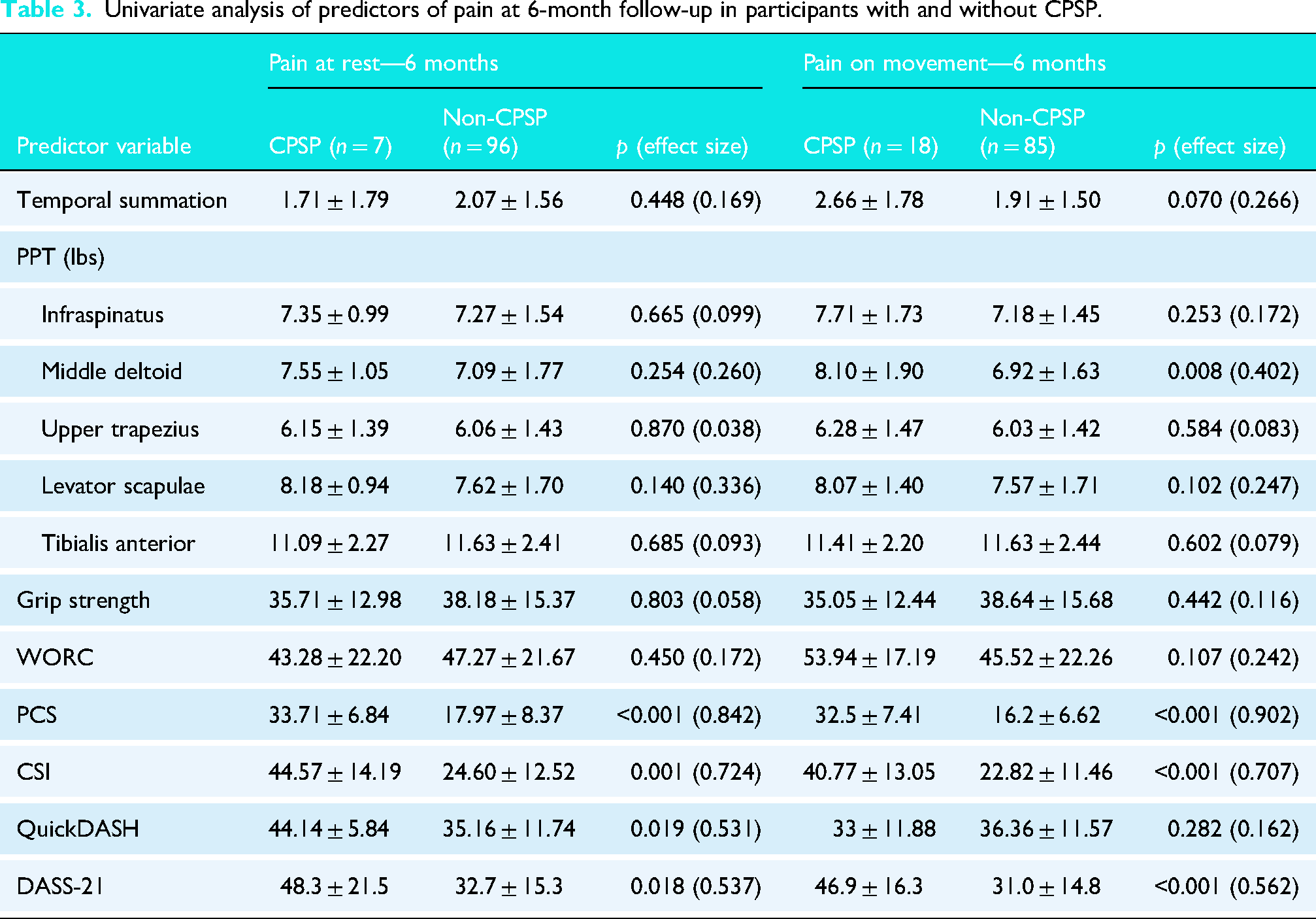
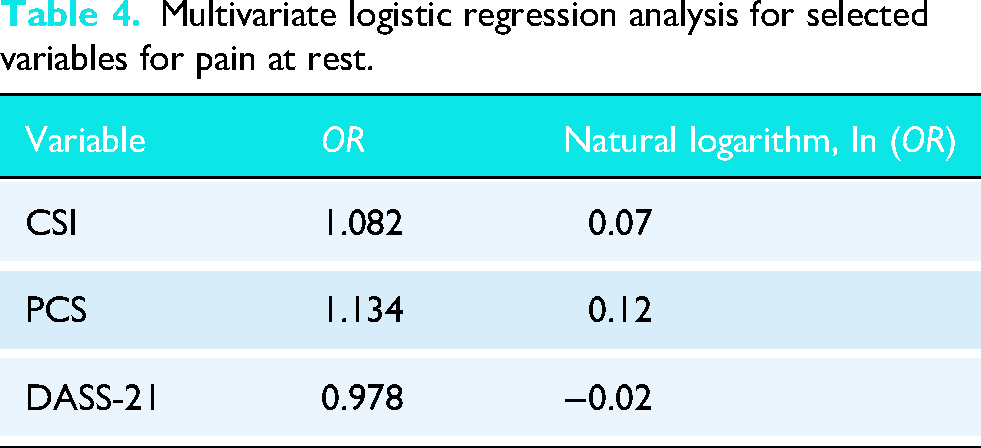
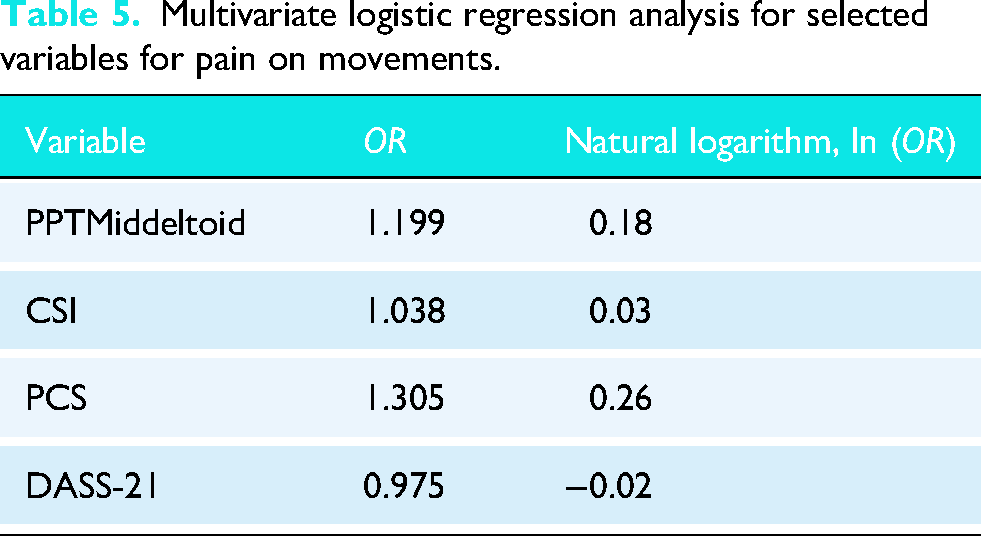
The results of the multivariate logistic regression for pain at rest and pain on movements are depicted in Tables 4 and 5, respectively. The CPSP subgroup exhibited significantly higher scores on CSI (p < 0.001), DASS-21 (p = 0.001), and PCS (p < 0.001), additionally on PPT middle deltoid (p = 0.007), in the CPSP on movements group compared to the non-CPSP group. For all other variables, including grip strength, WORC, TS, Quick DASH, and PPT over other muscles, no statistically significant differences were observed between the CPSP and non-CPSP groups. Based on binomial logistic regression coefficients, two equations were developed to predict the probability of CPSP in the shoulder following ARCR Figure 3.
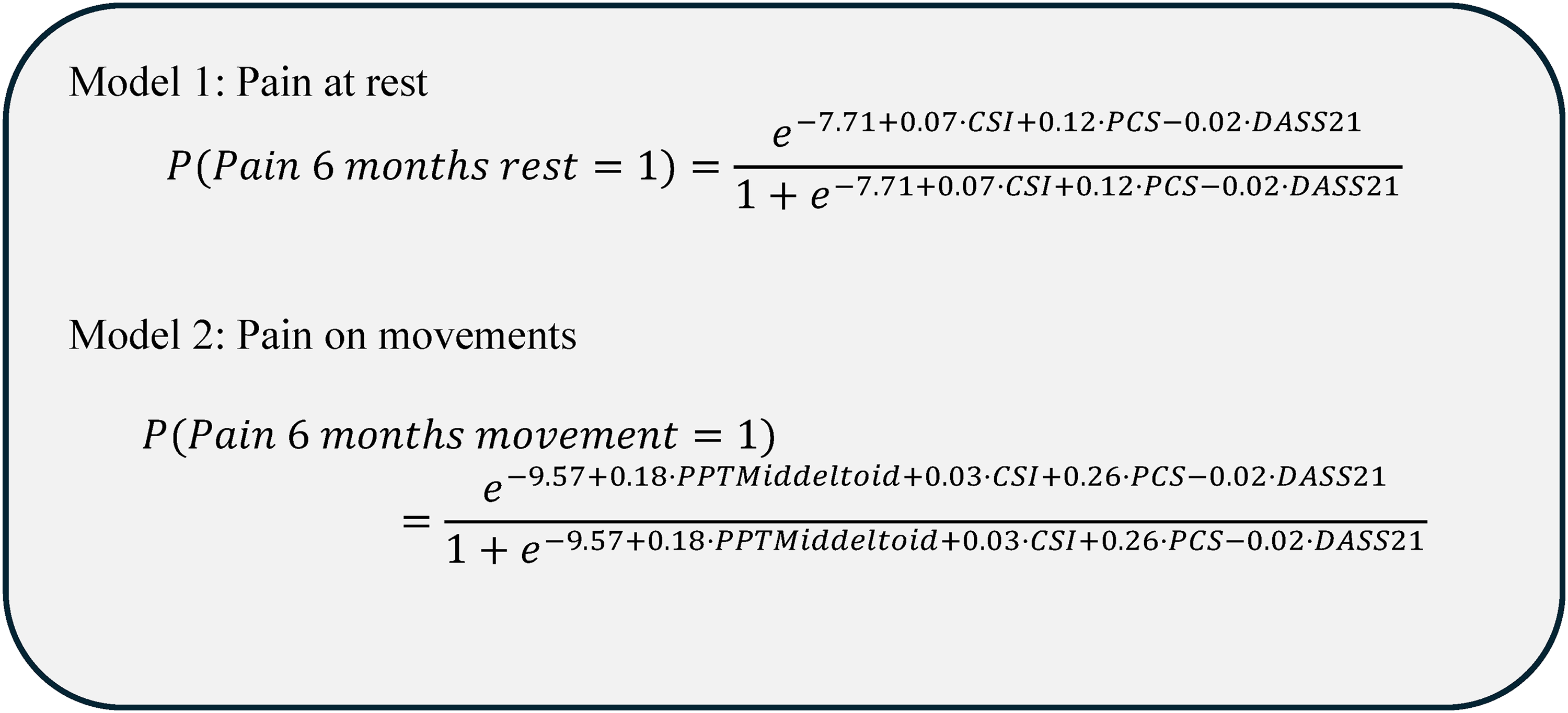
Prediction models for CPSP at rest and during shoulder movements.
Multivariate logistic regression analysis for selected variables for pain at rest.
Multivariate logistic regression analysis for selected variables for pain on movements.
There was a significant decline in the level of pain both at rest and on movement postoperatively (Figures 4 and 5); the magnitude of the change was greater for pain on movement than for pain at rest. The short-term rise, which occurs at around six weeks, has also been described in previous work, where it is thought to relate to surgical debridement and tissue repair, which may trigger inflammatory responses and discomfort during the early healing phase.
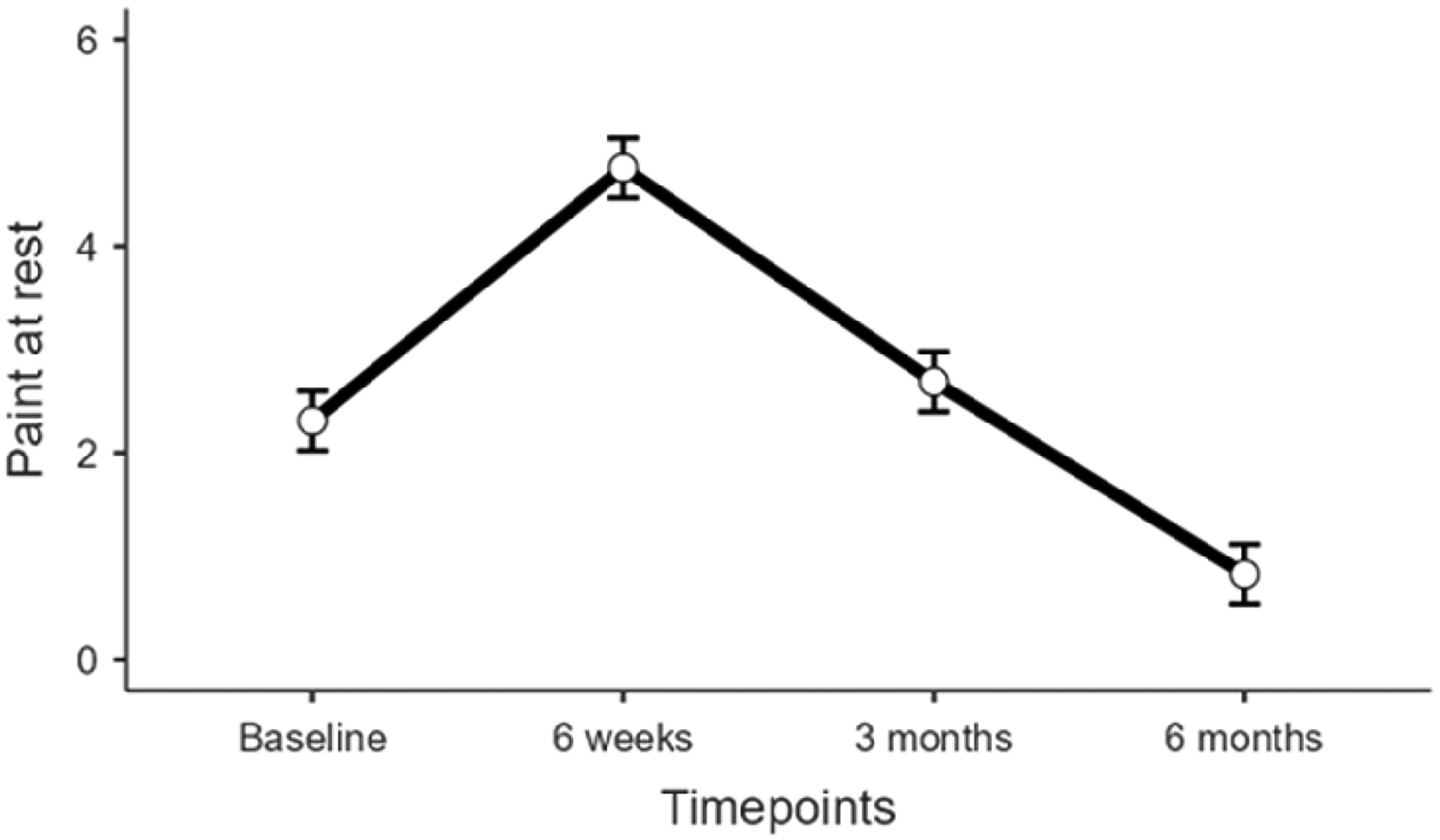
Change in pain at rest through the course of the study.
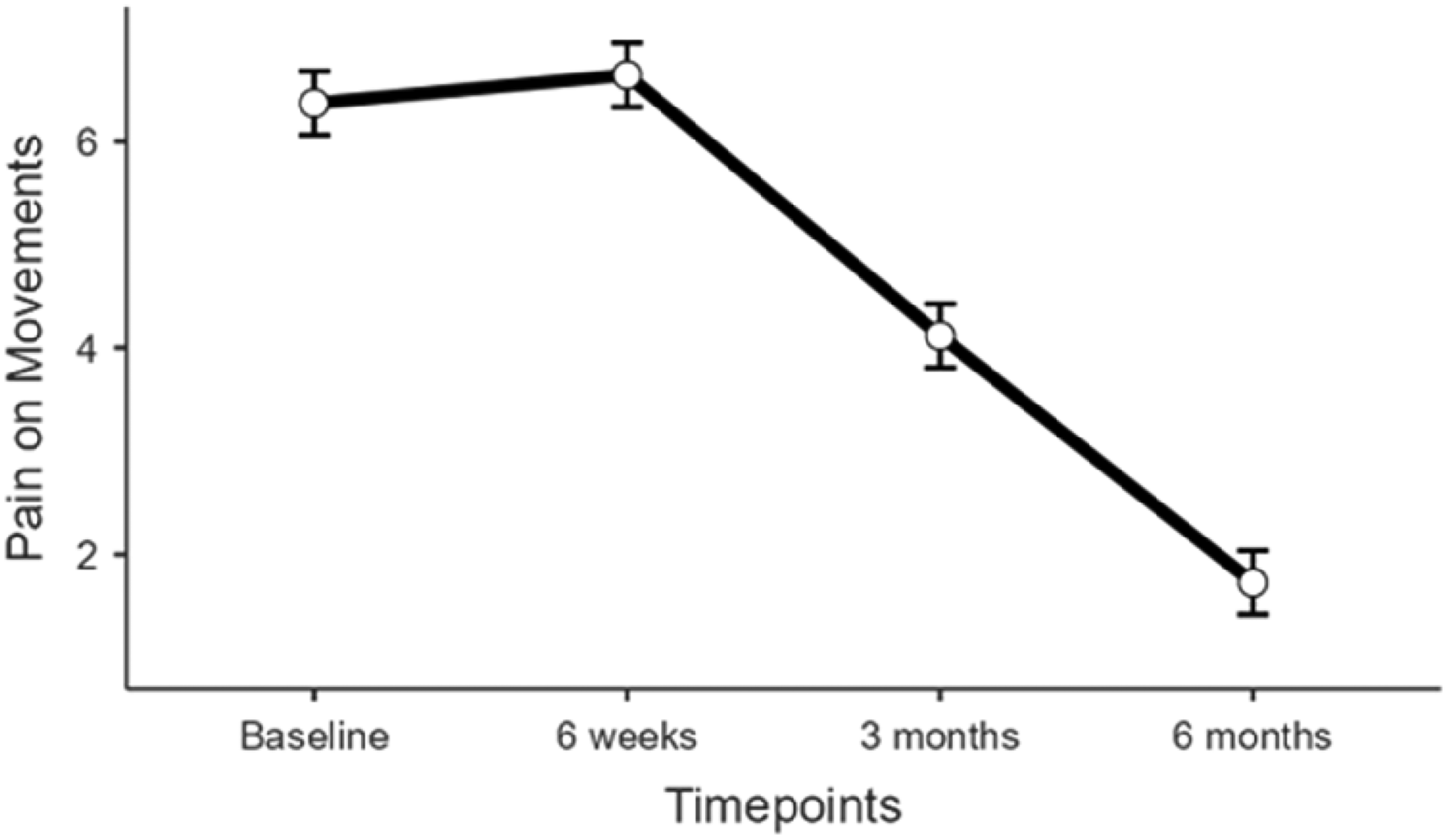
Change in pain on movements through the course of the study.
For each predictor, a bivariate analysis was conducted. The final model includes the statistically significant factors, and based on the final model, the receiver operating characteristic curve (ROC) analysis was performed. The results of the area under the ROC curve are identified for pain at rest (0.93) and pain on shoulder movements (0.94), as shown in Figures 6 and 7, respectively, indicating that the model is a good fit.
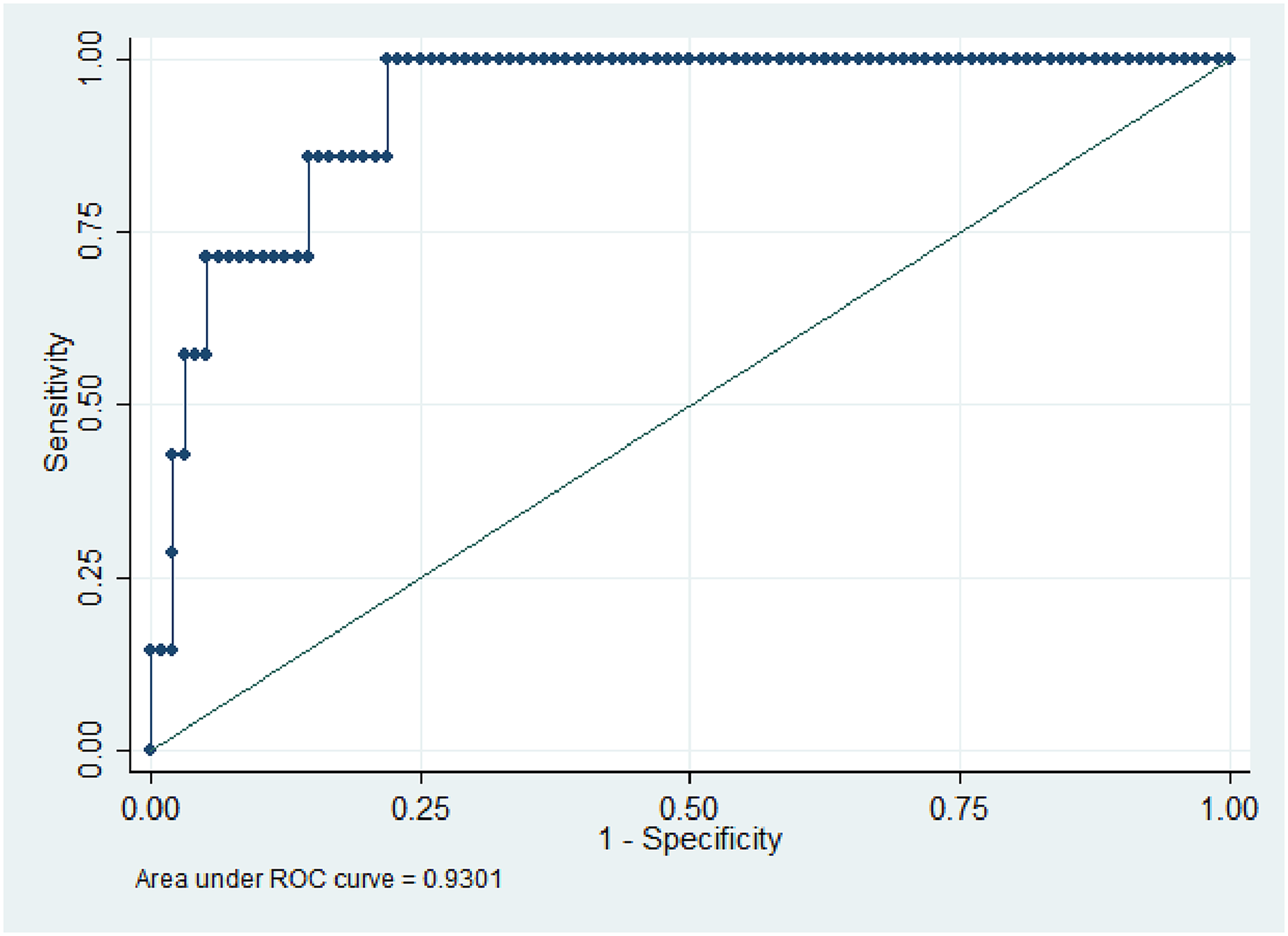
Receiver's operating characteristic curve for pain at rest.
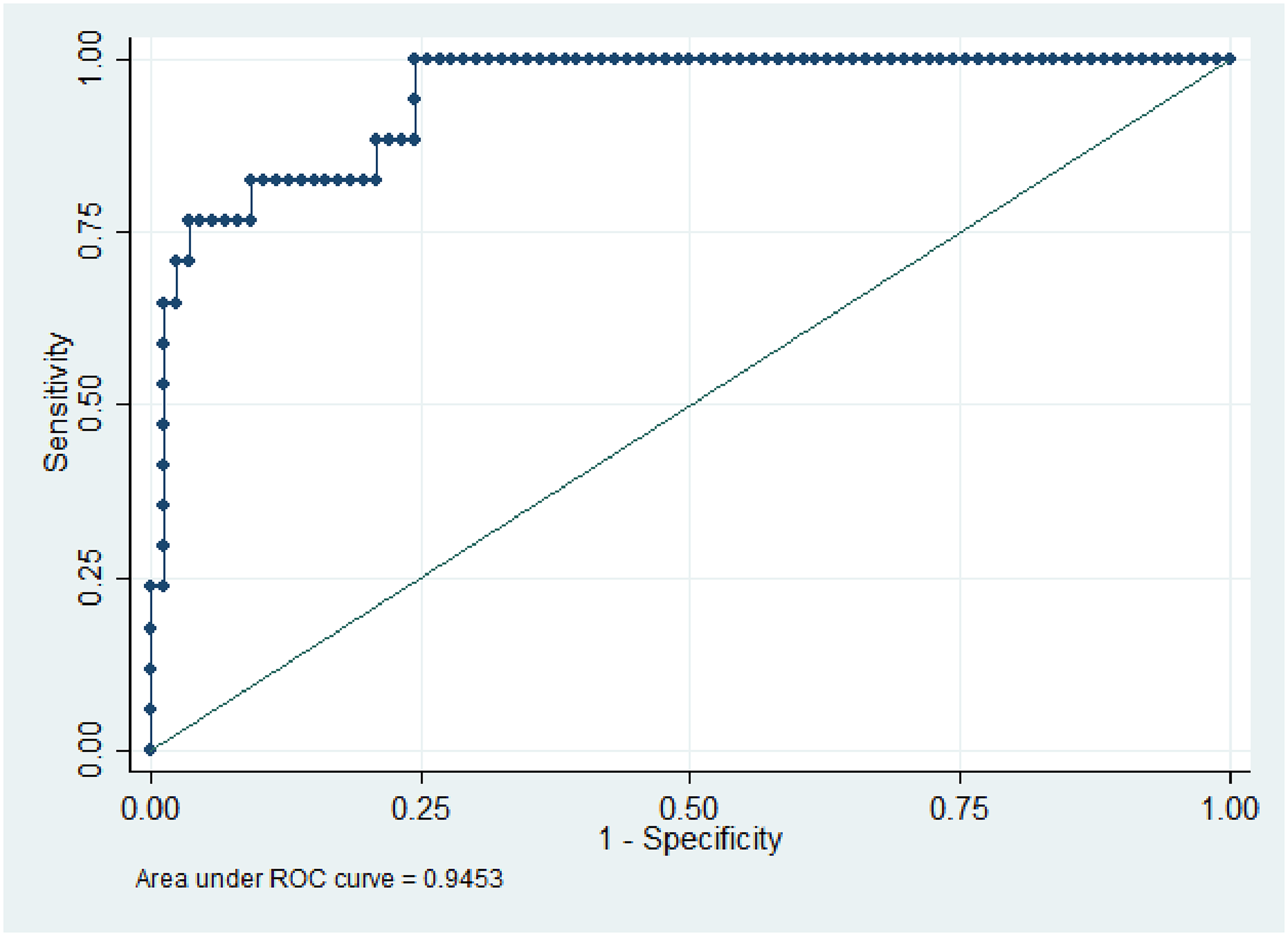
Receiver's operating characteristic curve for pain on movements.
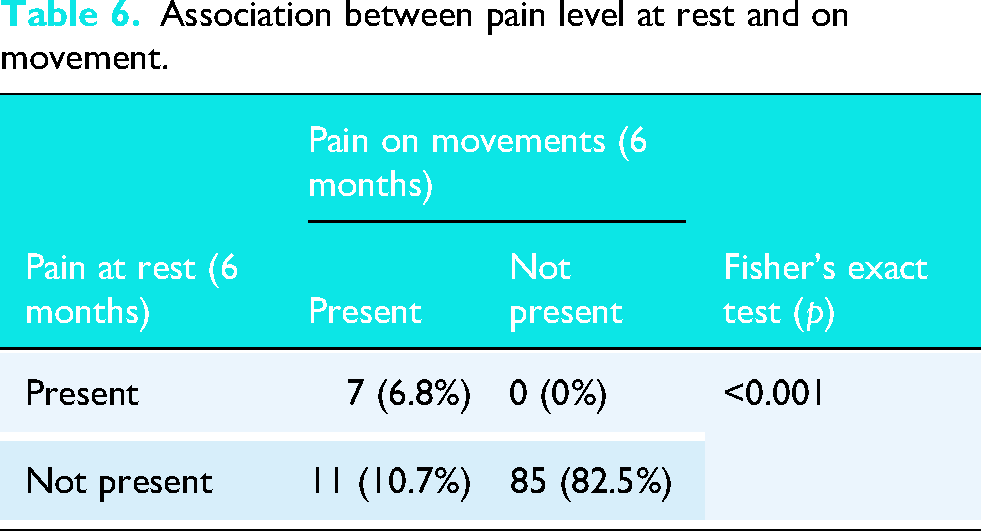
Fisher's exact test was conducted using pain at rest and pain during movement over a period of 6 months, revealing an association between pain at rest and pain on movements (p < 0.001). Additionally, 82.5% of the participants experienced no pain during either rest or movement (Table 6).
Association between pain level at rest and on movement.
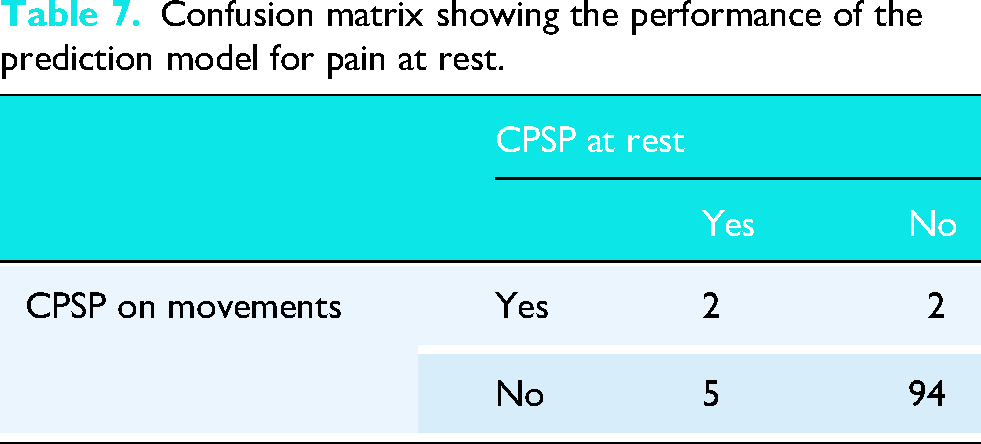
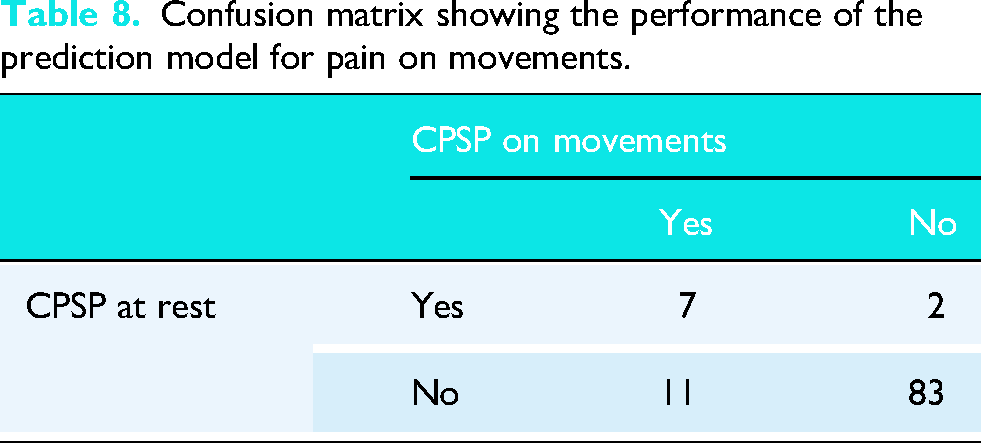
Based on the ROC curve analysis, the optimal cutoff value for the predicted probability was 0.5. The results of the area under the ROC curve analysis, the optimal cutoff value for the predicted probability was 0.5. Individuals with a predicted probability of less than 0.5 are classified as not having CPSP, while those with a predicted probability of 0.5 or higher are classified as having chronic pain. The detailed results are presented in the confusion matrix below Tables 7 and 8.
Confusion matrix showing the performance of the prediction model for pain at rest.
Confusion matrix showing the performance of the prediction model for pain on movements.
The overall accuracy of the predictive model for pain at rest was 93.20%, with a sensitivity of 28.57% and a specificity of 97.92%. A positive predictive value of 50.00% and a negative predictive value of 94.95%.
The overall accuracy of the predictive model for pain on movements was 92.23%, with a sensitivity of 64.71%, specificity of 97.67%, positive predictive value of 84.62%, and negative predictive value of 93.33%.
Discussion
This study contributes to and validates the existing research indicating a relationship between ARCR and CPSP. Identifying the predictors of CPSP can yield valuable insights into refining the assessment and management with the objective of improving patient outcomes after ARCR. In designing a prediction model for the risk of CPSP 6 months after primary ARCR, our final model included three pain at rest predictors: CSI, PCS, and DASS-21. By devising a clinically relevant prediction model to describe this association, CPSP on shoulder movements can be predicted using CSI, PCS, DASS-21, and PPT over the middle deltoid. The clinical utility of the present model incorporates clinically available predictors based on preoperative data, rendering them suitable for screening and thus able to inform pre-surgical intervention strategies.
Consistent with previous literature, we found that pain on movement was more prevalent (n = 18, 17.5%) than pain at rest (n = 7, 6.8%) 6 months post-surgery. This supports the notion that movement-evoked pain may be a more sensitive marker of CPSP and may reflect ongoing central sensitization mechanisms. 39 Importantly, although pain levels declined over time, a subset of patients continued to experience clinically relevant pain, underscoring the need for early risk stratification.
Participants who developed CPSP had significantly higher scores on the PCS, CSI, and DASS-21 scales and elevated PPTs at the middle deltoid muscle, indicating increased central sensitivity and psychological distress. These findings align with the biopsychosocial model of chronic pain, suggesting that persistent pain could be attributable to altered pain processing and psychological comorbidities.40,41 Our prediction models for CPSP at rest and movement demonstrated excellent discriminatory ability, with AUC's of 0.93 and 0.94, respectively. The model for movement-related CPSP showed superior sensitivity (64.7%) and positive predictive value (84.6%) compared to the model for pain at rest, which had a lower sensitivity (28.6%). This discrepancy highlights the greater complexity of predicting CPSP at rest and the potential utility of focusing on movement-evoked pain in clinical evaluations.
The CSI is a crucial predictor of CPSP following ARCR, and this study supports its applicability. The efficacy of CSI as a useful measure for central sensitization in this population is supported by the substantial correlation seen between elevated preoperative CSI scores with pain during movement and at rest 6 months after surgery. Higher CSI scores have been shown to strongly correlate with the development and maintenance of chronic pain in musculoskeletal disorders.42,43 Patients categorized as centrally sensitized by the CSI had considerably higher pain intensity and lower psychological evaluations, according to a cross-sectional study on unilateral chronic shoulder pain. 18 As reported by CSI, patients with RC tears have a significant prevalence of central sensitization syndrome, with rates of roughly 39% in large clinical cohorts and even higher in specific subgroups, such as those with concurrent mental health symptoms and longer symptom duration. 44
Catastrophizing is a psychological factor characterized by a negative cognitive distortion realized during actual or anticipated painful experiences, and this type of thinking can exacerbate the perception of pain and contribute to the chronicity of pain conditions. Pain catastrophizing is a strong predictor of CPSP. A retrospective cohort study found that higher preoperative pain catastrophizing scores predicted persistent pain after ARCR, independent of other psychological and surgical factors. 7 A systematic review revealed that 55% of studies found a significant association between pain catastrophizing and CPSP, especially following musculoskeletal surgery, with affected patients facing up to double the risk of persistent pain after their procedure. 45
An expanding body of research emphasizes the significant influence of psychological factors, particularly anxiety and depression, on post-surgical outcomes in orthopedic procedures. Systematic reviews and meta-analyses have consistently indicated that preoperative psychological distress is a strong predictor of CPSP, diminished functional outcomes, and reduced patient satisfaction.46,47 Evidence from prospective studies underscores the predictive capacity of postoperative anxiety, depression, and catastrophizing on CPSP after joint arthroplasties and spinal surgical procedures.48,49 Specifically, in ARCR, preexisting anxiety and depression have been associated with elevated postoperative pain and poorer clinical recovery. 50 A narrative review further suggests that unaddressed psychological comorbidities in orthopedic trauma patients can impede rehabilitation and extend recovery time, highlighting the need for integrated preoperative screening and mental health management. 51 Collectively, these findings reinforce the clinical importance of addressing psychological health to optimize surgical outcomes and minimize the risk of persistent postoperative pain.
While considering PPT over the middle deltoid, we found that the pain threshold was higher in this muscle for the pain-on-movement group. This contrasts with the literature describing a lower PPT in chronic pain participants. 52 We cannot explain this finding at the moment. Still, this unusual observation may be due to specific characteristics of the population studied, which can influence PPT values and the interpretation of pain sensitivity in chronic pain conditions.
Despite the strong model performance, the sensitivity of prediction model for pain at rest was modest. This could be attributed to the small number of patients reporting CPSP at rest (n = 7), which limits the power to detect all true cases. Nevertheless, both models’ high specificity and negative predictive values suggest that they may be beneficial for ruling out the risk of CPSP in clinical practice. These findings have important clinical implications. Preoperative screening using the prediction model can help with early identification of patients at risk for developing CPSP. Early intervention strategies aimed at central sensitization and psychological distress, such as pain neuroscience education, cognitive-behavioral therapy, or neuromodulatory approaches, may help reduce the progression to CPSP.53,54
Strengths and limitations
The model was created using a group of patients who were otherwise healthy and experienced only CPSP. Preoperative opioid medication history was not collected, and medication used postoperatively was not considered. The other limitation of our study is the lack of comprehensive data on concomitant procedures performed during surgery, which were not examined as predictors of outcomes. Similarly, individualized rehabilitation approaches, adherence to rehabilitation protocols, and the incidence of secondary postoperative stiffness were not documented or analysed. The relatively small number of patients developing CPSP, particularly at rest, may limit the generalizability and stability of the predictive model. Although we used validated tools for psychosocial and sensory assessment, other potential factors such as sleep disturbance, coping strategies, or inflammatory markers were not assessed. Before this preoperative prediction rule can be used clinically, external validation studies in patients from different clinical settings with and without underlying comorbidities are required.
Implications
External validation of our prediction model could establish a clinically valuable tool for identifying individuals at elevated risk of developing CPSP following ARCR. A comprehensive preoperative assessment, including screening for psychological factors such as pain catastrophizing, depression, anxiety, and stress, may facilitate timely referral to mental health professionals and improve patient outcomes. Such risk stratification would enable the targeted allocation of preventive interventions to those most vulnerable to CPSP.
Conclusion
In summary, the clinical prediction model presented here is a valuable tool for assessing preoperative risks and can also serve as a framework for developing personalized pain management strategies. By integrating the model's findings into clinical practice, we can move towards a more precise, patient-centered, and informed approach towards assessing and managing postoperative pain.
Footnotes
Abbreviations
Acknowledgments
The authors would like to thank all the participants for their valuable time and participation in our study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.