
Abstract
Background
This systematic review aimed to evaluate prognostic factors associated with outcomes following needling and shockwave therapy (SWT) for RCCT rotator cuff calcific tendinitis (RCCT).
Methods
MEDLINE, EMBASE, and CENTRAL databases were searched for studies on prognostic factors in RCCT treated with needling or SWT that included multivariable analyses. The risk of bias was assessed using the Quality in Prognosis Studies tool, and the quality of each prognostic factor was evaluated using a modified Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework.
Results
13 studies involving 1693 shoulder patients were included, of which 11 evaluated needling and two evaluated SWT, all showing moderate-to-high risk of bias. Across needling studies, 32 variables were evaluated in multivariable models, with five showing potential predictive value for treatment success based on GRADE quality: larger calcification size, Type III Gartner-Heyer (fluid-like) classification, shorter distance between the subacromial bursa and deposit, normal bursal appearance, and fewer needling sessions. In SWT studies, four variables were analysed, with Type III calcifications and shorter symptom duration associated with better outcomes.
Discussion
Certain disease- and procedural-related factors may predict better outcomes with needling or SWT for RCCT, though the evidence is limited and requires prospective validation to refine patient selection.
Level of Evidence
III.
Introduction
Rotator cuff calcific tendinopathy (RCCT) is a common cause of atraumatic shoulder pain, affecting up to 20% of adults, particularly those in middle age.1–3 It is characterized by the deposition of calcium hydroxyapatite crystals within the rotator cuff tendons, most frequently the supraspinatus.4,5 Given the typically self-limiting course of the disease, initial management is conservative, involving non-steroidal anti-inflammatory drugs (NSAIDs), activity modification, physiotherapy, and steroid injection.6–8 However, more than 50% of patients continue to experience pain and functional limitations despite conservative care. 9
In such cases, more targeted interventions such as ultrasound-guided needling have become an established minimally invasive treatment for RCCT.10,11 Needling involves the mechanical disruption and aspiration of calcific deposits to relieve symptoms and is typically done under ultrasound guidance. In a recent network meta-analysis of randomized trials, Arirachakaran et al. found that needling yields superior short-term outcomes compared to other non-surgical modalities such as steroid injection. 12 However, authors report that clinical outcomes after needling vary widely.13,14 Shockwave therapy (SWT) is another widely used non-invasive modality for RCCT that promotes tissue regeneration and calcium resorption through biological stimulation.15,16 Although multiple randomized controlled trials have shown SWT to be effective compared to other conservative treatments, the long-term outcomes remain inconsistent.17–20
Despite the high prevalence of RCCT and prior reviews comparing the effectiveness of needling and SWT as treatment modalities, there remains limited consolidated evidence identifying which factors predict clinical outcomes for these interventions.21–24 Given the use of both modalities in clinical practice, a deeper understanding of prognostic factors for each is essential to tailor treatment plans accordingly. Thus, this study aims to provide the first systematic review to comprehensively identify and describe prognostic factors associated with functional outcomes following needling interventions or shockwave therapies for RCCT, with a focus on variables supported by multivariable analyses.
Methods
This systematic review was conducted based on the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines. 25 The protocol was registered on PROSPERO on June 27, 2025 (CRD420251073642).
Search strategy
A systematic search was performed across MEDLINE, Embase, and CENTRAL databases from their inception to 6 January 2025. Additionally, bibliographic references of relevant articles were screened for eligible articles. The search strategy was based on the key terms ‘calcific tendinopathy’, ‘needling’, and ‘shockwave’ (Supplemental Table 1).
Included studies met the following criteria: (1) primary longitudinal design, (2) adult patients (>18 years) with rotator cuff calcific tendinopathy, (3) evaluation of needling interventions or shockwave therapies, and (4) reporting on multivariable factor analyses for treatment outcomes. Studies were excluded if they were (1) review articles, meta-analyses, conference abstracts, or case reports, (2) non-English publications, or (3) studies only reporting univariable analysis.
Study screening and selection
Search results were imported into Covidence (Veritas Health Innovation, Melbourne, Australia), a web-based platform used for managing systematic reviews. Three reviewers (AMA, OSA, and EO) independently screened titles, abstracts, and full-text articles. Any disagreements were discussed and resolved by consensus, with input from a senior author (AH) when needed.
Data extraction
Data were extracted using a standardized spreadsheet created in Google Sheets (Google LLC). Two reviewers (AMA and OSA) independently collected information on study characteristics, prognostic factors, and outcomes. For each study, the reported prognostic factors along with their definition and measurement, type of statistical analysis, outcome assessed and time point of assessment, effect size and direction, statistical significance, and, where available, the accuracy of the prognostic factor were extracted. The extraction process was guided by an adapted version of the Checklist for Critical Appraisal and Data Extraction for Systematic Reviews of Prediction Modelling Studies (Online Resource 1: Supplemental File). 26
Risk of bias assessment
The risk of bias was assessed independently by two authors (AMA and OSA) using the Quality in Prognosis Studies (QUIPS) tool, which covers six domains: study participation, study attrition, measurement of prognostic factors, measurement of outcomes, adjustment for other prognostic variables, and statistical analysis and reporting. 27 For the domain related to confounding control (adjustment for other prognostic variables), all studies were rated as having at least moderate risk of bias, given the lack of a standardized set of covariates for multivariable analysis. An overall rating of ‘low’ risk was given when all domains were low risk; ‘moderate’ when at least one domain was moderate and none were high; and ‘high’ when one or more domains were rated as high risk.
Quality of evidence
Effect estimates were extracted as reported in the original studies. The overall quality of evidence for each prognostic factor–outcome relationship was assessed using a modified version of the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) framework, adapted for use in prognostic research. 28 GRADE ratings were assigned as ‘low’, or ‘very low’, reflecting the confidence that the observed association between the prognostic factor and the outcome represents the true effect. In keeping with existing guidance, we did not upgrade quality for dose-response or large effect sizes, as such criteria are rarely applicable in prognostic factor reviews. 28 Consistent with prior prognostic shoulder studies, we focused our judgment on the inconsistency items across different studies. 29 When 50% or more of the studies had the same direction of findings, we ranked the overall quality of evidence as ‘low’. Factors supported by evidence rated as ‘low’ quality were narratively summarized in the results. Two reviewers (AMA and OSA) independently applied GRADE ratings for each prognostic factor-outcome relationship, with disagreements resolved by a senior author (AH).
Results
Study selection
The literature search yielded 2973 studies for initial screening, of which 318 underwent full-text review (Figure 1). Ultimately, 13 studies comprising 1693 shoulders met the inclusion criteria.9,30–41 Of these 13 studies, 11 studies focused on needling and two studies on SWT (Table 1). Studies were published between 2009 and 2024 and conducted across eight countries, with Italy being the most common country of origin (3/13).
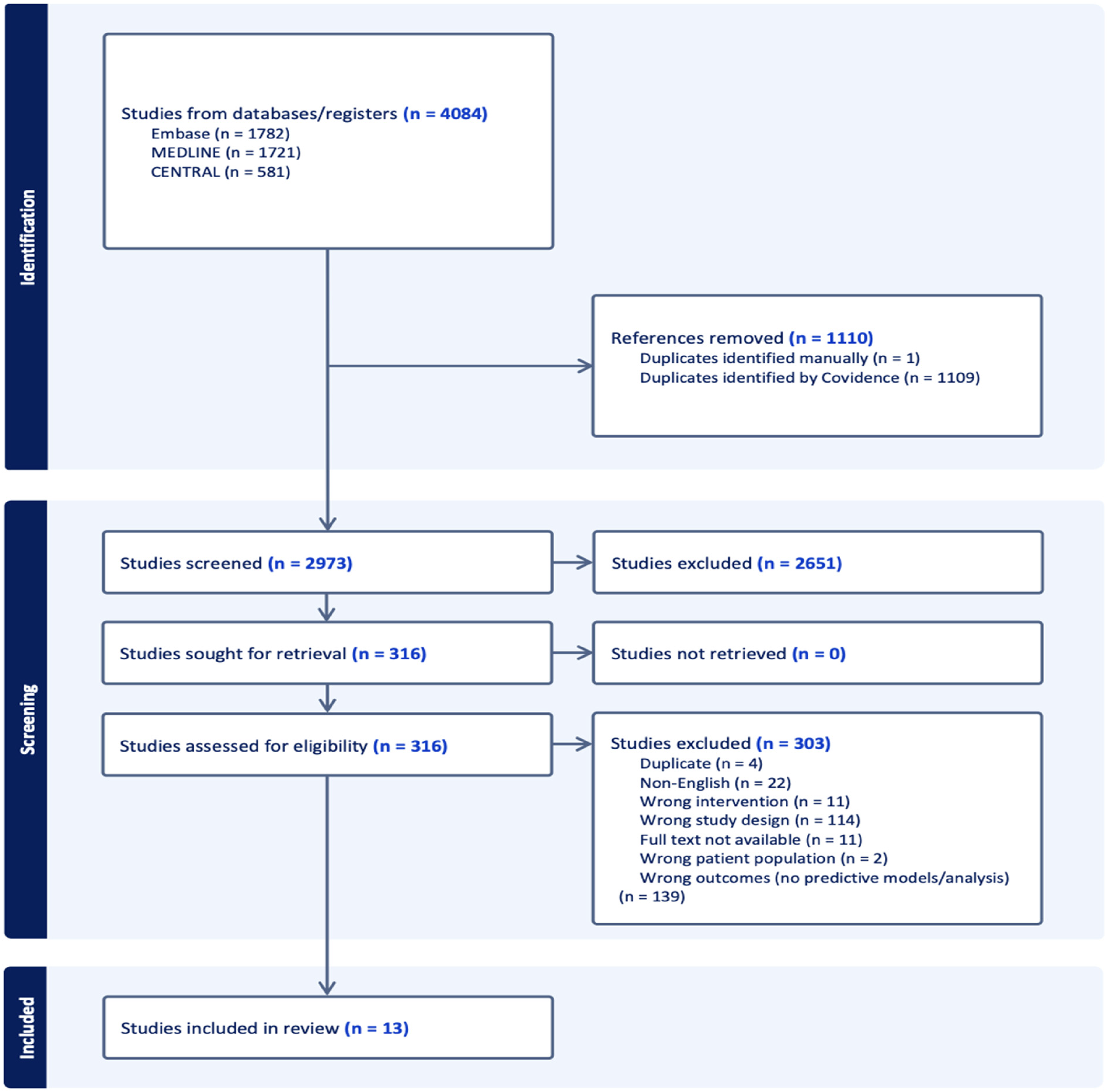
PRISMA flow diagram of included studies.
Study characteristics.
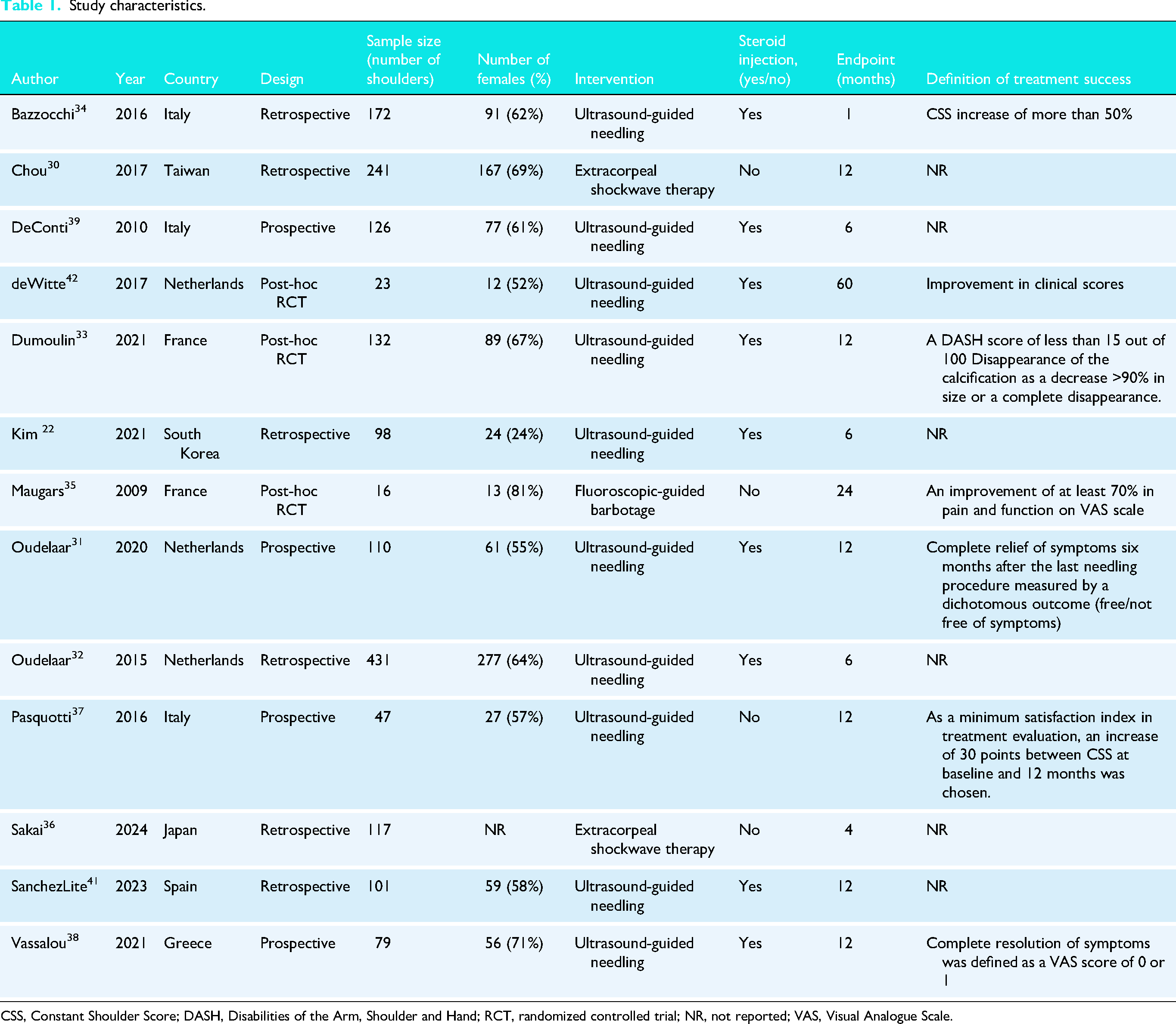
CSS, Constant Shoulder Score; DASH, Disabilities of the Arm, Shoulder and Hand; RCT, randomized controlled trial; NR, not reported; VAS, Visual Analogue Scale.
Quality of evidence
The overall quality of evidence across prognostic factor–outcome pairs ranged from low to very low (Table 3). Despite this, several factors consistently showed trends suggesting a potential association with clinical response to needling and SWT. However, the strength of these associations was limited by imprecise and inconsistent effect estimates, and a high risk of bias across studies, which contributed to downgrading in the GRADE assessment (Table 3).
Risk of bias
Six needling studies were rated as having an overall moderate risk of bias, while the remaining studies were classified as high risk (Figure 2). The ‘Statistical analysis and reporting’ domain was the most frequently downgraded area in the QUIPS assessment (Supplemental Table 3). This was primarily due to inadequate reporting of univariable and multivariable effect estimates, with many studies selectively reporting results for only a subset of assessed prognostic factors. The two SWT studies were rated as having an overall high risk of bias due to the same reasons.
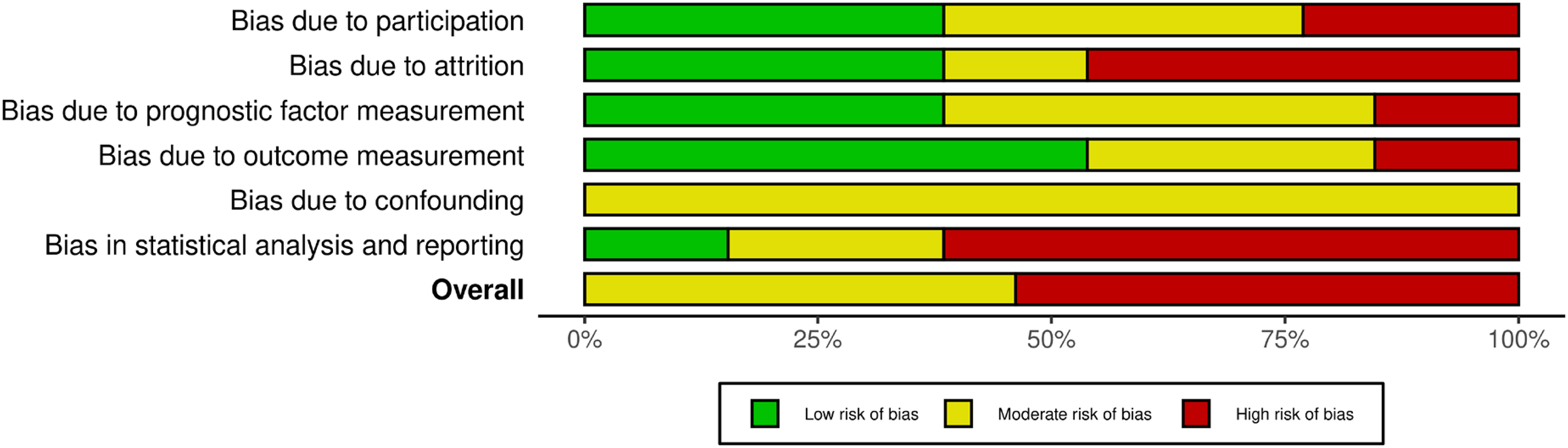
QUIPS risk of bias analysis.
Needling studies characteristics
There were 11 needling studies9,31–35,37–41 comprising a total of 1335 shoulders (59% female). Among which, five were retrospective, four were prospective, and two were post-hoc randomized controlled trials (Table 1). All procedures were performed under ultrasound guidance except for one study,1–6 which used fluoroscopy. In nine studies, a corticosteroid injection was administered following needling, while the remaining two studies35,37 used NSAIDs and physical therapy for post-procedural care (Supplemental Table 2). Follow-up durations ranged from one to 60 months. Eight studies reported the location of calcific deposits, with the supraspinatus tendon being the most frequently involved site, followed by the infraspinatus.
Definitions of treatment success were reported in seven studies,31,33–35,37,38,42 and varied across studies, but generally reflected improvement in validated functional outcome scores, such as the Constant Shoulder Score, VAS, and DASH (Table 1). The remaining five studies did not define a specific threshold for success but still reported functional scores or the extent of calcium resorption as reference points for post-treatment evaluation.
Shockwave therapy studies
Two retrospective studies,30,36 comprising a total of 358 shoulders (69% female), evaluated the use of SWT. Both studies used focused high-energy extracorporeal shockwave therapy, with energy flux densities ranging from 0.25 to 0.32 × mJ/mm2 (Supplemental Table 2). The number of sessions varied from two to nine. Neither of the studies included adjunct corticosteroid injections. Follow-up durations ranged from 4 to 12 months. Both studies did not state a definition of treatment success or failure but used the Constant Shoulder Score and resorption of calcific deposits as reference points.
Distribution of prognostic factors across needling studies
Five31–34,40 needling studies conducted univariate analysis, collectively evaluating 29 distinct prognostic variables (Table 2). The most frequently evaluated prognostic factors among these analyses were symptom duration and calcification classification, each examined in three studies. Among these 29 variables, 12 were carried forward to multivariable analyses.
Summary of prognostic factors in univariate analyses.
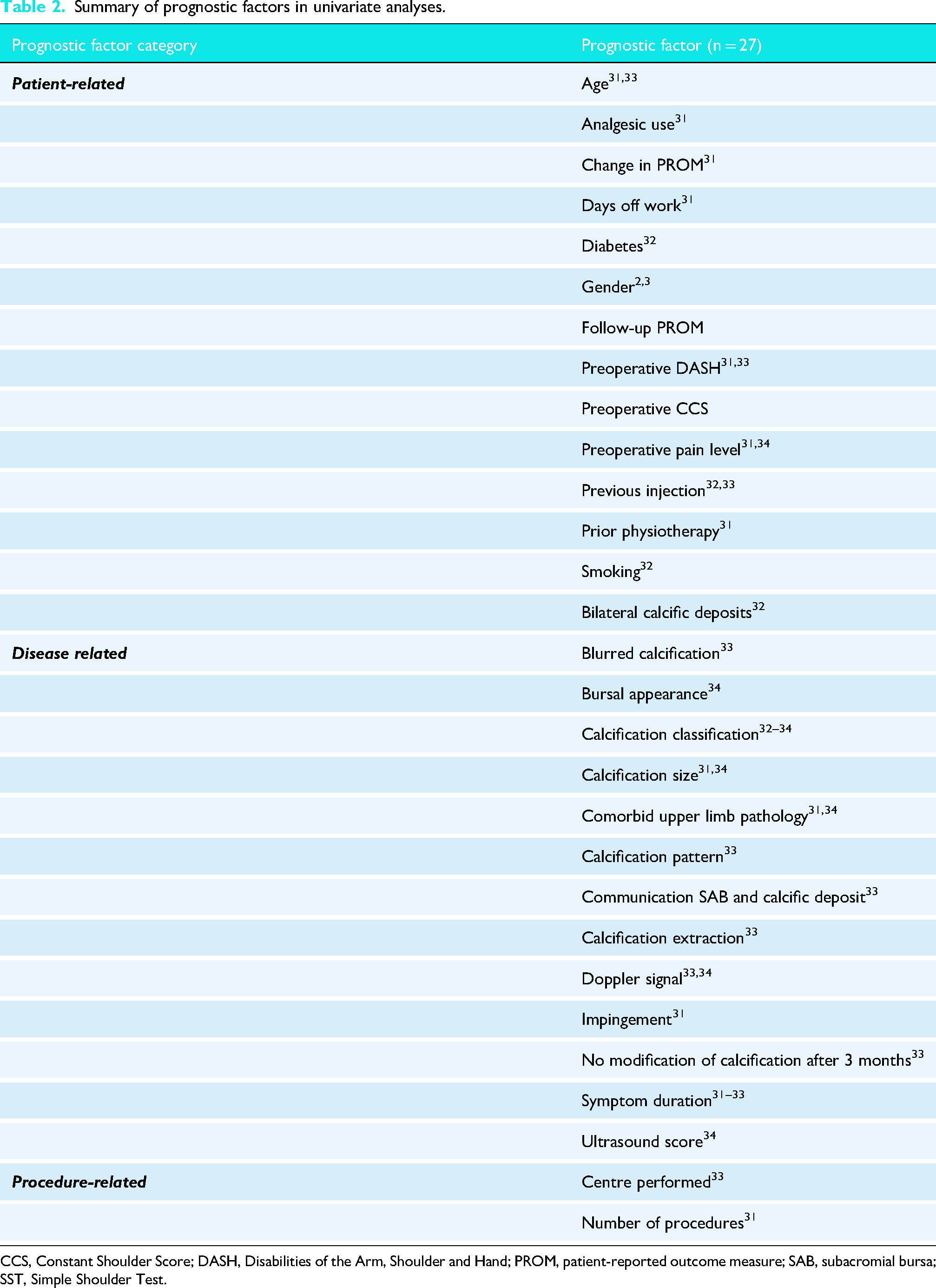
CCS, Constant Shoulder Score; DASH, Disabilities of the Arm, Shoulder and Hand; PROM, patient-reported outcome measure; SAB, subacromial bursa; SST, Simple Shoulder Test.
Across multivariable models, 32 distinct prognostic factors were reported (Table 3). Calcification classification remained the most commonly evaluated prognostic factor among these models, analysed in seven studies.32–35,37–39,42 Preoperative pain level was the most frequently assessed patient-related variable, appearing in four multivariable analyses.31,32,35,38
Summary of prognostic-factor outcomes across multivariable analyses.
+, Number of significant effects with a positive value ; 0, number of non-significant effects; -, number of significant effects with a negative value. CSS, Constant Shoulder Score; DASH, Disabilities of the Arm, Shoulder and Hand; FAS, French Society of Arthroscopy classification; GRADE, Grading of Recommendations Assessment, Development, and Evaluation; MRI, magnetic resonance imaging; NRS, Numeric Rating Scale; PROMs, patient-reported outcome measures; QoL, quality of life; SAB, subacromial bursa; SWT, shockwave therapy; US, ultrasound; VAS, Visual Analogue Scale.
Distribution of prognostic factors across SWT studies
No univariate analyses were conducted among the SWT studies. Four distinct prognostic variables were assessed in multivariate analyses, including symptom duration, calcification classification, calcification size, and blood flow around the deposit.
Prognostic factors in needling studies
Demographic factors
Several significant demographic predictive factors were identified in individual studies (Online Resource 1: Supplemental File). Bazzocchi et al. found that hypothyroidism and cardiovascular disease were each significantly associated with worse post-treatment pain, while concomitant upper limb pathology was paradoxically associated with improved pain outcomes. 34 Similarly, Sánchez-Lite et al. reported that the presence of upper limb pathology was linked to significantly higher odds of clinical response (OR 4.95; 95% CI, 1.05–24.47; P = .044). 41 Maugars et al. observed that manual labour and a greater number of days off work were both associated with higher postoperative pain levels. 35 Oudelaar et al. found that smoking daily for at least one year increased failure rates (OR 1.70; 95% CI, 1.00–2.70; P = .040). 32 Lastly, Kim et al. noted that calcification involving the dominant arm was significantly associated with an increased likelihood of requiring repeat needling procedures (OR 4.08; 95% CI, 1.03–16.08; P = .045). 40 As each of these factors was only reported in a single study, they were not evaluated using GRADE and require further investigation to confirm their prognostic relevance.
Bursal appearance
Two studies37,39 assessed the association between bursal appearance at baseline and needling success (Table 3). In one study, 39 patients with normal-appearing bursae on baseline ultrasound had significantly greater improvement in Constant scores compared to those with thickened or fibroadhesive bursae (P < .0001) (Online Resource 1: Supplemental File). The other reported a similar trend, with normal bursal appearance associated with greater odds of improvement relative to fibroadhesive bursae (OR, 3.393; 95% CI, 0.554–20.786), although this finding did not reach statistical significance (P = .187). 37 These results suggest that normal appearing bursa may be linked to improved functional outcomes following needling.
Calcification size
Associations between baseline calcification deposit size and patient-reported outcomes were examined in multivariable analyses across four needling studies31,35,38,41 (Table 3). One study 31 reported significant associations between larger calcification size and improvement in EQ-5D (β = 0.006, P = .011) and DASH (β = 0.313, P = .032) scores at 12 months (Online Resource 1: Supplemental File). Another study 38 reported that larger size was significantly associated with lower post-treatment VAS pain scores at 12 months (β = –0.082, P < .001) and a higher likelihood of complete pain resolution (OR, 1.207; P = .014). A third study assessed calcification size categorically and found higher odds of clinical response with larger deposits (OR, 3.529 for 11–20 mm vs. 5–10 mm), though the result did not reach statistical significance (P = .276). 41 Overall, these findings support an association between larger calcification size at baseline and better patient-reported outcome measured (PROMs) following needling.
Calcification classification
Eight multivariable analyses across four studies reported significant associations between the calcification classification and PROMs (Table 3, Online Resource 1: Supplemental File). One study 34 reported that Types II–III Gartner-Heyer showed the greatest improvement in Constant score at 1 month. Another study 39 found that Type III calcifications showed the greatest improvement in Constant scores at 6 months (P < .01). A third study 38 found that fluid-type calcifications were significantly associated with higher odds of achieving near-complete pain resolution (VAS < 1) at 12 months (OR, 9.056; 95% CI, 1.24–66.14; P = .03). A fourth study 35 found that Type A (FAS scale) calcifications were significantly associated with poorer VAS outcomes at 24 months, being more prevalent in the failure group than in the success group (49.1% vs. 30.6%; P = .05). These results suggest Gartner-Heyer Type III, or fluid-like calcification deposits are likely prognostic of improved PROMs following needling.
In terms of objective outcomes, one study 32 found that Gartner-Heyer Type I calcifications were significantly associated with a higher likelihood of requiring multiple procedures at 6 months (OR, 3.4; 95% CI, 1.6–7.5; P < .01). Another study 33 found that ‘hard’ calcification types had a significantly lower risk of calcification disappearance at 3 months (OR 0.274, 0.119–0.635, P = .003).
Number of procedures
Two studies31,41 reported significant associations between the number of needling procedures and post-treatment PROMs (Table 3). One study 41 showed that requiring only one aspiration was significantly associated with better clinical response at 12 months (OR, 2.073; 95% CI, 1.140–3.790; P = .017) (Online Resource 1: Supplemental File). The second study 31 reported that undergoing multiple needling procedures was associated with significantly higher pain scores at 12 months, with an average VAS increase of 12.34 points compared to patients treated with a single procedure (P = .009). These results suggested that requiring fewer needling procedures was associated with better PROMs.
Distance between the subacromial bursa and calcification
Two studies33,34 assessed the association between communication between the subacromial bursa (SAB) and the calcific deposit and PROMs (Table 3). Dumoulin et al. found that the presence of communication was associated with a nearly tenfold increase in the odds of achieving calcification disappearance at 12 months (OR, 9.835; 95% CI, 1.977–48.932; P = .005) 33 (Online Resource 1: Supplemental File). Oudelaar et al. similarly reported that a shorter pre-treatment distance between the SAB and the calcification, implying potential communication, was associated with significantly better NRS pain scores at one month (P < .05). 31 These findings suggest that communication between the SAB and the calcification may be predictive of better clinical outcomes following needling procedures.
Prognostic factors in SWT studies
Calcification classification
Multivariable analyses in both SWT studies30,36 identified Type I Gartner-Heyer calcific deposits as negative predictors of treatment success (Table 3). Sakai et al. 36 reported that Type I calcifications were significantly associated with more challenging resorption after 4 months (OR, 5.6; 95% CI, 1.73–13.3; P = .01) (Online Resource 1: Supplemental File). Similarly, Chou et al. 30 found that Type I deposits were independently predictive of worse Constant scores at 12 months (OR, 24.814; 95% CI, 9.417–65.385; P < .001).
Duration of symptoms
Both SWT studies analysed the association between symptom duration and posttreatment outcomes (Table 3). Chou et al. demonstrated that a longer duration of symptoms before SWT was associated with significantly poorer Constant scores (OR, 1.055; 95% CI, 1.016–1.094; P = .006 30 (Online Resource 1: Supplemental File). Sakai et al. reported that shorter symptom duration was significantly associated with a higher likelihood of complete calcium resorption (OR, 1.06; 95% CI, 0.97–1.26; P = .046). 36 These results suggest shorter symptom duration is a likely prognostic factor for better outcomes following SWT.
Discussion
Across 13 studies involving 1693 shoulders, several factors were identified that may help predict patient response to needling and SWT. For needling, larger calcification size, Gartner-Heyer Type III (fluid-like) morphology, a shorter distance between the subacromial bursa and the deposit, normal bursal appearance, and fewer needling sessions were associated with better outcomes. For SWT, shorter symptom duration and Type III calcifications appeared to be favourable predictors. Despite heterogeneity in study design and reporting, several overarching patterns emerged that offer clinically useful insights to help tailor established minimally invasive treatment choices in RCCT.
Prior reviews have focused on the effectiveness of conservative interventions for RCCT, including needling and SWT, with mixed findings regarding comparative efficacy.21–24 The present review examined prognostic factors associated with the outcomes of these treatment modalities. The patient- and disease-specific predictors identified provide complementary insights that may help inform patient selection for non-surgical management of RCCT.
Several studies have examined the influence of deposit characteristics on the prognosis of RCCT.4,7,12,41,43 Ogon et al. identified the presence of a Gartner-Heyer Type III calcific deposit as a predictor of improved pain following nonoperative treatment for RCCT. 7 The present review supports this, highlighting that soft, liquefied, or fluid-like calcifications (e.g., Gartner types II–III) are associated with better PROMs, consistent with the hypothesis, likely because these deposits represent the resorptive phase and are more amenable to mechanical disruption and aspiration.4,45 In contrast, dense or hard calcifications often resist fragmentation, requiring multiple treatment sessions and exhibiting slower or incomplete resolution of symptoms, consistent with findings by Oudelaar et al., who reported that Gartner-Heyer Type I calcifications significantly increased the odds of requiring repeated needling procedures. 32 Similarly, repeat needling itself was associated with poorer outcomes in the present review. While Dummond Junior et al. found that calcific deposits larger than 10 mm were less susceptible to needling and more likely to require surgical intervention, the current review identified larger deposits as a positive prognostic factor for needling outcomes. 43 This may reflect the ease of targeting and evacuating these lesions, a finding consistent with recent observational studies. 43
While various ultrasound parameters have been investigated in RCCT literature, no definitive ultrasound predictors of conservative treatment outcomes have been established.44,46,47 Interestingly, this review identified a new and underreported ultrasound finding, suggesting that the anatomical relationship between the calcification and the subacromial bursa may be influential. Communication or close proximity between the deposit and the bursa is associated with superior symptom relief and higher rates of radiographic resolution after needling. This supports the hypothesis that spontaneous or procedural communication allows more effective of calcific material into the subacromial space, thereby promoting clearance and reducing local inflammation.33,48 Such communication may also indicate a more resorptive phase of the disease, during which needling intervention is likely to be more efficacious. 45 Previous studies have shown that the presence of a positive Doppler signal in shoulder tendons might be a marker for better shoulder pain.44,49–51 While this factor has been explored in the existing literature, it has not been evaluated in multivariable models. Bazzochi et al. found Doppler positivity significant in univariate analysis, whereas Dumoulin et al. highlighted the need for future multivariable analysis to confirm its predictive value in needling.33,34 This review did, however, find that a normal-appearing bursa on ultrasound was associated with better outcomes after needling, suggesting that preserved bursal integrity may reflect a less advanced or less inflamed disease state. These findings highlight the prognostic value of a detailed pre-procedural ultrasound assessment in guiding treatment decisions for RCCT with needling.
While this review focused primarily on needling interventions, SWT is another widely used, non-invasive option for treating RCCT. Although fewer studies evaluating SWT met the criteria for inclusion in the multivariable analysis synthesis, prior trials suggest that overlapping prognostic indicators, such as calcification type, symptom duration, and tendon quality, are present. Notably, shorter symptom duration emerged as a likely predictor of improved outcomes in SWT studies. Notably, however, when evaluated using the GRADE approach, it was found to be less prognostic in needling, with statistical significance reported in only one study, which had a high risk of bias, and overall, the quality of evidence was very low. By contrast, Type I Gartner-Heyer calcifications have been demonstrated to be likely predictive of worse outcomes across both SWT and needling literature, indicating that these dense deposits may be less responsive to either modality. A randomized controlled trial by Louwrens et al. found no differences in clinical outcome between Gartner-Heyer Type I and II calcifications for needling versus SWT treatment. 21
Clinically, these findings offer a more nuanced framework to guide patient counselling and procedural planning for RCCT. The consolidated literature suggests that when available, ultrasound evaluation of deposit morphology, size, and bursal anatomy may help stratify prognosis and tailor follow-up. The present review suggests that patients with smaller deposits, wherein communication between the deposit and SAB cannot be achieved or if the bursa appears degenerated, clinicians may opt for SWT over needling for these patients. Results of the study by Oudelaar et al. demonstrate that previous unsuccessful SWT treatments did not affect the outcome of needling, suggesting needling is therefore also indicated after failure of other therapies for RCCT. 31 The present study indicates that patients who present with a longer duration of symptoms may be better suited for needling than SWT. Furthermore, softer, less-defined (Garter-Heyer Type III) deposits can often be cleared with needling or SWT, but chronic, dense (Gartner-Heyer Type I) lesions may require surgical removal if conservative therapy fails. Notably, this review did not find any consistent prognostic demographic factors across needling and SWT multivariable analyses. Although most patients with RCCT were female, no study found sex to be a significant prognostic factor. However, several individual studies found various significant factors, including smoking history, hypothyroidism, and age, which require further analysis. Future prospective studies should standardize outcome definitions and imaging classifications and evaluate whether specific calcification characteristics and ultrasound parameters can improve outcomes in patients with RCCT. Comparative studies are also needed to directly contrast prognostic factors between needling and SWT modalities, thereby refining patient selection. Ultimately, refining patient selection and procedural targeting with the findings from this review may enhance the therapeutic value of minimally invasive treatments for RCCT.
This review has several limitations. The most significant is the marked heterogeneity among included studies. Needling studies varied widely in patient selection, procedural technique (ultrasound- vs fluoroscopy-guided, with or without steroid injection), outcome definitions, and follow-up duration, making it difficult to isolate the effect of needling alone. SWT studies also rarely distinguished between treatment success and failure, limiting their prognostic value. Additionally, the lack of data on the natural history of RCCT and the frequent use of co-interventions further limit the interpretation of treatment effects. Treatment success was variably defined, follow-up was generally brief, and patient demographics were inconsistent, contributing to substantial clinical and methodological heterogeneity. Because data were reported inconsistently, including outcomes at non-uniform time points, selective prognostic variables, and limited multivariable adjustment, a pooled statistical analysis was not feasible. The risk of bias was moderate to high across most papers, and the quality of evidence for nearly all prognostic factors was low or very low, primarily due to imprecision and inconsistency. Accordingly, observed trends should be interpreted cautiously, and no causal inferences can be drawn. Nonetheless, the heterogeneity present in the literature underscores the need for standardized definitions, consistent outcome reporting, and prospective validation of prognostic factors in future studies on these non-surgical treatments for RCCT.
Conclusion
This review identified five potentially prognostic factors that may influence outcomes following needling for RCCT: larger calcification size, Gartner-Heyer Type III (fluid-like) morphology, shorter distance between the subacromial bursa and deposit, normal bursal appearance, and fewer needling sessions. For SWT, shorter symptom duration and Type III morphology may predict better outcomes. However, the strength of evidence remains limited, with most findings derived from underpowered single studies with moderate-to-high risk of bias and should be interpreted with caution. Future work should include studies examining the natural history of RCCT and randomized controlled trials with true placebo controls and minimal co-interventions to confirm their value and build a more precise patient-selection algorithm for RCCT.
Supplemental Material
sj-docx-1-sel-10.1177_17585732251414964 - Supplemental material for Prognostic factors for outcomes following needling and shockwave therapy in rotator cuff calcific tendinitis: A systematic review
Supplemental material, sj-docx-1-sel-10.1177_17585732251414964 for Prognostic factors for outcomes following needling and shockwave therapy in rotator cuff calcific tendinitis: A systematic review by Ayomide Michael Ade-Conde, Loiy Alkhatib, Ashraf Hantouly and Oyinade Stephanie Ade-Conde, Emmanuel Olaonipekun, Danielle Dagher, Moin Khan in Shoulder & Elbow
Supplemental Material
sj-docx-2-sel-10.1177_17585732251414964 - Supplemental material for Prognostic factors for outcomes following needling and shockwave therapy in rotator cuff calcific tendinitis: A systematic review
Supplemental material, sj-docx-2-sel-10.1177_17585732251414964 for Prognostic factors for outcomes following needling and shockwave therapy in rotator cuff calcific tendinitis: A systematic review by Ayomide Michael Ade-Conde, Loiy Alkhatib, Ashraf Hantouly and Oyinade Stephanie Ade-Conde, Emmanuel Olaonipekun, Danielle Dagher, Moin Khan in Shoulder & Elbow
Supplemental Material
sj-docx-3-sel-10.1177_17585732251414964 - Supplemental material for Prognostic factors for outcomes following needling and shockwave therapy in rotator cuff calcific tendinitis: A systematic review
Supplemental material, sj-docx-3-sel-10.1177_17585732251414964 for Prognostic factors for outcomes following needling and shockwave therapy in rotator cuff calcific tendinitis: A systematic review by Ayomide Michael Ade-Conde, Loiy Alkhatib, Ashraf Hantouly and Oyinade Stephanie Ade-Conde, Emmanuel Olaonipekun, Danielle Dagher, Moin Khan in Shoulder & Elbow
Supplemental Material
sj-xlsx-4-sel-10.1177_17585732251414964 - Supplemental material for Prognostic factors for outcomes following needling and shockwave therapy in rotator cuff calcific tendinitis: A systematic review
Supplemental material, sj-xlsx-4-sel-10.1177_17585732251414964 for Prognostic factors for outcomes following needling and shockwave therapy in rotator cuff calcific tendinitis: A systematic review by Ayomide Michael Ade-Conde, Loiy Alkhatib, Ashraf Hantouly and Oyinade Stephanie Ade-Conde, Emmanuel Olaonipekun, Danielle Dagher, Moin Khan in Shoulder & Elbow
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.