
Abstract
Background
The association between preoperative mental health trends and arthroscopic rotator cuff repair (RCR) outcomes and patient satisfaction has not been previously described. We investigated the association between a subjective change in preoperative mental health and patient-reported outcome measures (PROMs) and achievement of patient satisfaction and substantial clinical benefit (SCB), defined as an improvement of American Shoulder and Elbow Surgeons Standardized Shoulder Assessment score ≥ 17.5, following RCR.
Methods
Among patients undergoing RCR, various PROMs were collected preoperatively and at follow-up intervals up to 2 years postoperatively. Patient satisfaction and achievement of SCB were analyzed relative to subjective reports of better, worse, or unchanged mental health in the year preceding RCR and preoperative PROMs.
Results
Eighty-eight patients (47 male and 41 female) with a median age of 60.0 years (interquartile range (IQR), 10.0) were included in this study. All patients (n = 13) who reported improved mental health status preceding RCR had significantly better satisfaction (P = 0.03) and SCB (P ≤ 0.05) at 2 years postoperatively compared to patients who reported worse or unchanged mental status.
Discussion
Subjective improvement in mental health status preceding arthroscopic RCR was associated with patient satisfaction and achievement of SCB at 2 years postoperatively.
Introduction
Rotator cuff tears (RCT) are a common shoulder pathology that occur due to traumatic injury or degenerative changes and are associated with an increased prevalence based on patient age. 1 Although many RCTs are asymptomatic, 2 arthroscopic rotator cuff repair (RCR) is the primary surgical treatment for the 36% of patients with symptomatic RCTs.3,4 Patient-reported outcomes of pain and disability after arthroscopic RCR demonstrate high response variability even after successful repair of the anatomic defect. Emphasis on the biopsychosocial model of care has suggested that factors such as patient expectations, emotional distress, and mental health play a larger role in postoperative outcomes of arthroscopic RCR than previously thought.5–7
The current literature is indeterminate regarding the association between preoperative mental health and postoperative patient satisfaction following arthroscopic RCR. Preoperative biomedical characteristics8–10 are associated with patient satisfaction following arthroscopic RCR. However, there are conflicting reports on the association between preoperative mental health and patient satisfaction after arthroscopic RCR.8–10 Furthermore, the effect of change in mental status in the preoperative period (i.e. the year prior to surgery) on arthroscopic RCR outcomes and patient satisfaction has not previously been investigated.
While the current literature suggests that preoperative mental status may influence postoperative outcomes and patient satisfaction following arthroscopic RCR, the degree of association between these factors remains undetermined. Additionally, the manner in which surgeons can directly assess their patients’ mental health, apart from diagnosed psychiatric illnesses, in order to gain insights into their postoperative outcomes and satisfaction has not been adequately described. In this study, we aim to investigate the association between a subjective change in preoperative mental health and preoperative patient-reported outcome measures (PROMs) and achievement of patient satisfaction and substantial clinical benefit (SCB) following RCR. We hypothesize that a self-assessed improvement in mental health in the year prior to arthroscopic RCR is significantly associated with improved postoperative outcomes and increased patient satisfaction following arthroscopic RCR. Additionally, we aim to investigate the association between preoperative responses to individual items of the Veterans RAND 12-Item Health Survey (VR-12) and achievement of patient satisfaction and SCB. We hypothesize that responses to VR-12 Item 9 are significantly associated with the achievement of SCB and complete patient satisfaction at 2 years postoperative. Finally, we aim to demonstrate the magnitude of change in PROMs between preoperative and 2 years following arthroscopic RCR. We hypothesize that all PROMs are significantly improved at 2 years postoperative versus baseline scores.
Methods
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of the University of Texas Medical Branch (IRB #20-0306). All study participants provided written informed consent. This is a retrospective review of PROMs before and following arthroscopic RCR (Current Procedural Terminology code 29827). STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) guidelines were implemented. 11 The primary outcomes of this study were achieving complete patient satisfaction and SCB in American Shoulder and Elbow Surgeons (ASES) score at 2 years postoperative. Secondary outcomes included improvements in PROMs relative to baseline at 2 years post-RCR. All procedures were performed by one fellowship-trained shoulder and elbow surgeon. A database of PROMs was maintained for patients who underwent arthroscopic RCR between 2 March 2018 to 13 January 2021. Recorded PROMs included pain visual analog scale (VAS), measures of shoulder function including ASES Standardized Shoulder Assessment and Single Assessment Numeric Evaluation (SANE), and VR-12 Mental Component Summary (MCS) and Physical Component Summary (PCS) which are measures of psychological and overall physical function, respectively. Patients completed these instruments immediately preoperatively and at postoperative intervals of 2 weeks, 6 weeks, 3 months, 6 months, 1 year, and 2 years. Preoperative mental health change was assessed using VR-12 Item 9 (a nonvalidated measure of preoperative mental health change), in which patients were asked “Compared to one year ago, how would you rate your emotional problems (such as feeling anxious, depressed, or irritable) now?” Patient demographic data including age and sex were recorded. A nonvalidated patient satisfaction questionnaire (Standard Late Postoperative Form) consisting of four questions assessing patient-reported pain and shoulder function was administered at 2 years postoperatively (Supplemental Table 1). The magnitude of difference between ASES scores before surgery and 2 years postoperative was used to determine whether SCB was achieved in accordance with Cvetanovich et al., 12 in which improvement of ASES score ≥ 17.5 was considered an achievement of SCB. Preoperative ASES data was not recorded for 1 of the 88 patients, which prevented the determination of achievement of SCB in this patient. The magnitude of difference between PROMs at 2 years postoperative versus preoperative was used to determine whether minimal clinically important difference (MCID), defined as the change in outcome score that results in the smallest, appreciable clinical improvement after surgery, 6 was achieved following RCR (VR-12 MCS, 6.0; 13 VR-12 PCS, 4.9; 13 ASES, 11.1; 12 SANE, 16.9; 12 VAS, 1.5). 14
Based on responses to the patient satisfaction questionnaire at 2 years postoperative, patients were stratified into two groups. Patients who reported that their expectations regarding improvement in pain and function in all four domains were either met or exceeded were considered completely satisfied, and patients who reported that their expectations were not met in one or more domains were considered unsatisfied. Patients who underwent arthroscopic RCR during the study period and completed PROMs and the satisfaction questionnaire at their 2-year follow-up appointment or later were considered eligible for this study. Due to variations in scheduling and clinical availability, patients whose final follow-up appointment occurred ≤60 days before 2 years postoperative were considered eligible for this study. Patients who were lost to follow-up before 2 years postoperative were excluded.
Patient demographics
Between 2 March 2018 to 13 January 2021, 107 arthroscopic RCRs were performed by a single shoulder and elbow surgeon at our institution. Of the 107 eligible patients, 19 patients were lost to follow-up before 2 years postoperative and were excluded. The remaining 88 (82%) patients completed the Standard Late Postoperative form and PROMs at 2 years postoperative and were included in this study. Demographic data and concomitant procedures for included patients are shown in Table 1. Average follow-up duration was 2.1 years (range 1.8–3.8). Median age (P = 0.48), sex (P = 0.73), and baseline PROMs did not differ significantly between patients lost to follow up (VR-12 MCS median, 43.2, interquartile range (IQR), 22.9, P = 0.18; VR-12 PCS median, 33.8, IQR, 11.1, P = 0.14; ASES median, 40.0, IQR, 18.7, P = 0.25; SANE median, 50.0, IQR, 48.8, P = 0.18; VAS median, 6.0, IQR, 4.4, P = 0.44) and included patients (Table 2).
Demographic data and concomitant procedures.
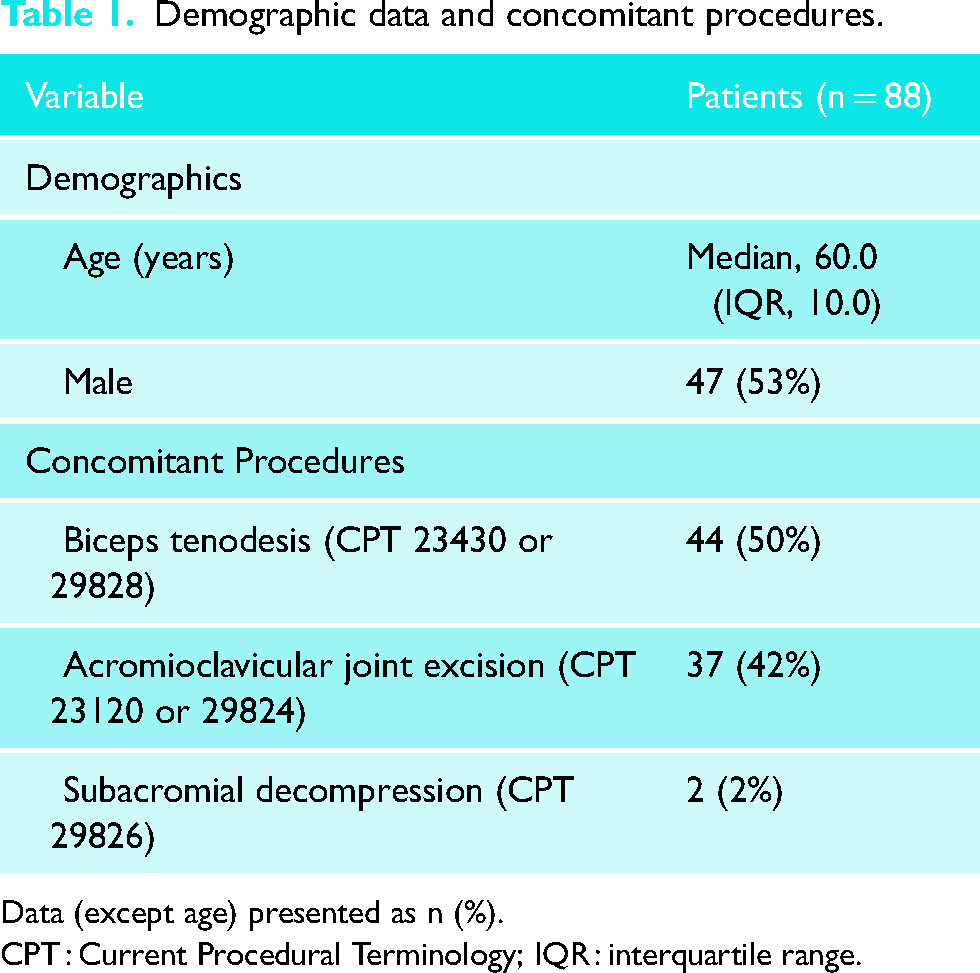
Data (except age) presented as n (%).
CPT : Current Procedural Terminology; IQR : interquartile range.
Two years versus preoperative patient-reported outcome measures.
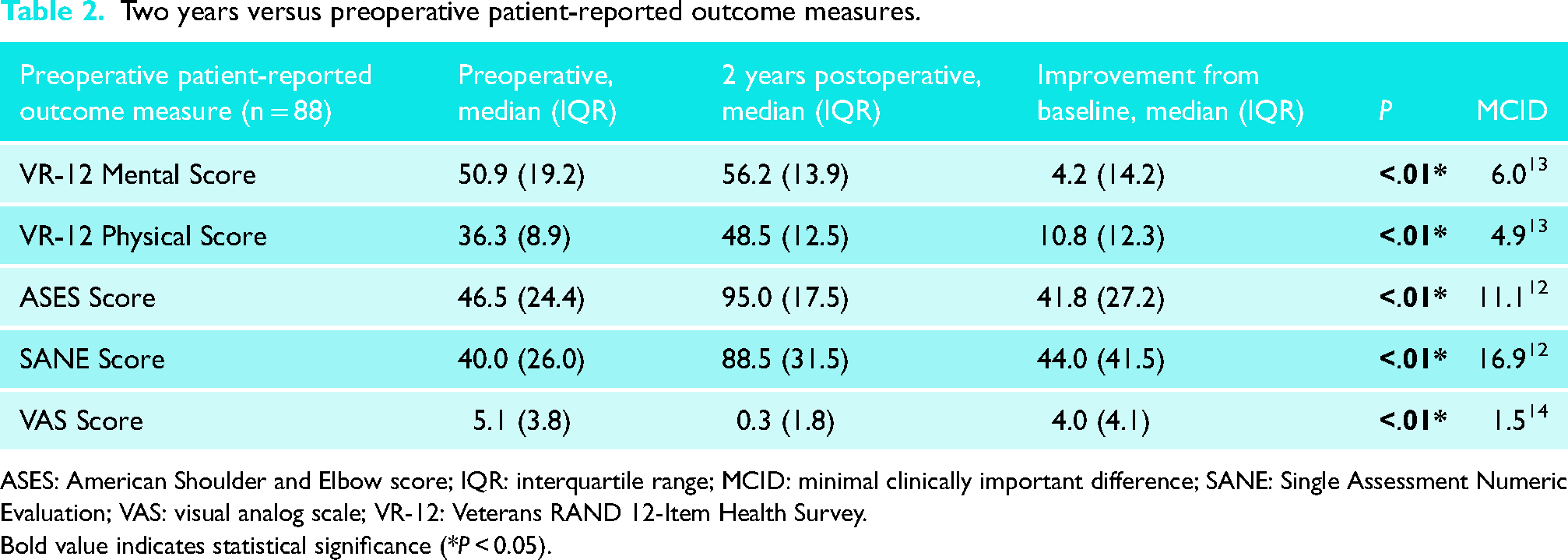
ASES: American Shoulder and Elbow score; IQR: interquartile range; MCID: minimal clinically important difference; SANE: Single Assessment Numeric Evaluation; VAS: visual analog scale; VR-12: Veterans RAND 12-Item Health Survey.
Bold value indicates statistical significance (*P < 0.05).
Postoperative rehabilitation protocol
Rehabilitation after rotator cuff repair followed a standardized protocol. Crescent-shaped small and medium-sized tears (≤ 3 cm anteroposterior width) without retraction were treated with sling immobilization for 4 weeks and early passive range of motion exercises. Gentle active range of motion and light resistance exercises were initiated at 4 weeks. Progressive strengthening was added at 10 to 12 weeks after surgery. For larger and/or retracted tears, sling immobilization was maintained for 6 weeks with supported passive table slides started at 2 weeks. Active range of motion was initiated at 6 weeks and strengthening at 12 weeks.
Statistical analyses
Descriptive statistics were reported with median and IQR. Univariate logistic regression was performed to investigate the association between preoperative PROMs and achievement of SCB and patient satisfaction at 2 years postoperative. A chi-square test was performed to investigate the association between responses to preoperative VR-12 items and achievement of SCB and patient satisfaction at 2 years postoperative. The Shapiro-Wilk test was conducted to assess the normality of preoperative and postoperative outcome data. Upon determination that the data were not normally distributed, the Wilcoxon signed-rank test was used to compare VR-12 MCS, VR-12 PCS, SANE score, ASES score, and VAS preoperatively versus 2 years postoperative and to compare preoperative VR-12 MCS before versus during the COVID-19 pandemic. Spearman's rank correlation coefficient was utilized to determine the strength and direction of the association between preoperative VR-12 MCS and 2-year ASES scores. Statistical analyses were performed using JMP (Version 17.1.0, SAS Institute Inc., Cary, NC, 1989–2021). Statistical significance was defined as P < 0.05 for all statistical analyses. A retrospective power analysis was conducted for the achievement of patient satisfaction stratified by preoperative VR-12 Item 9 responses (i.e. “better” vs. “worse” or “unchanged”) to evaluate the adequacy of the sample size. The power was calculated to be 99%, indicating a very high probability of detecting significant associations between preoperative VR-12 Item 9 responses and the achievement of patient satisfaction at 2 years postoperative.
Results
At 2 years postoperative, 74 patients reported that all of their expectations were either met or exceeded, and 14 patients reported that their expectations were not met in at least one domain. SCB in ASES score was achieved in 75 patients and was not achieved in 12 patients. Preoperative ASES data was not recorded for 1 of the 88 included patients, which prevented the determination of achievement of SCB in this patient.
Outcome measures
Preoperative VR-12 Item 9 responses are shown in Figure 1. Among the patients who reported preoperatively that their emotional problems were much better or slightly better compared to one year ago on VR-12 Item 9, 100% were completely satisfied (n = 13/13, P = 0.03; Figure 2) and achieved SCB (n = 12/12, P < 0.05; Figure 3) at 2 years postoperative. Upon comparison of individual VR-12 Item 9 responses, significantly more patients who reported a preoperative improvement in mental status achieved satisfaction (n = 13/13) compared to patients who reported unchanged (n = 45/55; P = 0.03) and worsened mental status (n = 16/20; P = 0.04) (Figure 4). Significantly more patients who reported a preoperative improvement in mental status achieved SCB (n = 12/12) compared to patients who reported unchanged mental status (n = 46/55; P < 0.05) but not worsened mental status (n = 17/20; P = 0.08) (Figure 5). The majority of patients (89%, n = 67/75) who achieved SCB reported complete satisfaction at 2 years postoperative, compared to a 50% satisfaction rate (n = 6/12) among patients who did not achieve SCB (χ2 (1, N = 87) = 9.208; P < 0.01).
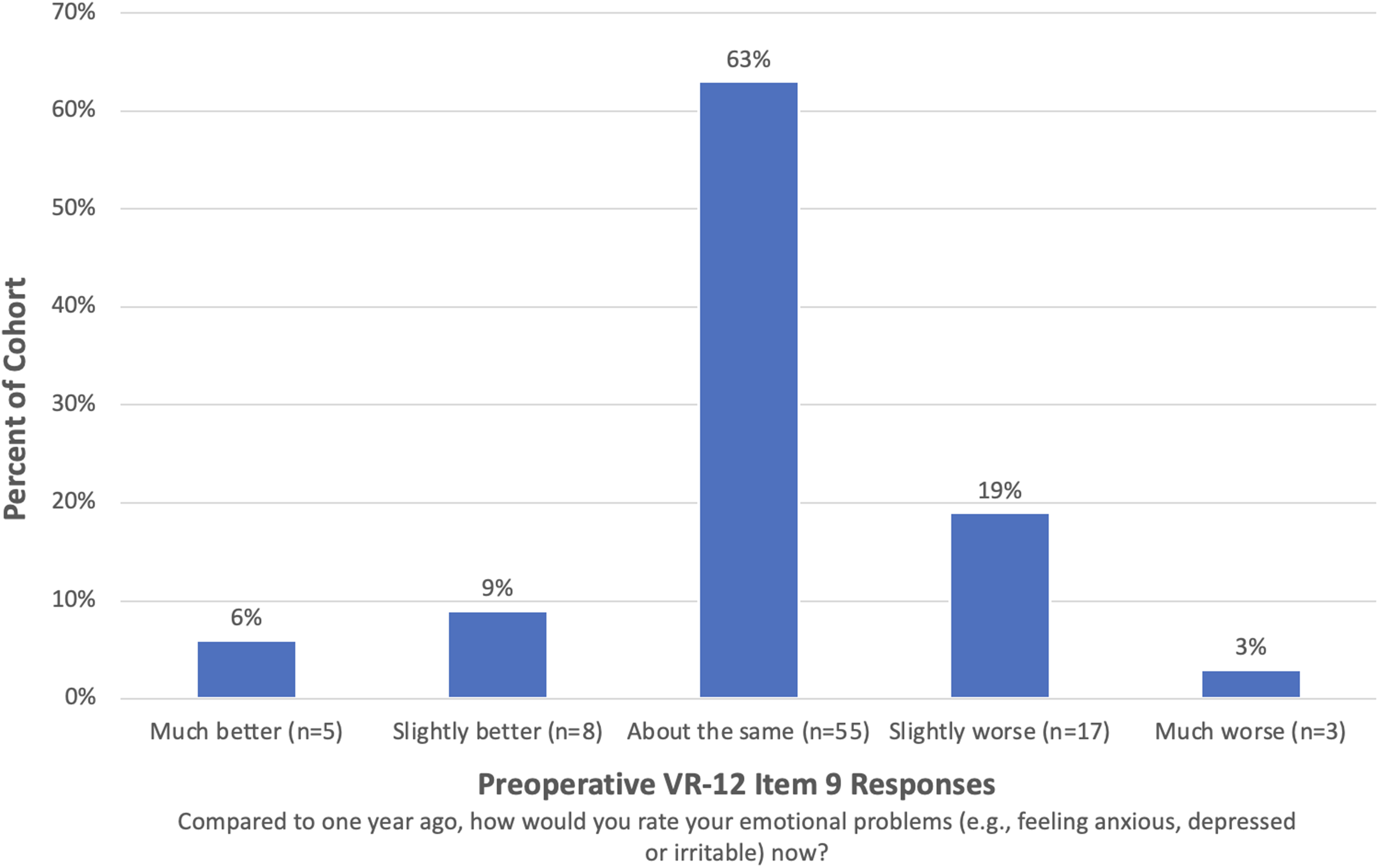
Preoperative Veterans RAND 12-Item Health Survey Item 9 responses. VR-12: Veterans RAND 12-Item Health Survey.
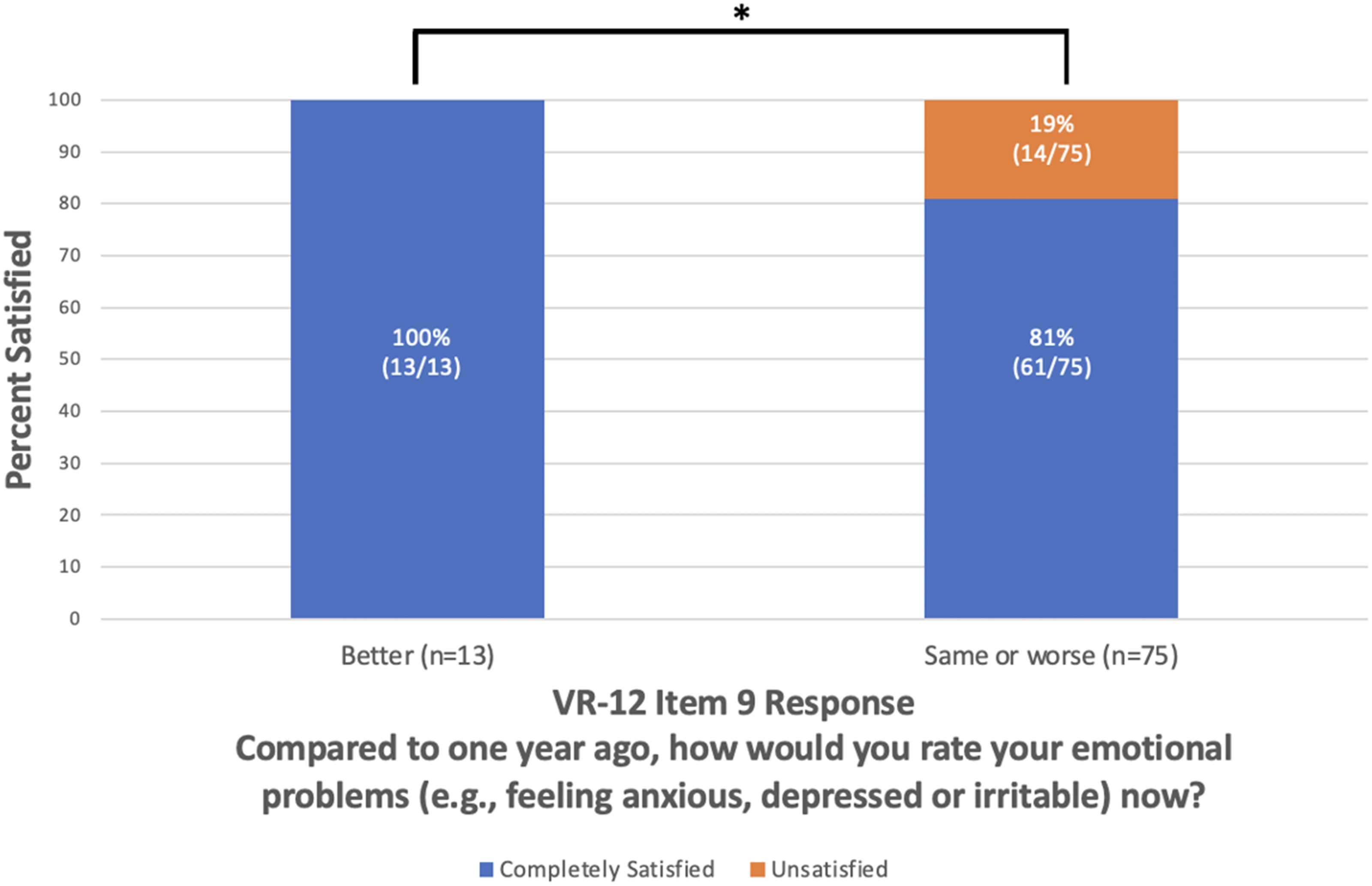
Overall satisfaction at 2 years postoperative vs. preoperative Veterans RAND 12-Item Health Survey Item 9. *P < 0.05, VR-12: Veterans RAND 12-Item Health Survey.
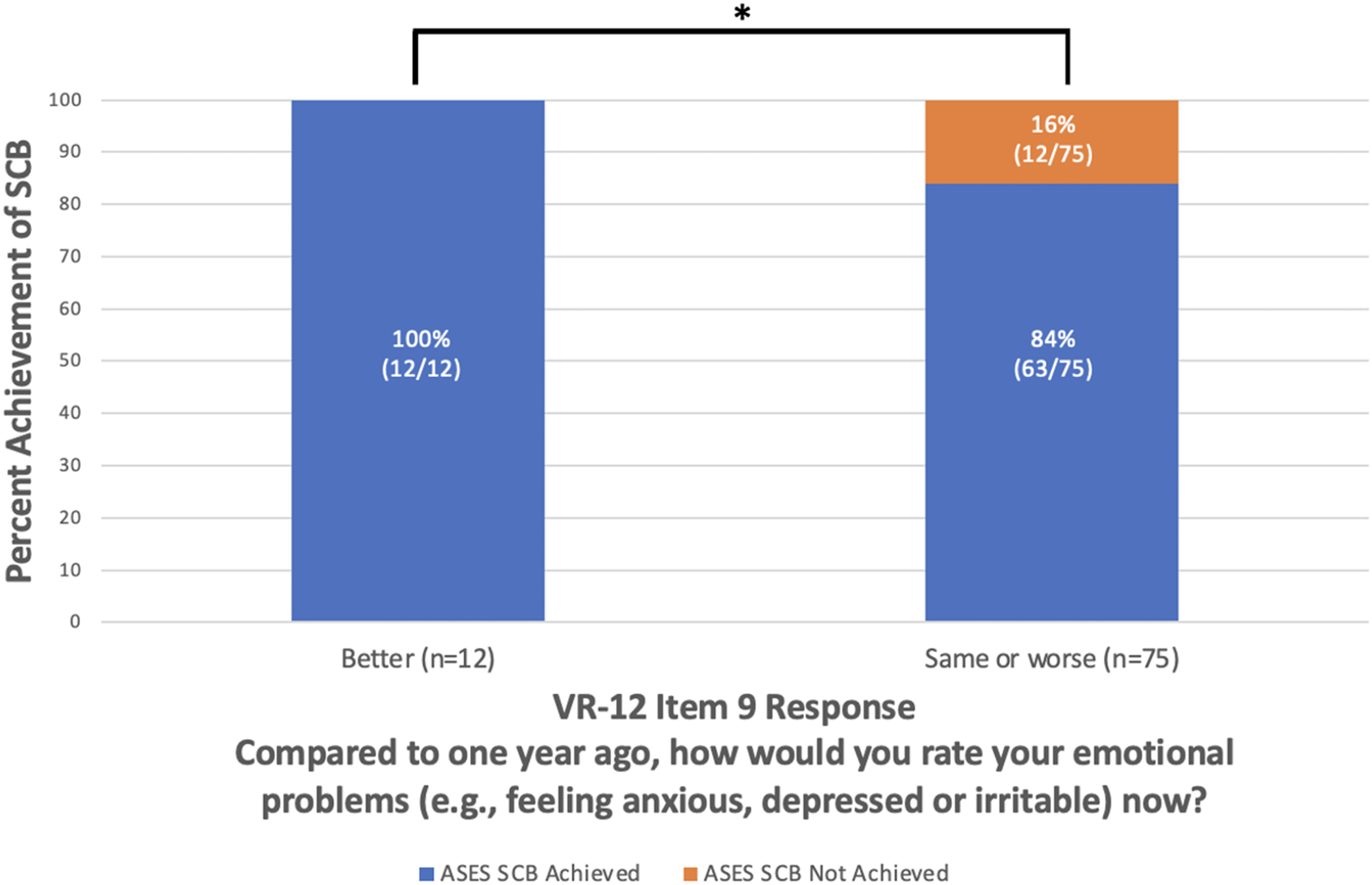
Achievement of American Shoulder and Elbow Surgeons substantial clinical benefit at 2 years postoperative versus preoperative Veterans RAND 12-Item Health Survey Item 9. *P < 0.05, SCB: substantial clinical benefit; VR-12: Veterans RAND 12-Item Health Survey.
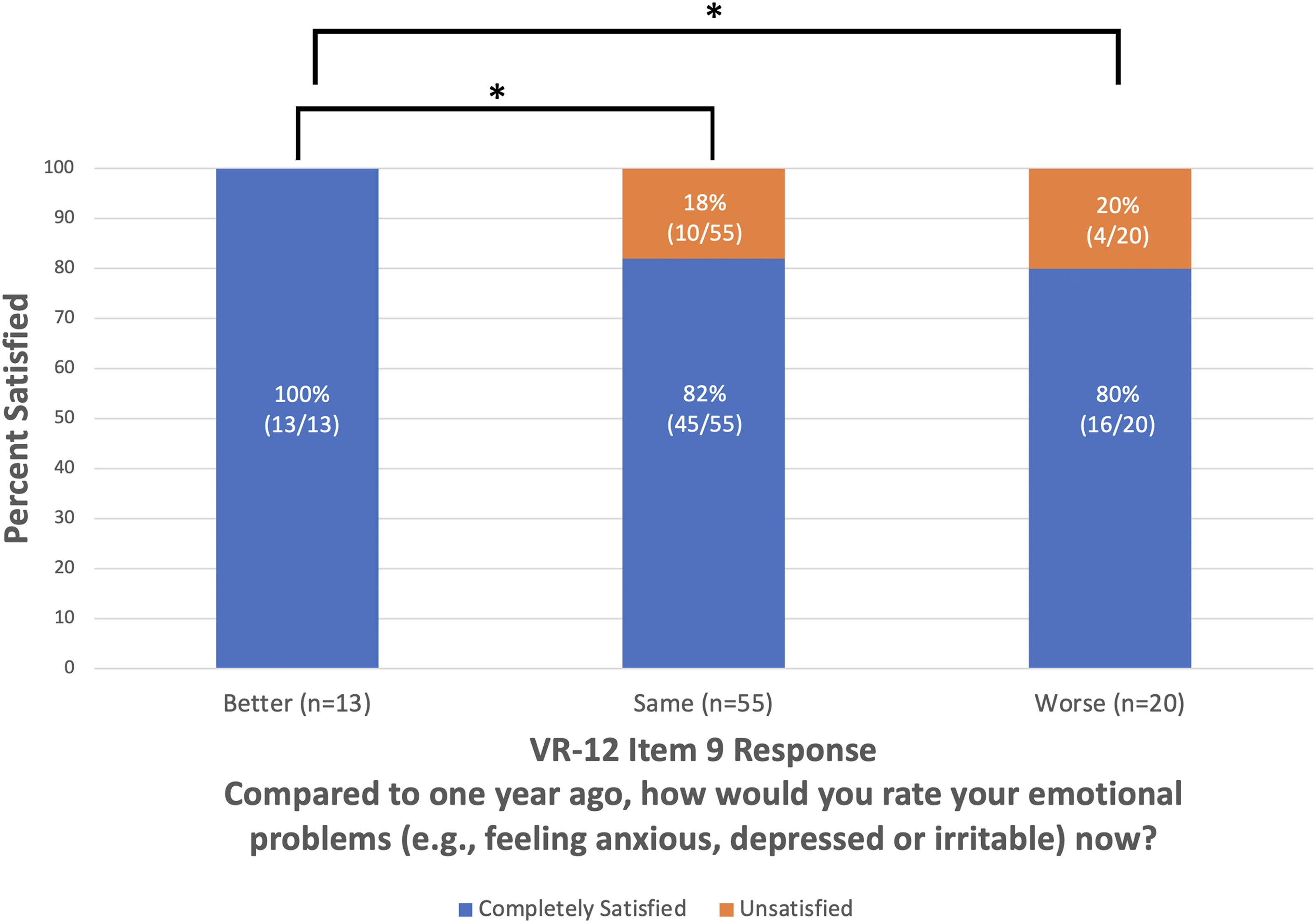
Satisfaction at 2 years postoperative versus individual responses to preoperative Veterans RAND 12-Item Health Survey Item 9. *P < 0.05, VR-12: Veterans RAND 12-Item Health Survey.
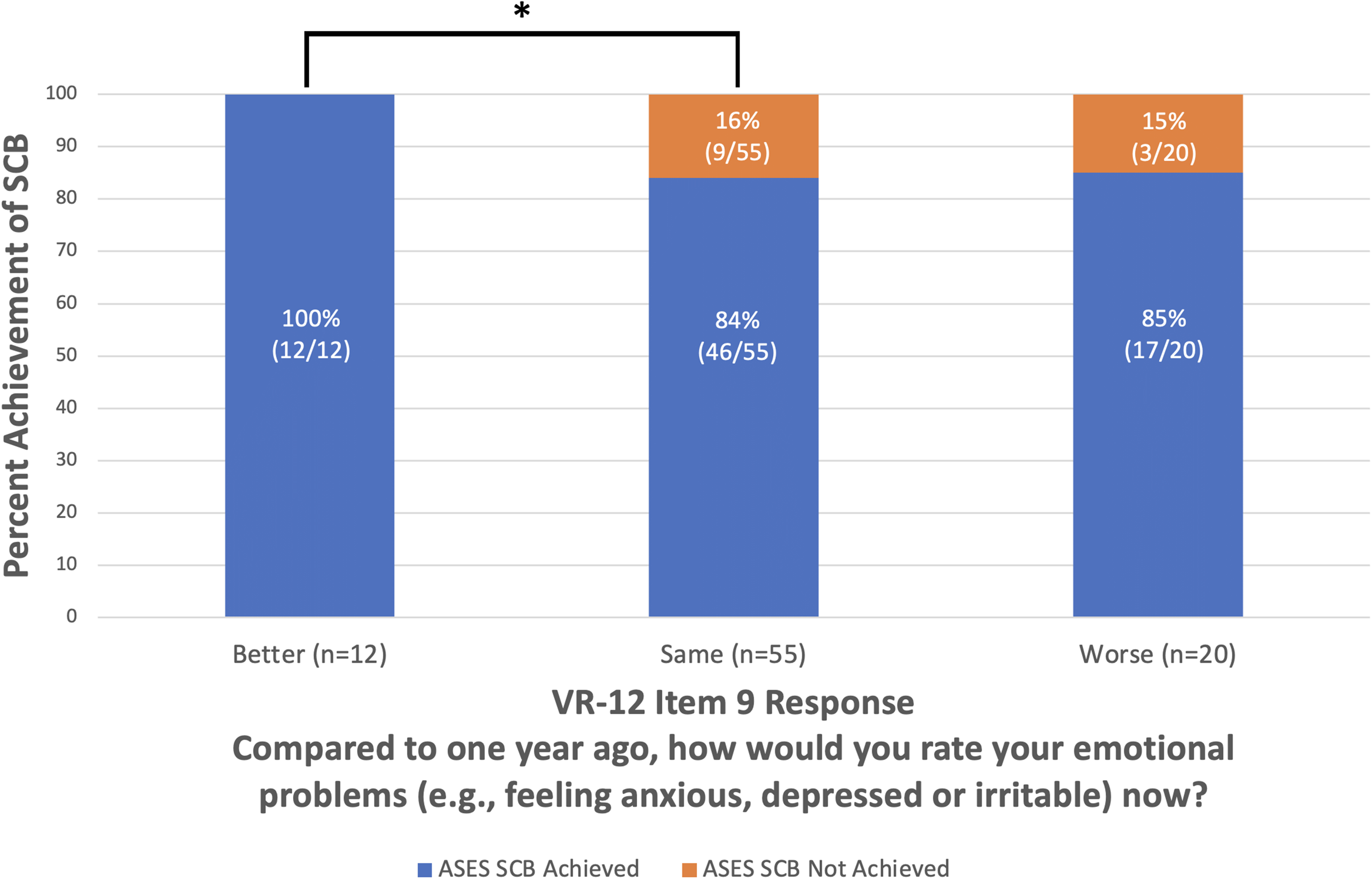
Achievement of American Shoulder and Elbow Surgeons substantial clinical benefit at 2 years postoperative versus individual responses to preoperative Veterans RAND 12-Item Health Survey Item 9. *P < 0.05, SCB: substantial clinical benefit; VR-12: Veterans RAND 12-Item Health Survey.
Among the 16% (14/88) of patients in this cohort who were unsatisfied, 71% (10/14) reported unchanged mental health and 29% (4/14) reported worsened mental health within the year preceding RCR. The 14% (12/87) of patients who failed to achieve SCB consisted of 75% (9/12) of patients who reported unchanged mental health and 25% (3/12) of patients who reported worsened mental health within the year preceding surgery (Supplemental Table 2).
There was a statistically significant improvement versus preoperative for all measures at 2 years postoperative. MCID was achieved for VR-12 PCS, ASES, SANE, and VAS at 2 years postoperative (Table 2). Of the preoperative PROMs, VR-12 MCS was the only measure associated with achievement of SCB (odds ratio, 1.07; 95% confidence interval, 1.01–1.13; P = 0.02) (Table 3). Other associations between notable items of VR-12 and achievement of SCB and postoperative satisfaction are shown in Table 4. VR-12 items that were not significantly associated with achievement of SCB or patient satisfaction at 2 years postoperative are shown in Supplemental Table 3.
Odds ratios of achievement of substantial clinical benefit and postoperative satisfaction at 2 years postoperative by preoperative patient-reported outcome measures.
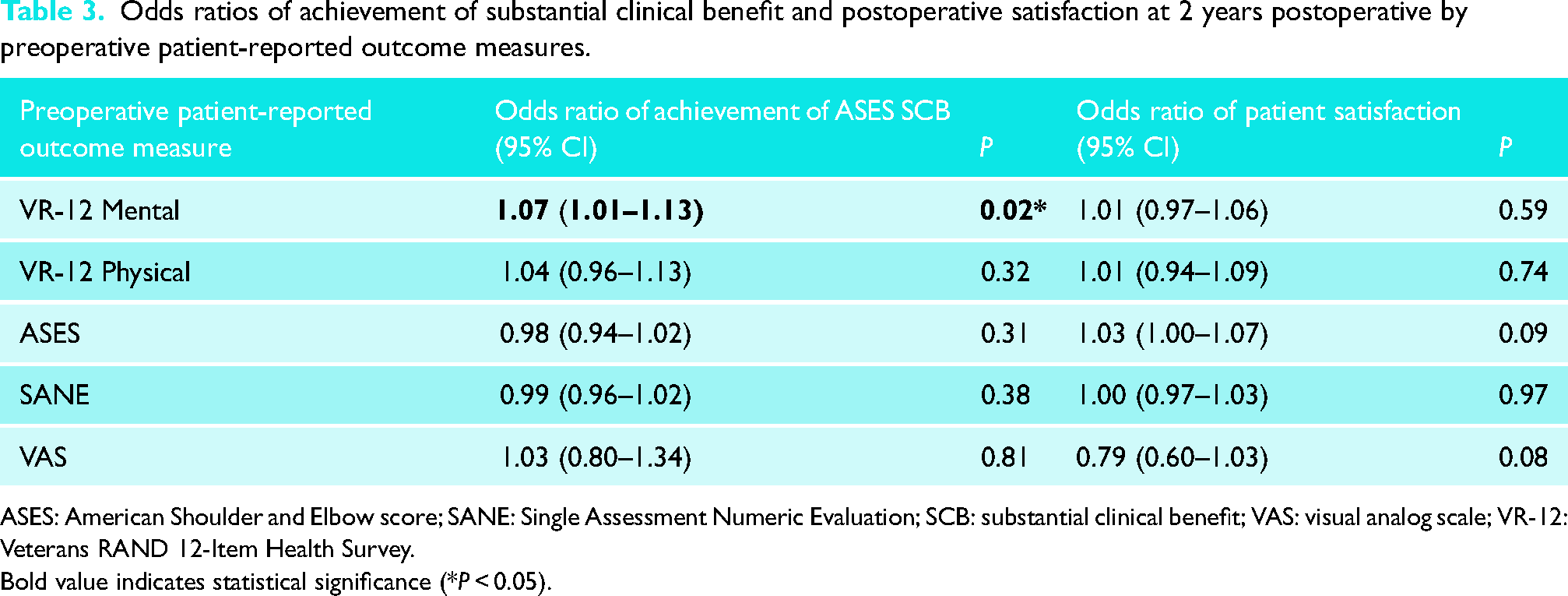
ASES: American Shoulder and Elbow score; SANE: Single Assessment Numeric Evaluation; SCB: substantial clinical benefit; VAS: visual analog scale; VR-12: Veterans RAND 12-Item Health Survey.
Bold value indicates statistical significance (*P < 0.05).
Associations between notable items of VR-12 and substantial clinical benefit and postoperative satisfaction at 2 years.
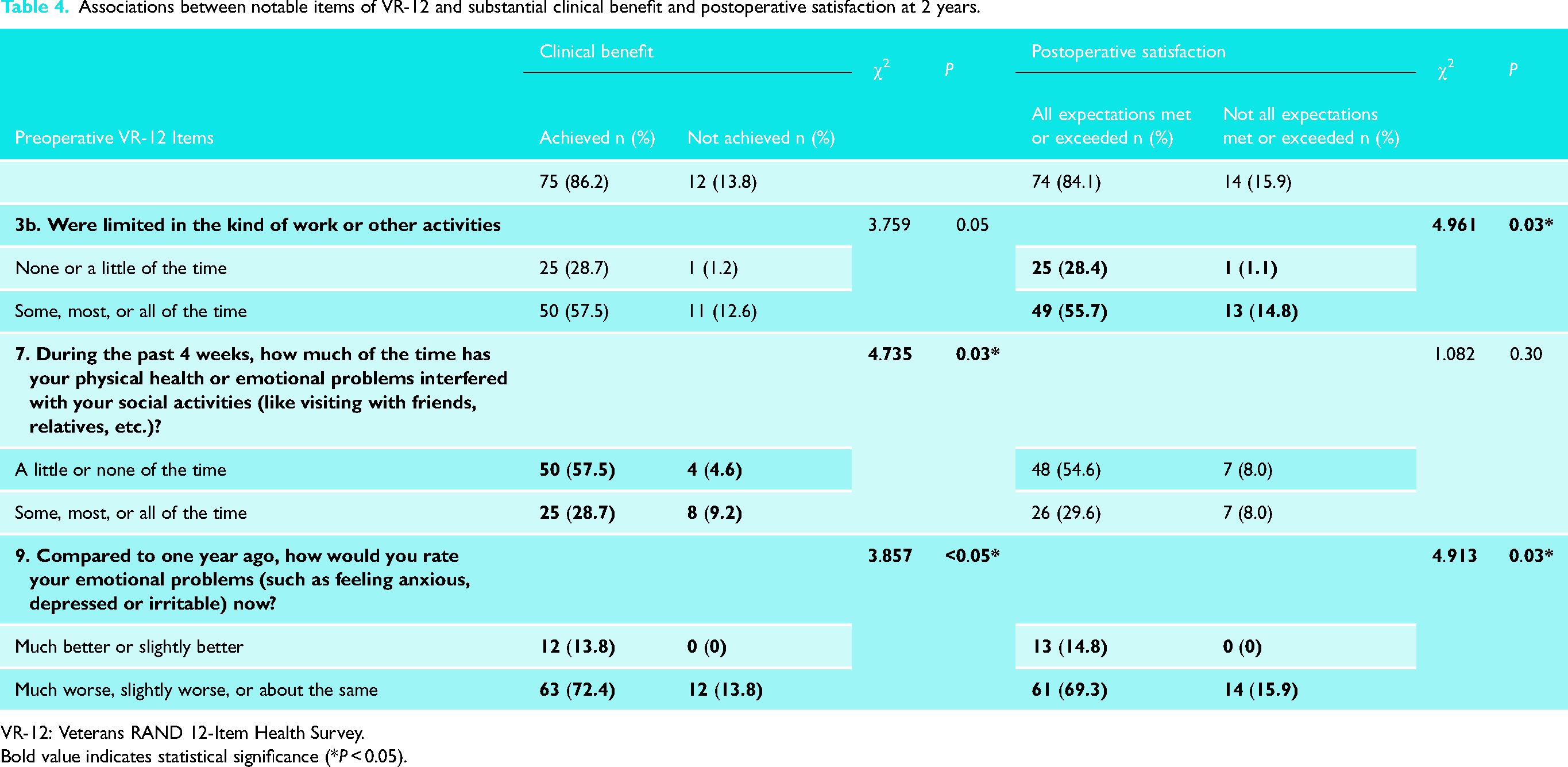
VR-12: Veterans RAND 12-Item Health Survey.
Bold value indicates statistical significance (*P < 0.05).
Demographic characteristics, including age (P = 0.83) and sex (P = 0.70), of the patients who reported a subjective improvement in preoperative mental status did not differ significantly from patients who reported unchanged or worsened mental status. Demographic characteristics did not differ significantly between patients who achieved SCB (age, P = 0.26; sex, P = 0.45) or complete satisfaction (age, P = 0.49; sex, P = 0.70) and patients who did not. Achievement of SCB and satisfaction were not significantly associated with concomitant procedures, including biceps tenodesis (SCB, P = 0.97; satisfaction, P = 1.00), acromioclavicular joint excision (SCB, P = 0.54; satisfaction, P = 0.60), or subacromial decompression (SCB, P = 0.21; satisfaction, P = 0.40). Preoperative VR-12 MCS did not differ significantly between patients who underwent surgery before versus during the COVID-19 pandemic (Supplemental Table 4).
Preoperative VR-12 MCS was positively correlated with ASES score at 2 years postoperative (r(86) = 0.22, P = 0.04) (Supplemental Figure 1). Among patients who reported improved mental status in the year preceding RCR, median preoperative MCS was 51.7 (IQR, 14.4) and 2-year ASES score was 94.6 (IQR, 12.1) (r(11) = −0.07, P = 0.82). Patients who reported unchanged mental status in the year preceding RCR had a median preoperative MCS of 54.7 (IQR, 16.4) and 2-year ASES score of 96.3 (IQR, 18.4) (r(53) = 0.18, P = 0.20). Among patients who reported worsened mental status in the year preceding RCR, median preoperative MCS was 37.0 (IQR, 14.3) and 2-year ASES score was 95.0 (IQR, 30.2) (r(18) = 0.23, P = 0.32).
Discussion
This study found that a self-assessed improvement in mental health preoperatively was associated with patient satisfaction and achievement of SCB at 2 years after arthroscopic RCR. Higher preoperative mental status was associated with greater odds of achievement of SCB at 2 years postoperative. Additionally, a weakly positive correlation was observed between preoperative VR-12 MCS score and ASES score at 2 years postoperative. These findings contribute to the growing body of literature describing the association between preoperative mental health and postoperative outcomes of RCR. Although 100% achievement of satisfaction and SCB was observed among patients who reported an improvement in mental health in the year preceding RCR, these patients constituted a notably minor segment of the small 88-patient cohort.
Previous studies have described the detrimental impact of poor preoperative mental health (i.e. anxiety and/or depression) on patient outcomes following arthroscopic RCR, as well as other orthopedic shoulder procedures such as total shoulder arthroplasty.15–20 Our findings are consistent with the current literature in this regard and are unique in that a patient-reported upward trend in mental health, as assessed by VR-12 Item 9, in the year prior to arthroscopic RCR was significantly associated with improved functional outcomes at 2 years.
The association between preoperative mental health and postoperative patient satisfaction has been described in the orthopedic literature for multiple procedures.21–23 Tashjian et al. 8 previously described the association between met expectations following arthroscopic RCR and patient satisfaction. This association supports the stratification of patients who responded that their expectations were met or exceeded in all four domains into the “completely satisfied” group for the purpose of analysis in this study. Among the currently available literature, this study is the first to describe a significant association between a patient-reported subjective improvement in mental health prior to arthroscopic RCR and increased patient satisfaction at 2 years postoperative.
We speculate that VR-12 Item 9 may serve as an indicator of preoperative patient optimism in addition to assessing mental health status. Previous studies have shown higher preoperative patient expectations to be associated with increased functional outcomes and patient satisfaction following arthroscopic RCR.5,10,24 Thus, more optimistic patients in our cohort may have been more likely to report that their emotional problems were better compared to one year ago and subsequently may have been more likely to experience an associated improvement in functional outcome and satisfaction. Based on these findings, asking patients “Compared to one year ago, how would you rate your emotional problems (such as feeling anxious, depressed or irritable) now?” may provide surgeons with valuable insights into their patients’ postoperative satisfaction and clinical outcomes. However, the findings of the present study should not be interpreted as evidence to withhold indicated procedures from patients with preoperative psychological dysfunction, nor to delay surgery in order to allow for the improvement of subjective mental health. Rather, the identification of a “better” response to VR-12 Item 9 preoperatively should be cautiously interpreted as a potential associator of desirable postoperative outcomes as opposed to a preoperative marker to be optimized. Additionally, posing the aforementioned question to patients is an innocuous method of initiating a conversation regarding mental health—a worthwhile endeavor during preoperative surgical counseling considering the associations between mental health, patient expectations, and postoperative outcomes.5,7,25
The present study isolated and analyzed the association between a subjective preoperative improvement in mental health and arthroscopic RCR outcomes by grouping patients who reported unchanged preoperative mental status with those who reported worsened preoperative mental status. Because 63% (55/88) of the patients in this cohort reported their mental status was “about the same” in the year preceding surgery, the results of this analysis are sensitive to the grouping of these patients. The decision to group patients with unchanged preoperative mental status together with patients who reported worsened mental status was made with the awareness that many patients with acceptable mental status who maintained good mental health (i.e., patients without psychological dysfunction) during the year preceding surgery likely constituted a large proportion of the “about the same” responders. Categorizing patients in this fashion was not performed to imply a comparable association between stable and declining preoperative mental status regarding arthroscopic RCR outcomes. Rather, grouping in this manner allowed for a singular determination of the association between a self-assessed improvement in mental health and arthroscopic RCR outcomes and the identification of a promising preoperative indicator of desirable postoperative outcomes (i.e. “better” response to VR-12 Item 9). Furthermore, clustering patients in this manner is supported by the subgroups of patients who were unsatisfied and/or failed to achieve SCB being constituted entirely of “same” and “worse” respondents to VR-12 Item 9 preoperatively (Supplemental Table 2). Because all “better” respondents to VR-12 Item 9 preoperatively were satisfied and achieved SCB, while multiple “same” and “worse” respondents failed to achieve these outcomes, grouping patients in this fashion allowed for the investigation of individual differentiating factors between these subgroups.
Limitations
This study has several limitations, the first being that our data were collected from the patients of a single surgeon. Another limitation is the use of the VR-12 MCS and Item 9 of the VR-12 to assess emotional and mental health. Although an association between lower VR-12 MCS and psychiatric diagnoses has been previously described, 26 the VR-12 is not a diagnostic psychiatric instrument. An additional limitation of the present study is the use of a postoperative patient satisfaction survey that has not been previously validated in the literature. The findings of this study are also limited by the inability to analyze the association between patient characteristics (e.g. body mass index, smoking status, prior shoulder injections, mental health diagnoses, and health concerns prohibiting recall), tear characteristics (e.g. atraumatic versus traumatic, tear chronicity, tear thickness, number of tendons involved, and Goutallier classification), surgery characteristics (e.g. primary versus revision surgery, need for augmentation or reconstruction, number of anchors used, and RCR failure rate), and postoperative functional outcomes and satisfaction within this cohort. Furthermore, the lack of access to this data prevented the utilization of these characteristics as inclusion/exclusion criteria for this study. Another limitation is the potential for recall bias among the included patients, especially given many of these patients were treated during the COVID-19 pandemic, which may have influenced their subjective perception of mental health over the study period and the year preceding surgery. 27 An additional limitation is the use of univariate logistic regression to investigate the association between preoperative PROMs and achievement of SCB and patient satisfaction, as this analysis does not account for the confounding variables that may influence the findings of this study. A final limitation of this study is the small sample size and the resultant risk that the results of this study may be attributable to chance due to it being underpowered. This limitation is furthered by the group of interest (i.e. patients who reported a subjective improvement in preoperative mental status) being limited to 13 patients. However, the median improvements in PROMs (i.e. VR-12 PCS, ASES, SANE, and VAS) among this cohort reached statistical significance and exceeded thresholds for minimal clinically important differences at 2 years postoperative (Table 2). These findings suggest the patients in this cohort experienced some degree of clinically relevant functional benefits and support the present investigation into factors associated with these improvements (i.e. “better” response on VR-12 Item 9).
To increase the generalizability of these findings, future investigations should seek to include data from multiple surgeons and institutions. Future studies should also measure preoperative emotional health using a validated psychiatric assessment instrument, such as the Patient Health Questionnaire-9 or Hospital Anxiety and Depression Scale (HADS), which may provide a more complete picture of an individual's preoperative mental and emotional health. Sabo et al. 28 previously demonstrated lower preoperative HADS score to be significantly correlated with increased patient-reported rotator cuff disease severity following RCR. By using a validated psychiatric instrument to assess the trend of mental health across the year prior to arthroscopic RCR, future studies may be able to distinguish whether a quantifiable upward trend in mental health scores or the patient's perception that their mental health has improved are more influential on postoperative outcomes and satisfaction. Additionally, investigating PROMs after arthroscopic RCR in patients with psychiatric disorders diagnosed by validated criteria, such as from the Diagnostic and Statistical Manual of Mental Disorders, may help to discern how the results of our study apply to various subpopulations (e.g. those with and without diagnosed psychiatric disorders). Finally, future studies on this topic should utilize a validated patient satisfaction questionnaire, such as the Patient Satisfaction Questionnaire-18, when assessing satisfaction after arthroscopic RCR.
Despite these limitations, this study presents follow-up data on patient satisfaction and functional outcomes with an 82% follow-up rate at 2 years. Because much of the currently available literature regarding the association between preoperative patient characteristics and arthroscopic RCR outcomes only reports longitudinal outcome data up to 12 months postoperatively,29–31 this study is notable in that we have presented patient outcomes at 24 months postoperative. With 37% of retears occurring after 12 months postarthroscopic RCR, 32 we believe that this extended follow-up duration provides valuable insight into the association between preoperative mental status and arthroscopic RCR outcomes, including patient satisfaction.
Conclusion
A self-assessed improvement in mental health in the year preceding arthroscopic RCR was associated with patient satisfaction and achievement of SCB at 2 years postoperative. Preoperative VR-12 MCS score demonstrated a weakly positive correlation with ASES score at 2 years postoperative. Despite these findings, the degree of association between preoperative mental health and outcomes of arthroscopic RCR remains uncertain due to the limitations of this study. Additional investigation into the associations between psychological factors, including subjective trends in preoperative mental status, and postoperative outcomes of RCR are warranted.
Supplemental Material
sj-docx-1-sel-10.1177_17585732241274577 - Supplemental material for The association between self-assessed improvement in mental health preceding rotator cuff repair and patient satisfaction: A retrospective cohort study
Supplemental material, sj-docx-1-sel-10.1177_17585732241274577 for The association between self-assessed improvement in mental health preceding rotator cuff repair and patient satisfaction: A retrospective cohort study by Brady P Moore, Dexter Allen, David S Clark and Jeremy S Somerson in Shoulder & Elbow
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.