
Abstract
Background
Failed Latarjet procedures pose a surgical challenge due to complex anatomical issues. This systematic review investigates salvage techniques for recurrent instability following a Latarjet procedure.
Methods
A search was conducted on MEDLINE and PubMed Central following the methodology registered to International Prospective Register of Systematic Reviews. Inclusion criteria focused on identifying revision procedures following a Latarjet procedure. Exclusion criteria filtered out irrelevant studies, such as those focused on Bankart procedures. After a multistage selection process, 10 eligible studies were included for data extraction.
Results
The most frequently utilized technique for salvage was variations of the Eden–Hybinette procedure. Complications associated with these salvage procedures include graft-related problems and donor site morbidity. Patients reported significant improvements in multiple patient-reported outcome scores, and multiple studies indicated high rates of return to sports activities. However, it is noteworthy that there remains an average recurrence rate of 7%.
Discussion
The review emphasizes the limited therapeutic options available largely due to shoulder anatomy alterations. Despite promising trends in patient-reported outcomes, recurrence remains possible post-salvage surgeries.
Conclusion
Addressing recurrent instability after a Latarjet procedure continues to be a unique surgical challenge. However, this systematic review highlights encouraging indications, with positive trends evident in patient-reported outcomes.
Introduction
This systematic review delves into the salvage procedures available for patients who have experienced suboptimal outcomes following a Latarjet intervention. Over time, there has been a noticeable shift in the approach to managing patients with failed soft-tissue Bankart repairs. 1 Surgeons are increasingly favoring anatomical reconstruction of the anterior glenoid surface using bone-block techniques instead of revisiting soft-tissue repairs. Among these techniques, variations of the open Latarjet procedure have gained prominence. 2 The Latarjet procedure is noteworthy for its creation of a “dynamic-sling” effect of the conjoint tendon and the utilization of the coracoid tip as a local, autologous transfer, mitigating potential donor site morbidity. 2 Arthroscopic bone-block procedures have also emerged as viable alternatives. However, with the growing number of Latarjet procedures being performed, the rate of failures is increasing. 3
These cases often exhibit significant glenoid bone loss, either independently or concomitantly with humeral bone loss, leading to a complex surgical scenario. Additionally, the weakness or absence of anterior capsule-labral structures adds another layer of complexity to revision surgeries. 4 Moreover, anterior scarring around the subscapularis complicates the surgical approach. The absence of the conjoint tendon as a medial landmark also places critical neurovascular structures at risk.
One of the central challenges in addressing failed Latarjet procedures lies in the dissection of the scarred subscapularis, which may have been manipulated during the initial Latarjet surgery. This process is essential for the revision procedure and can pose potential risks to neurovascular structures especially when the subscapularis must be released.
The surgical options available to tackle the complexities of a failed Latarjet procedure are somewhat limited. When examining salvage procedures, they can be categorized into two main groups. Some salvage procedures focus on restoring stability solely through soft tissue repair, while others incorporate an additional bone block for reinforcement. A significant number of failed Latarjet procedures necessitate the inclusion of an additional bone block for effective reconstruction. Among these procedures, the most common technique is the Eden–Hybinette procedure, which involves harvesting the necessary bone graft from the iliac crest. It is worth noting that the Eden–Hybinette procedure has a longstanding history of use spanning over a century and was the primary choice before the Latarjet procedure gained prominence, largely due to its dynamic sling effect, which enhances stability. 5
In consideration of these multifaceted issues, this systematic review aims to comprehensively explore salvage procedures for failed Latarjet interventions. It seeks to illuminate the nuances of surgical strategies, outcomes, and the critical factors that influence their success.
Material and methods
For this systematic review, we initiated an extensive search across two prominent databases: MEDLINE and PubMed Central (PMC). Before starting the review of the literature, the methodology was published on International Prospective Register of Systematic Reviews (PROSPERO) ID CRD42023469290.
The inclusion criteria included studies written in English that focus explicitly on revision procedures after a failed Latarjet procedure. Furthermore, selected papers were required to contain patient-reported outcomes (PROs), enabling a comprehensive analysis of procedural success. The exclusion criteria included systematic reviews, studies on surgical techniques, articles concentrating on procedures following a Bankart procedure rather than Latarjet, or those involving nonrevision procedures. In addition, any studies focusing on arthroplasty were excluded.
After the methodology was created, the study selection process went through a multistage approach by two independent reviewers to comprehensively identify pertinent literature. In each stage of the review, the articles excluded were recorded and eventually categorized in a PRISMA flow diagram (Figure 1).
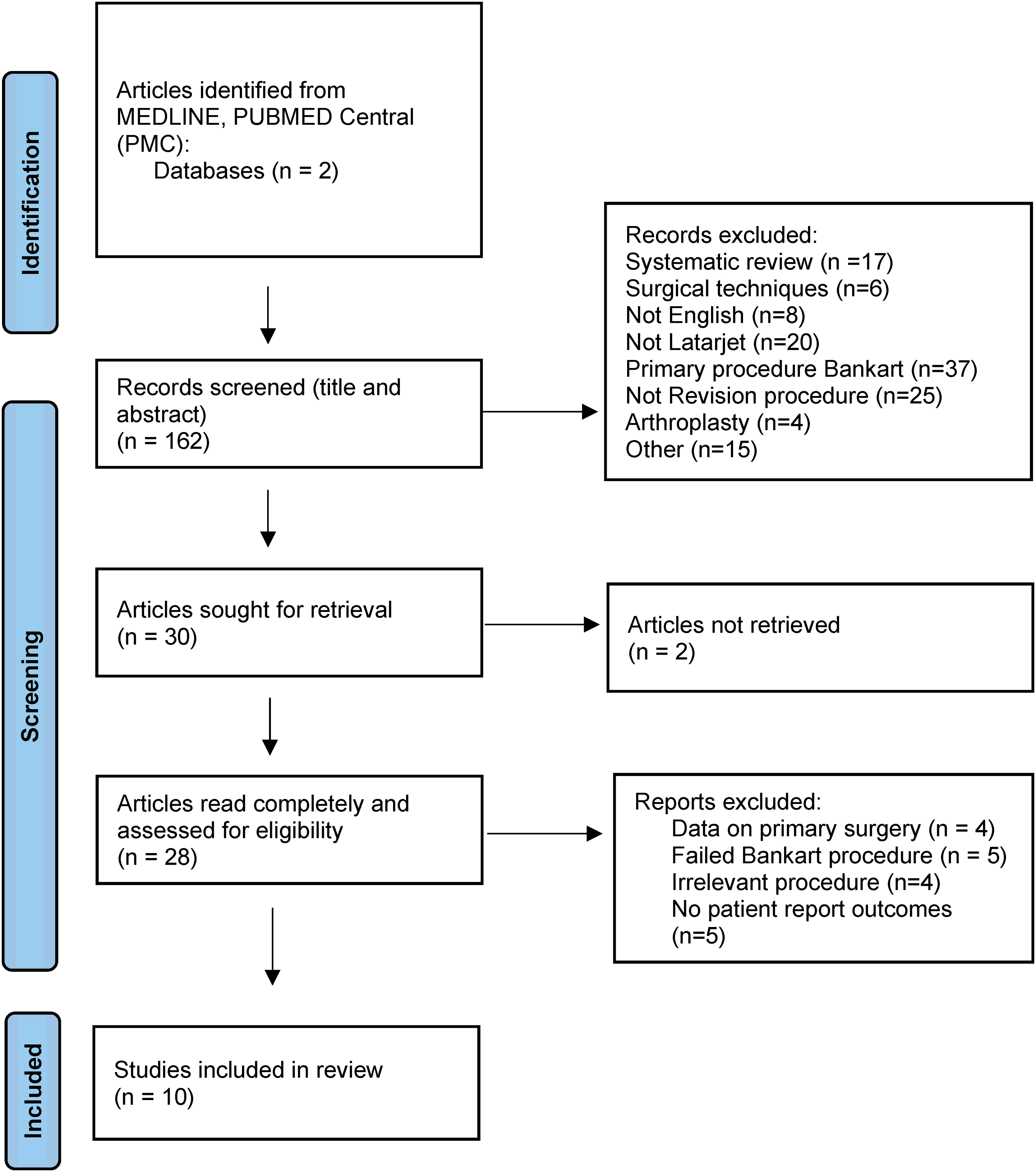
PRISMA flow diagram.
Initially, a total of 162 records were retrieved from the MEDLINE and PMC databases. These records underwent screening, with the evaluation of titles. During this phase, 17 records were excluded as they were systematic reviews, six articles were excluded as they were surgical techniques, and eight records were omitted due to non-English language. After reading the abstracts, 20 records were discarded for not pertaining to a Latarjet procedure, 37 records were excluded for concentrating on the primary Bankart procedure rather than Latarjet, 25 records were removed for not involving revision procedures, 4 records were excluded for focusing on arthroplasty, and 15 records were omitted for various other reasons.
Following the screening process, 30 articles were selected for full-text review. Two articles were unavailable for full-text retrieval. Upon thorough examination, a significant portion of the papers did not meet the inclusion criteria. Notably, nine studies centered around irrelevant primary procedures like the Bankart, four articles emphasized primary procedures instead of revisions, and five articles lacked outcome reporting. Illustrated in Figure 1, the final number of included studies was 10. Once the final studies were selected, two independent reviewers performed data extraction and inputted data into a master spreadsheet for further analysis.
Results
Table 1 provides a comprehensive list of procedures documented in the literature for addressing failed Latarjet procedures. Our systematic review identified 301 relevant procedures for patients who had a Latarjet procedure that eventually failed and required further intervention.
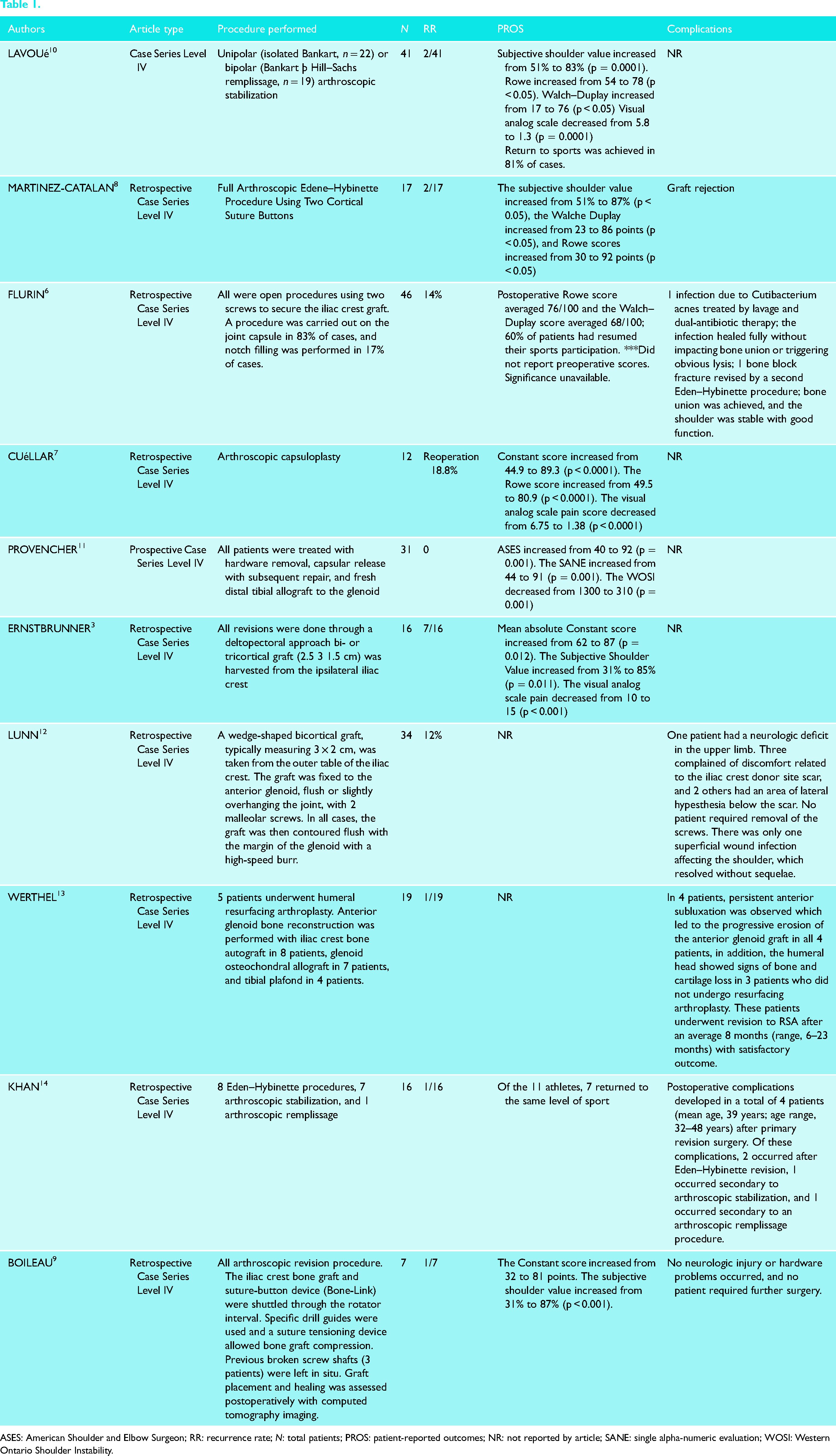
ASES: American Shoulder and Elbow Surgeon; RR: recurrence rate; N: total patients; PROS: patient-reported outcomes; NR: not reported by article; SANE: single alpha-numeric evaluation; WOSI: Western Ontario Shoulder Instability.
When examining Table 1, the specific surgical techniques can be further categorized based on their methods of stabilization. Among these techniques, a small subset focuses solely on soft tissue repair. Lavoue, and Cuellar focused on soft tissue repairs, which yielded highly favorable outcomes with no reported complications. Lavoue's work underscores the effectiveness of the Bankart with Remplissage procedure for labral repair, while Cuellar et al. emphasize the benefits of capsule repair in enhancing shoulder stability.6,7
As an alternative to soft tissue repair, revision of a failed Latarjet procedure may involve reconstruction using a bone graft. Our systematic review highlights the prevalent use of bone grafts in such cases, primarily due to the increased stability required. Notably, 70% of the procedures analyzed in our study were based on modifications of the Eden–Hybinette technique. While the Eden–Hybinette technique emerged as the predominant salvage procedure in our review, variations exist concerning the source of the bone graft and approach.
Two papers describe using an arthroscopic approach to address these revision cases.8,9 In their papers, they emphasize the shorter recovery times and reduced postoperative complications compared to more extensive open procedures. However, it is important to note that arthroscopic techniques for these very rare cases may require a learning curve and have certain limitations.
When analyzing the graft's source, the coracoid is no longer an option due to the primary Latarjet procedure. The most common site for the bone block is the original Eden–Hybinette procedure which involves obtaining bone from the iliac crest. Only one paper harvested the bone graft from a different site. In the Provencher paper, they found success using a graft from the distal tibia. 8 When examining the 6 variations of the original Eden–Hybinette procedure, differences emerge in how the bone graft was utilized such as the specific anchors used and the accompanying procedures performed alongside grafting.
Table 1 provides a comprehensive overview of potential complications and risks associated with a diverse range of surgical procedures employed for salvage Latarjet shoulder stabilization and reconstruction. This challenging patient population presents numerous potential complications. Notably, the open procedure carries the risk of neurologic complications due to disrupted anatomy. While many of the papers discussed this risk, none of the studies reported nerve damage in the upper extremity.
The most common complication reported was associated with the failure of the bone block. The use of distal tibial or iliac crest allografts introduces inherent risks, including graft rejection, infection, nonunion, and graft resorption. Boileau et al. and Werthel et al. specifically examine cases where the graft size was insufficient to provide stability even after the procedure is complete due to erosion and degeneration.9,13 Martinez-Catalan et al. and Flurin et al. discuss graft rejection and subsequent osteolysis or nonunion that may be associated.6,8 The paper by Flurin also reports on infection from the open case.
Alongside complications reported at the shoulder, there were also complications reported at the graft harvest site. The study by Werthel et al. highlighted issues related to these grafts. 13 Patients may experience chronic pain and sensory disturbances, particularly dysesthesia of the lateral cutaneous femoral nerve.
It is essential to acknowledge that some studies, including those by Lavoue, Cuellar, and Provencher, did not report on complications.7,10,11 The absence of reported complications in these studies underscores the imperative need for further research and data collection to comprehensively assess the safety profile of these procedures.
Recurrent instability was the most common PRO identified across all the studies. This systematic review found the average rate of instability to be 7% following the salvage procedures, underscoring the complexity of these cases. Notably, Ernstbrunner and Cuéllar's study reported the highest recurrence rates at 44% and 18.8%, respectively.3,7 In contrast, Provencher observed no recurrences in their patient cohorts. 11 These varying recurrence rates underscore the need for more research into which procedures are most appropriate for patients with a failed Latarjet procedure.
In addition to assessing the recurrence rate, we analyzed further reported PROs. Notably, the studies by Lunn et al. and Werthel et al. lacked any PROs beyond the recurrence rate.12,13 By delving into the PRO data for the remaining eight papers, we can discern specific improvements and challenges observed in these studies. As a whole the study outcome scores were positive especially considering the limited options available for this subset of patients.
Of the shoulder scores, the most reported was the subjective shoulder value. The studies by Lavoue et al., Martinez-Catalan et al., Boileau et al., and Ernstbrunner et al. reported a significant increase in the subjective shoulder value p-values of 0.0001, <0.05, <0.001, and 0.011, respectively.3,8–10 Interestingly, the study by Ernstbrunner excluded all the failed procedures in their PRO analysis. Another commonly reported score was the Rowe score. The studies by Lavoue et al. and Cuellar et al. reported significant improvements p-values of <0.05 and <0.0001, respectively.7,10 While the Provencher et al. did not report a subjective shoulder value or Rowe score, they did report significant improvements in the American Shoulder and Elbow Surgeons, single alpha-numeric evaluation, and Western Ontario Shoulder Instability Index scores all with p-values of 0.001. 11
Along with the outcome scores return to sport are helpful for determining the benefit of these salvage procedures. The highest return to sport was in 81% in the Lavoue study. 10 The Flurin et al. and Khan et al. studies also had a high return to sport of 60% and 64%, respectively.6,14
Discussion
Given the substantial alterations in shoulder anatomy resulting from the initial surgery, the therapeutic options available for these patients are decidedly limited. There are very few studies that examine the outcomes of these patients. It is essential to acknowledge that the interventions discussed in this systematic review are far from routine procedures and carry significant risks for patients.
Soft tissue repair vs. bone-block procedures
When addressing the challenge of recurrent instability following an unsuccessful Latarjet procedure, the first step in deciding the best therapeutic option is choosing between soft tissue repair and bone block procedures. Our systematic review reveals that bone block procedures are more frequently employed as salvage interventions, primarily because soft tissue repairs struggle to adequately address the complexities of these cases. Notably, the studies exclusively focused on soft tissue repairs were conducted by Lavoue and Cuellar,7,10 both of which did not report significant complications. The study by Khan reported a mix of arthroscopic stabilization or bone-block stabilization depending on the unique presentation. 14 Similarly, their paper found success with arthroscopic stabilization but emphasized proper patient selection. It is important to highlight that soft tissue techniques were also frequently used in conjunction with bone block procedures. Provencher and Werthel, for instance, incorporated soft tissue techniques to complement their bone block procedures.11,13
Among the various bone block procedures, different iterations of the Eden–Hybinette technique emerged as the most commonly preferred option. Nonetheless, it is essential to emphasize that further research is imperative to explore the optimal integration of soft tissue techniques alongside the Eden–Hybinette procedure. Additionally, more in-depth investigation into the precise sizing of allografts and the choice of anchors used would greatly enhance our understanding of this complex issue.
Complications
The inherent complexity of these procedures is primarily rooted in the challenging anatomical alterations required for the shoulder. Among the reported complications, graft failure, encompassing issues such as resorption, erosion, and nonunion, stands out as the most common concern.
Maintaining an appropriate balance in the size of the bone graft is paramount. Boileau et al.'s findings emphasize that a graft that is too small can result in recurrent instability, while a graft that is overly large, as described by Werthel et al., may lead to future erosion.9,13 Another risk associated with bone grafts is nonunion, a topic discussed in studies by Martinez-Catalan and Flurin.6,8
Furthermore, in addition to the challenges posed by the shoulder itself, the graft harvesting process presents potential morbidity concerns. Notably, the study by Lunn highlighted specific morbidities associated with iliac crest bone graft harvesting. 12
Patient outcomes and recurrence rates
Shifting our focus toward the outcomes of the salvage procedures, we can explore two crucial aspects: recurrence rates and PROs. Both of these metrics are important to consider when determining if these drastic procedures will have a therapeutic benefit to the patient.
Our systematic review revealed substantial benefits for patients undergoing these procedures, with multiple PRO scores showing significant improvement. These positive outcomes underscore the viability of this option for individuals experiencing recurrent instability post Latarjet procedure. While valuable for managing this patient subset, the findings should also inform the decision-making process regarding the initial consideration of a Latarjet procedure.
Despite overall positive outcomes, it is imperative to scrutinize the findings in light of infrequent occurrences. The procedures entail notable complications due to their highly invasive technique, and patients may still experience instability, as indicated by the average recurrence rate of 7% across the 301 patients.
Limitations of study
This systematic review on salvage procedures for failed Latarjet interventions faces several limitations that should be considered when interpreting its findings. Firstly, the number of eligible studies was relatively small, reflecting the scarcity of high-quality research on this topic. It should be noted that there have been advancements in surgical techniques for these individuals in recent years. Two notable articles by Hewins and Shao in the journal Arthroscopy Techniques discuss these innovative techniques.15,16 These papers show promising results but must be further examined in future research with papers that contain PROs.
The absence of comparative studies in the literature is a notable limitation in discerning the optimal therapeutic option for patients. Furthermore, a lack of long-term follow-up data in numerous studies impedes the assessment of outcome durability.
Lastly, publication bias and heterogeneous patient populations may impact the results of this systematic review. The inclusion criteria for the articles varied widely making it hard to generalize the findings to specific subgroups in the future. Future research efforts should prioritize well-designed comparative analyses and long-term follow-up studies to enhance our understanding of the optimal approaches for addressing failed Latarjet interventions.
Conclusion
This systematic review delves into the challenging realm of salvage procedures for patients with recurrent instability after Latarjet interventions, highlighting the preference for bone block procedures, primarily variations of the Eden–Hybinette technique, in managing these cases. While these procedures can lead to significant improvements in PROs, they still carry a risk of recurrence, along with complications and risks associated with graft-related issues and donor site morbidity, emphasizing the complexity of these surgeries. However, this review has limitations such as a limited number of high-quality studies and heterogeneity among procedures. Future research should provide comparative analyses and long-term follow-up studies to enhance our understanding of the best approaches for addressing recurrent instability after Latarjet procedures. In conclusion, managing recurrent instability following a Latarjet procedure remains a challenging surgical task. Nevertheless, this systematic review reveals promising prospects with positive trends observed in PROs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.