
Abstract
Background
The objective of this study was to retrospectively report on the outcomes of female patients undergoing the Latarjet procedure.
Methods
Female patients undergoing the Latarjet procedure with minimum 1 year follow-up were identified and contacted to obtain Numeric Pain Rating Scale (NPRS), Subjective Shoulder Value (SSV), and return to sport (RTS) data. Eligible females were then matched 1:1 with a male counterpart based on laterality and age (± 3 years), and outcomes compared.
Results
A total of 20 female patients with a mean follow-up of 73.8 months reported postoperative NPRS and SSV scores of 2.2 ± 2.3 and 69.3 ± 22.0, respectively. Of the nine athletes, 3 (33%) reported a successful RTS at a mean of 9 months. Four patients (20.0%) required reoperation at a mean of 27.1 months. The matched analysis demonstrated similar NPRS scores between male and female patients and a trend towards lower SSV scores and rates of RTS.
Conclusion
At mid-term follow-up female patients reported pain levels similar to female-specific literature reports, but overall low subjective shoulder function and RTS. Compared to propensity-matched males, females reported similar levels of pain, lower shoulder function, and lower rates of RTS, however, differences did not reach statistical significance.
Level of Evidence
IV, retrospective case series.
Keywords
Introduction
The morbidity associated with glenohumeral instability and associated dislocation is significant. A recent epidemiologic study reported an incidence of shoulder dislocation as high as 23.9 per 100,000 person years, with an estimated 71.8% of dislocations occurring in male patients. 1 Recurrence rates between 26% and 90% have been reported when nonoperative management is undertaken, with younger age thought to be a risk factor for recurrance.2–4 As episodes of instability recur, glenoid bone loss increases which may further compromise stability. 5
Surgical management of recurrent shoulder dislocation is often indicated and has been shown to reduce healthcare expenditure by reducing the risk of recurrent dislocation and thus the development of osteoarthritis.4,6 Glenoid bone loss greater than 13.5% may be a threshold for consideration of bony augmentation to achieve stability. 7 When bony augmentation is desired, the Latarjet procedure is frequently used with long-term outcomes showing excellent patient subjective Rowe, Disabilities of Arm, Shoulder and Hand (DASH), and Subjective Shoulder Value (SSV) scores.8,9
While these studies provide a convincing argument for the Latarjet procedure in the setting of glenohumeral instability and critical bone loss, most focus on high-risk subgroups, mainly young men who play sport. Despite nearly 30% of first-time anterior shoulder dislocations occurring in females, there remains a paucity of data on female specific outcomes and complications.4,10 The limited data on the Latarjet procedure in female patients has demonstrated a potentially increased risk of recurrence and clinical failure. 11 Further, compared to males, lower postoperative return to sport and shoulder scores have been reported, suggesting that current strategies are not adequately meeting the demands of these patients. 12 This disparity in outcomes highlights the need for more data on female patients undergoing the Latarjet procedure such that decisions regarding risk stratification and procedure type can be made in a manner that promotes more equitable outcomes. Thus, the purpose of this study was to investigate and retrospectively report on the outcomes of female patients undergoing the Latarjet procedure, namely subjective shoulder function, pain, and return to sport (RTS).
Methods
Data collection
After obtaining approval from the Wake Forest School of Medicine Institutional Review Board (IRB00084659), a query of our institutional administrative database using the Current Procedural Terminology (CPT®) code 23462 (Latarjet coracoid process transfer) was performed to identify patients who underwent the Latarjet procedure between January 2010 and October 2021. All female patients who underwent the Latarjet procedure, with minimum 1-year follow-up, were considered for inclusion in the study. Patients with inadequate follow-up and those who did not undergo the Latarjet procedure were excluded. Patients were included regardless of prior surgeries or concomitant injuries. For further analysis and comparison, eligible female patients were then paired with male patients who had also undergone the Latarjet procedure during the study period on the basis of laterality and age (± 3 years).
We retrospectively reviewed clinical and operative notes of all eligible patients. For each patient, we reviewed electronic medical records and obtained demographic, operative, and postoperative data. Patients were contacted via telephone or email by an independent observer other than the primary surgeon and interviewed to obtain Numeric Pain Rating Scale (NPRS), SSV, and RTS data. The SSV score is a patient-based PRO that has been demonstrated to correlate with more extensive process-based PROs such as the American Shoulder and Elbow Surgeons (ASES) and Rowe scores. 13 In scenarios where an in-person return to clinic is not possible, the SSV is a simple, cost-effective, and meaningful method of evaluating general functional outcomes. 13 Patients were considered to be actively engaged in sports if they endorsed participation in athletic activity in the three years prior to surgery. RTS was considered as a return to activity at any performance level in the postoperative period, with performance level subjectively determined by the patient to be same, better, or worse. Verbal consent was obtained using standardized IRB-approved scripts for all patients prior to obtaining outcomes data. Patients were informed of all potential risks, namely the potential for loss of patient data and confidentiality and given the option to withdraw from the study at any point without repercussion.
Statistical analysis
All data underwent descriptive statistical analysis using SAS version 9.4 (SAS Institute, Cary, NC). A two-sample t-test was used for continuous data and significance was determined by an alpha level of 0.05. All data in the document are presented as n (%) where categorical and mean ± standard deviation (range) where continuous unless otherwise specified. For the analysis of SSV and NPRS scores patients were stratified on the basis of achieving the Patient Acceptable Symptom State (PASS). The PASS represents the level of postoperative outcome score required to reflect patient satisfaction. 14 The current literature on the Latarjet procedure has defined this threshold as a postoperative Single Assessment Numeric Evaluation (SANE)/SSV score of at least 82.5 and visual analog score for pain (VAS-pain) of 2.5 and below. 15 Given the correlation between VAS-pain and NPRS scores, an NPRS score of 2.5 was used to define the PASS for the purposes of this study. 16
Results
Female patient demographics
From a review of 252 patient visits identified via CPT® code 23462, we identified 33 consecutive unique female patients (Figure 1). After applying inclusion and exclusion criteria, a total of 30 patients were eligible for participation in the study. Of these, one (3.33%) declined to participate and 9 (30.0%) were unable to be contacted, leaving 20 patients (66.7%) available for analysis. The mean age at the time of surgery was 34.9 ± 16.6 years (range, 18–75). The mean Body Mass Index (BMI) was 25.8 ± 5.7 kg/m2 (range, 16.1–37.2) and three patients (15.0%) smoked tobacco use at the time of surgery. Two patients (10%) had a history of epilepsy, both of which were stable on anti-seizure medication at the time of surgery. No patients had a known history of hyperlaxity or connective tissue disorder. Nine patients (45.0%) were actively playing a sport in the three years prior to surgery, and all athletes endorsed competing at the amateur level. The mean time from surgery to final follow-up was 73.8 months (range, 22.3–144.3 months).
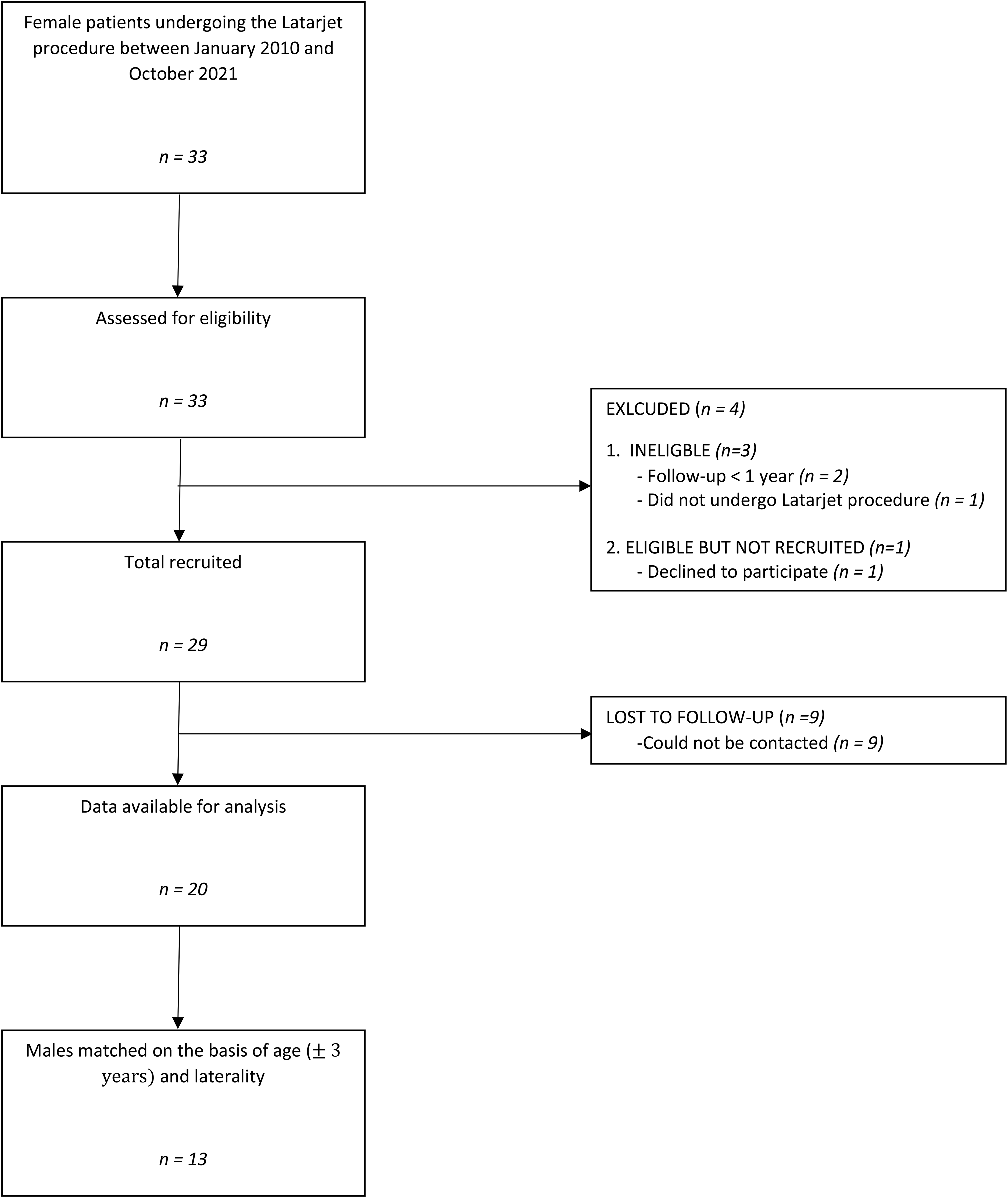
Female Latarjet consort diagram.
Operative details
The majority of surgeries were performed on the patient's right shoulder (60.0%). Further details of surgical technique are highlighted in Table 1. All 20 surgeries (100%) utilized metal screws and were performed using an open standard deltopectoral approach. Coracoid fixation was achieved with two screws in 19 patients (95%) and one screw in a single patient (5%). Exposure of the glenohumeral joint was achieved via subscapularis split in 13 patients (65%) and via tenotomy in 6 (30%). The approach was not documented for one patient (5%). Eleven of the 20 analyzed patients (55.0%) underwent a concurrent procedure at the discretion of the treating surgeon in addition to the Latarjet surgery. Thirteen patients (65.0%) had undergone a prior soft tissue stabilization procedure (either open or arthroscopic) on the ipsilateral shoulder.
Operative details (n = 20) a .
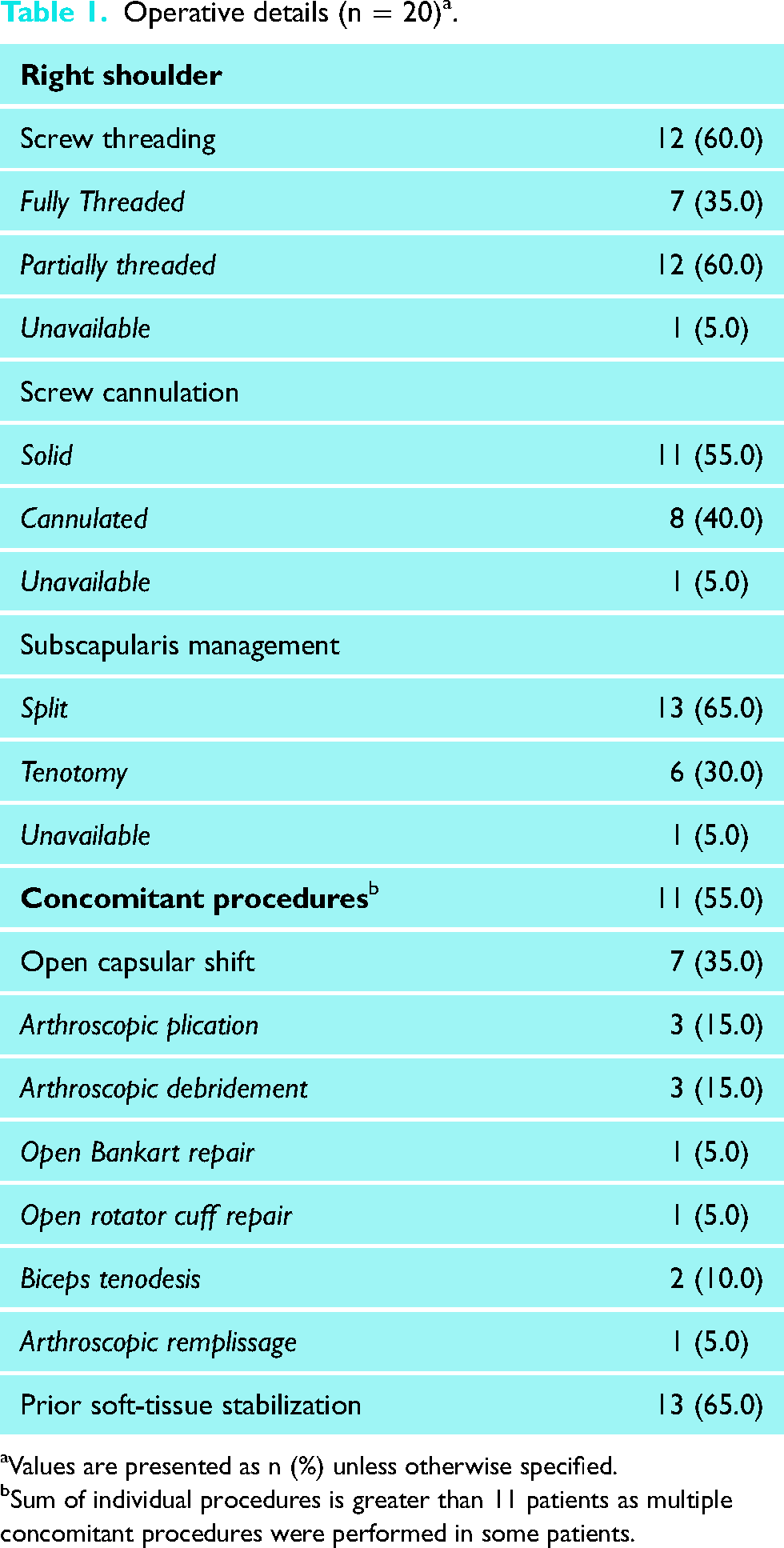
Values are presented as n (%) unless otherwise specified.
Sum of individual procedures is greater than 11 patients as multiple concomitant procedures were performed in some patients.
Subjective shoulder value (SSV)
The mean SSV score across all female patients was 69.3 ± 22.0 at final follow-up, with five patients (25.0%) being at or above the PASS score of 82.5 (Table 2). Although the study was not powered to detect a significant difference, compared to patients above the PASS, patients below the PASS were older, had more frequently undergone soft-tissue stabilization prior to Latarjet, more frequently underwent subscapularis tenotomy intraoperatively, and were less likely to have had a successful RTS postoperatively.
Variables associated with SSV scores greater and less than the PASS. a
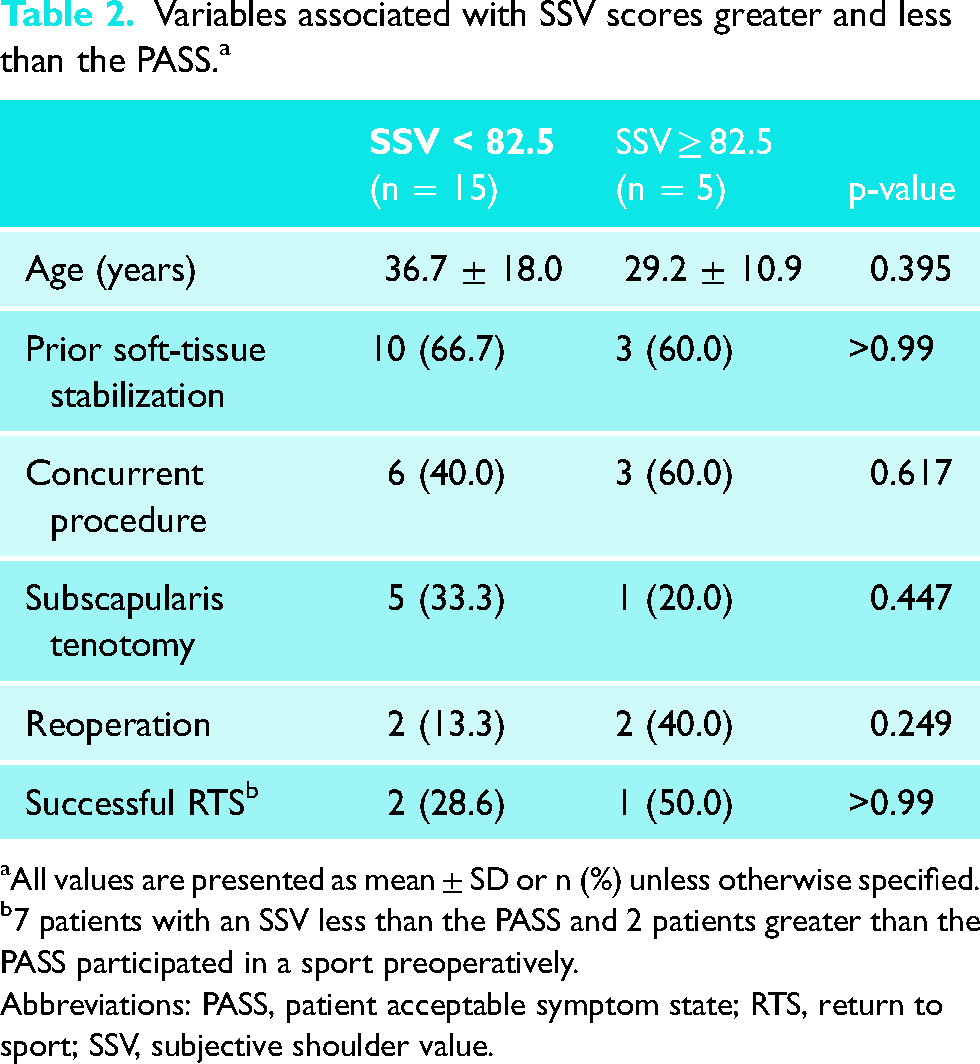
All values are presented as mean ± SD or n (%) unless otherwise specified.
7 patients with an SSV less than the PASS and 2 patients greater than the PASS participated in a sport preoperatively.
Abbreviations: PASS, patient acceptable symptom state; RTS, return to sport; SSV, subjective shoulder value.
Numeric pain rating scale (NPRS)
The mean NPRS value was 2.2 ± 2.3 at final follow-up, with 12 patients (60.0%) achieving the PASS (Table 3). Compared to patients not achieving the PASS, patients achieving the PASS were younger, had less frequently undergone soft-tissue stabilization prior to Latarjet, more frequently underwent subscapularis tenotomy intraoperatively, and were more likely to have had a successful RTS postoperatively, however, differences were not significant.
Variables associated with NPRS scores greater and less than the PASS. a
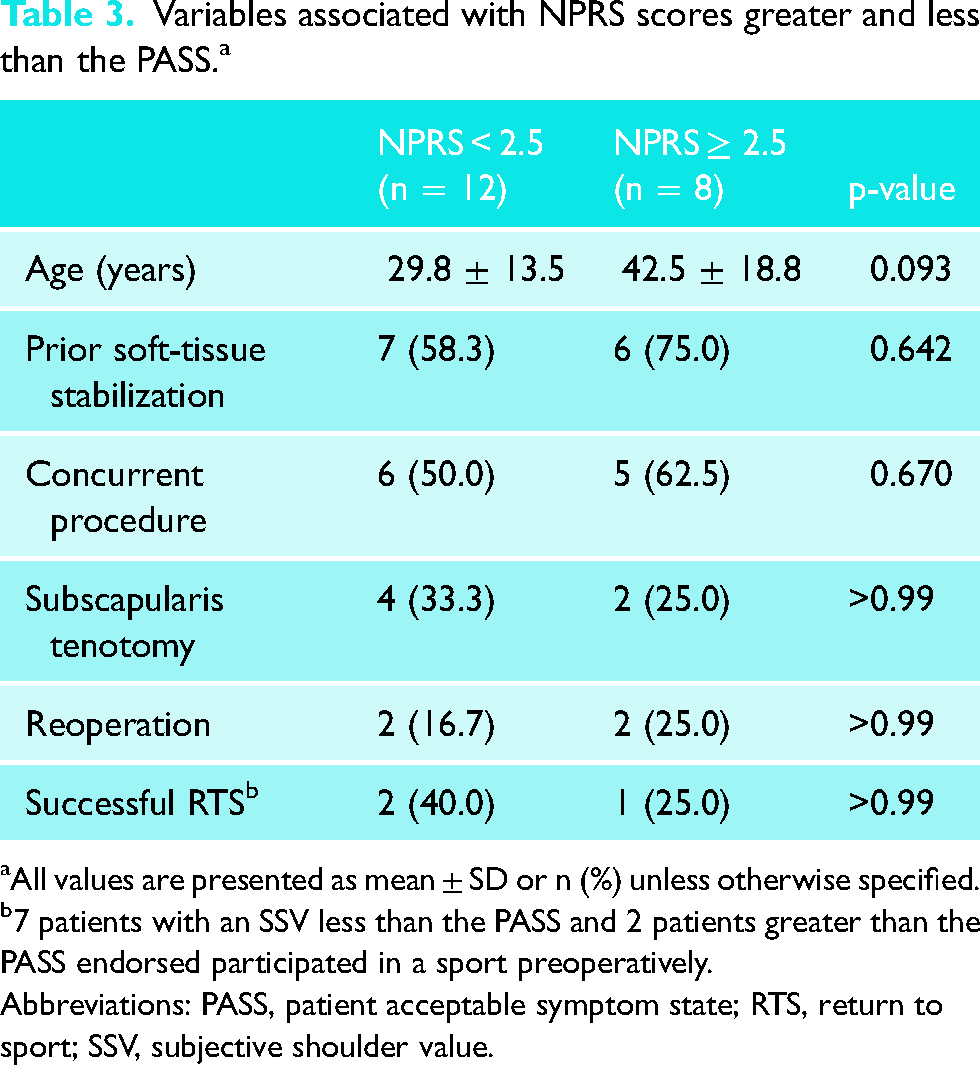
All values are presented as mean ± SD or n (%) unless otherwise specified.
7 patients with an SSV less than the PASS and 2 patients greater than the PASS endorsed participated in a sport preoperatively.
Abbreviations: PASS, patient acceptable symptom state; RTS, return to sport; SSV, subjective shoulder value.
Return to sport
Of the nine (45.0%) patients who reported playing a sport in the 3 years prior to surgery, 3 (33.3%) had a successful RTS at a mean of 19 months (range, 8–36 months) (Table 4). Among these three patients, the level of play upon return was variable (1 worse, 1 same, 1 better). Amongst the six patients (66.7%) who did not RTS, two (33.3%) cited a shoulder specific reason. Sport participation stratified by RTS status is outlined in Table 5.
Patient reported outcomes and RTS data after undergoing Latarjet procedure. a
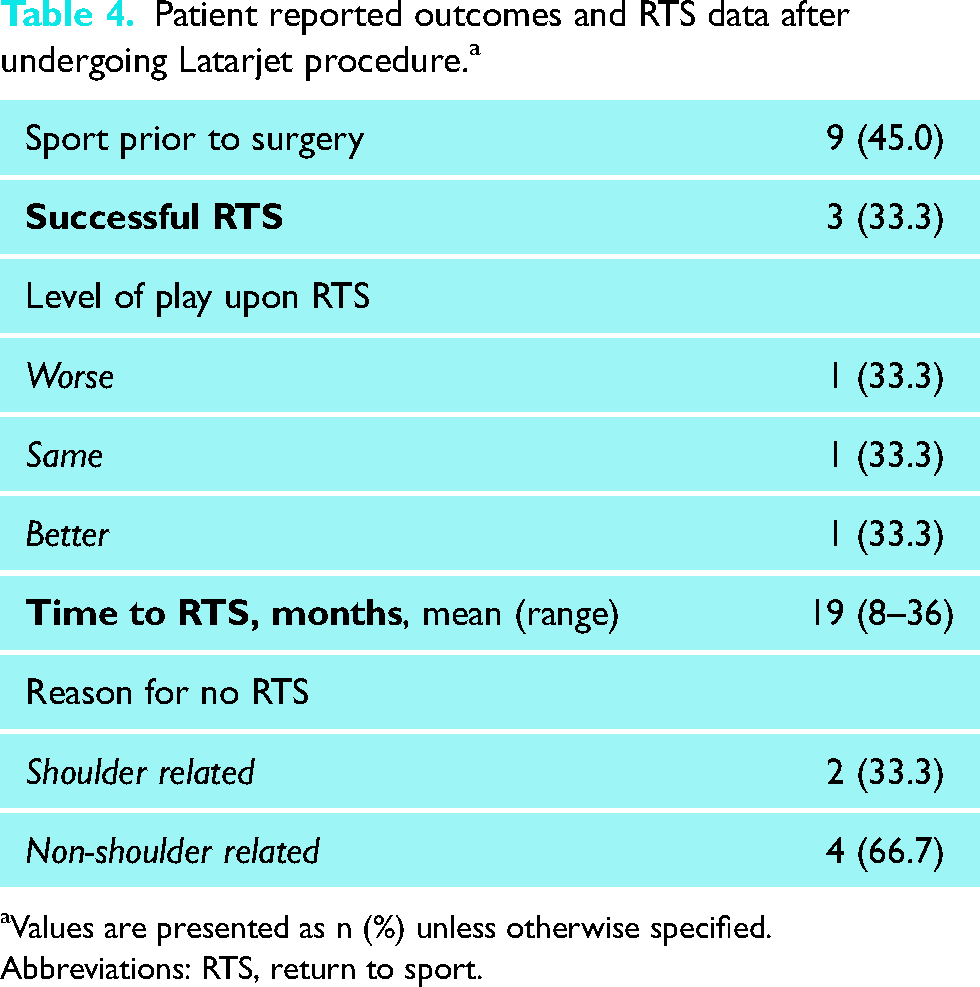
Values are presented as n (%) unless otherwise specified.
Abbreviations: RTS, return to sport.
RTS data categorized by initial sport. a
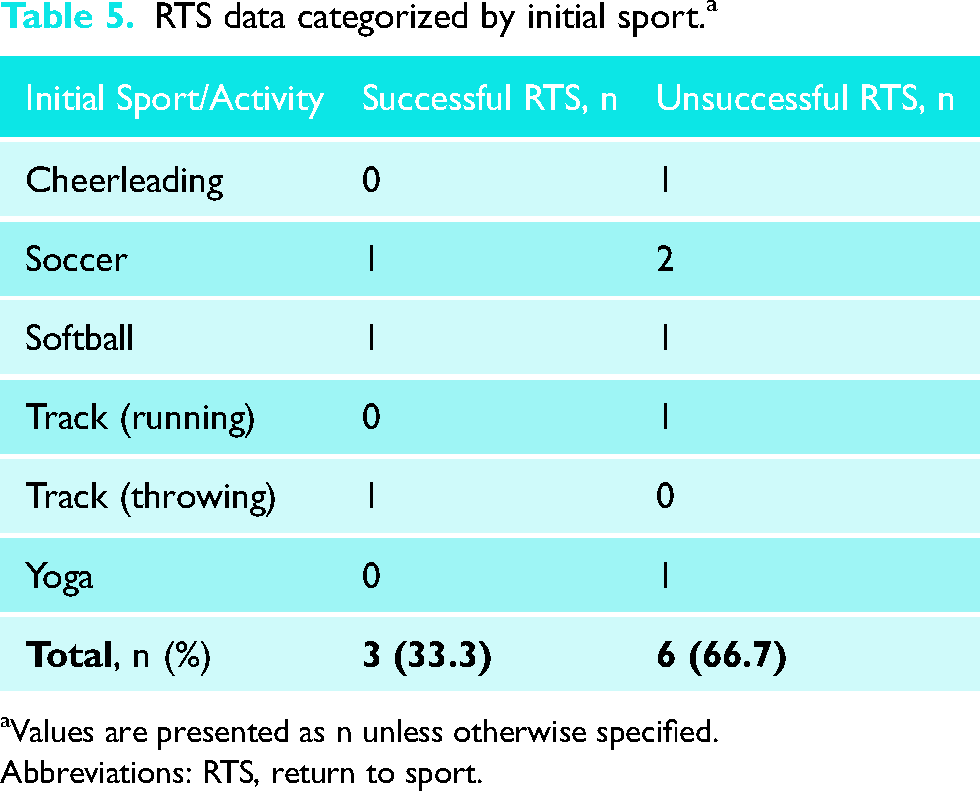
Values are presented as n unless otherwise specified.
Abbreviations: RTS, return to sport.
Reoperation
Four patients (20.0%) required reoperation at a mean of 27.1 months (range, 8.3–69.7 months). The average age at reoperation was 37 years (range, 19–67 years). One patient underwent a Latarjet procedure at age 66 after experiencing a traumatic anterior dislocation and associated comminuted glenoid rim fracture. After undergoing open reduction and internal fixation of the glenoid rim fracture, the patient continued to report recurrent episodes of subluxation at which point a Latarjet procedure was performed. This patient went on to require reverse total shoulder arthroplasty due to the development of posttraumatic arthritis limiting activities of daily living. One additional patient underwent total shoulder arthroplasty at the age of 34 due to the development of significant posttraumatic arthritis resulting in functional limitation. For the remaining two patients, one required screw removal due to symptomatic hardware, while the other underwent a diagnostic arthroscopy due to subjective feelings of recurrent instability. In this patient, no pathologic findings were identified intraoperatively, and no further intervention was undertaken.
Matched analysis
From the 20 female patients included in this study, 17 were able to be matched with a male counterpart on the basis of laterality and age (±3 years). Thirteen of the 17 pairs had complete follow-up data, thus a total of 26 patients (13 male, 13 female) were included in the matched analysis. One of the nine female athletes could not be matched to a male counterpart. Overall, a greater proportion of female patients (30.1% vs. 7.7%) underwent intraoperative subscapularis tenotomy while more male patients participated in a preoperative sport (10/13 [76.9%] vs. 8/13 [61.5%]) and reported a successful RTS, however, differences were not significant (Table 6). The mean time to RTS was 10 months (range, 4–24 months) for males and 19 months (range, 8–36 months) for females. Although there was a trend towards lower SSV scores in the female cohort, the difference did not reach statistical significance. No difference in NPRS scores was observed.
Patient demographics and outcomes when matched for laterality and age (± 3 years). a
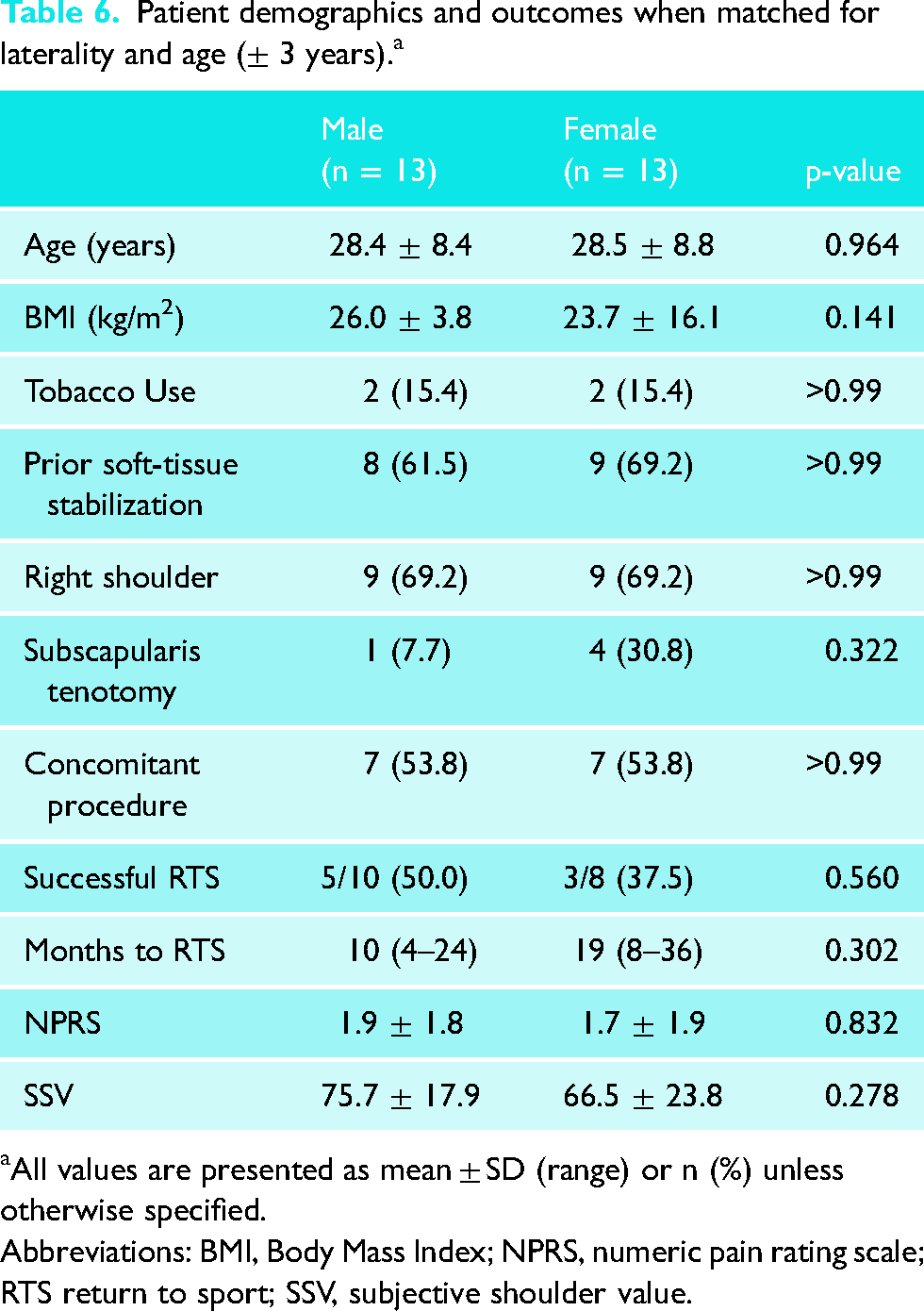
All values are presented as mean ± SD (range) or n (%) unless otherwise specified.
Abbreviations: BMI, Body Mass Index; NPRS, numeric pain rating scale; RTS return to sport; SSV, subjective shoulder value.
Discussion
Data regarding the outcomes of the Latarjet procedure in female patients remains limited with existing literature reporting conflicting results. Some studies have demonstrated a trend towards worse outcomes and lower rates of RTS when compared to males,8,12 while others have reported high rates of RTS and improved functionality.17,18 The findings from our study demonstrate pain levels similar to female-specific literature reports, but overall low subjective shoulder function and RTS amongst female patients undergoing the Latarjet procedure at mid-term follow-up. 18 Compared to propensity-matched males, females reported similar levels of pain and a trend towards lower subjective shoulder function and RTS.
Assessing shoulder function with the SSV, at final follow-up, the mean score across all female patients was 69.3 ± 22.0. Further, although not statistically significant, our study found that in comparison to patients above the PASS, patients below the PASS were older, had more frequently undergone soft-tissue stabilization prior to Latarjet, more frequently underwent subscapularis tenotomy intraoperatively, and were less likely to have had a successful RTS postoperatively. A case-series published by du Plessis et al. reported a median SSV score of 87 amongst female patients undergoing the modified Latarjet procedure.
12
Due to a paucity of data, the authors could not compare their findings to female-specific literature reports, but did note that their reported outcome scores were lower than those reported in the literature for case series of predominantly male patients.
12
Conversely, a prospective case-series recently published by Lima et al. reported significant improvement in postoperative shoulder function in female patients undergoing the Latarjet procedure.
17
At 3 year follow-up, patients reported improved shoulder function evaluated via the Western Ontario Shoulder Index (WOSI) and American Shoulder and Elbow Surgeons (ASES) score, with 100% of patients achieving the MCID for WOSI by 6 months.
17
Similarly, Frank et al. reported a significant improvement in ASES scores from 42.8 ± 19.5 to 80.7 ± 21.0 (p = 0.001) at a mean follow-up of 40.2 ± 22.9 months in female patients with
Regarding differences in outcomes between patients with and without prior soft tissue stabilization, similar to our findings, Werthel et al. reported inferior Simple Shoulder Test (SST) scores while Flinkkilä et al. reported inferior SSV and WOSI scores in patients undergoing a Latarjet procedure after a failed arthroscopic procedure.19,20 Conversely, in a retrospective cohort study of 205 open Latarjet procedures, Yapp et al. reported no differences in postoperative Quick DASH or WOSI scores between patients with and without prior stabilization surgery at a mean of 5.6 year follow-up (range, 2–11 years). 21
At an average of 73.8 months follow-up, the average NPRS score across all female patients was 2.2 ± 2.3. Similar to patients achieving the PASS for SSV scores, although statistically insignificant, patients achieving the PASS for NPRS scores were younger, had less frequently undergone soft-tissue stabilization prior to Latarjet, more frequently underwent subscapularis tenotomy intraoperatively, and were more likely to have had a successful RTS postoperatively. A retrospective cohort study Werthel et al. reported higher postoperative pain in patients undergoing the Latarjet procedure after a failed arthroscopic Bankart repair when compared to patients undergoing primary Latarjet, which is similar to our results. 19 In their study defining the PASS for VAS-pain after opening Latarjet, Menendez et al. found that 84.0% of patients achieved the PASS, a rate 24% higher than our study. 15 Amongst studies reporting sex-specific outcomes, VAS-pain scores as low as 0.92 have been reported in females at 2-year follow-up, further demonstrating the importance of additional data. 17
The results of this study further highlight potential discrepancies in the rate of RTS between male and female patients undergoing the Latarjet procedure. Amongst females, 3 of 9 (33.3%) reported a successful RTS. Sex-related differences in RTS are crucial to consider given the prevalence of shoulder instability in athletes and the overall importance of athletics on a patient's quality of life. A systematic review investigating rates of RTS after the Latarjet procedure reported an RTS rate of 89% at a mean of 5.8 months (range, 3.2–8 months), however, outcomes were not stratified by sex. 22 Studies reporting on rates of RTS in female patients have reported rates between 30% and 93%.12,17,18 Additionally, there remains a paucity of data regarding the role of competition level on rates of RTS amongst female athletes. In a study incorporating multiple professional and overhead athletes, Lima et al. reported an RTS of 93%, clarifying that differences in outcomes between amateur and professional athletes remain unclear. Although our rate of RTS is on par with several studies investigating female-specific rates of RTS after undergoing the Latarjet procedure, it is clear that this significant disparity precludes any definitive conclusions from being made and further clarifies the lack of understanding regarding sex-related differences in physiology, mechanism of injury, and rehabilitation.
Rates of reoperation after the Latarjet procedure are highly variable with rates ranging between 1% and 17%.12,17,18,23–26 The rate of reoperation in this study was 20%, with 4 of 20 female patients undergoing reoperation at a mean of 27.1 months (range 8.3–69.7 months). Two patients (10%) required conversion to shoulder arthroplasty. Amongst female-specific literature, Frank et al. reported a reoperation rate of 11.8%. Specifically, one patient required proximal biceps tenodesis and arthroscopic cuff debridement for a rotator cuff tear, while another required total shoulder arthroplasty for recurrent instability. 18 In a cohort of 29 female patients du Plessis et al. reported a reoperation rate of 13.8%, with three patients undergoing an Eden-Hybinette procedure for recurrent instability, and one patient undergoing arthroscopy and removal of screws for graft fracture. 12 More generally, in a systematic review of patients undergoing bony stabilization for anterior shoulder instability, amongst 45 studies and 1904 shoulders, Griesser et al. reported a pooled reoperation rate of 7% at a mean follow-up of 6.8 years. A total of 46 patients (34.8%) required hardware removal, while 5 (3.8%) ultimately required total shoulder arthroplasty. 26 The slightly higher rate of reoperation observed in this study is likely a reflection of the follow-up time and the influence of small sample size on reoperation rates expressed as a percentage. Older age could also be a contributing factor. Prior studies have reported female patients to have a higher age at primary dislocation and surgery therefore our study group may differ from those more commonly described in the literature.10,12 Further, in a series of 30 patients undergoing shoulder arthroplasty after prior Latarjet surgery, Willemot et al. reported a mean time between coracoid transfer and arthroplasty of 20 years, further demonstrating the importance of long-term follow-up. 27
Compared to propensity matched males, female patients reported an SSV score 9.2 points lower (75.7 ± 17.9 vs. 66.5 ± 23.8, p = 0.278). Although this difference is less than the 12.4 point minimal clinically important difference (MCID), 15 there exists a trend towards worse shoulder function in female patients. In a retrospective case-control study evaluating outcomes in patients after either Bankart repair or the Bristow-Latarjet procedure, Hovelius et al. reported a trend towards worse SSV scores in female patients (78.3 vs. 80.8, p = 0.172) at a mean of 17 years (range, 13–22 years). 8 Sex-specific outcomes were not stratified by procedure type. It has been theorized that variation in anatomy between males and females may contribute to differences in postoperative shoulder function. Morphologic differences including coracoid width, length, and thickness have been identified, which may be of particular importance during the mid-range of rotation where the coracoid contributes an estimated 38% to 49% to stability.28–31
Compared to propensity matched males, female patients reported similar postoperative NPRS scores (1.7 ± 1.9 vs. 1.9 ± 1.8, p = 0.832). In a series 17 female patients undergoing the Latarjet procedure, Frank et al. reported a post-operative VAS-pain score of 1.4 ± 2.6. 18 With an estimated 36% of patients reporting residual shoulder pain 10 years after the Latarjet procedure, postoperative pain and improvement from preoperative levels remains an important and complex consdieration. 32 Although likely multifactorial in origin, it is possible that progressive glenohumeral degeneration contributes to the prevalence of long-term pain. 33
This study is not without limitation as it is a single-center retrospective investigation of a population less frequently affected by glenohumeral instability. Relatively low follow-up (66.7%) may have introduced attrition bias, and a lack of preoperative measurements prevented quantification of patient improvement over time. The use of the SSV in isolation without an adjunctive process-based PRO limits conclusions regarding whether clinical objectives were achieved. Given the overall small cohort, matching was only performed on the basis of age and laterality, with other potentially important variables including method of subscapularis management, concomitant procedures, and type of sport not considered. It should be noted that only laterality (i.e., side of surgical procedure) was considered, and not hand dominance. This decision was made because hand dominance was not reliably available in a retrospective manner and therefore unable to be used to generate the matched cohort. Because this was a convenience sample, three female patients were unable to be matched to a male counterpart, thus compromising the strength of the matched analysis. Additionally, 13 (65%) of the included patients had undergone prior soft tissue stabilization which is relevant as bony reconstruction after failed prior surgical intervention has been associated with inferior outcomes. 25 Further, we did not quantify glenoid bone loss which may contribute to patient outcomes given the potential relevance of coracoid graft size. Lastly, this was a convenience sample and therefore the study was almost certainly underpowered to detect significant differences in postoperative outcomes. Nonetheless, the presented results highlight sex-specific trends in outcomes after the Latarjet procedure. Our investigation is one of few focusing on females undergoing the Latarjet procedure thus bringing awareness to the need for future studies regarding this population.
Conclusion
At mid-term follow-up female patients reported pain levels similar to female-specific literature reports, but overall low subjective shoulder function and RTS. Compared to propensity-matched males, females reported similar levels of pain, lower shoulder function, and lower rates of RTS, however, differences did not reach statistical significance. The role of patient sex should be explored further as a variable to be taken into consideration when determining appropriate treatment options for shoulder instability.
Footnotes
Previous communication
A portion of the data will be presented as a poster at the AOSSM 2023 Annual Meeting.
Contributorship
All 11 authors meet full four-point ICMJE criteria for authorship. ANB: The Author declares that there is no conflict of interest. AJR: The Author declares that there is no conflict of interest. AGD: The Author declares that there is no conflict of interest. AAH: The Author declares that there is no conflict of interest. JDM: The Author declares that there is no conflict of interest. AMI: The Author declares that there is no conflict of interest. DPT: The Author declares that there is no conflict of interest. JEF: The Author declares that there is no conflict of interest. SCS: Author SCS is a paid consultant for Medacta. NH: Author NH is a paid consultant for Stryker. BMS: Author BMS receives research support from Arthrex, Inc. and publishing royalties, financial, or material support from Nova Science Publishers.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB approval
Wake Forrest School of Medicine IRB (IRB00084659)
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Guarantor
BMS
Informed consent
This research meets the criteria for a waiver of written (signed) consent according to 45 CFR 46.117(c)(2). This research meets the criteria for a waiver of HIPPA authorization according to 45 CFR 164.512. Verbal consent was obtained from all patients prior to obtaining outcomes data.