
Abstract
Background
The purpose of this study was to systematically review the rate and timing of return to play in overhead athletes following operative management of anterior shoulder instability.
Methods
A systematic literature search based on PRISMA guidelines, utilizing the EMBASE, MEDLINE, and The Cochrane Library Databases. Eligible for inclusion were clinical studies reporting on return to play among overhead athletes following arthroscopic Bankart repair, open Latarjet procedure or Remplissage procedure.
Results
There are 23 studies included with 961 patients. Among those undergoing arthroscopic Bankart repair, the rate of return to play was 86.2%, with 70.6% returning to the same level of play and the mean time to return to play was 7.1 months. Among those undergoing an open Latarjet procedure, the rate of return to play was 80.9%, with 77.7% returning to the same level of play and the mean time to return to play was 5.1 months. Among those undergoing a Remplissage procedure, the rate of return to play was 70.6%, with 70.0% returning to the same level of play or mean time to return to play.
Discussion
Overall, there were high rates of return to play following operative management of anterior shoulder instability in overhead athletes.
Introduction
Traumatic anterior shoulder instability is a common injury among young, athletic populations with risk being greatest among males and athletes involved in collision sports. The incidence of anterior shoulder instability in the general population is estimated to be 1% to 2%,1,2 but in a collegiate athletic population it was estimated to be as high as 0.12 per 1,000 athlete exposures. 3 Operative management has been shown to not only reduce the rate of recurrent instability,4,5 but also result in subsequently higher rates of return to play (RTP) among athletic populations.6,7
In overhead athletes, surgical management of anterior shoulder instability may result in a loss of external rotation, which may limit the athlete's ability to RTP at their pre-injury level 8 ; therefore, special attention needs to be placed in the management of this specific population. There are multiple operative treatment options for anterior shoulder instability, including arthroscopic Bankart repair, the Latarjet procedure, and the Remplissage procedure, with each having their own relative indications based on the type of defect or lesion and potential advantages and disadvantages.2,9–13 Even though RTP after shoulder instability surgery has been thoroughly studied among other high-shoulder-demanding populations, such as collision athletes, RTP outcomes in overhead athletes are lacking. As such, despite RTP being a critical gauge for postoperative success in athletes, to date, there is a need for studies to systematically evaluate rates and times of RTP after shoulder instability surgery in overhead athletes.
The purpose of this study was to systematically review the rate and timing of RTP in overhead athletes following operative management of anterior shoulder instability. Our hypothesis was that there would be a low rate of RTP among overhead athletes due to potential decrease in range of shoulder motion following operative management of anterior shoulder instability.
Methods
Study selection
The literature search was performed by two authors (K.L. and M.B.), who used PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines and reviewed the search results; a senior author (E.H.) arbitrated on any disagreement. The titles and abstracts identified in the search were screened, and potentially eligible studies received a full-text review.
Search strategy
The following search terms were used in PubMed, and EMBASE databases in August 2022 as the search algorithm: (Bankart or Latarjet or Remplissage) and (overhead or athlete or sport or return to sport [RTS] or play or RTP). No time limit was given to publication date.
Eligibility criteria
The inclusion criteria were the following: (1) clinical study on athletes, amateurs and professionals, participating in overhead sports, such as baseball, basketball, football, volleyball, handball, badminton, tennis, softball, weightlifting, judo, swimming, and rock climbing, (2) reported on RTP, ((3) operative management of anterior shoulder instability, including both primary and revision stabilization, (4) published in a peer-reviewed journal, and 5) published in English. The exclusion criteria were the following: (1) review studies, (2) cadaveric studies, (3) biomechanical studies, (4) case reports, and (5) abstract only.
Data extraction and analysis
The relevant information regarding the study characteristics, including the study design, the level of evidence (LOE), the methodological quality of evidence (MQOE), the population, clinical outcome measures, and the follow-up time points, was collected by two blinded reviewers (K.L. and M.B.) using a predetermined data sheet, with the results compared by a third independent reviewer (E.H.). The LOE was evaluated based on the guidelines by the Oxford Centre for Evidence-Based Medicine. 14 The MQOE was evaluated by use of a modified Coleman methodology score. 15 Studies were considered excellent quality if they scored 85–100, good quality if they scored 70–84, fair quality if they scored 55–69, and poor quality if they scored less than 55. The criteria for quality of RTP were based on the previously published criteria of Zaman et al. 16 These criteria consisted of RTP timeline, conditional criteria, measurement of conditional criteria, and rehabilitation protocol. A score of 4 indicated well-defined RTP criteria, a score of 1–3 indicated poorly defined criteria, and a score of 0 indicated no criteria. Clinical outcomes extracted and analyzed were (1) overall rate of RTP and return to previous levels among overhead athletes; (2) time of RTP; (3) sports-specific RTP; (4) RTP criteria; and (5) recurrent instability; defined as subluxation or dislocation after stabilization.
Statistics
Quantitative statistical analysis was performed by use of Microsoft Excel.
Results
Literature search
The initial literature search resulted in 2222 total studies. After removal of duplicates, the articles were screened for inclusion and exclusion criteria, and 1652 unique studies were evaluated, and full texts were assessed for eligibility. This review included 23 clinical studies (Figure 1).
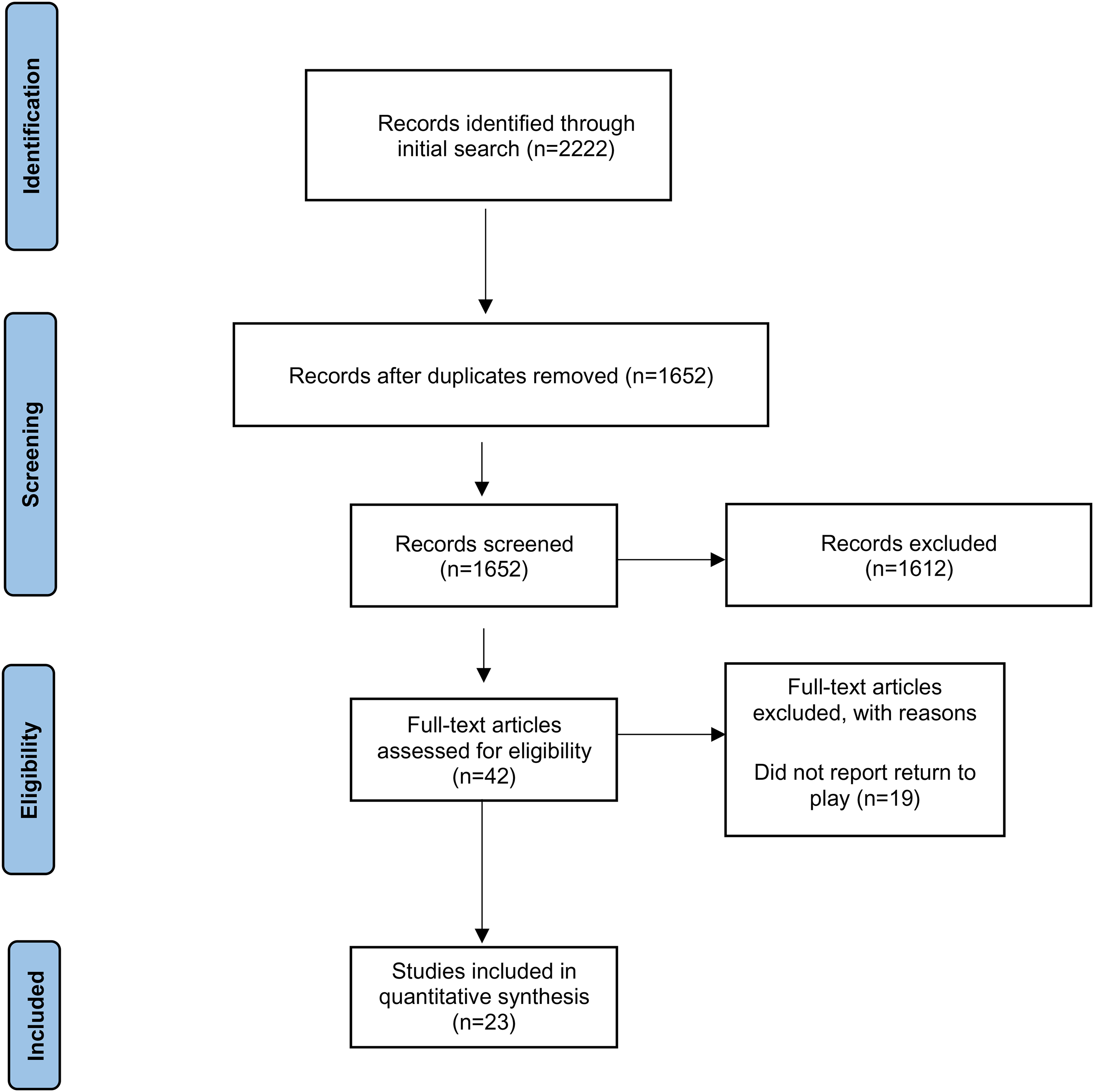
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) study selection flow diagram.
Study characteristics and patient demographics
Our review found 23 studies including 961 patients that met our inclusion criteria. The mean MQOE of the studies was 68, which is the top end of fair quality evidence. Out of the studies that reported sex demographics for overhead sports most patients were male (86.1%), with a mean age of 25.1 years and a mean follow-up of 42.7 months. The study characteristics and patient demographics are shown in Table 1.
Study demographics.
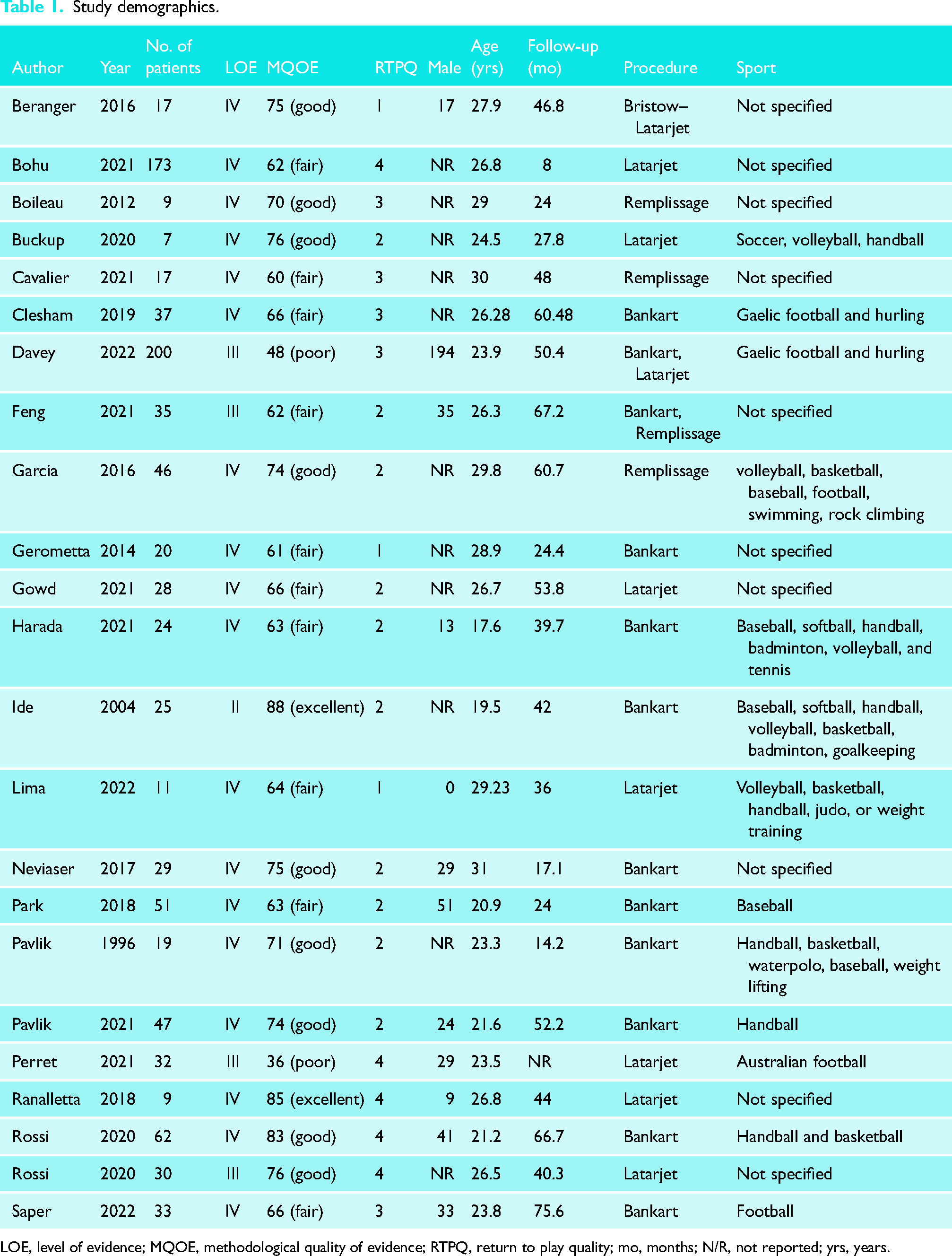
LOE, level of evidence; MQOE, methodological quality of evidence; RTPQ, return to play quality; mo, months; N/R, not reported; yrs, years.
Arthroscopic Bankart repair
Among those undergoing arthroscopic Bankart repair, the rate of RTP was 85.5%, with 70.6% returning to the same level of play. Furthermore, the mean time to RTP was 7.1 months. Recurrent instability occurred in 5.8% of athletes.8,17–27
Open Latarjet procedure
Among those undergoing an open Latarjet procedure, the rate of RTP was 80.9%, with 77.7% returning to the same level of play. Furthermore, the mean time to RTP was 5.1 months. Recurrent instability occurred in 4.4% of athletes.25,28–35
Remplissage procedure
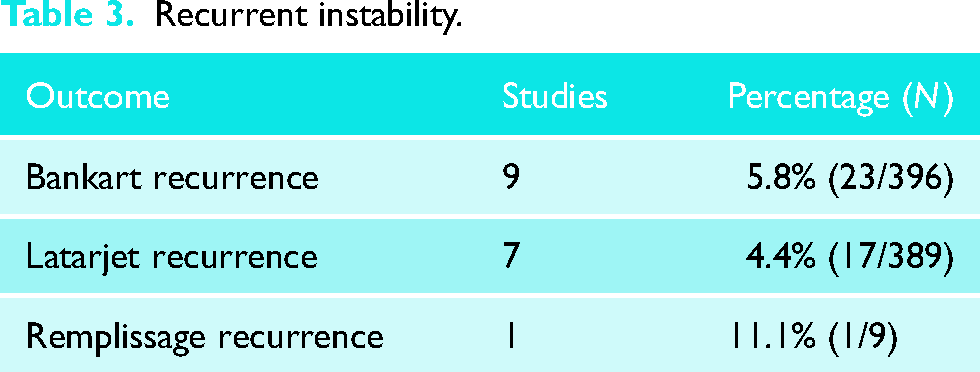
Among those undergoing a Remplissage procedure, the rate of RTP was 70.6% with 70% returning to the same level of play. No studies reported on the mean time of RTP for a Remplissage procedure. One study reported recurrent instability in one athlete after stabilization.23,36–38
RTP is shown in Table 2. Recurrent instability is shown in Table 3.
Return to play.
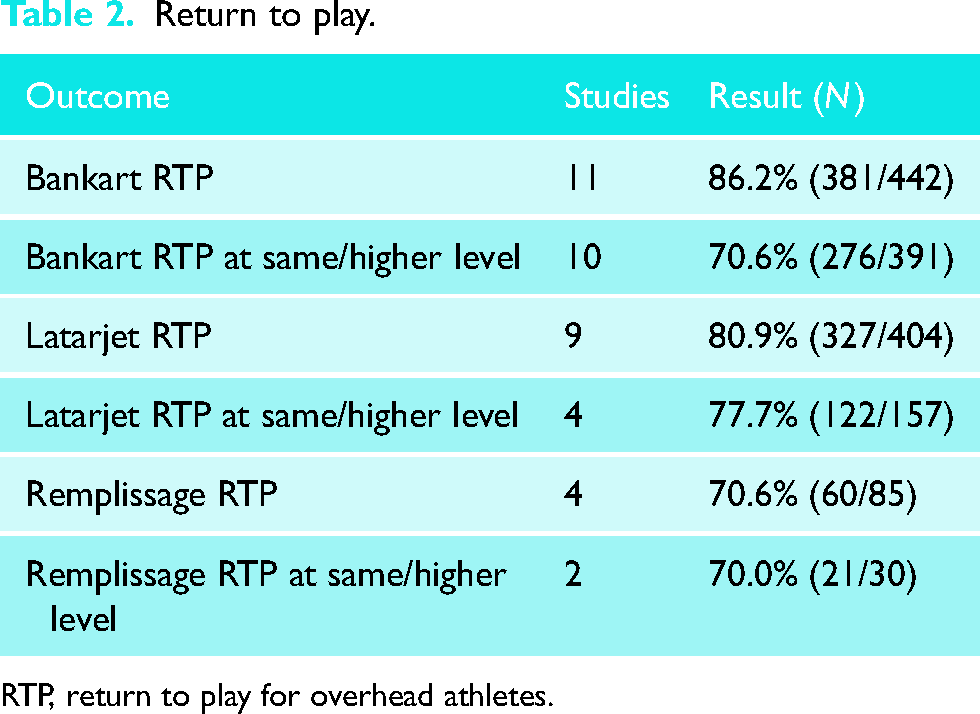
RTP, return to play for overhead athletes.
Sports-specific return to play
Analysis of sports-specific RTP demonstrated that majority of athletes were able to return to their sport and return at a similar or higher level. Athletes participating in swimming, judo, or weight training had the greatest rate of RTP, 100%, while rock climbers had the lowest, 50%.34,36 However, 100% of the volleyball players that returned to play were able to return at the same or higher level of intensity alongside athletes participating in weight training and judo.8,34,36 Tennis and softball had the lowest rate of return to pre-injury level, 50%. 8 Sports-specific RTP is shown in Table 4.
Sports-specific return to play.
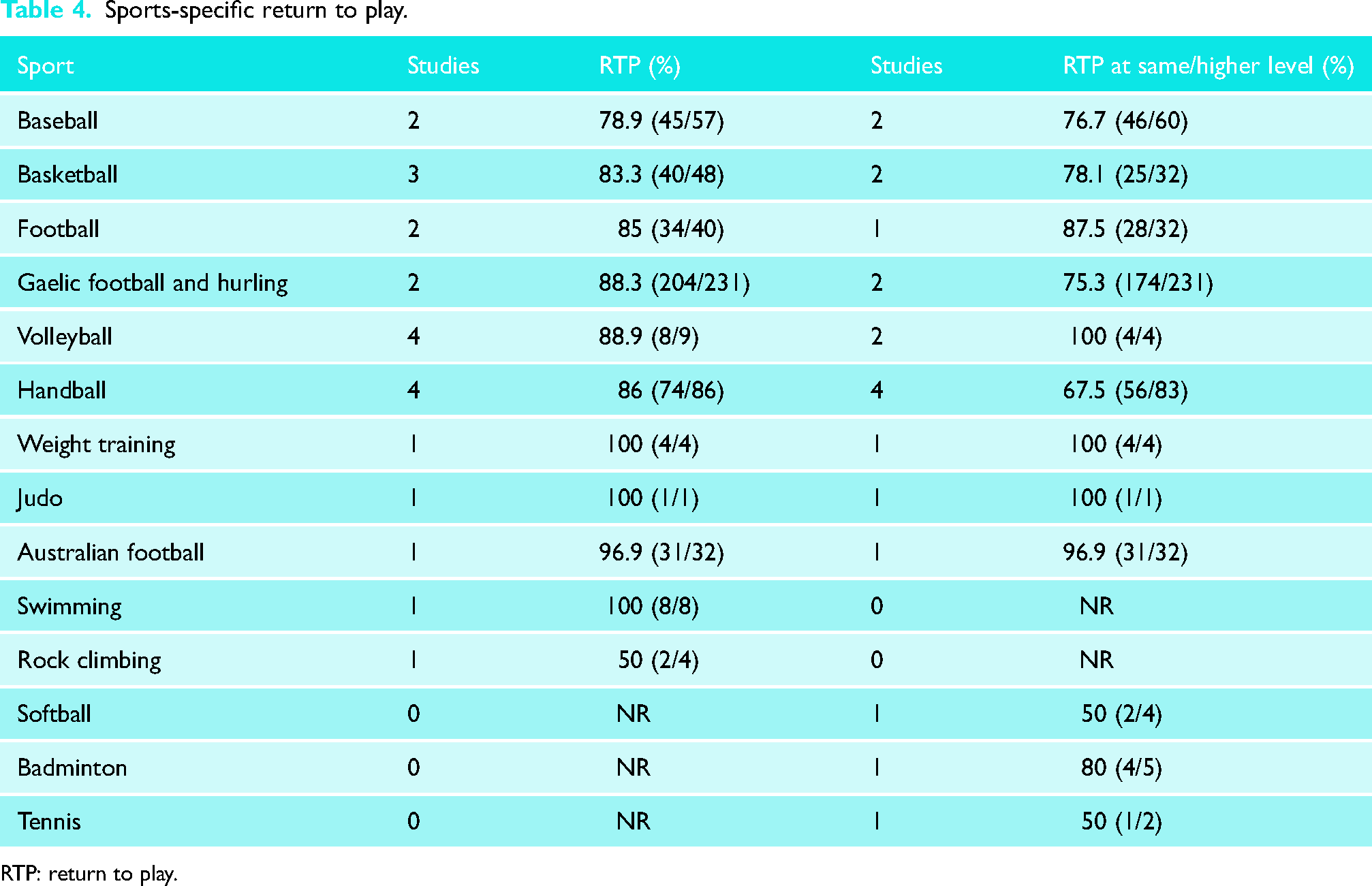
RTP: return to play.
Return to play criteria
The overall RTP criteria were reported in the majority of the studies (100%); time to RTS was the most commonly reported item (100%). A wide discrepancy was found in reported time of return, ranging from 3 to 11 months, with 4 months being the most commonly used time point (65.2%). Other criteria, including computed tomography imaging to assess bone union (4.3%), clinical examination or decision (8.7%), strength (13.0%), pain (21.7%), and range of motion (17.4%), were less commonly reported. The mean score for quality of RTP criteria was 2.5 (range, 1–4) (Table 5).
RTP criteria.
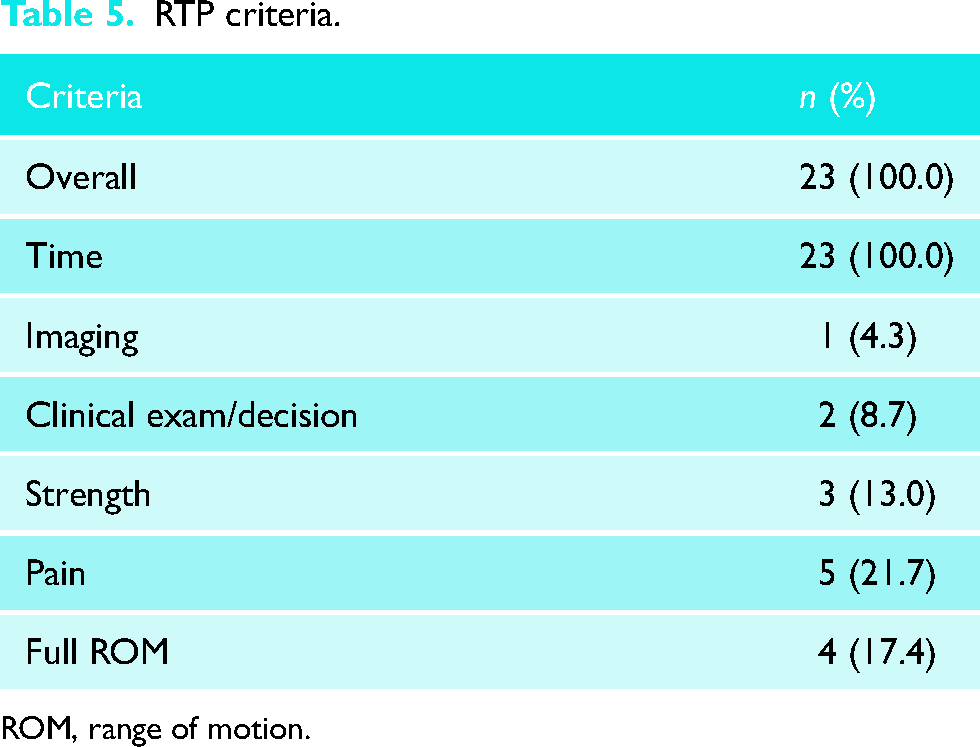
ROM, range of motion.
Discussion
The most important finding from the current study was that there were high rates of RTP following operative management of anterior shoulder instability in overhead athletes. Second, there was a drop off in the rate of athletes that were able to RTP at their previous competitive level. Third, there was a high variability in the RTP outcomes. Fourth, there was a low rate of recurrent instability after operative management in this population (Table 3). Finally, even though this systematic review provides important insights regarding RTP outcomes following shoulder instability surgery, it also highlights the lack of literature on overhead athletes following anterior shoulder instability surgery.
Recurrent instability.
RTP is often an athlete's primary concern with anterior shoulder instability. Indeed, Hurley et al. 39 found that the biggest predictor of satisfaction at 5-year post-surgical intervention was the ability to RTP. Overall, we found high rates of return to sports irrespective of surgical technique ranging from 70% to 86% with mean times of RTP of 5 to 7 months. We hypothesized low rates of RTP due to possible loss of external rotation after surgical management. However, our findings suggest that overhead athletes are still able to RTP at high rates indicating that loss of motion may not be clinically significant for all overhead athletes. Moreover, RTP to pre-injury levels rates were 71% for arthroscopic Bankart repair and 77% for Latarjet procedure. This is consistent with previous reports, in a systematic review Hurley et al. 40 analyzed RTP outcomes following Latarjet procedure finding an overall RTP rate of 90% and a return to the same level of play of 81% in overhead athletes with a mean time to return to sports of 6 months. These findings suggest that not all athletes may be able to RTP at their pre-injury level or at all; therefore, patient expectations should be set when they are having their pre-operative counseling.
Moreover, we found a wide variation in RTP and return to same level rates following shoulder instability surgery. Several factors have been shown to influence the ability to RTS following shoulder instability surgery. First, it is still unclear how and when to clear an athlete to safely return to sports among studies. Indeed, previous studies have emphasized the necessity of specific criteria for the RTP. Ciccoti et al. 41 systematically evaluated the criteria for RTS after surgical stabilization of anterior shoulder instability, identifying 13 different combinations of criteria for returning to sports, which highlights the lack of consensus among experts regarding this topic. Therefore, further validation of criteria in overhead athletes may thus be useful to optimize outcomes in these patients.
Second, psychological factors have been shown to play an important role in return to sports following shoulder instability surgery.42–44 Indeed, Rossi et al. 42 and Hurley et al.45,46 evaluated athletes who failed to RTP after the Latarjet procedure and arthroscopic Bankart repair, finding that psychological readiness to RTP was predictive of an athlete’s ability to return to sports and return to the same level of play.
Third, the type of sport, type of athlete, and position of play may have a significant impact on RTP outcomes. In our analysis of sports-specific RTP, the percentage of athletes who were able to RTP at the same level ranged from 50% to 100%, the lowest being handball and the greatest being volleyball, weight training, and judo; although only one patient participated in judo. These findings are consistent with Rossi et al. 42 finding a lower rate of return to pre-injury level in contact sports that posed a high demand on the shoulder due to repetitive trauma from contact with another competitor or the floor (martial arts) as opposed to a higher rate of return to pre-injury level in sports that did not require as great of a demand on the shoulder. There are also differences in RTP based upon position of play. For instance, Park et al. 18 analyzed RTP outcomes in elite professional baseball players finding high rates RTP and levels of play of 82% and 80%, respectively. However, these values varied significantly among positions pitchers, catchers, and field positions, with pitchers showing lower rates of RTP and a higher rehabilitation time period. Similarly, Lu et al. 47 analyzed national Basketball Association players who sustained a shoulder instability event, showing that 100% of athletes RTP after shoulder instability surgery. The purpose of this observation is to emphasize the importance of clearly distinguishing amateur and professional athletes and playing positions before undergoing surgery to provide them with specific and appropriate counseling.
We also considered if outcomes differed between patients undergoing primary surgery as compared to those undergoing revisions. Although several of the studies included both groups, only two studies28,30 compared outcomes between these two patient populations. Neither of which found a statistically significant difference in rate of RTP nor time to RTP between patients receiving primary or revision surgery.
Moreover, one of the main challenges in returning overhead athletes to play is restoration of range of motion necessary to perform the sport-specific tasks, which may itself be impacted by the initial instability event. Following this, operative intervention may further cause a restriction in range of motion. While a randomized controlled trial found arthroscopic Bankart repair resulted in worse abducted external range of motion than non-operative management, this is the most anatomic procedure and may result in improved motion compared to the Latarjet procedure and Remplissage. There is a concern in performing a Latarjet procedure as it is non-anatomic and may limit range of motion or have negative implications for throwing mechanics in this population. 48 Furthermore, performing a subscapularis tenotomy as opposed to a subscapularis split approach may result in worse range of motion and strength, and is thus inadvisable in this group. 49 Finally, with the Remplissage procedure, the infill with the infraspinatus has been shown to result in loss of external rotation which can impact throwing. However, this can be minimized by placing the anchor in the safe zone at least 1 cm lateral and no greater than 3 cm distal to the acromion, and avoiding over medialization. 50 Therefore, future biomechanical and clinical studies are needed to ascertain how the various operative techniques impact throwing motions or the sport-specific overhead abilities.
Limitations
This study has some limitations. Most of the studies in the analysis were retrospective, and thus all the limitations of these studies apply. Additionally, due to lack of controls it was not possible to perform a meta-analysis of the outcomes and compare rates of RTP among the various procedures. Additionally, due to report inconsistencies in the included studies, it was not possible to analyze potential risk factors that may account for inability to RTP. Finally, majority of the studies did not provide sports-specific data; thus, our analysis of sports-specific RTP was limited.
Conclusion
Overall, there were high rates of RTP following operative management of anterior shoulder instability in overhead athletes. Further studies evaluating RTP outcomes while accounting for sources of variation such as RTP criteria, type of sport, type of athlete, and type of surgery are still needed.
Footnotes
Author contributorship
KL and MB independently conducted the title and abstract and full-text review. They also were responsible for data collection and drafted the manuscript. Any disagreements were arbitrated by EH, who also created the study idea, participated in its design, and assisted in drafting the manuscript. JL, IP, SF, OA, and CK critically reviewed and revised the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Not applicable.