
Abstract
Objective
To systematically scope the literature on posterior shoulder tightness (PST) and define a therapist-instructed and therapist-administered management framework.
Design
Scoping review.
Literature search
We searched MEDLINE, EMBASE, CINAHL, Scopus and Google Scholar from inception to December 2021.
Study selection criteria
Peer-reviewed studies written in English, French, Greek, Japanese or Tamil, with extractable pre- and post-intervention data. Physiotherapy interventions amenable for posterior shoulder structural (muscle, capsule) causes of PST within an adult population.
Data synthesis
Arksey and O’Malley's framework was implemented and the PRISMA extension for scoping reviews directed our data synthesis. The data charted from each study included authors, title, study year, location, study design; participant number, age, sex; PST intervention and parameters; patient-reported outcomes; and results. Themes were organized into therapist-instructed and therapist-administered rehabilitation strategies, as well as combined treatment methods.
Results
Of 2777 articles identified from our search strategy, 21 articles were included. Therapist-instructed interventions included cross-body stretch (CBS), sleeper stretch (SS), a combination of the two and general stretching. Therapist-administered interventions included CBS, SS, instrument-assisted soft tissue mobilization (IASTM), muscle energy techniques, dry needling and Fauls protocol (12 therapist-assisted stretches). Combined interventions of tape with self-stretching and IASTM and stretching were also identified.
Conclusion
Based on the current evidence, CBS and SS are the most researched treatments for PST and seem to be effective at improving PST. Furthermore, stabilization of the scapula while performing these stretches optimized the stretch targeted to the PST and ROM benefits for horizontal adduction.
Introduction
Posterior shoulder tightness (PST) is a common impairment found in both athletic and nonathletic populations.1–10 It is defined as the “limitation of the extensibility within the posterior shoulder including contractile (muscle), non-contractile elements (capsule) and osseous changes as seen in the form of humeral torsion.” 11 A correlation between PST and increased injury rates has been documented in the literature, especially in overhead athletes.2,4,12–14 Various shoulder diagnoses are associated with contractile, non-contractile and bony structures. While these diagnoses may present with decreased horizontal adduction (HAdd) and internal rotation (IR), their clinical history will often differ in presentation. PST reduces glenohumeral joint (GHJ) range of motion (ROM) into HAdd and IR.11,15,16 The shoulder has complex motion and PST has been associated with a variety of shoulder issues such as glenohumeral internal rotation deficit (GIRD),16–20 subacromial impingement,21–25 anterior and posterior glenohumeral laxity,4,21,26 scapular dyskinesia6,19,27–29 and internal impingement of the shoulder.4,30–32 Therefore, the term PST will be used to describe decreased HAdd, IR and low flexion (LF) based on tightness associated with posterior shoulder structures such as the infraspinatus, teres minor, posterior deltoid muscles and posterior glenohumeral capsule.8,11,15,16 Since it is difficult to differentiate the posterior GHJ structures with active and passive mobility testing both contractile and non-contractile structures will be considered involved in PST.
Despite the breadth of research regarding non-operative PST assessment and treatment in the literature, there continues to be a lack of consensus regarding best practice for clinical management of PST. A recent systematic review and meta-analysis by Salamh et al. 33 analyzed the efficacy of non-operative interventions to improve PST. Their review concluded that therapist-administered interventions had a moderate effect size of improving PST ROM. 33 While Salamh's review concludes therapist-administered interventions play a role in treatment, the review did not explore the various intervention components within these treatments, for example, therapist-provided or -instructed stretching.
There are many barriers to implementing evidence-based practice (EBP) in physiotherapy. Namely, one barrier to EBP implementation is the lack of resources for multiple journals. One method to ameliorate this lack of resources is to provide robust reviews of common rehabilitation topics. 34 Our initial search revealed a lack of consensus for PST treatment and no clinician protocol or treatment parameters to inform frequency, intensity, duration, etc. Individual studies may widen the breadth of knowledge on a topic such as PST, but for that research to make a clinically important difference in a patient's life, the research findings must be usable as well as robust. 35 The primary objective of this scoping review was to identify non-operative rehabilitation strategies for the posterior shoulder structures (infraspinatus, teres minor, posterior deltoid muscles, posterior glenohumeral capsule) that cause PST.
Methods
Framework/design
Due to the broad research question and emerging evidence base on PST, a scoping review methodology following Arksey and O’Malley's 5-step framework was selected. 36 This review was reported according to the PRISMA Extension for Scoping Reviews and registered with Open Science Framework https://osf.io/c7dxr. 37 Due to the exploratory nature of scoping reviews, formal quality assessment of included studies was not performed. 38 The study team consisted of two expert physiotherapists, an orthopedic surgeon subspecialized in the care of shoulder disorders, a Ph.D. candidate and four Advanced Health Care Physiotherapists.
Search
The systematic search strategy was developed and refined by the research team with assistance from an experienced health sciences librarian (Appendix A). Appropriate search terms were identified and combined using Boolean operators. A search of five electronic databases (MEDLINE, EMBASE, CINAHL, Scopus and Google Scholar) from inception to December 18, 2021 was conducted. All references were imported to Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org) and duplicates were removed. Relevant reference lists and book chapters were hand searched for additional resources.
Study selection
Once duplicates were removed, titles and abstracts were initially screened for relevance, followed by a full-text review using predetermined inclusion and exclusion criteria (Table 1). All manuscripts were separately reviewed by two pairs of reviewers (YF, MK; HT, MA) and conflicts were resolved by discussion and/or a third expert reviewer (KJF, JS).
Inclusion and exclusion criteria for posterior shoulder tightness treatment.
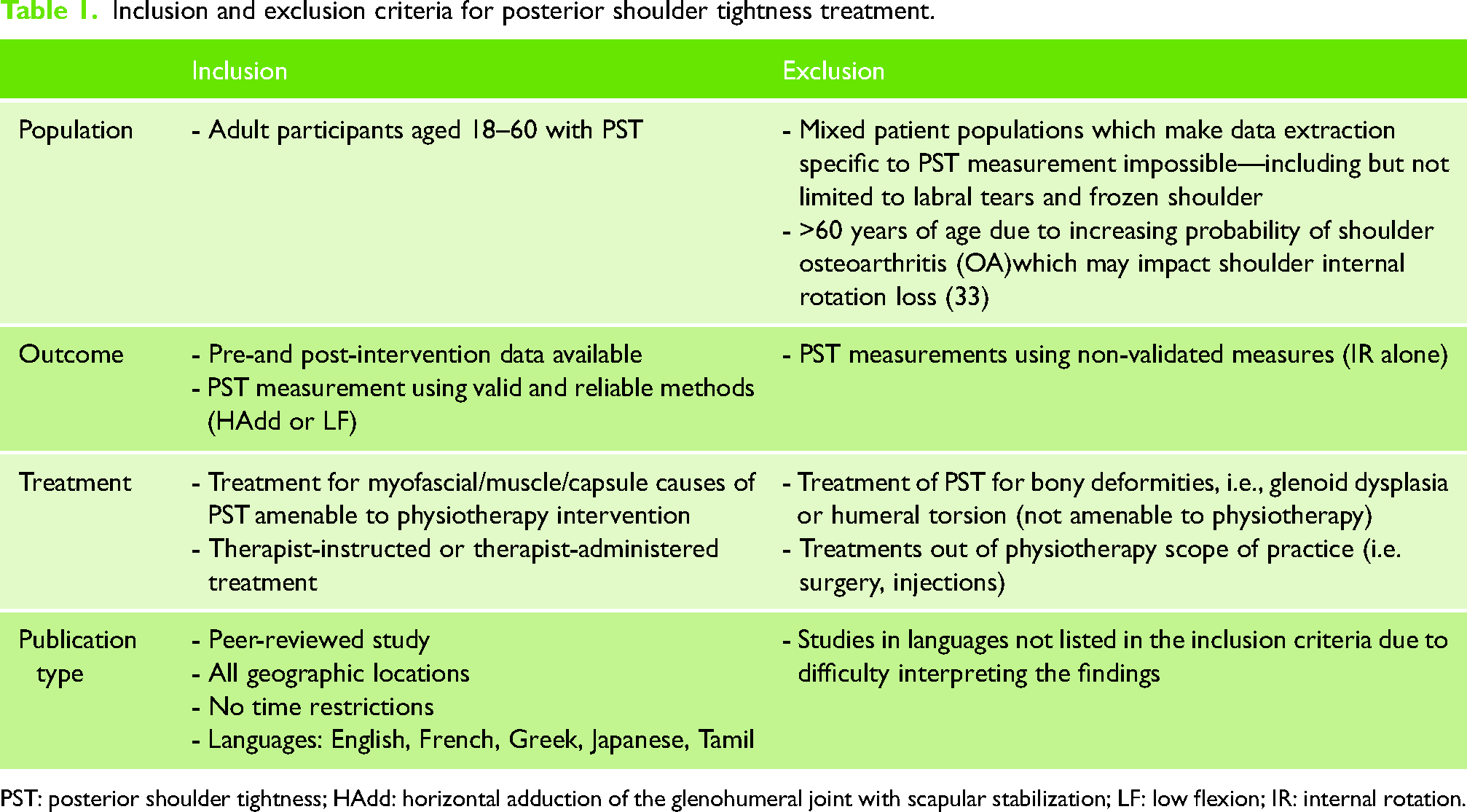
PST: posterior shoulder tightness; HAdd: horizontal adduction of the glenohumeral joint with scapular stabilization; LF: low flexion; IR: internal rotation.
Studies with valid and reliable assessments associated with PST were eligible for this review. This included HAdd of the GHJ including scapular stabilization (HAdd), IR or LF (Figure 1
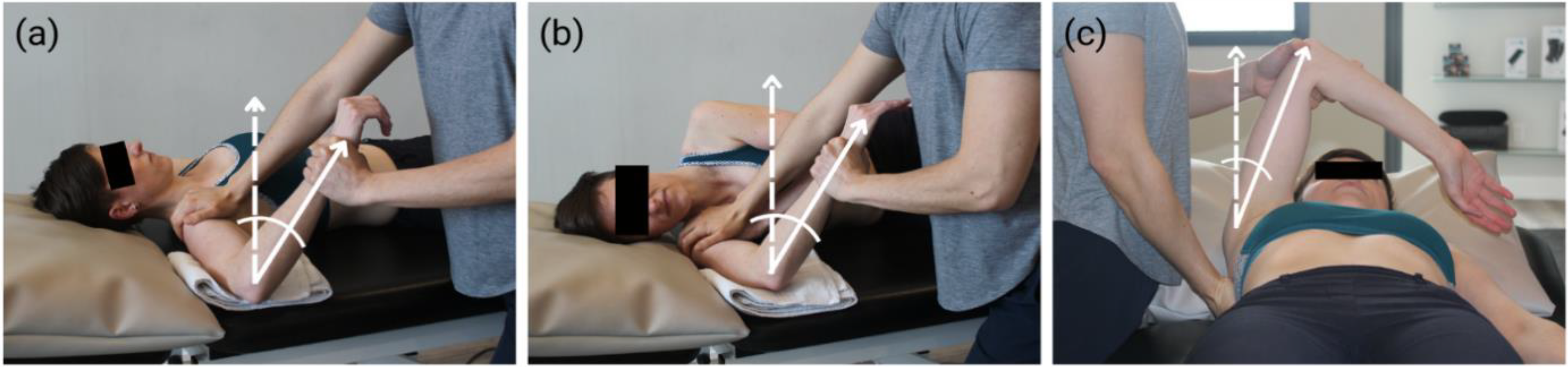
PST Assessment Methods. (a) Internal rotation at 90° abduction. (b) Low flexion. (c) Horizontal adduction.
Data charting
Data charted from each study included authors, title, study year, location, study design; participant number, age, sex; PST intervention and parameters; patient-reported outcomes; and results. Data charting was completed by two reviewers (MK, MA) to ensure consensus using a custom-designed form developed by the study team (Appendix B
Data synthesis
Study and intervention details were described and numerically summarized. Themes were organized into therapist-instructed and therapist-administered rehabilitation strategies, as well as combined treatment methods. Regular study meetings occurred to discuss data collection and the interpretation of emerging themes for the treatment of PST.
Results
Study selection
Our search identified 2777 articles, of which 672 were duplicates, 1870 did not pass the title and abstract screening and 1 article could not be retrieved. A further 214 articles were excluded from the full-text review because 42 had treatment that was not specific to PST, 30 had outcomes that were not specific to PST, 29 did not offer any treatment, 65 were not peer-reviewed, 19 did not meet the age criteria, 16 had no extractable data and 13 did not meet the language inclusion criteria. References of the included articles and other relevant book chapters were screened and resulted in five eligible articles. Four were excluded because two had outcomes not specific to PST and two had treatment not specific to PST. In total, 21 articles (13 randomized controlled trials [RCTs], 7 prospective cohort studies and 1 case report) were included in this scoping review (Figure 2). Measurement reliability of the HAdd and LF by the study raters was reported in 10 of 21 studies (Appendix B). Details of each included study are summarized in Table 2.
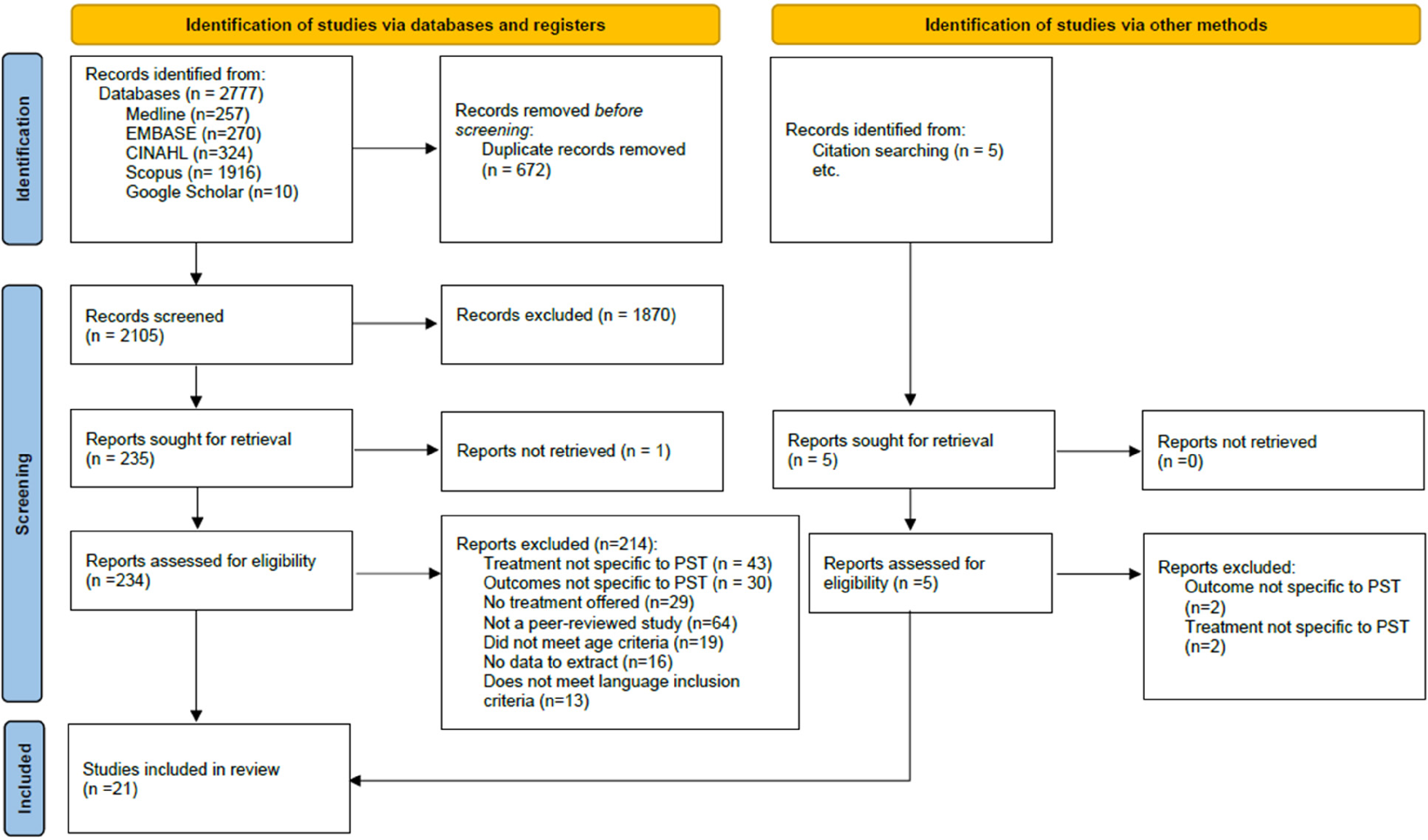
PRISMA flow diagram for study selection and exclusion.
Summary of included studies.
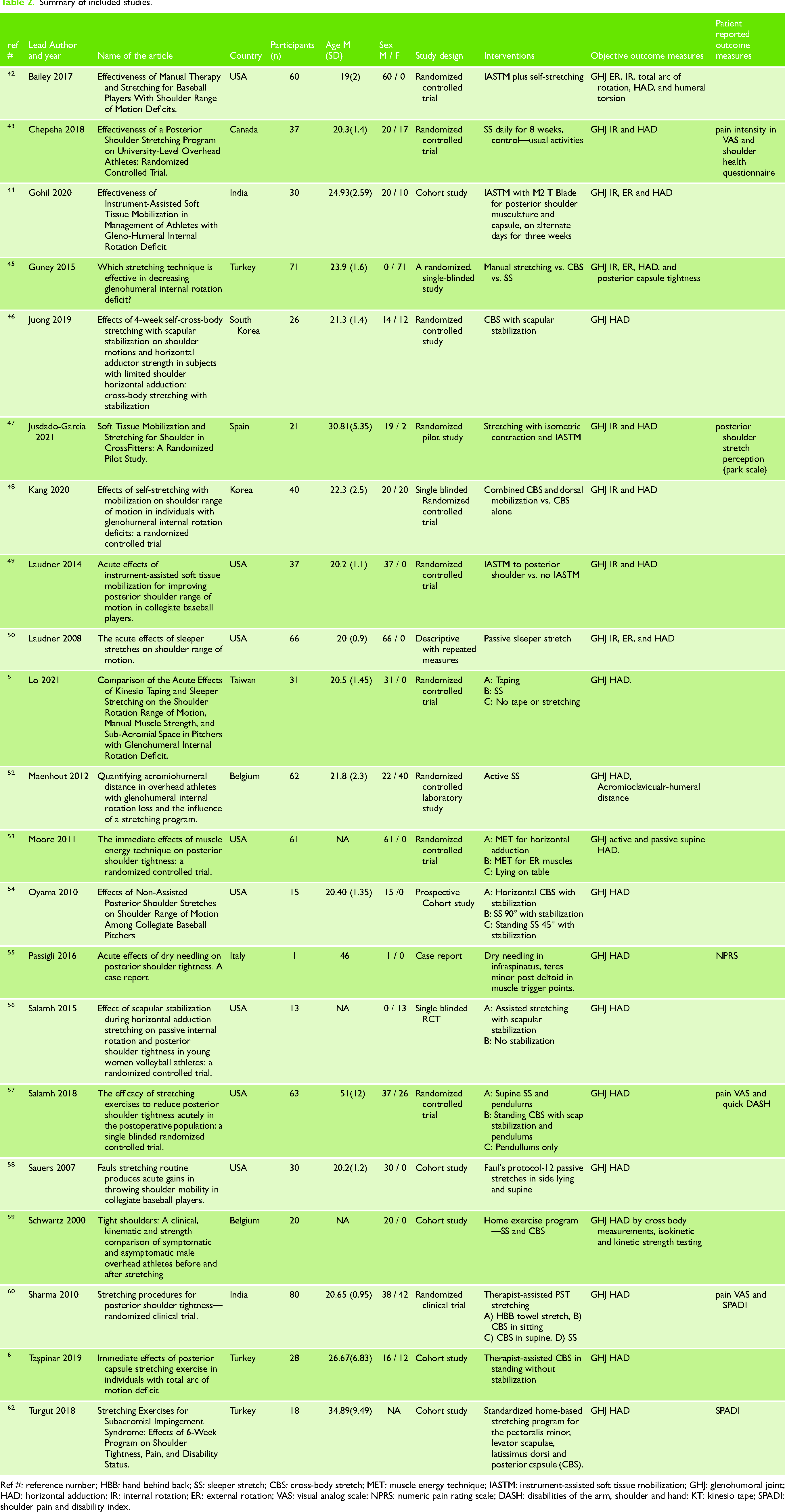
Ref #: reference number; HBB: hand behind back; SS: sleeper stretch; CBS: cross-body stretch; MET: muscle energy technique; IASTM: instrument-assisted soft tissue mobilization; GHJ: glenohumoral joint; HAD: horizontal adduction; IR: internal rotation; ER: external rotation; VAS: visual analog scale; NPRS: numeric pain rating scale; DASH: disabilities of the arm, shoulder and hand; KT: kinesio tape; SPADI: shoulder pain and disability index.
Overview of PST intervention strategies
Therapist-administered interventions
Out of the 21 included studies listed in Table 2, 10 (415 participants total) focused on therapist-administered interventions for PST. An overview of these results can be found in Figure 3. One study looked at the impact of dry needling on PST and two studies investigated instrument-assisted soft tissue mobilization (IASTM). A total of five studies looked at the impact of assisted stretching on PST. The stretches ranged from sleeper stretch (SS), cross-body stretch (CBS), stretches from Fauls protocol (12 therapist-administered stretches, see Appendix C for details) and stretches involving muscle energy technique (MET). The impact of scapular stabilization with stretching on PST was also reported.
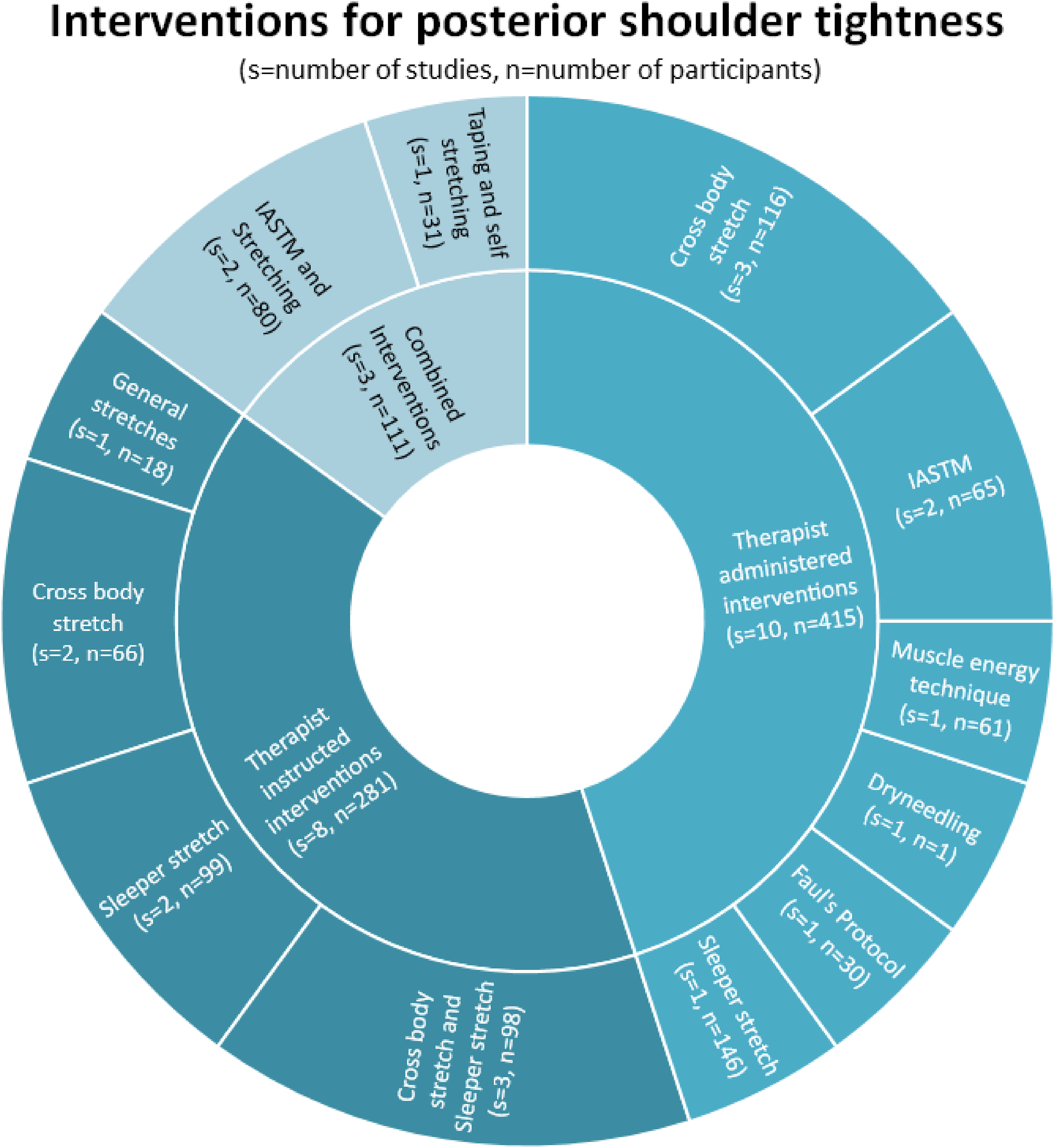
Total number of studies and participants for each intervention type.
Manual therapy
An increase in HAdd ROM was found immediately after therapist-assisted CBS 61 and greater improvement with scapular stabilization. 56 GIRD and PST improvement was significantly greater using therapist-assisted CBS compared to self-SS and self-CBS. 45 An immediate increase in HAdd was noted with MET to the horizontal adductors 53 and with sustained stretch for HAdd and IR at the end of a 3-week follow-up period. 50
Therapist-assisted SS produced the greatest improvement in HAdd (4.3 cm) compared to CBS in sitting (0.75 cm), CBS in supine (2 cm) and towel stretch (0.85 cm). 60 Improvement in HAdd was noted with Fauls protocol stretching. 58
Instrument-assisted soft tissue mobilization
A significant increase in HAdd and IR was found with IASTM to the posterior shoulder. 49 The ROM improvement was still significant at the end of 3 weeks. 44
Dry needling
A case study of a patient with PST showed an immediate clinically meaningful improvement in pain and shoulder ROM following dry needling of the infraspinatus, teres minor and posterior deltoid muscles. 55 This suggests that muscular impairment may be a significant source of pain and ROM limitation in PST.
Therapist-instructed interventions
Out of 21 studies, 8 studies (281 participants total) focused on therapist-instructed exercise programs for PST (Figure 4). All noted a significant short-term change in HAdd ROM compared to the control. Parameters for each of the stretches are listed in Table 3. All data regarding pre- and post-intervention results are listed in Appendix B.

PST Treatment Methods. (a) Self SS. (b) Self CBS-anterior view. (c) Self CBS-posterior view.
Summary of intervention parameters and results of included studies.
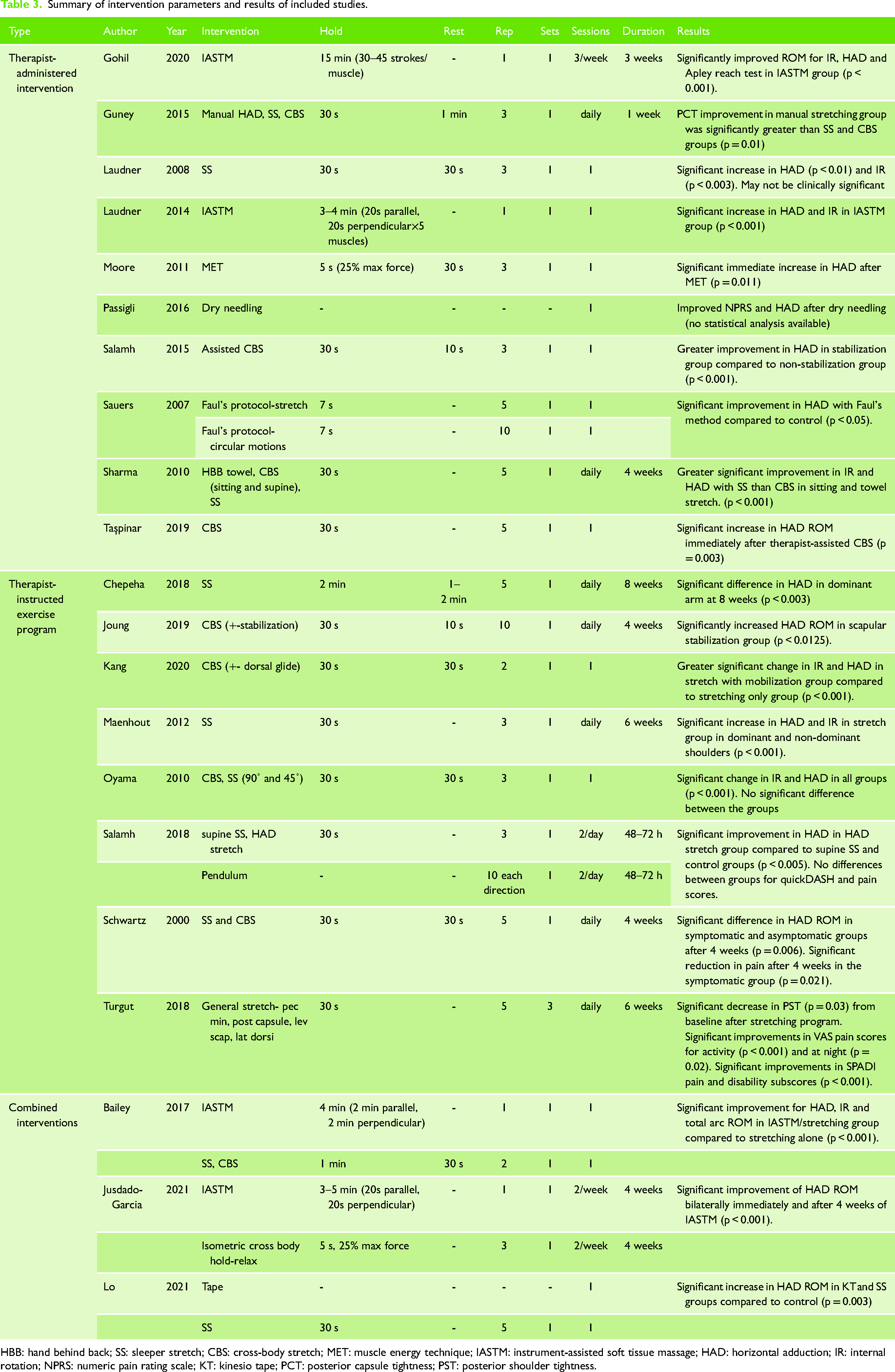
HBB: hand behind back; SS: sleeper stretch; CBS: cross-body stretch; MET: muscle energy technique; IASTM: instrument-assisted soft tissue massage; HAD: horizontal adduction; IR: internal rotation; NPRS: numeric pain rating scale; KT: kinesio tape; PCT: posterior capsule tightness; PST: posterior shoulder tightness.
Sleeper stretch
Two studies looked at the effect of SS on PST. Both studies instructed participants to complete SS in side-lying with scapular stabilization.43,52
Cross-body stretch
The CBS, also named HAdd or cross arm stretch, was performed in standing 48 and side-lying. 46 Of note, Joung et al. 46 reported a statistically greater increase in HAdd in the scapular stabilization group. Kang et al. 48 noted a greater improvement in HAdd with the addition of a self-dorsal glide mobilization to the CBS.
SS and CBS
Two studies compared the SS and CBS.54,57 Oyama et al. 54 found no statistical difference in HAdd ROM between the SS and CBS groups. However, Salamh et al. 57 reported a greater improvement in HAdd ROM in the CBS group compared to the supine SS group. Another study looked at the effects of the SS and CBS together and found significant improvements in HAdd ROM after the combined intervention. 59 These studies varied in their administration of the CBS between supine, 57 side-lying 59 and standing. 54 One study found no difference in quick-DASH and pain scores between groups, 57 while 1 reported a significant decrease in pain scores in the symptomatic group. 59
General stretches
One study looked at general stretches. These included pectoralis minor, levator scapulae, latissimus dorsi and posterior capsule (CBS) stretches without stabilization. 62 This study found a significant decrease in PST and pectoralis minor tightness post-intervention. This study also found that pain (Visual Analogue Scale [VAS]) and Shoulder Pain and Disability Index (SPADI) scores were improved at 6 weeks. 62
Combined interventions
A combination of therapist-instructed programs and therapist-administered interventions for PST were studied in 3 out of 21 studies (n = 112 participants). Two studies compared the effect of IASTM and self-stretches on PST. One study looked at the effect of taping versus SS on PST.
IASTM and stretching
Two studies showed significant improvements in HAdd, IR and total arc ROM with IASTM and stretching compared to stretching alone.42,47 These improvements were maintained after 4 weeks. 47
Tape and SS
Lo et al. 51 reported that the application of Kinesiology tape (K-tape) and SS both improved shoulder IR, HAdd and total rotation in pitchers with GIRD.
Discussion
This study used a scoping review to review the content of therapist-instructed and therapist-administered rehabilitation strategies in published physical therapy interventions for PST. A variety of shoulder disorders may present with PST and a thorough clinical history and physical examination is mandatory to determine the suitability of rehabilitation strategies for PST. Patients that do not respond to a rehabilitation program for PST should be referred for additional medical assessment and diagnostic imaging to investigate for pathologies such as excessive humeral torsion for suspected GIRD or glenoid dysplasia for posterior shoulder instability.
The therapist-instructed methods focus on a variety of stretching techniques. CBS and SS were the most researched (16/21 articles) and appear to be effective in improving PST. Therefore, both CBS and SS can be used to increase posterior shoulder extensibility. Kolber 63 reports that it is important to measure PST with the scapula in a stabilized fashion. Similarly, it is important to maintain shoulder retraction during any cross-body or SS to optimize the stretch targeted to the PST and maximize ROM benefits.
The therapist-administered methods maintained a focus on CBS and SS, both of which were applied passively to the patient. In-clinic stretching can complement therapist-instructed stretching as it allows the patient to experience the sensation, which can in turn be recreated independently. MET, IASTM and dry needling also improved PST, but the evidence is limited as there were only single studies of each found in this scoping review.
Combining stretching with IASTM or taping may also be effective in reducing PST. Due to the heterogeneity of intervention type and parameters, it is difficult to compare the effectiveness of the given interventions. Thus, future studies should utilize standardized methodologies to investigate the effects of treatment interventions with clinically applicable parameters.
Knowledge gaps and future research
This scoping review provides for a detailed exploration of non-operative rehabilitation options for PST that is not expanded upon in a recent PST treatment systematic reviews. 33 In addition to therapist-administered interventions, the research supports the use of therapist-instructed home exercises to improve posterior shoulder muscle and capsule extensibility. Although half of the included articles were published more than 5 years ago, we noticed an interesting trend. The more recent studies (within 5 years) focused on therapist-instructed exercises whereas the older studies (greater than 5 years) focused on passive treatment techniques.
Despite the support for PST rehabilitation, there was inconsistency in the dosing prescribed for the exercises, as well as manual therapy techniques. There is no consensus on stretching parameters for PST and the majority of research on stretching parameters has been done on the lower extremity, but it would seem to be reasonable to apply the proposed dosing to muscles in the upper extremity. 64 Therefore, based on the majority of the dosing parameters within this review (Table 3) and considering general exercise principles, we suggest 30 s hold for a total of 2 min daily, for a minimum of 4 weeks. 64 Ideally leading to a shift in alternative methods of increasing muscle extensibility in the future.
Further, there is no consensus on the optimal assessment strategy of PST. Within this review, only 10 of 21 studies included rater reliability for HAdd and none mentioned LF. Salamh et al. 11 recommend HAdd as it is the most researched method. However, when examining the validity of PST assessment, IR of the GHJ is often used as the reference criterion of PST. A recent study by Hall et al. 39 suggests the use of greater than 10° difference side-to-side in more than 2 out of 3 clinical tests (GHJ-IR, HAdd and LF) or a difference of 20° or more in a single test. 39 Perhaps a PST assessment cluster that combines Hall's 3 clinical tests with a subjective history of overhead sport or occupation would detect and assess PST with greater validity and reliability.
Future research should continue to establish a valid, reliable and responsive measure of PST that will allow for the identification of PST through side-to-side differences in shoulder ROM and detect clinically important improvements in PST pre- and post-intervention.
Strengths and limitations
This study followed methodological standards for conducting and reporting scoping reviews. Due to this methodology, evidence for the effectiveness of the retrieved interventions or a critical appraisal of the literature was not completed. The heterogeneity of study designs and study quality rating should be considered when interpreting the results. Despite these weaknesses, the scoping review design facilitated the retrieval of a wide breadth of studies to inform evidence-based treatment methods for PST and to identify knowledge gaps within PST literature.
It is possible that not all relevant studies were identified despite a systematic search strategy because the terminology for PST is not standardized. Due to inconsistent definitions of PST and insufficient assessment and reporting methods within a study lead to its exclusion, even if the study may have contributed additional information to the review. As noted in the discussion, this is a barrier to high-quality research in the field of PST.
There were population trends within the studies that may decrease the generalizability of the review results. There were more males (n = 511) than females (n = 265) and the mean age of patients was 25.8 years old. This decreases the external validity of this review's findings and applicability to middle-aged and older adults, especially females. Most notably, the majority of PST research has been conducted on overhead athletes.1–7,10 Investigating the effects of PST on non-athletic populations, especially those that work overhead8,9 would improve the applicability of the identified treatment methods to the general population.
Clinical implications and applications
We recommend stretching as one part of the core treatment method for PST. The stretch can be therapist-administered or taught as a home exercise. The CBS and SS, with scapular stabilization, both result in HAdd ROM improvements. IASTM, MET, general stretching, taping and dry needling can also be utilized. There were no adverse effects reported but due to the lack of study numbers and quality, it is key for the clinician to provide an individualized treatment plan based on the client's presentation. See Appendix D for clinical applications using small vignettes.
Conclusion
Stretching is part of the core treatment approach for PST in this scoping review. A combination of study heterogeneity, parameter inconsistency and inconclusive optimal assessment strategy must be further researched and improved to support the implementation of effective PST treatment in research or practice.
Supplemental Material
sj-docx-1-sel-10.1177_17585732231193166 - Supplemental material for An evidence-informed rehabilitation management framework for posterior shoulder tightness: A scoping review
Supplemental material, sj-docx-1-sel-10.1177_17585732231193166 for An evidence-informed rehabilitation management framework for posterior shoulder tightness: A scoping review by Yukino Fukushima, Murali Avilineni, Michelle Kao, Haider Tirmizey, Kenneth J. Faber, Rochelle Furtado and Jackie Sadi in Shoulder & Elbow
Supplemental Material
sj-xlsx-2-sel-10.1177_17585732231193166 - Supplemental material for An evidence-informed rehabilitation management framework for posterior shoulder tightness: A scoping review
Supplemental material, sj-xlsx-2-sel-10.1177_17585732231193166 for An evidence-informed rehabilitation management framework for posterior shoulder tightness: A scoping review by Yukino Fukushima, Murali Avilineni, Michelle Kao, Haider Tirmizey, Kenneth J. Faber, Rochelle Furtado and Jackie Sadi in Shoulder & Elbow
Supplemental Material
sj-docx-3-sel-10.1177_17585732231193166 - Supplemental material for An evidence-informed rehabilitation management framework for posterior shoulder tightness: A scoping review
Supplemental material, sj-docx-3-sel-10.1177_17585732231193166 for An evidence-informed rehabilitation management framework for posterior shoulder tightness: A scoping review by Yukino Fukushima, Murali Avilineni, Michelle Kao, Haider Tirmizey, Kenneth J. Faber, Rochelle Furtado and Jackie Sadi in Shoulder & Elbow
Footnotes
Acknowledgments
Meagan Stanley, Teaching and Learning Librarian for the Faculty of Health Sciences Librarian, Western University.
Contributorship
Yukino Fukushima is involved in abstract screening, study selection, data extraction, results analysis, editing manuscript, and primary author. Murali Avilineni is involved in abstract screening, study selection, data extraction, results analysis, table, and figure creation. Michelle Kao is involved in abstract screening, study selection, data extraction, results analysis, table, and figure creation. Haider Tirmizey is involved in abstract screening, study selection, data extraction, results analysis, and references. Kenneth J Faber is involved in research and project development, results analysis, and editing manuscript. Rochelle Furtado is involved in methods development/review, editing manuscript, and corresponding author. Jackie Sadi is involved in research and project development, result analysis, and editing manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
JS
Supplemental Material
Supplemental material for this article is available online.
This study Protocol was registered with: Open Science Framework https://osf.io/c7dxr. All data relevant to the study are included in the article or are available as supplementary files. No patient-identifiable data are available.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.