
Abstract
Purpose
Arthroscopic Bankart repair (ABR) may be more effective than nonoperative management for patients with anterior shoulder instability following first-time dislocation. The purpose of the study was to determine the most cost-effective treatment strategy by evaluating the incremental cost-effectiveness ratio (ICER) for ABR versus nonoperative treatment.
Methods
This cost-effectiveness study utilized a Markov decision chain and Monte Carlo simulation. Probabilities, health utility values, and outcome data regarding ABR and nonoperative management of first-time shoulder instability derived from level I/II evidence. Costs were tabulated from Centers for Medicaid & Medicare Services. Probabilistic sensitivity analysis was performed using >100,000 repetitions of the Monte Carlo simulation. A willingness-to-pay (WTP) threshold was set at $50,000.
Results
The expected cost for operative management higher than nonoperative management ($32,765 vs $29,343). However, ABR (5.48 quality-adjusted life years (QALYs)) was the more effective treatment strategy compared to nonoperative management (4.61 QALYs). The ICER for ABR was $3943. Probabilistic sensitivity analysis showed that ABR was the most cost-effective strategy in 100% of simulations.
Discussion
ABR is more cost-effective than nonoperative management for first-time anterior shoulder dislocation. The threshold analysis demonstrated that when accounting for WTP, ABR was found to be the more cost-effective strategy.
Introduction
Anterior glenohumeral instability is a common clinical problem, encompassing over 11% of all traumatic shoulder injuries; younger males, particularly those under 30 years old, have been found to experience rates of instability following primary dislocation as high as 3% per year.1–4 Each subsequent dislocation episode has the potential to increase the degree of glenoid bone loss, which may subsequently lead to long-term recurrent instability.5,6 Arthroscopic Bankart repair (ABR) is the most commonly performed procedure worldwide for anterior shoulder instability, and ABR has demonstrated significant improvement in patient-reported outcomes and low complication rates.7,8 Additionally, ABR allows for a high rate of return to sport, with prior systematic reviews finding 88% to 97.5% of patients returned to sport postoperatively.9–12
Traditionally, patients with a first-time dislocation have been managed nonoperatively, however, risk of recurrent episodes have been reported to be as high as 96%.3,13–15 Considering the high rates of recurrence after first-time instability, a debate exists of whether ABR should be routinely performed in patients following a first-time anterior shoulder dislocation.3,16 A recent meta-analysis by Hurley et al. 10 found that ABR results in a 7-fold decrease in the rate of recurrence following initial episodes of anterior shoulder dislocation compared to nonoperative management. However, it is unclear whether ABR or nonoperative management is the more cost-effective treatment.3,17,18
While prior studies have evaluated the cost-effectiveness and potential for cost minimization with ABR, lower-level evidence was utilized.19,20 As additional level I and II evidence has become available,3,21–24 no study has compared the cost-effectiveness of ABR to nonoperative management based exclusively on this currently available prospective data. Therefore, an updated cost-effectiveness study is warranted. The purpose of this study was to examine the cost-effectiveness of ABR versus nonoperative management in first-time anterior shoulder dislocation. Our hypothesis was that surgical management would be more cost-effective for patients with anterior shoulder instability following first-time shoulder dislocation.
Methods
A decision analytic model from the healthcare system perspective25–28 was used to determine the cost-effectiveness of the two most common treatment strategies for first-time shoulder dislocation patients: ABR and nonoperative management. The primary effectiveness outcome was measured in quality-adjusted life-years (QALYs). One QALY is assumed to be equal to 1 year in “perfect health.” 29 This quality of life was quantitatively measured by utility, where 1 represents the utility of the state lived in “perfect health” and 0 represents the minimum utility (i.e. “dead”). Costs of treatment were expressed in 2021 American dollars. The model was created using decision analysis software (TreeAge Pro 2020, Williamstown, MA, USA).
Base case and model assumptions
For the base case scenario, patients were assumed to be experiencing their first episode of shoulder instability and to have failed nonoperative management strategies. Costs associated with primary evaluation of anterior shoulder instability were assumed to have taken place prior to the point at which a decision regarding operative versus nonoperative management would be made. Therefore, these costs, including costs associated with ED evaluation and imaging, are considered irrelevant from the perspective of this base case, and were excluded from the model. Given the low rates of complication following ABR and existing cost-effectiveness analyses suggesting a negligible impact of these complications on model costs, utilities, and overall dominant treatment in the context of arthroscopic procedures, the decision was made to exclude postoperative complications from the model, with the exception being recurrent instability.19,30,31
Model description
Patients had equal access to either of the model treatment strategies. After a treatment was selected, two health states were possible. Patients would either experience relief of shoulder pain, labeled as “healthy,” or they would experience recurrence of shoulder pain due to recurrent instability, labeled “recurrent instability.” In the case of successful treatment (“healthy” status), patients would either maintain stability, labeled “stay stable,” progressing to the “healthy” status, or they would have an episode of recurrent instability, labeled “recurrence,” and progress to the “recurrent instability” status. Patients reaching the terminal “healthy” status would then return to the “healthy” state for subsequent Markov cycles. If a patient progressed to the terminal “recurrent instability” status, they would move to the “recurrent instability” health state. Patients who reached the “recurrent instability” health state were assumed to have two options: conservative management, labeled “nonoperative management,” or ABR, labeled “surgical management.” Regardless of this subsequent management, patients were assumed to progress to the terminal “healthy” node returning them to the “healthy” state for subsequent Markov cycles where they would again be able to pass through “stay stable” or “recurrence.” This decision tree model is visually represented in Figure 1.
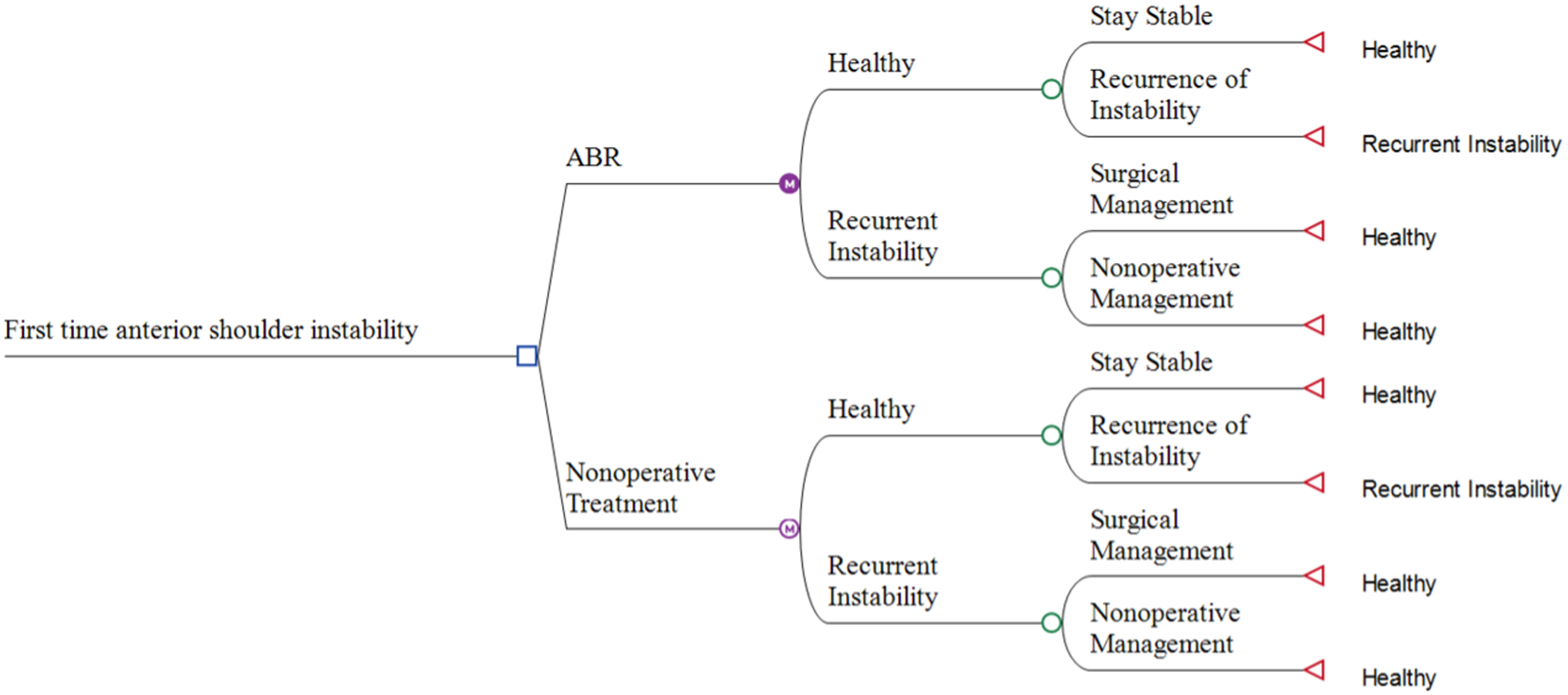
Decision tree for the management of first time anterior shoulder instability with ABR versus nonoperative treatment. ABR: arthroscopic Bankart repair.
Patients who experience recurrent instability following initial treatment are more likely to experience subsequent episodes of instability. Therefore, tracking of the number of times patients experienced recurrent instability was included in the model. This tracking was applied to the probability of progression to recurrent instability, increasing the probability of recurrence with increasing occurrences. Additionally, the utility gained from treatment is assumed to decrease for each episode of instability after treatment. Tracking of the number of times patients underwent ABR was implemented in the model. The utility gained from surgery or nonoperative treatment was reduced by 0.1 for each subsequent treatment.
The weighted average follow-up times of level I and II evidence were utilized to set a Markov cycle of 2 years and a model time horizon of 6 years. Patients were assumed to have a maximum of two surgeries and three rounds of nonoperative treatment. Furthermore, the literature reflects that if a patient does not experience recurrent instability within the first 2 years following treatment, the probability of recurrence decreases.18,32,33 Therefore, each Markov cycle represented 2 years and a decay formula was utilized to reflect the probability of recurrence for subsequent cycles through the model if they did not experience recurrent instability early on following initial treatment.
Probabilities
Probabilities and health utility values were determined through comprehensive literature review. Outcome data regarding ABR and nonoperative management of first-time shoulder instability was utilized from only level I and II evidence in the literature.3,17,18,34–41 A PubMed literature search was conducted using search terms including “nonoperative shoulder instability,” “conservative treatment shoulder instability,” “first-time shoulder dislocation,” “Bankart outcomes,” and “recurrent shoulder instability.” Relevant papers were screened by three authors, all sports-fellowship trained orthopedic surgeons to identify recurrence rate and outcome data. Probabilities of recurrence and subsequent surgery following initial treatment were calculated using the weighted averages from this level I and II evidence studies.
To accurately represent the uncertainty within the model, the highest and lowest probabilities from the selected studies were applied to the probability distribution in sensitivity analysis. The means of probability distributions were overridden by the weighted mean calculated. Therefore, in analyses of the model that do not involve sampling (i.e. cost-effectiveness analysis), the weighted mean probability was utilized. The probabilities, distributions, and references can be viewed in detail in Table 1.
Probability, utility, and cost input values.
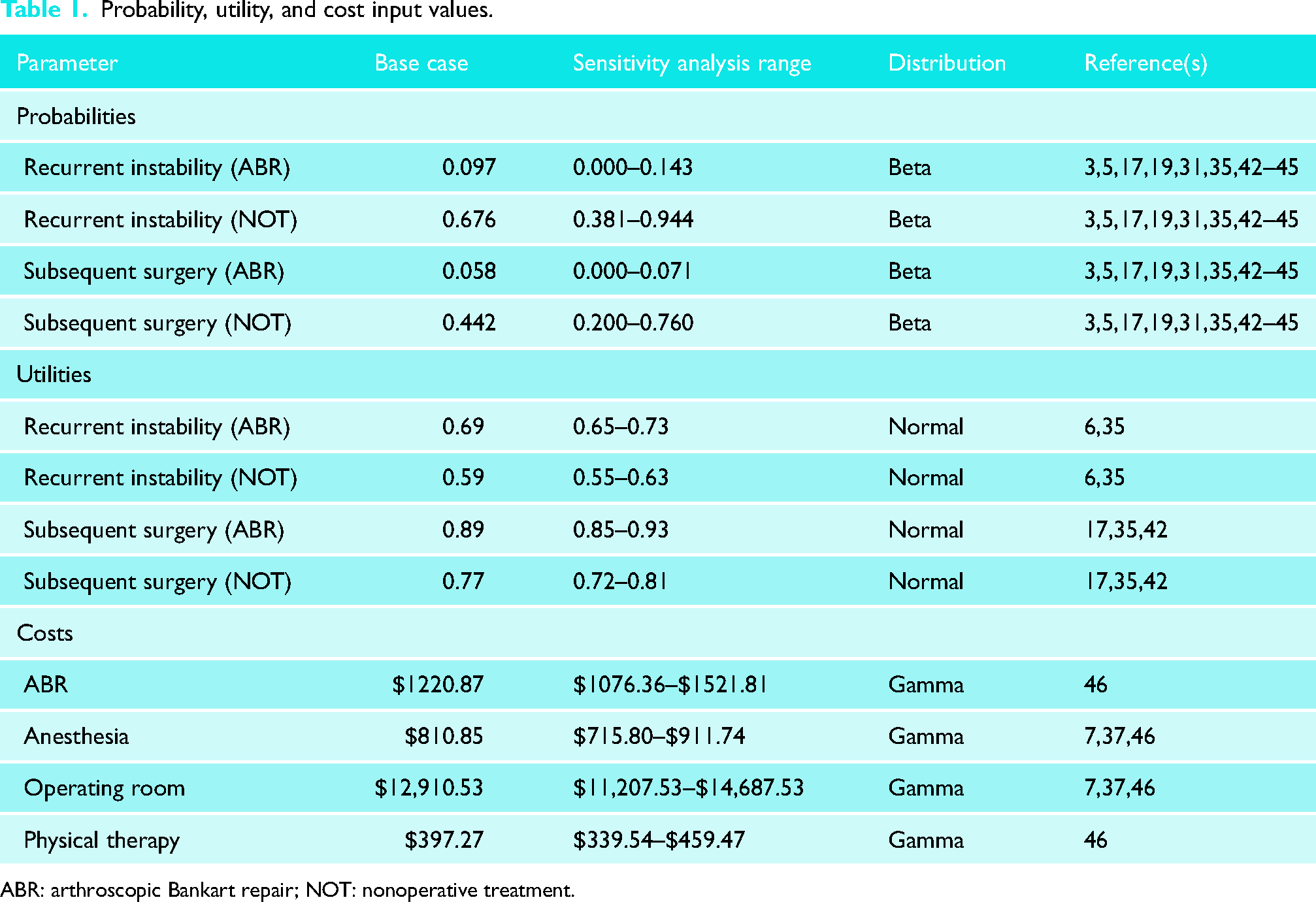
ABR: arthroscopic Bankart repair; NOT: nonoperative treatment.
Utilities
Utilities were calculated using the weighted averages from level I and II evidence that recorded Western Ontario Shoulder Instability Index scores.3,18,35,41,47,48 These utility values were compared to those used in previous cost-effectiveness analyses of nonoperative and arthroscopic treatment of shoulder instability to confirm their validity.19,49
Uncertainty within the model was represented using the highest and lowest utility values from the selected level I and II evidence. These values were applied to distributions of utility during sensitivity analysis, however, means of utility distributions were overridden by the calculated weighted average in analyses of the model that did not involve sampling (i.e. cost-effectiveness analysis). The utilities, distributions, and references can be viewed in greater detail in Table 1.
Costs
The total costs for each treatment pathway were tabulated using cost data from the Centers for Medicaid and Medicare Services (CMS), 50 comprehensive literature review,42,51,52 and publicly available records of healthcare costs. To accurately represent uncertainty within the model, the highest and lowest costs from CMS and publicly available health records were applied to distributions of cost during sensitivity analysis. The means of cost distributions were overridden by the average calculated from CMS and publicly available records. Thus, the calculated average cost was used in analyses which did not require sampling (i.e. cost-effectiveness analysis). A detailed list of costs, distributions, and references may be found in Table 1.
Statistical analysis
The primary outcomes of interest within this model are effectiveness (QALYs), costs, and incremental cost-effectiveness ratios (ICERs). An ICER represents the dollar cost per additional unit of effectiveness (QALY) between treatments. In other words, an ICER represents the amount of money required to gain a unit of effectiveness when comparing two treatments. The willingness-to-pay threshold (WTP) was set as $50,000/QALY. This WTP value represents the amount of money the average person is willing to spend to gain an additional unit of effectiveness (i.e. 1 QALY). Acceptable WTP thresholds range from $50,000 to $100,000 in the existing cost-effectiveness literature.43,53,54 All inputs were tested with one-way sensitivity analysis over a broad range of values identified using beta, normal, and gamma distributions for probability, utility, and cost, respectively (Table 2). One-way sensitivity analysis was performed one variable at a time while keeping all other variables fixed. Variables were further evaluated with threshold analyses if the model's results were sensitive in one-way sensitivity analysis. As is recommended for a Markov model, probabilistic sensitivity analysis was performed using the Monte Carlo simulation method for over 100,000 simulations. A cost-effectiveness acceptability curve was obtained from the probabilistic sensitivity analysis up to a willingness-to-pay of $100,000.
Incremental cost-effectiveness summary.

ABR: arthroscopic Bankart repair; ICER: incremental cost-effectiveness ratio; QALY: quality-adjusted life year.
Results
Cost-effectiveness analysis
Three Markov cycles, each representing 2 years, were performed for a time horizon of 6 years. Nonoperative treatment ($29,343) was found to be less expensive than ABR ($32,765). However, ABR (5.48 QALYs) was found to be the more effective treatment strategy compared to nonoperative management (4.61 QALYs). In cost-effectiveness analyses, treatments that are “dominated” are treatments that are less effective and more costly. In this model, neither treatment was dominated. This is illustrated in Figure 2 where any treatments found to the left of the undominated line represent treatments that are both more expensive and less beneficial.

Cost-effectiveness analysis demonstrating willingness-to-pay threshold.
The difference in cost between nonoperative treatment and ABR (incremental cost) and difference in effectiveness between nonoperative treatment and ABR (incremental effect) are used to find the ICER. 55 When compared to nonoperative management, ABR's incremental cost was $3422 and the incremental effectiveness was 0.87 QALYs. The ICER for ABR was $3943, below the willingness-to-pay threshold of $50,000, and thus was considered cost-effective. These results are summarized in Table 2.
Sensitivity analyses
One-way sensitivity analysis demonstrated that the results of our cost-effectiveness model were sensitive to the utility of nonoperative treatment, probability of recurrent instability following arthroscopy, and probability of subsequent ABR following failed nonoperative treatment. No combination of these variables changed the results of the model in one-way or two-way sensitivity analysis. However, in three-way sensitivity analysis, nonoperative treatment became the preferred strategy only when the health benefit of nonoperative treatment was equal to 1 QALY, the probability of recurrent instability following nonoperative treatment was ≤ 0.38, and the probability of subsequent ABR after failed nonoperative treatment was ≥ 0.76. The model's results were consistent regardless of fluctuation in values for any other variables. Probabilistic sensitivity analysis showed ABR was the most cost-effective strategy in 100% of simulations. The cost-effectiveness acceptability curve depicted that ABR was considered the most cost-effective management strategy for all WTP thresholds > $3859.96 through $100,000 spent per QALY gained (Figure 3).
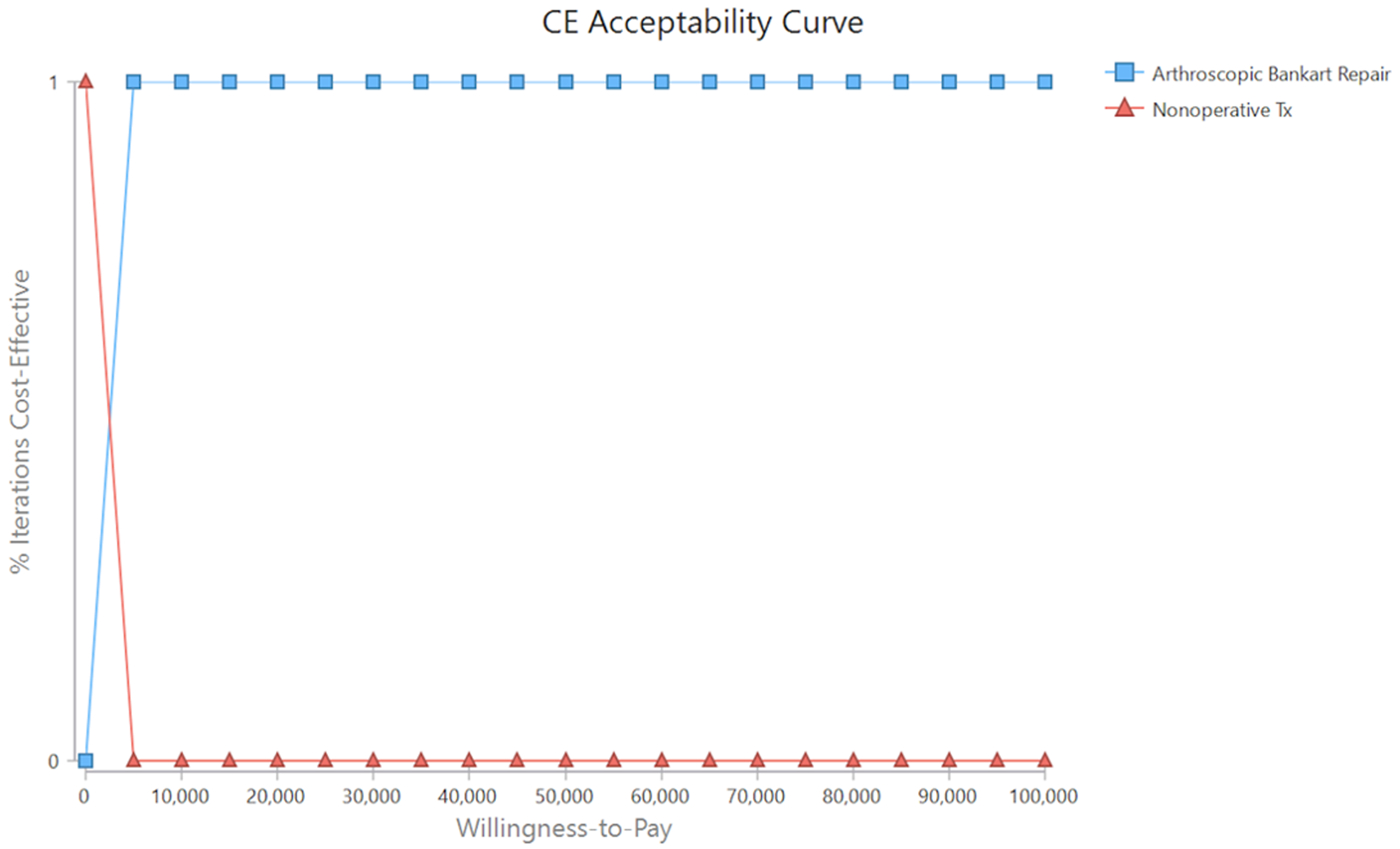
Cost-effectiveness acceptability curve between ABR versus nonoperative treatment. ABR: arthroscopic Bankart repair.
Discussion
Our model results showed that ABR is a cost-effective option for the treatment of first-time anterior shoulder dislocation patients, and a more cost-effective treatment option than nonoperative management across a wide range of willingness-to-pay thresholds. Although ABR has higher upfront costs than nonoperative management, the potential health utility gained over time may make this an economically advisable management strategy for patients with anterior shoulder instability following first-time shoulder dislocation.
As the burden of healthcare spending continues to grow, quantifying the economic ramifications of this expenditure is of the utmost importance. In 2021, the Organization for Cooperation and Development (OECD) estimated total healthcare spending in the United States accounted for 17.8% of gross domestic product (GDP), which translates to just over $12,318 per capita. 56 The bloated healthcare costs observed in the United States are due to a multitude of complex and interrelated issues. One of the contributors is the tendency for the medical community to favor more expensive interventions, assuming superior health benefit and effectiveness44,57,58; a main criticism of this justification is the lack of supporting evidence. 58 Additionally, the OECD estimates that the United Kingdom 2021 healthcare costs account for 11.9% of the GDP, slightly above the European average of 9.9%, which has been rising annually. 56 The United States has increased healthcare costs with treatments costing at least 40% more than any other country in the world. 56
Cost-effectiveness analyses weigh both monetary costs and potential health benefits to provide evidence-based insight into the appropriateness of healthcare spending. ABR is a more expensive and aggressive treatment in comparison to nonoperative treatment for first-time shoulder instability. Conventionally, nonoperative treatment is pursued initially, proceeding to surgical intervention only after failure of nonoperative management. However, the current literature suggests that in the context of first-time anterior shoulder instability, this strategy may not be optimal.
ABR is the most commonly performed procedure worldwide for anterior shoulder instability, especially in the setting of subcritical bone loss. 59 In a recent meta-analysis by Hurley et al. 10 level I and II evidence was used exclusively to compare outcomes of treatment for first-time shoulder dislocation with ABR versus nonoperative management. It was found that the rate of recurrent instability was seven times higher in those who underwent nonoperative management compared to initial surgical treatment for first-time dislocation. Thus, they advocated for ABR in first-time dislocators due to reduced rate of recurrence. To support this paradigm shift, it is imperative to consider cost-effectiveness, which was the purpose of this study.
Previous high-quality cost-effectiveness analyses have been performed; however, these have traditionally relied heavily upon level III evidence and expert opinion. Crall et al. 19 performed a cost-effectiveness analysis of ABR compared to nonoperative treatment for the management of first-time anterior shoulder dislocation finding ABR to be most cost-effective in most clinical scenarios. One of the main limitations of their study was the reliance on lower-quality evidence. Furthermore, since publication of their analysis in 2012, the existing literature has grown considerably permitting the current analysis to incorporate several high-quality studies not previously available.35–37
In the model utilized by Crall et al., 19 probabilities for recurrent instability following ABR and nonoperative treatment were 0.109 and 0.56, respectively. These rates are relatively similar to those found in the present analysis. However, the rate of surgery following failed treatment in the model utilized by Crall et al. 19 was 0.5 for both management options, and this rate was based on expert opinion. In their analysis, it was found that changing these probabilities of surgery after initial treatment did change the preferred management strategy. In comparison to the probabilities guided by expert opinion, the present analysis utilized level I and II evidence to calculate weighted means of 0.058 and 0.442 for the rate of surgical intervention following initial ABR and nonoperative treatment, respectively. The ability to include these data-driven probabilities enhances the strength of our model.
As well as being more cost-effective to perform a primary ABR, it should also be noted that ABR following recurrent instability has a higher recurrence rate than following a first-time dislocation, due to increased soft-tissue damage and glenohumeral bone loss.45,46,60 This was accounted for by our model, which suggests that patients may benefit from surgical intervention. Furthermore, recurrent instability can result in increased cartilage injuries, which can predispose patients to increased risk of long-term arthropathy. 46 However, not all patients wish to undergo surgery after a primary instability event and it is important to appropriately counsel these patients based on their risk factors, such as participation in high-risk sports.
There are several limitations to the present study. Our model assumed that a patient would gain a given healthy utility value that is consistent over the model time horizon of 6 years. This is not necessarily the case in real life. For instance, the normal course following surgery consists of a steady increase in function and decrease in pain as recovery and healing progresses. Therefore, the actual QALYs gained over the course of 2 years may be lower than what our model reflects. Another assumption in our model was negligible influence of postoperative complications such as infection or stiffness due to the exceedingly low rates and minimal added cost. Crall et al. 19 noted a minimal influence of postoperative complications therefore we felt exclusion was acceptable. Formulas were used to account for a variety of progressive growth and decay in the model that were based on convention and may not truly reflect real-world observations. However, the use of these formulas is common in the existing cost-effectiveness literature. Additionally, restrictions were set on the number of times patients would undergo treatment as well as the options for treatment. There are several arthroscopic and open procedures utilized to treat shoulder instability and surgeons may recommend a different procedure. Finally, a limitation of this study is that it was performed based on US healthcare costs. Although given that a healthcare system with higher costs, this likely means that the relative cost-effectiveness of ABR may be higher in other healthcare systems.
In conclusion, ABR is more cost-effective than nonoperative management for first-time anterior shoulder dislocation, yielding a superior payoff in terms of dollars spent for health gained. Although ABR is more expensive upfront than nonoperative management, the potential health utility gained through initial surgical management may make this the economically advisable management strategy, though treatment decision-making remains complex.
Footnotes
Contributorship
ZIL led the preparation of the manuscript. ETH, SG, and DHM performed data collection and editing of the manuscript. AMB and SG performed the statistical analysis. SG conceived the study idea. MS assisted with revisions. KAC, EJS, and LMJ co-designed the study, supervised the systematic literature review, and edited the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KAC receives research support from Stryker and consulting fees from Mitek. EJS receives consulting fees from Arthrex, Cartiheal, Better PT, Flexion Therapeutics, Joint Restoration Foundation, Organogenesis, Smith & Nephew, Subchondral Solutions, Vericel. LMJ receives research support from Arthrex, Mitek, Smith & Nephew and receives publishing royalties from Wolters Kluwer Health.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
SG.