
Abstract
Background
Performance-based tests for patients with anterior shoulder dislocation are lacking. This study determined the reliability and validity of the supine moving apprehension test designed to assess the ability to control anterior instability loads.
Methods
Thirty-six participants were recruited (18 healthy individuals, and 18 patients following anterior shoulder dislocation). Healthy participants performed the supine moving apprehension test on 2 separate occasions to determine test-retest reliability. Patients completed the supine moving apprehension test and the Western Ontario Shoulder Instability index before and 6 months after surgical stabilization of their shoulder. The presence of anterior apprehension was also documented post-operatively.
Results
The supine moving apprehension test demonstrated good test-retest reliability (intraclass correlation coefficient = 0.74−0.84). Patients performed 18−30 repetitions less than healthy individuals during the supine moving apprehension test (P < 0.01). A strong correlation was found between supine moving apprehension test scores and Western Ontario Shoulder Instability post-operatively (r = −0.74, P ≤ 0.01). Supine moving apprehension test scores significantly improved among patients following surgery (P < 0.01). Patients with a negative apprehension test post-operatively performed the supine moving apprehension test significantly better than patients with a positive apprehension test (P < 0.01).
Conclusions
The supine moving apprehension test is reliable and valid among patients with anterior shoulder dislocation and may serve to assess patients’ ability to control shoulder anterior instability loads.
Introduction
Conservative as well as post-operative rehabilitation for anterior shoulder instability begins with efforts to regain range of motion (ROM) followed by strengthening and exercises to restore neuromuscular control. 1–4 Over the course of rehabilitation, clinicians employ different self-reported and physical impairment measures to gauge patient progress. Serial ROM measurements serve as good indicators of progress early during the rehabilitation process, while scapular control, muscular strength, and endurance are suitable during more advanced stages, as well as for determining readiness to return to unrestricted activity.3,5,6 Despite their undisputed importance, measures of ROM and strength may not provide adequate information regarding shoulder stability, neuromuscular control or residual disability following surgical stabilization of anterior shoulder instability.7,8 The anterior apprehension test is another measure often used to ascertain re-stabilization and determine readiness to return to unrestricted activity following surgical stabilization of the shoulder. 6 However, the apprehension test is designed to elicit the sensation of instability and thus may not provide sufficient information regarding the ability to control and protect the shoulder from potentially injurious loads.
Shoulder dislocation often occurs during high-intensity athletic activities.9,10 The majority of dislocations are anterior and typically occur when sudden forces at the extreme ends of glenohumeral abduction-external rotation are adequate to displace the humeral head anteriorly. 11 The anterior shoulder musculature, namely the pectoralis major, anterior deltoid, biceps brachii, coracobrachialis, and subscapularis are considered dynamic anterior stabilizers of the shoulder and therefore most suited to protect it from anterior dislocation. 12 Accordingly, several studies demonstrated diminished and or delayed activation of the pectoralis major, 13 biceps brachii, 13 and subscapularis 14 among patients with anterior shoulder instability, and rehabilitation programs often advocate strengthening of the shoulder internal rotators and adductors, as well as training to decelerate the shoulder from moving into excessive horizontal abduction and/or external rotation.2,15,16
Based on these findings the supine moving apprehension test (SMAT) was designed to specifically assess the ability to control anterior shoulder instability loads. The purpose of this study was to determine the reliability and validity of the SMAT. We hypothesized that (a) the SMAT would demonstrate excellent inter-rater and good test-retest reliability; (b) healthy individuals would perform the SMAT better than patients suffering anterior shoulder dislocation (known-groups validity); (c) the SMAT would be moderately correlated with quality of life among patients with anterior shoulder dislocation (convergent validity), and (d) the SMAT score would improve significantly among patients following stabilization surgery, and that following stabilization SMAT scores would be better among patients with a negative versus a positive anterior apprehension test.
Materials and methods
Participants
Healthy participants were recruited from a university campus while patients were recruited from a shoulder surgery clinic within a large medical center. Healthy participants were recruited if they were 18–35 years old and willing to consent to the study. Potential participants were excluded from the healthy group if they had a history of a major upper extremity injury (fracture, dislocation), or had a history of low back, mid-back, neck, or upper extremity pain over the 12 months preceding their participation in the study. Injured participants were eligible to participate if they were 18 years or older, if they were seeking surgical treatment for one or more episodes of anterior dislocation and had radiological evidence of lesions corroborating anterior instability such as a Bankart and/or a Hill-Sachs lesion on magnetic resonance imaging. Potential participants were excluded from the injured group if they underwent a previous surgical procedure in the unstable shoulder, if they complained of bilateral shoulder instability, or if they could not read Hebrew and/or English language.
Examiners
A physical therapist with over 20 years of experience in the management of shoulder disorders performed all testing of injured participants. Healthy participants were examined by the same physical therapist as well as three physical therapist students who have completed all didactic and practical musculoskeletal education. Prior to data collection all examiners underwent 24-h education sessions including background and rationale for the study, as well as description of all procedures. This was followed by pilot testing of 12 healthy volunteers (not included in data analysis).
Procedure
All participants first underwent informed consent and the rights of subjects were protected. Pertinent demographic information was recorded from healthy participants including age, height, weight, limb dominance (based on their preferred arm for throwing a ball). Participants in the injured group also provided the date of injury and the overall number of shoulder dislocations. Injured participants also completed the Western Ontario Shoulder Instability Index (WOSI), a self-reported measure quality of life related to shoulder instability. 17
Healthy participants were tested on 2 occasions separated by a mean of 34 days. On each testing session, healthy participants performed the SMAT on their dominant and non-dominant arm in a random order based a random list of numbers prepared in advance (www.random.org). Two examiners simultaneously assessed the SMAT of healthy participants in order to determine inter-rater reliability. Injured participants were first tested during their pre-operative consultation (one week before surgery) and once again during their 6-month post-operative follow-up. The average time from the pre- to post-operative evaluation was 184 days.
Tests and measures
SMAT: The SMAT was performed in a gradual manner so as not to exceed participants’ ability to protect their shoulders and maintain stability throughout the test. All procedures were first performed on the uninjured side of patients or a randomly selected side of healthy participants. Participants assumed a supine lying position and were first asked to actively maintain their shoulder at 135° and then 180° of shoulder abduction in the frontal plane with the elbow fully extended (i.e., upper extremity parallel to the surface of the table). If participants could not maintain these positions actively no further testing was performed and the SMAT was rated as “0.” If participants were able to assume both positions, the procedure was repeated using a body mass-adjusted dumbbell so that participants weighing between 50 and 83 kg held a 2 Kg dumbbell, while participants weighing 84 Kg or more held a 3 kg dumbbell. If participants could not maintain the 2 positions while holding the weight no further testing was performed and the SMAT was rated as “0.” If participants were able to maintain both positions while holding the weight, the dynamic test was performed. The beginning position was with the participant lying in a supine position while holding the weight just over their chest. (Figure 1(a)). Participants then moved their shoulder to 135° of abduction with the elbow extended (Figure 1(b)), returned to the starting position, and immediately moved their shoulder to 180° of abduction with the elbow fully extended (Figure 1(c)) and finally returned to the starting position (Supplemental video 1). This cycle constituted 1 repetition of the dynamic test. During the motion into either position (135° or 180°) participants were allowed to move out of the frontal plane (typically forward) as long as the final position (135° and 180°) was established in the frontal plane with the elbow fully extended. Participants were given three trial repetitions at a self-selected speed followed by three additional trial repetitions in which they were encouraged to perform the test as fast as they could. Following completion of all trial repetitions the test was performed by counting the number of repetitions each participant could complete within a 1-min period. During the test the examiner stood to the side of the table in line with the participant's head and marked the 135° angle with his hand.
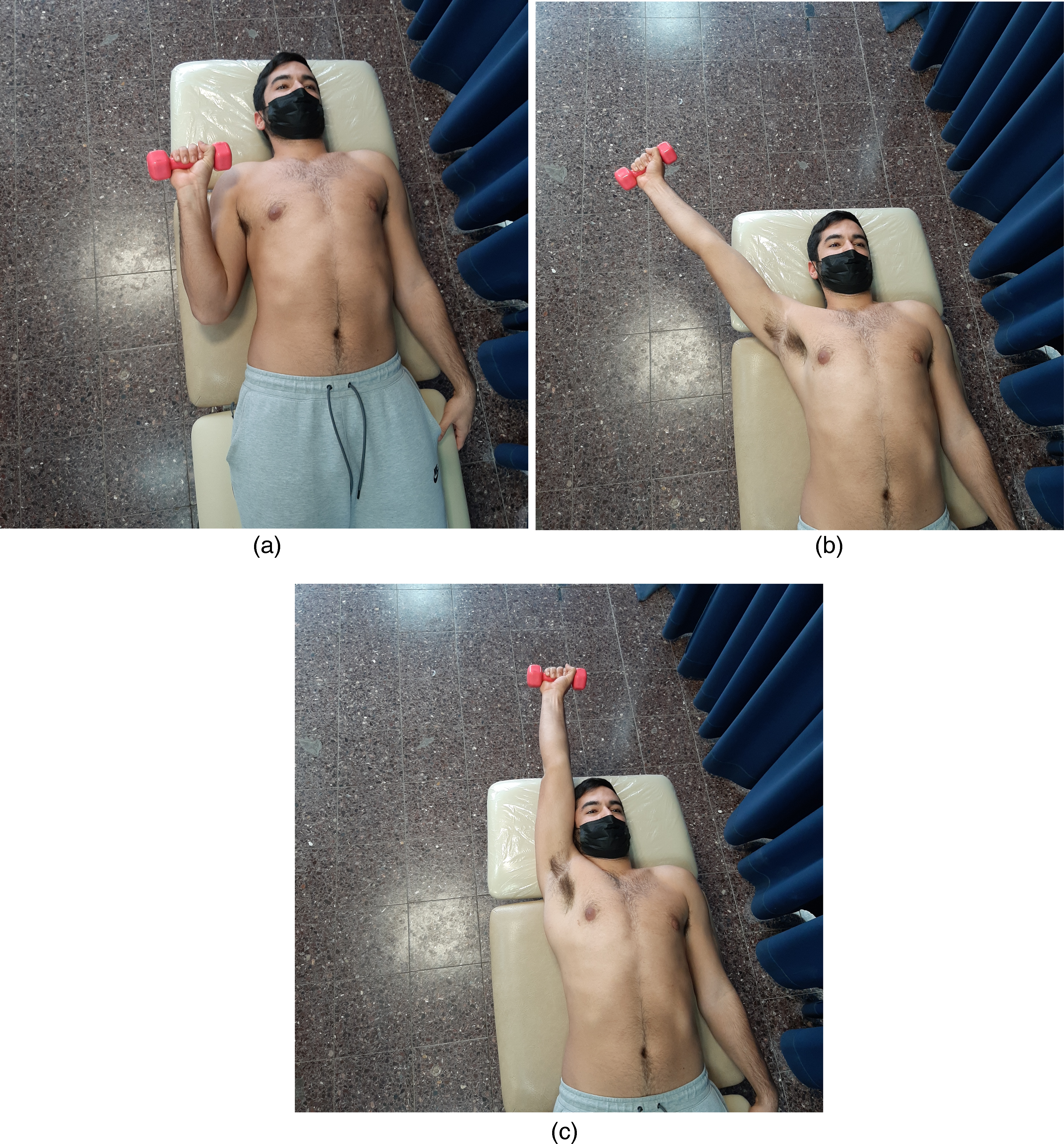
(a) supine moving apprehension test—starting position. (b). Supine moving apprehension test—135° position. (c) Supine moving apprehension test—180° position.
Supine apprehension test: The test was performed in a supine position as described by Safran et al. 18 The arm was first brought to 90° of shoulder abduction with the elbow bent 90° and the examiner supporting the distal arm and distal forearm. The shoulder was then rotated from neutral toward 90° of external rotation. The test was rated positive if the participant displayed unwillingness and apprehension in allowing the shoulder to rotate into 90° of external rotation depicted either by fascial expression, verbal communication, or physical resistance to movement. In the absence of all three the test was rated as negative.
Statistical analysis
All data were entered into SPSS 25 for statistical analysis. Descriptive statistics, including age, height weight, and mean scores for the pre- and post-operative SMAT, WOSI scores, were calculated for all participants. Data was analysed for normality and found not to be normally distributed therefore all comparisons and correlations were performed using non-parametric analyses. To detect the presence of a learning effect a Wilcoxon-Sign-Rank test was performed to compare SMAT scores (dominant and non-dominant side) between the first and second day of testing among healthy participants. Intraclass correlation coefficient (ICC2, 1) was used to determine inter-rater and test-retest (intrarater) reliability of the SMAT among healthy participants. Measurement error and responsiveness of the SMAT were measured with the standard error of the measure (SEM) based on the formula SEM = SD X √(1-ICC) and minimal detectable change (MDC) with 95% confidence based on the formula MDC95 = SEM X 1.96 X √2. Known-groups validity was determined using a Mann-Whitney U test to compare the SMAT scores between the involved shoulder of injured participants and a matched side (dominant or non-dominant) of healthy participants. Convergent validity was determined by analysing the correlation (Spearman Rho) between the pre- and post-operative SMAT and WOSI scores. For construct validity, a Wilcoxon-Sign-Rank test was performed to assess for differences between the pre- and post-operative SMAT scores of either side among injured participants as well as for the difference between SMAT change scores (post-operative minus pre-operative) of the operated versus non-operated side. In addition, a Mann-Whitney U test was performed to compare SMAT scores between injured participants with a positive and negative apprehension test following surgery. Finally, subgroup analysis was performed to compare pre- and post-operative SMAT scores based on the presence/absence of a Hill-Sachs lesion or a bony Bankart lesion (Mann Whitney U test), and to assess for the correlation (Spearman Rho) between pre- and post-operative SMAT score and the time period since the most recent dislocation, as well as the total number of previous shoulder dislocations.
Results
Eighteen healthy males and 18 males following anterior shoulder dislocation were recruited for the study. We sought to recruit both male and female participants, however over the 12-month recruitment period only two females were screened for inclusion into the anterior dislocation group. One had bilateral symptoms and a previous stabilization surgery on one of her shoulders, while the other declined surgery. We, therefore, ended up with an all-male sample. The mean age, height and weight of healthy participants were 25.9 ± 1.9 years, 174.2 ± 8.7 cm, and 74.4 ± 12.3 kg. Sixteen (88.9%) healthy participants were right-hand dominant. The mean age, height and weight of injured participants were 23.5 ± 5.2 years, 179.1 ± 6.3 cm, and 77.7 ± 13.4 kg, respectively. Sixteen (88.9%) injured participants were right-handed, while the dominant shoulder was involved among 9 (50.0%) injured participants. Fifteen (83.3%) injured participants underwent an arthroscopic Bankart repair (4 with Remplissage augmentation), while 3 (16.7%) injured participants underwent a Latarjet procedure.
Reliability
The SMAT scores during day 1 and day 2 testing as measured by both examiners are displayed in Table 1. Wilcoxon-Signed-Rank tests indicated a statistically significant greater number of repetitions on day 2 testing versus day 1 on the dominant and non-dominant side indicating the presence of a learning effect. Additionally, a statistically significant greater number of repetitions was performed with the dominant versus non-dominant side as measured by both examiners on both testing days. Intraclass correlation coefficient (95% confidence interval [CI]) for interrater reliability was 0.97 (0.92–0.99) and 0.96 (0.89–0.97) for the dominant and non-dominant SMAT, respectively. The ICC (95% CI) for test-retest reliability was 0.84 (0.63–0.94) and 0.74 (0.45–0.89) for the dominant and non-dominant side SMAT, respectively. The resultant MDC95 for the dominant and non-dominant SMAT were 10 and 12 repetitions, respectively.
Median (interquartile range) of supine moving apprehension test (SMAT) scores (repetitions) among healthy participants on day 1 and day 2 testing.
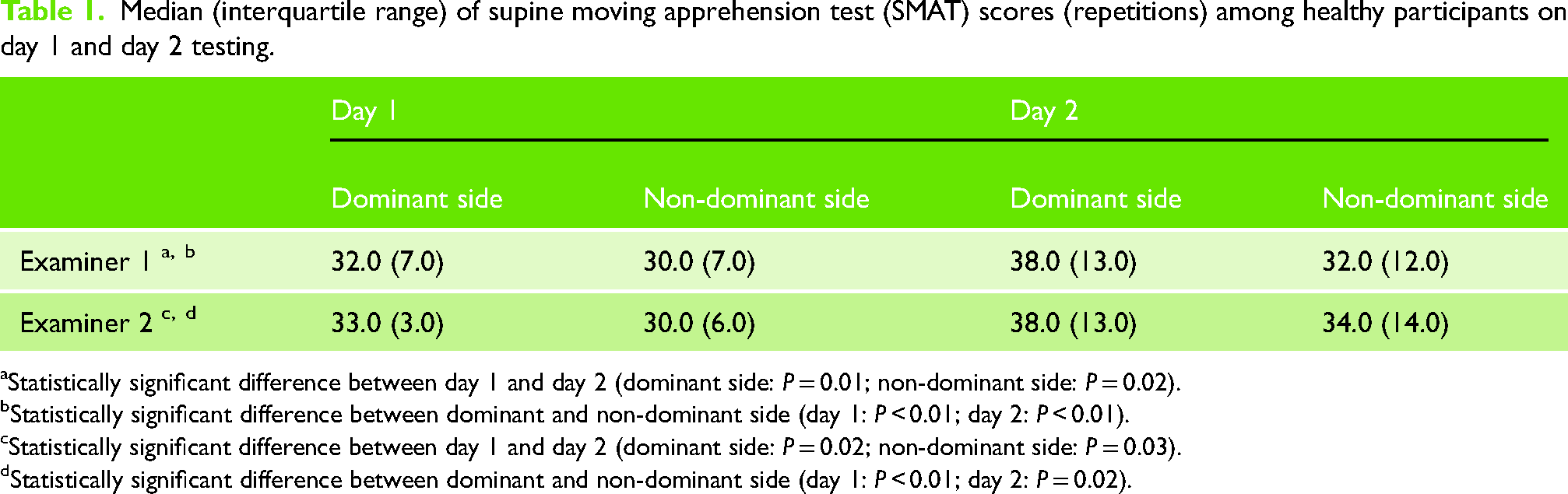
Statistically significant difference between day 1 and day 2 (dominant side: P = 0.01; non-dominant side: P = 0.02).
Statistically significant difference between dominant and non-dominant side (day 1: P < 0.01; day 2: P < 0.01).
Statistically significant difference between day 1 and day 2 (dominant side: P = 0.02; non-dominant side: P = 0.03).
Statistically significant difference between dominant and non-dominant side (day 1: P < 0.01; day 2: P = 0.02).
Known-groups validity
Descriptive statistics of SMAT scores among healthy participants during day 1 testing and injured participants during the pre-operative testing session are displayed in Table 2. Injured participants were able to perform a lower number of repetitions during the SMAT using either side (involved or uninvolved) compared with the matched side of healthy participants (Injured-involved vs. healthy-matched: 0 versus 30 repetitions, P < 0.001; Injured-uninvolved versus healthy-matched: 16 versus 34 repetitions, P < 0.001).
SMAT scores (repetitions) among injured participants (pre-operatively) and matched side of healthy participants (day 1).
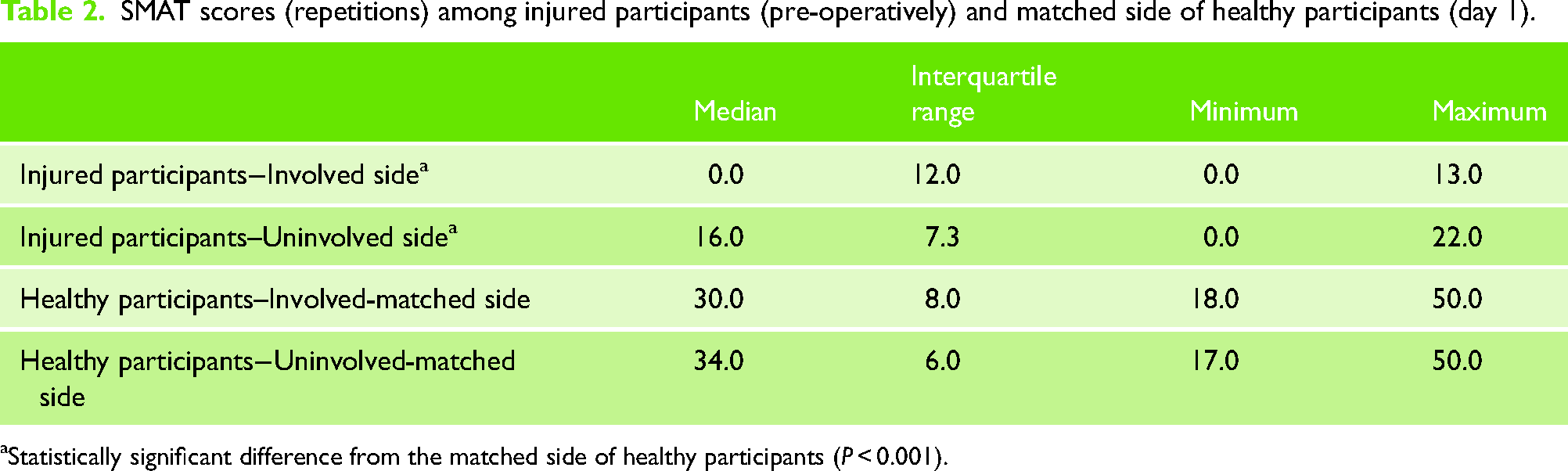
Statistically significant difference from the matched side of healthy participants (P < 0.001).
Convergent validity
The Spearman Rho analysis is summarized in Table 3. The correlation between the pre-operative WOSI and pre-operative SMAT was not statistically significant. Post-operatively a strong negative correlation was found between the WOSI and SMAT of the involved shoulder (r = −0.74, P ≤ 0.01) indicating a higher instability-related quality of life was associated with a greater SMAT score on the involved shoulder.
Correlation (spearman rho) analysis between pre- and post-operative SMAT (involved side) and WOSI scores among injured participants.
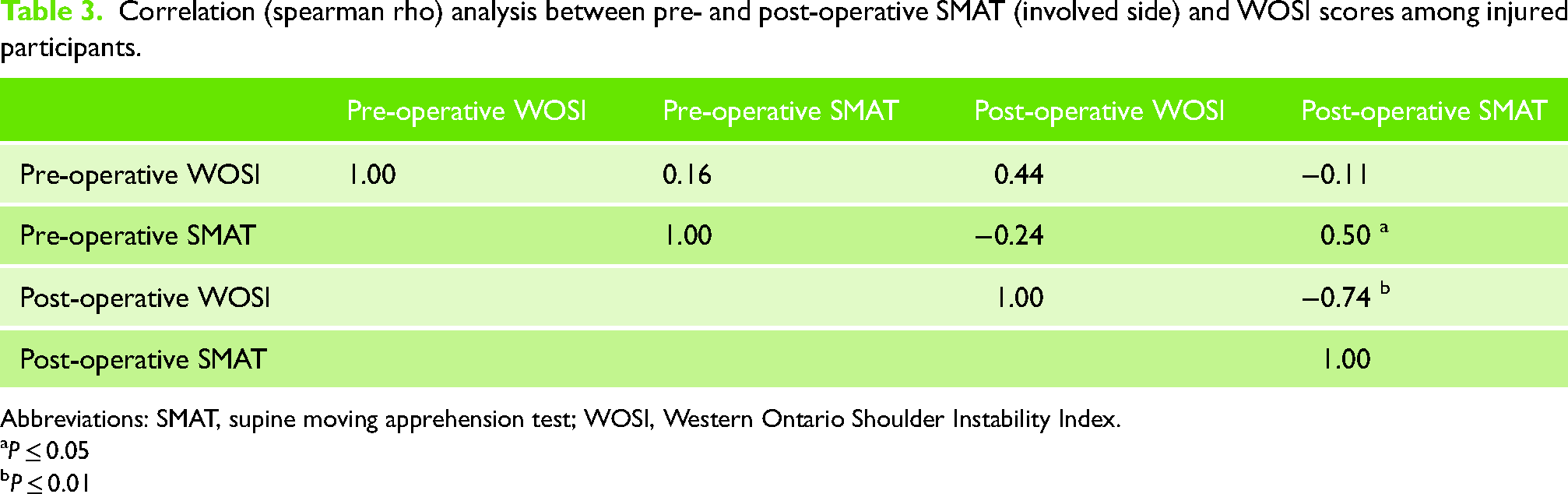
Abbreviations: SMAT, supine moving apprehension test; WOSI, Western Ontario Shoulder Instability Index.
P ≤ 0.05
P ≤ 0.01
Construct validity
The SMAT scores on the operated and non-operated side before and after surgery are summarized in Table 4. The SMAT scores significantly improved following surgery on both sides (P < 0.01). A statistical trend was detected toward a greater change score on the involved versus the uninvolved shoulder (15.0 versus 9.0 repetitions, P = 0.07). Finally, SMAT scores were significantly greater among participants with a negative compared with participants with a positive apprehension test following surgery (22.5 versus 0.0, P < 0.01).
Median (interquartile range) of pre-operative, post-operative, and change score of the SMAT on the involved and uninvolved side of injured participants.
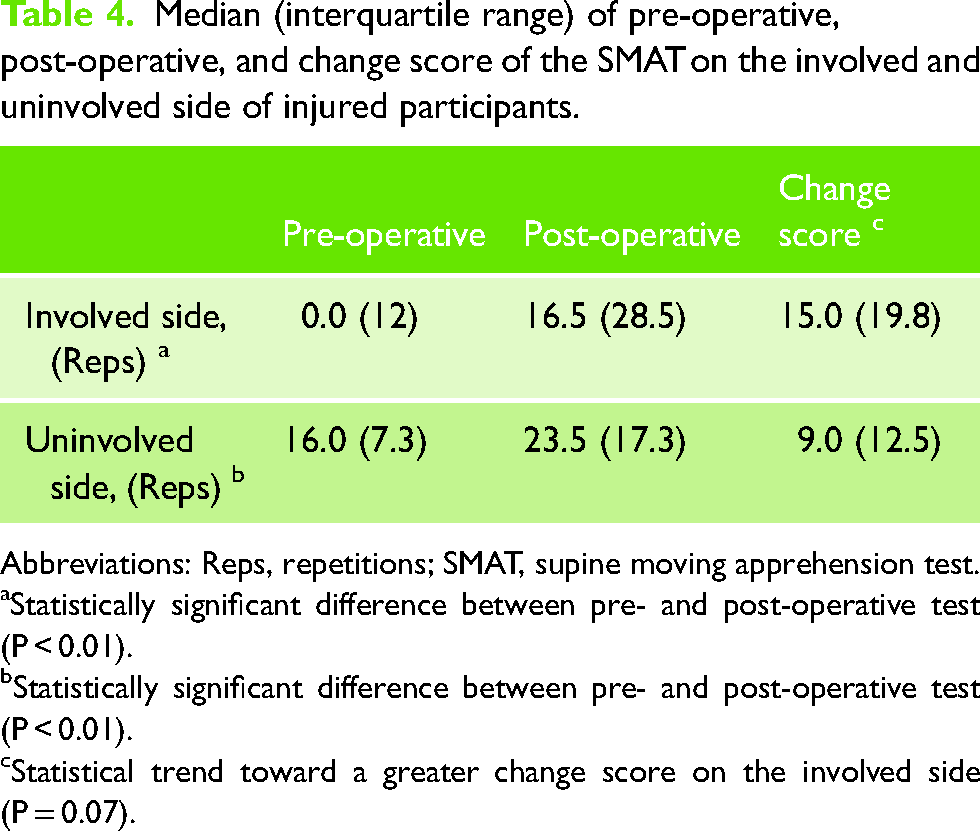
Abbreviations: Reps, repetitions; SMAT, supine moving apprehension test.
Statistically significant difference between pre- and post-operative test (P < 0.01).
Statistically significant difference between pre- and post-operative test (P < 0.01).
Statistical trend toward a greater change score on the involved side (P = 0.07).
Subgroup analysis
The SMAT scores did not differ between patients with or without a Hill-Sachs lesion (pre-operative SMAT, P = 0.42; post-operative SMAT, P = 0.68). The SMAT scores did not differ between patients with or without a bony Bankart lesion (pre-operative SMAT, P = 0.72; post-operative SMAT, P = 0.15). The SMAT scores did not correlate with the time period since the most recent episode of shoulder dislocation (pre-operative SMAT, r = −0.20, P = 0.47; post-operative SMAT, r = −0.04, P = 0.89). Finally, while pre-operative SMAT scores did not correlate with the number of previous dislocations (r = −0.26, P = 0.32), post-operative SMAT scores were negatively correlated with the number of previous dislocations (r = −0.55, P = 0.02). The negative nature of this correlation indicates that a greater number of previous dislocations was associated with lower post-operative SMAT scores.
Discussion
The SMAT is reliable and valid among patients with anterior shoulder dislocation. Along with an excellent inter-rater and good test-retest reliability, a learning effect does seem to affect performance of the SMAT with repeat applications, and consequently, it is imperative to consider the MDC when assessing for change over time. The validity of the SMAT is supported by several different findings. First, a clear difference exists between SMAT scores of healthy individuals and those of patients with anterior shoulder instability. Furthermore, only 7 of 18 (38.9%) injured participants were able to perform the SMAT on their injured side compared with all 18 healthy participants. Second, the performance of the SMAT was significantly improved among injured participants following stabilization surgery. Although improvement was evident bilaterally, only the change score of the injured side surpassed the MDC95 of the SMAT. Thirdly, following surgery patients with residual apprehension, who may be less confident regarding the stability of their shoulder, performed significantly worse on the SMAT compared with those with no apprehension. And, finally, a strong correlation was found between the post-operative SMAT score and quality of life-related to shoulder instability. The absence of such a correlation pre-operatively was most likely due to the inability of most injured participants to perform the SMAT before surgery.
Several physical performance measures have been previously developed for patients with shoulder disorders. Although the reliability of these tests has been established,19–25 little evidence exists to support their validity. 26 Furthermore, given that all these tests involve weight bearing on the upper extremity with the shoulder flexed approximately 90° they are more likely to result in a posterior shear force across the glenohumeral joint, 27 suggesting they may be less relevant for patients with anterior shoulder instability. 27 The shoulder endurance test 28 and the posterior shoulder endurance test 29 were designed to assess posterior rotator cuff endurance, which may be relevant for overhead athletes but is not specific for athletes with anterior shoulder instability. Finally, the athlete shoulder test which seems to place anteriorly directed forces on the abducted shoulder has yet to be validated and is also limited by the need for expensive measuring equipment. 30 Given the void in performance-based measures specifically designed to challenge anterior shoulder stability, the SMAT seems particularly valuable and represents a useful tool to fill this gap.
Interestingly, patients with shoulder instability demonstrated inferior SMAT scores on their injured as well as their uninjured side compared with healthy controls. This is particularly noteworthy as all injured participants denied any symptoms of shoulder instability on the uninvolved side. A possible explanation for this is the presence of a learned protective behavior affecting performance on the uninvolved side. Injured participants may have performed the SMAT more cautiously (slower) based on their perception of its potential to induce shoulder instability. This is supported by previous findings of changes within cortical areas regulating motor planning, cognitive control of motion, and recognition of threatening conditions among patients following anterior shoulder dislocation.31,32 Alternatively, it may be that some intrinsic qualities inherent to individuals with shoulder dislocation may also hinder the performance of the SMAT on either side. Qualities such as generalized ligamentous laxity and increased shoulder external rotation ROM that have been previously associated with a shoulder dislocation, 33 may also manifest in poor performance of the SMAT. In that sense, the SMAT may hold potential in screening for the risk of shoulder dislocation among young and active individuals.
Another notable finding is the negative correlation between the previous number of dislocations and post-operative SMAT scores. Post-hoc analysis based on a median split of the number of previous dislocations (median = 4) revealed that patients with ≥ 4 previous dislocations demonstrated a lower post-operative SMAT score compared with patients with ≤ 3 previous dislocations (9.9 versus 25.9 repetitions, Mann-Whitney U test, P = 0.02). Eshoj et al. 34 did not find differences in quality of life, fear of reinjury, proprioception, or strength among patients following a single versus patients following multiple shoulder dislocations. 34 Concomitant with the lack of correlation between pre-operative SMAT scores and the number of previous dislocations, these findings suggest patients with more previous dislocations may be less able to regain dynamic shoulder control following surgery. More emphasis on neuromuscular control may need to be placed post-operatively among patients with more previous shoulder dislocations.
Our study has several limitations. Although ultimately designed to assist in determining readiness to return to sport, the predictive validity of the SMAT in so doing cannot be determined from the present study. A prospective design, monitoring the level of sport participation as well as recurrence rates would ultimately serve to answer this question. Second, the sample size is relatively small and consists of male participants only. However, post hoc power analysis revealed 42 participants (21 in each group) would have been needed to establish known-groups validity and 12 injured participants would have been needed to establish construct validity assuming a large effect size (d = 0.8), a P-value ≤ 0.05, and 80% power. Given the very large effect size associated with most analyses it seems our study had enough power to detect statistically significant effects. Third, we did not document the presence of generalized ligamentous laxity among participants of this study, and therefore we cannot determine any possible associations between its presence and performance of the SMAT on the involved or uninvolved side. Finally, the extent to which loads placed on the shoulder during the SMAT simulate the actual forces associated with shoulder dislocation is still unknown. Establishing these would add valuable information regarding the SMAT and further establish its validity among patients with anterior shoulder instability.
Conclusion
The SMAT is reliable and valid among patients with anterior shoulder dislocation. Given the lack of performance-based measures specifically designed to challenge anterior shoulder stability, the SMAT may serve a valuable addition to the assessment of patients following shoulder dislocation. Further study is needed to establish the utility of the SMAT in determining readiness to return to sport following shoulder dislocation.
Supplemental Material
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.