
Abstract
A proportion of patients with anterior glenohumeral instability present with bipolar bone loss comprising large Hill-Sachs lesions and substantial glenoid defect. These are surgically difficult cases to treat. We describe a novel surgical procedure of bulk size-matched osteochondral allograft reconstruction for massive Hill-Sachs lesions combined with the Latarjet procedure for these challenging cases.
Keywords
Introduction
Traumatic glenohumeral instability is a common orthopaedic problem, with an overall incidence of about 7.5 to 51 per 100,000 person-years.1–5 Recurrent subluxation and dislocation can result in worsening damage to the glenohumeral joint, namely fracture or erosion of the anteroinferior glenoid margin with indentation or impaction fracture of the posterior humeral head, the Hill–Sachs lesion. Griffith et al. 6 found that 41% of patients with a first-time dislocation and 86% of those with recurrent instability had glenoid bone loss. Hill–Sachs lesions are reported in 65% to 67% of cases following first-time dislocations and in 84% to 93% of recurrent dislocations.7,8 Bipolar bone loss, the combination of glenoid and humeral bone loss, has reported prevalence of 64% to 70% in first-time anterior dislocations and 79% to 84% in recurrent anterior dislocations.6,9
The interplay between glenoid bone defect and Hill–Sach's lesion in shoulder instability was first publicised with the description of ‘engaging’ versus ‘non-engaging’ Hill–Sachs lesions. 10 Itoi and others11,12 introduced the concept of the glenoid track, in which the intact glenoid width is compared with the dimensions of the Hill–Sachs lesion. Shoulders with bipolar bone loss in which the Hill–Sachs widths are larger compared to the intact glenoid are termed ‘off-track’ lesions. These dislocate more readily and have higher failure rates with Bankart repairs.11,13,14
Bone defects of glenoid over 20% to 25% glenoid width, when associated with large Hill–Sachs lesions pose particularly difficult problem. The ‘remplissage’ procedure has shown good outcomes but there are concerns about loss of range of motion.15–17 For larger humeral head defects, alternative surgical options have been proposed. These include humeroplasty or disimpaction of the defect, rotational osteotomy, partial or complete resurfacing, hemiarthroplasty and bone graft reconstruction with autograft (iliac crest) or with allograft. 18
We describe our surgical technique for management of patients with both a large Hill–Sachs lesion and substantial glenoid bone loss and report the outcomes of a series of 10 patients who underwent this procedure.
Materials and methods
Between 2013 and 2019, 10 patients with recurrent anterior instability underwent combined osteochondral bulk humeral allograft reconstruction for large Hill–Sachs lesion combined with Latarjet anterior stabilisation. All patients had undergone examination under anaesthesia and arthroscopic evaluation prior to definitive surgery. The indication for the procedures was ‘engaging’ Hill–Sachs lesion or ‘off-track’ bipolar bone loss. Patients with humeral head defects presented to the central articular area of the glenoid during functional ranges of movements were also included for Hill–Sachs bone grafting.
Radiographic evaluation
Imaging included magnetic resonance (MR) arthrograms and/or computed tomography (CT) scans with three-dimensional reformatting. The diameter of the humeral head was determined. Size-matched fresh frozen humeral head allografts of the dimension (+/−4 mm of the diameter of the patient's humeral head) were ordered from the NHS Blood and Transfusion Service (Liverpool). From the scans, dimensions of the glenoid bone loss and Hills–Sachs lesions were measured (Figure 1). ‘On-track’ or ‘off-track’ bipolar relationship was estimated as described by Giacomo, Itoi and Burkhart. 12
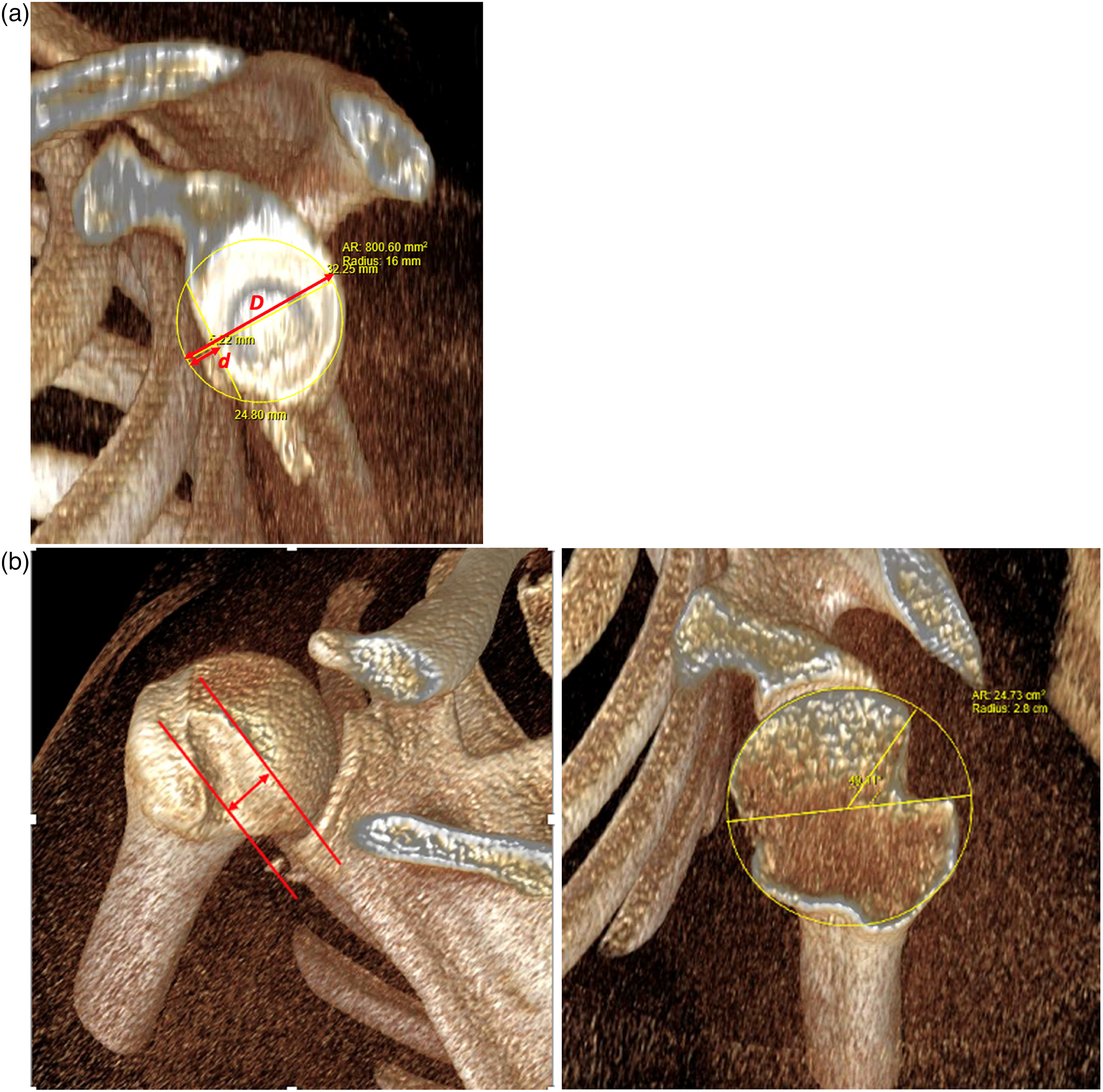
(a) Measurements of glenoid bone loss. For estimation of the intact glenoid, the ‘best-fit circle’ method was applied, fitting a circle to the posterior and inferior parts of the glenoid. This circle is considered to approximate the original shape of the glenoid. The diameter of the circle ‘D’ represents the width of the intact glenoid and radius r = D/2. The radial extent of the perimeter of the circle towards the defect is the amount of bone that is lost and is expressed as ‘d’. The size of the defect is expressed as: linear glenoid bone loss = d/D. The intact glenoid surface area, SAG, can be calculated, SAG = πr2. The surface area of the glenoid defect, a circular segment, can be obtained by using the length of the linear glenoid defect, d. The formula for this is:
Surgical technique
Under general anaesthesia and interscalene regional anaesthetic block, the patient is positioned in a modified ‘deck-chair’ and a deltopectoral approach made to the shoulder (Figure 2). The arm is held by an arm holder or supported in a gutter by the patient's side.
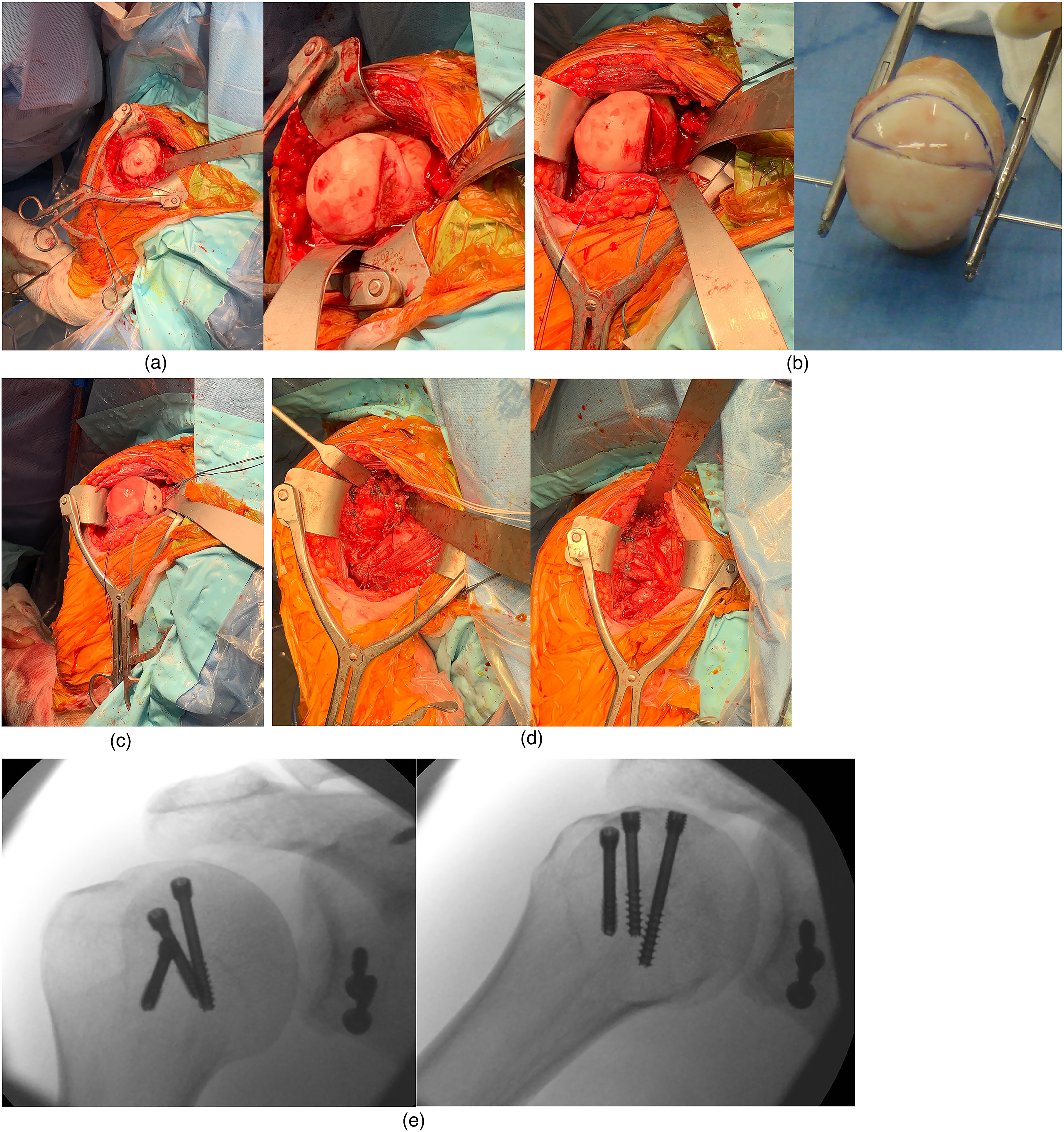
(a) Exposure of the Hill–Sachs lesion. Following an anterior capsulotomy, the humeral head is delivered, and the Hill–Sachs lesion exposed through extension and external rotation of the arm, while translating the humeral head anteriorly. Excessive extension and traction are avoided to prevent axillary nerve and brachial plexus injury. (b) Preparation of the Hill–Sachs osteochondral allograft. The edges of the Hill–Sachs defect are prepared and dimensions measured. The surface area of the defect is then traced onto sterile paper and drawn onto the size-matched osteochondral allograft. A 2 mm K-wire is used to handle the allograft when the wedge allograft is harvested at a back table with a surgical saw. (c) Implantation of the osteochondral allograft. The allograft is then presented onto the defect and further adjustments are made to fit into the prepared Hill–Sachs defect. The allograft is secured with three 4.5 mm headless compression screws. (d) Latarjet procedure, capsular repair and closure. The Latarjet procedure is then completed through transfer of the coracoid onto the anterior glenoid edge, followed by the repair of the ‘T’ capsulotomy. The subscapularis tenotomy is then repaired, followed by repair of the pectoralis minor onto the coracoid ‘stump’. (e) Intra-operative radiographs depicting the congruence of the allograft with the humeral head curvature, secured with three 4.5 mm headless compression screws. Note also the coracoid transfer of the Latarjet procedure, held with two screws, and a suture anchor at base of the excised coracoid for reattachment of pectoralis minor.
The Latarjet component of operation is performed in accordance with Burkhart's description. 19 The coracoid is osteotomised close to its base, anterior to the coracoclavicular ligament and mobilised together with the attached coracobrachialis and short head of biceps. The musculocutaneous nerve is always identified and safeguarded.
An ‘L-shaped’ subscapularis tenotomy is performed, preserving the lower one-third to protect the axillary nerve. This is done in a stepwise approach to ensure the glenohumeral joint capsule and subscapularis tendon are taken as separate layers. First, a horizonal split by blunt dissection in line with the muscle fibres of the subscapularis is made. We find it easiest to start medially where the red muscle belly is readily distinguishable from the white capsule. A Gelpi retractor is inserted into the split and a small swab pushed between the capsule and subscapularis to separate them. Once the muscle and capsule are separated the tenotomy can be completed by heading laterally along the horizontal limb and then cranially. We do this with careful sharp dissection using a fresh number 15 scalpel on a long handle. The tendon is held with a stay suture.
Next, the joint is entered through a T-shaped capsulotomy with the top of the T medially. This needs to be done with great care as the capsule can be attenuated from the recurrent dislocations. Securing the two leaves with a stay suture makes them easier to identify and repair at the end of the operation.
The humeral head is then delivered. The Hill–Sachs lesion can be exposed with the arm extended and externally rotated, with the humeral head translated forward. To prevent axillary nerve and brachial plexus traction, excessive external rotation and traction to the arm is avoided. This part of the operation carries the highest risk of traction on the brachial plexus. In the event of any delay, we advocate relocating the humeral head and resting the shoulder in neutral rotation.
The defect is prepared by osteotomising the side wall of the wedged defect until healthy bleeding bone is encountered. The Hill–Sachs surface defect is traced onto a sterile paper as a template. The dimensions of the prepared lesion are carefully measured (the 2 borders of surface arc of the ‘lune’ and the 2 depths of the wedge).
The sterile template is then traced onto the humeral head allograft. The wedge is carefully harvested from the humeral head allograft and shaped to fit onto the patient's Hill–Sachs defect. The allograft is secured with a temporary K-wire while 4.5 mm headless compression screws are inserted (DePuy Synthes), stably fixing and compressing the allograft onto the host humeral head.
The humeral head is then relocated and the Latarjet operation completed. The coracoid and strap muscles are transferred and attached with two screws to the anteroinferior edge of the glenoid to form a ‘congruent arc’. The anterior capsule and labrum repair are reattached to the host's original anterior glenoid with suture anchors to render the coracoid graft extracapsular. The suture anchors are inserted onto the anterior rim of the glenoid prior to coracoid fixation to ensure that the coracoid graft remains extra-articular. The wound is then closed following careful repair of subscapularis and reattachment of pectoralis minor onto the base of the osteotomised coracoid.
Post-operatively, the patient is immobilised in a sling for 4 weeks but permitting passive movement ranges within safe zones immediately. Active-assisted exercises commence from 4 weeks with the aim of restoring movement span by 3 months. Between 3 and 6 months, the focus is on shoulder stability with scapular setting, proprioceptive exercises and targeted sports-related or function-related rehabilitation.
Results
All 10 patients were male (Table 1). The average age of the time of surgery was 28 years (21–34). The cohort had endured an average of 5.3 years (1–15) of anterior instability and have experienced on average 7 dislocations (4–16) before the combined humeral head reconstruction and Latarjet operation.
Patient details and outcomes.
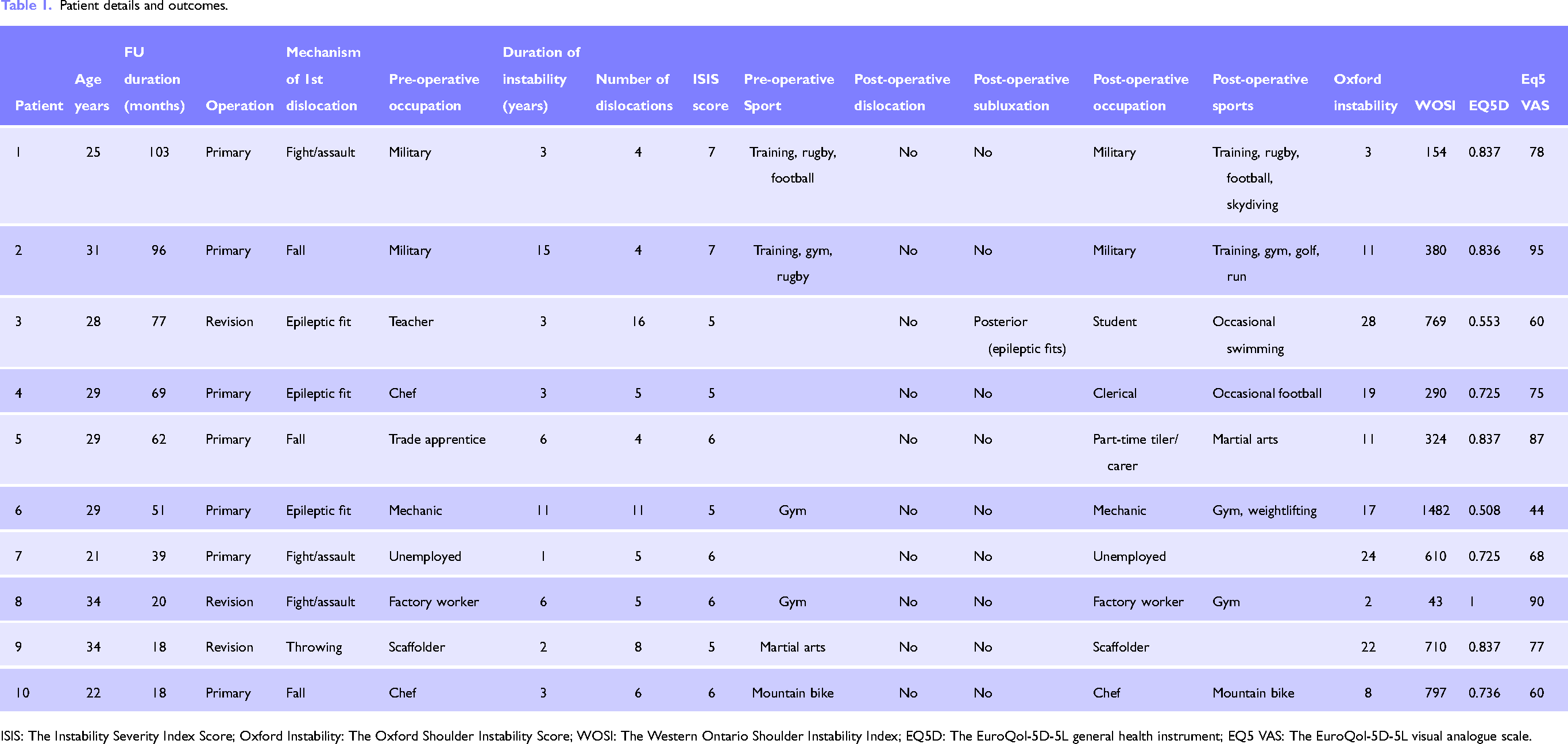
ISIS: The Instability Severity Index Score; Oxford Instability: The Oxford Shoulder Instability Score; WOSI: The Western Ontario Shoulder Instability Index; EQ5D: The EuroQol-5D-5L general health instrument; EQ5 VAS: The EuroQol-5D-5L visual analogue scale.
The average linear glenoid bone defect was 21% (18–25). The average surface area glenoid bone loss was 14.9% (13.0–19.5). The Hill–Sachs lesion occupied average of 24.5% (19.7–30.6) of the humeral articular surface. Total glenoid and humeral bone loss in relation to the total glenoid and humeral articular surface was 23.0% (18.7–28.0). Seven of the cohort had ‘off-track’ lesions, while 3 were marginally ‘on-track’ with width of glenoid versus Hill–Sachs difference of <1 mm.
None of the patients reported further anterior dislocation of the operated shoulder. However, two patients subjectively describe symptoms of instability: Patient 6 interpretes crepitus on movement as instability while Patient 3, an epileptic, subluxes posteriorly and self-relocates after fits. Both patients had neither excessive anterior laxity/translation nor apprehension on clinical testing.
Seven patients reported some intermittent pain in the shoulder: three moderate and four mild. There were no cases of infection in this cohort. Three patients had transient axillary nerve palsy, but all recovered within 4 to 6 weeks.
Eight of the 10 patients are in employment, including 2 military personnel who continue to enjoy successful careers in the army. Eight are still participating in sports. Range of movements in the 6 patients who were examined were: external rotation 30 to 70 degrees, flexion 160 to 180 degrees and abduction 160 to 170 degrees.
Radiographs at follow-up revealed partial resorption of the allograft in three patients (Figure 3). The most severe was Patient 6, with substantial surface loss, while two patients had relatively minor osteolysis around the screw heads (Patients 9 and 10).

Osteolysis of osteochondral graft. Patient 6. (a) Immediate post-operative radiograph. (b) Radiographs at 51 months: osteolysis of the allograft is observed. The patient suffered an epileptic fit 3 weeks after surgery. Also note that the headless compression screws were smaller than the preferred 4.5 mm screws. Patient 9. (c) Intra-operative radiograph. (d) Radiographs at 18 months: minor osteolysis around one of the screws but the allograft has incorporated. Although the screw heads appeared higher than the subchondral bone, the screws were level against the chondral cartilage of the allograft.
Discussion
We are not aware of any other publications to date that described the combined surgical procedure of bulk osteochondral allograft for a massive Hill–Sachs lesion in conjunction with the Latarjet operation for large bipolar bone loss. Our case series suggest that this operation is a solution to this difficult problem. There were no anterior dislocations reported in our patients after surgery. Movement ranges were preserved. The procedure enabled our cohort to return to their employment and sports.
Although the transplanted allograft had incorporated into the host humeral heads, we have observed osteolysis on the subchondral surface of the allograft, particularly in the regions surrounding the compression screws. This might be attributable to early instability of the osteochondral graft fixation. A further reason may be that fresh frozen allografts, rather than fresh allografts were used. This, as suggested by Saltzman et al., 20 might be associated with graft necrosis or resorption.
Most authors agree that with glenoid bone loss between 20% and 25%, restoration of the glenoid deficit can convert an ‘off-track’ to an ‘on-track’ glenoid lesion.21–25 When associated with a large Hill–Sachs lesion, ‘remplissage’ with Latarjet, has been recommended.26,27 However, to restore the humeral head articular arc, resurfacing of the Hill–Sachs defect remains the only option. This can reduce the degree of anterior translation before dislocation and restore the concavity-compression mechanism. The congruent articular surfaces create greater contact area and reduce articular contact pressure between the glenoid and humeral head. Improvement in the range of motion can be expected with the elimination of the engaging lesion.28,29
The literature is currently limited to case series for humeral head allograft transplantation. Two studies reported no recurrent dislocations and high satisfaction rates.30,31 In a systematic review by Saltzman et al., 20 improvements in range of motion and functional scores were observed. However, complications of allograft necrosis occurred in 8.7% and resorption in 36.2%.
Only one study has reported simultaneous Hill–Sachs and anteroinferior glenoid reconstruction. Haber et al. 32 published a case report in which distal tibial allograft (DTA) was used for glenoid reconstruction together with allograft Hill–Sachs reconstruction. Their rationale for DTA over Latarjet is that the former has better joint congruity and denser trabecular matrix, making it an optimal graft.33,34 However, we favour the Latarjet procedure as it confers additional dynamic stabilising effect of the transferred coracobrachialis and short head of biceps.
This study has the limitation of a small retrospective survey without a control group. Although the results are promising, longer-term evaluation will be helpful to assess the impact of graft osteolysis. Further comparative research of glenoid reconstruction with either Hill–Sachs allograft or ‘remplissage’ should be done to define which is superior.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.