
Abstract
Background
The purpose of this retrospective study was to analyze whether chemically sterilized tendon allografts perform as well as other non-sterilized allografts and autografts as described in the literature for anatomical acromioclavicular joint stabilization for the treatment of Rockwood III–V. Allografts are still described as a factor for higher re-rupture rates.
Methods
Retrospective data were collected from 21 acromioclavicular joint stabilizations performed by a single surgeon and performed between 2011 and 2014 using sterilized semitendinosus allografts. The primary endpoints were re-rupture and complication rates. Secondary endpoints were AC-joint stability, pain level, return to work and sport and the range of motion.
Results
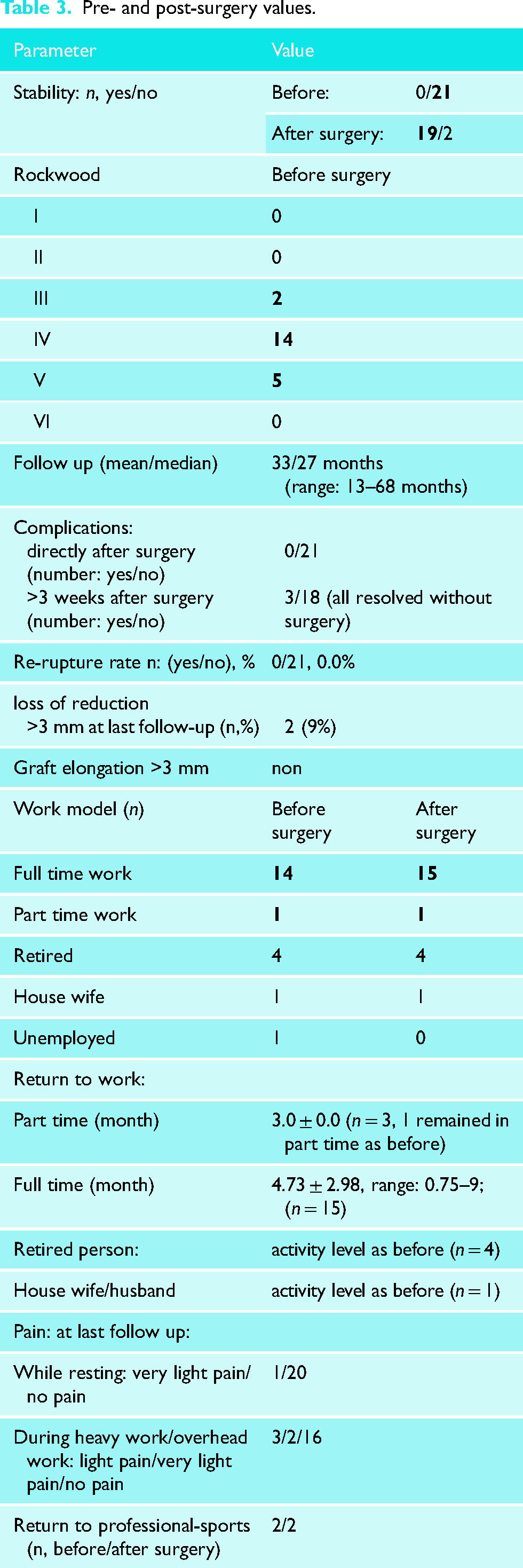
No re-ruptures occurred during the mean follow-up time of 33 months. Zero complications occurred directly after surgery, but three complications later than three weeks after surgery. All cases resolved without further surgery. After surgery, stability significantly improved for all patients. Post-surgery, 19 patients had stable acromioclavicular joints and only two patients showed minor instabilities. Range of motion returned to the range of the healthy shoulders for all patients.
Conclusion
Chemically sterilized semitendinosus allograft use for anatomic AC-joint stabilization is equivalent to the use of other allografts or autografts and required no hardware removal. No donor age or graft size dependence was observed, due to zero re-ruptures.
Introduction
Acromioclavicular (AC) joint injuries are common in athletic populations1–3 and more so in males than in females.2–4 An overall incidence rate of 9.2 per 1000 person-years was reported. 5 AC-joint injuries are most commonly caused by direct trauma to the lateral part of the shoulder or acromion with the arm in an adducted position. The force drives the acromion inferiorly, with the clavicle remaining in its anatomical position. 2 Sequential injury occurs with the rupture of the AC-joint capsule structure, discus, AC ligaments and extends to the coracoclavicular (CC) ligaments. 2 Severe injuries may also disrupt the attachments of the deltoid and trapezius. 2 Studies show that operative management of Rockwood grade III acromioclavicular dislocations results in better cosmetic outcomes but longer patient sick leave.6,7 The treatment of AC-joint injuries is still controversial,2,4,7–12 and various procedures have been described.1,4,7,8,11–13 Surgeons must approach this injury with meticulous attention to detail and technique. 14 The anatomical technique aims to reconstruct the coracoclavicular ligaments by bringing the clavicle back into its anatomical position. Biomechanical studies have shown superior reconstruction strength and stability when using the anatomical technique compared with standard non-anatomical techniques.1,14 It has been reported that reconstruction with free tendon grafts displays a low rate of unplanned re-operations, a high subjective score and a low complication rate. 15 Reconstruction of the CC- and AC-ligaments with an allogenic tendon provides good stability of the AC-joint7,10–12,16–20 and has gained popularity in the past few decades.7,13,20–23 The clavicle is further strengthened by AC-ligament reconstruction allowing for horizontal stabilisation of the clavicle. 10 The tendon allograft plays an important role in AC reconstruction, particularly for patients who have a shortage of autograft tendons or for those who do not want to use their own functioning tendons. 10 Advantages of allografts include attenuated donor site morbidity13,18 and a wider selection of graft sizes and tissue types. 24 The disadvantages may include slower biological remodelling and a theoretical risk of disease transmission, 24 that is minimised when using sterilized grafts. The sterilization of allografts is an important aspect as gamma-irradiated achilles allografts have shown increased failure rates when compared to their non-irradiated counterparts. 25 In addition to this, gamma-irradiated bone-patellar tendon-bone allografts elongate 27% more than without radiation. 26 Biological grafts are preferred over synthetic grafts because of their superior clinical and radiographic outcome.27,28 Moreover, literature addressing sterilized allografts is still scarce. Currently, there is no consensus regarding the optimal graft choices for AC-joint stabilization. Semitendinosus (ST) allografts1,2,11,13,17,20,22,29,30 are mainly used for AC joint reconstruction with other allografts also being used.2,7,10,11,20,27 Costic et al. 31 concluded that with semitendinosus grafts, the course of the ligaments can be imitated, providing stability to the clavicle similar to that provided by the intact ligaments. From a biomechanical point of view, an anatomical reconstruction using a free tendon graft and imitating the two-bundle course of the CC-ligament complex provides improved stability. Biomechanical studies have shown that, compared with other constructs, the semitendinosus tendon displays a clinically irrelevant (<3 mm) permanent elongation after cyclic loading and a stiffness that more closely resembles the stiffness of the intact CC-ligaments. 9 The semitendinosus graft has an ultimate failure load that is equivalent to the native CC ligament. 14 The strength of the semitendinosus graft also decreases the risk for premature failure, theoretically promoting an earlier postoperative range of motion and rehabilitation, resulting in less shoulder stiffness, thus facilitating an earlier return to sports. 32 These grafts (ST) are long enough to allow anatomical reconstruction that duplicates the origins and insertions of the trapezoid and conoid ligaments, further reinforcing the ruptured AC ligaments. 32
The hypothesis of this study is that chemically sterilized allograft use for anatomical AC reconstruction would reveal similar results to other allografts reported in the literature with respect to re-rupture rate, complications and functionality.
Methods
Data collection
The ethic vote was received from the Ethic commission of the ‘Bayrische Landesärztekammer’ (2020–1025). The observational study was designed as a retrospective data collection of surgeries performed between 2011 and 2014 in one treatment centre only that was performed by a single surgeon. During this period, only one surgery method was used. Thus, no control group is available and a comparison to the literature will be performed. The inclusion criteria consisted of the tendon allograft used (provided by the DIZG gGmbH between 2011 and 2015), patient age (over 18 years) and at least 10 days between accident and surgery to only include sub-acute and chronic patients. A total of 21 patients were included and treated by a single surgeon. One patient was excluded due to an acute surgery. Acute cases (up to 9 days post-trauma) had been treated with arthroscopic tight rope technique. This special surgical procedure used for sub-acute or chronic cases does not occur every week, thus the number of patients to be included is limited. The primary outcome of the study was the re-rupture rate and complications after a mean follow-up of 33 months. Secondary endpoints were the stability of the AC joint (restored craniocaudal and horizontal stability, loss of reduction), pain level (classified as severe, moderate, light, very light or no pain), return to work, sport and the range of motion according to the Neutral-0-Method. 33 All data were collected anonymously in a questionnaire provided by the DIZG gGmbH.
Grafts
All allografts analyzed were provided by the German Institute for Cell- and Tissue Replacement (DIZG gemeinnützige GmbH). They were sterilized using a validated, GMP-compliant process and approved as medicinal products under §21 of the German Medicinal Products Act (license number: PEI.H.03356.01.1). In summary: All tissues are acquired from non-profit tissue recovery partners after informed consent. Tendons and ligaments from a single donor are thawed at 2–8 °C and remnants of blood, fat and connective tissue are removed. For sterilization, tissues are fully submerged in validated tissue-preserving sterilization solution (2% peracetic acid, 96% ethanol, aqua ad iniectabilia; ratio v/v/v | 2/1/1) and incubated with constant agitation, at low pressure and at room temperature for 4 h. Subsequently, tissues are rinsed in a washing process using aqua ad iniectabilia. Under aseptic conditions (class A clean room), the sterile grafts are then transferred into primary and secondary packaging. The allografts are stored at −40 °C and can be used for up to two years.
Surgical technique
Radiographs are performed in craniocaudal, anteroposterior and axial view to evaluate the displacement of the clavicle (Figure 1). The patient is in the ‘beach chair’ position with the arm positioned on an automated arm holder (Trimano®, Arthrex, Naples, FL, USA). Open surgery is performed for all patients with a vertical incision of approximately 7 cm long and 2 cm medially to the AC joint, in the coracoid direction. A delto-pectoral split approach is used to access the coracoid base for the management of the caudal graft placement and for the reinforcement suture. In acute injuries, access to the AC joint, capsular structures, disk, distal clavicle occurs through the ruptured capsule and the trapezius-deltoid fascia. In chronic instabilities, an approximately 5 cm longitudinal cut is performed through scar tissue centred over the distal clavicle and oriented to the anterior part of the acromion without damaging the deltoid or the trapezius muscle. Resection of the ruptured disk is performed. The torn acromioclavicular joint capsule is prepared meticulously for additional capsular reconstruction using trans-osseous non-absorbable Etibond sutures to the ventral and dorsal distal clavicle (Figure 2).
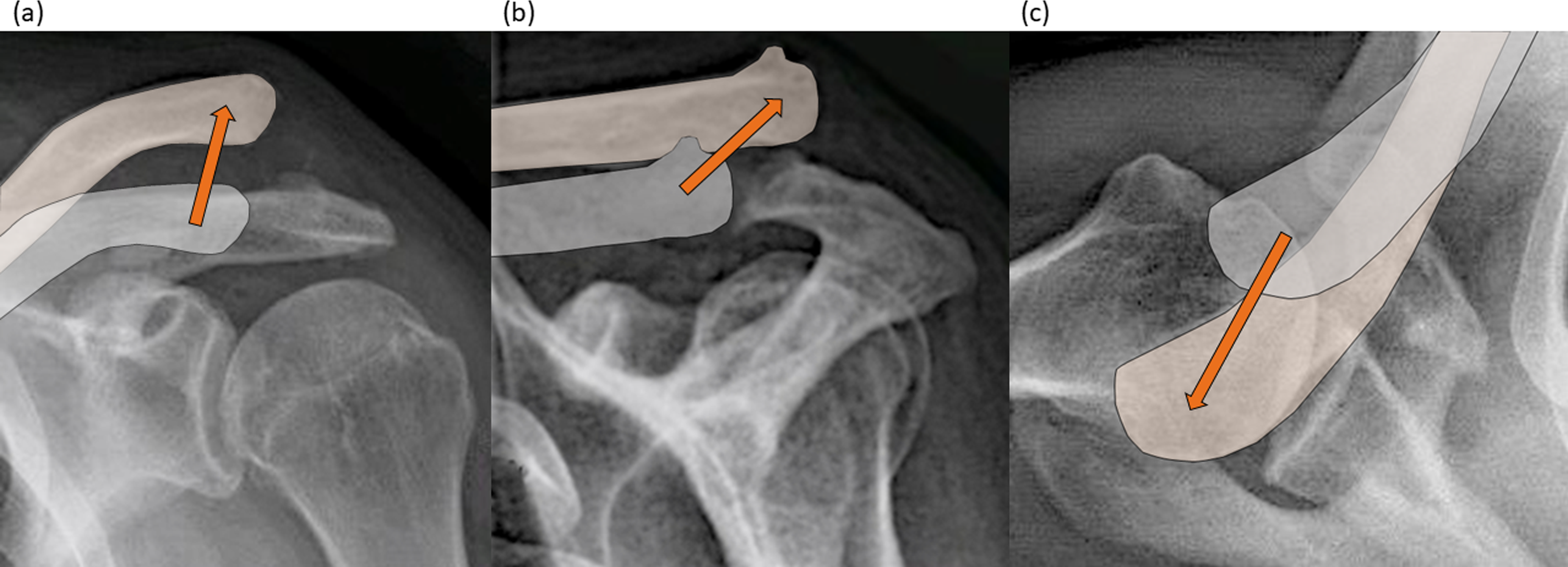
AC joint instability: presurgical radiographs, which show the natural position of the clavicle in relation to the acromion (grey) and the current displaced position of the clavicle (beige) in (a) craniocaudal, (b) anteroposterior and (c) axial view. Arrows show in which direction the clavicle is displaced in relation to the acromioclavicular joint.
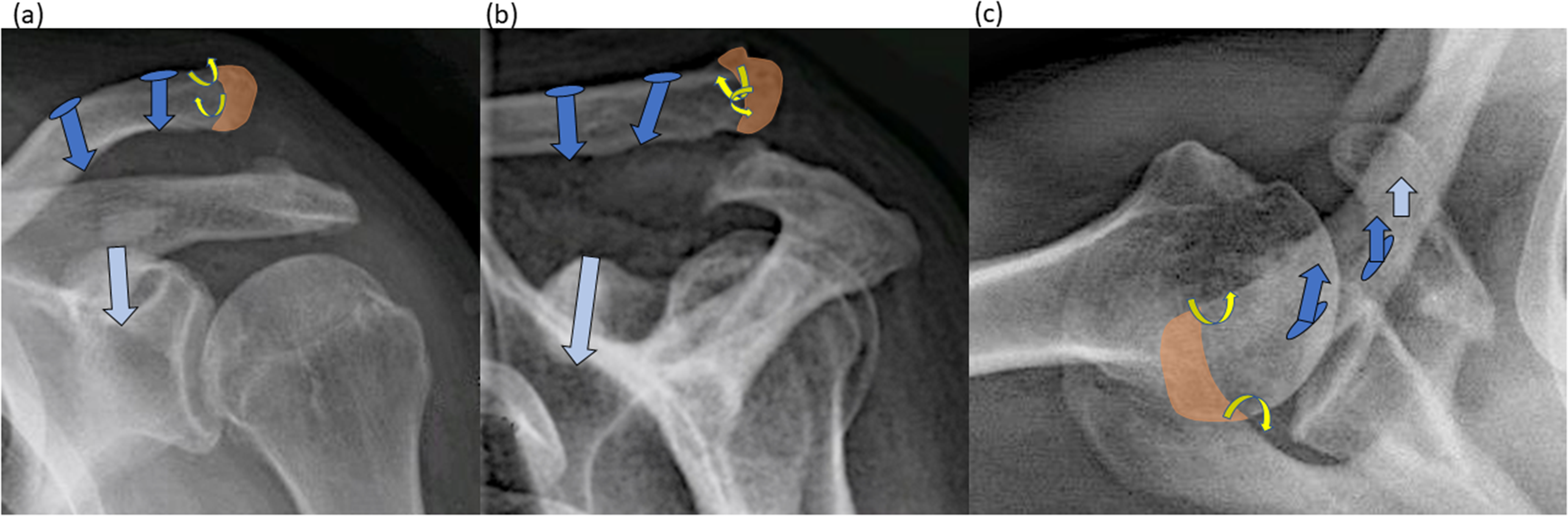
Bone measures: preparation of the drill holes (blue arrows clavicle, light blue arrow in the coracoid) and trans-osseous monocortical holes (yellow) of the distal clavicle in (a) craniocaudal, (b) anteroposterior and (c) axial view. (a)-(c): Orange part of the clavicle: distal clavicle resection approx. 5–7 mm and preparation of cortico-cancellous bone chips (for later filling of the drill holes); light blue arrow: drill hole 3.5 mm in diameter centrally at the coracoid base dorsal of M. pectoralis minor insertion and coracoacromial ligament; blue arrows with circle: 2 approx. 2 × 5mm slit-shaped bone tunnels adapted to the semitendinosus tendon from craniodorsal to caudal–ventral approx. 1.5 cm and 3.5 cm medial to distal clavicle for allograft ‘anatomic’ reconstruction of CC-ligaments; trans-osseous monocortical holes (yellow) of the distal clavicle (2 × 1.5 mm) for later trans-osseous AC joint capsular fixation.
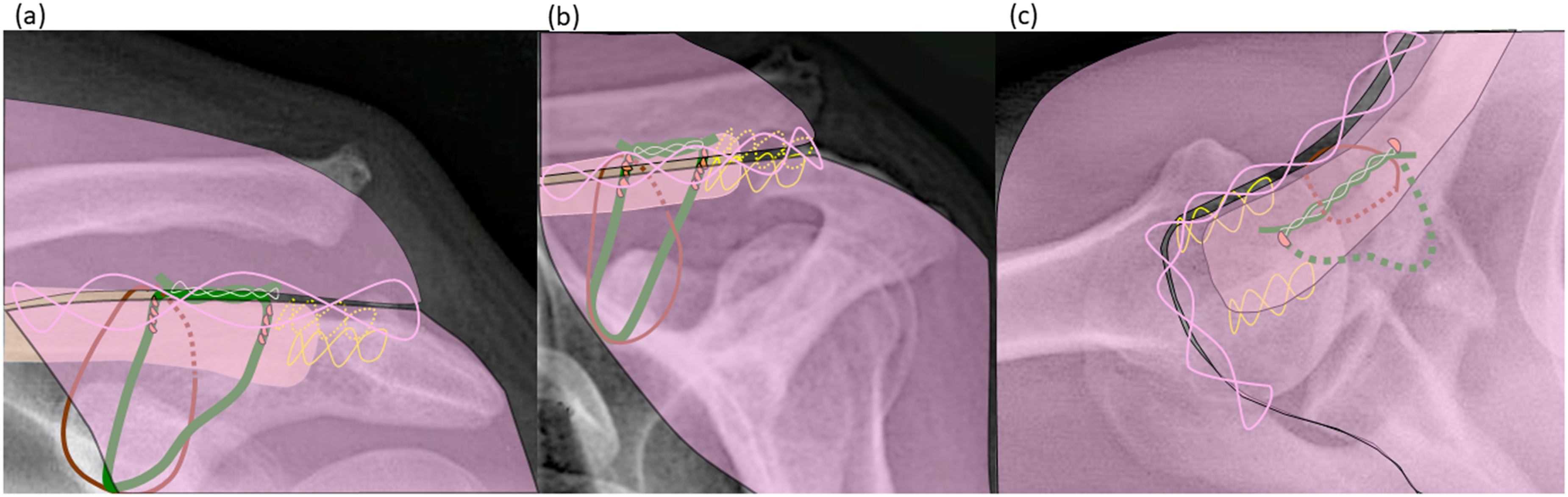
Resection of 5–7 mm of the distal clavicle is performed (Figure 2) in order to shorten the bone and to avoid potential secondary arthritis. Additionally, it is performed to obtain bone chips for impaction bone grafting for additional ligament stabilization in the bone tunnels (coracoid and clavicle). For better tendon-to-bone healing, three bone tunnels are prepared to pass the semitendinosus allograft through the bone. Two bone tunnels at the lateral portion of the clavicle close to the anatomical insertion points of CC-ligaments are prepared (Figure 2) and one bone tunnel at the coracoid base (clear blue, Figure 2). Finally, to achieve anatomical CC-ligament reconstruction, an approximately 25-cm long semitendinosus-allograft (green) is folded in half and passed trans-osseus through the bone tunnel at the coracoid base, posteriorly from the pectoralis minor tendon and coracoacromial ligament (Figure 3). The equally long ends of the graft are then superiorly oriented posteriorly from the deltoid muscle and then passed through the clavicular bone tunnels (Figure 3). In addition, a protection suture (Mersilene® band) for the allograft is placed (brown, Figure 3) as described by others.7,12,20,21 This protection suture avoids the elongation of the biological allograft in the early phase after surgery until the allograft is remodelled. Therefore, a 4-mm Mersilene® (brown, Ethicon, Norderstedt, Germany) suture band is passed behind the conjoint tendon under the coracoid tip and then passed around the clavicle in the middle of the two bone tunnels (Figure 3). Clavicle reduction (red arrow, Figure 4) is performed and then the protection suture (brown) is tensioned and fixed with a slight overcorrection in the vertical and horizontal orientation (Figure 4). The graft (green) is tensioned and the prepared bone chips (orange drops, Figure 4) are impacted in the clavicle bone tunnels for press-fit-fixation of the semitendinosus allograft. Using a tendon passer, the approximately 4 cm free ST double bundle tendon allograft is interlaced and then sutured to one another (Figure 4). The initially prepared trans-osseus non-resorbable sutures in the distal clavicle are now passed through the scared AC-joint capsule ventrally and dorsally, so that the joint capsule can be attached tightly to the already stabilized clavicle. This gives additional horizontal stability. Finally, the trapezius-deltoid fascia is closed over the clavicle and the graft (Figure 5). This leads to much better healing and integration due to the blood supply of the adjacent deltoid and trapezius muscle and provides additional vertical and horizontal stability. 29
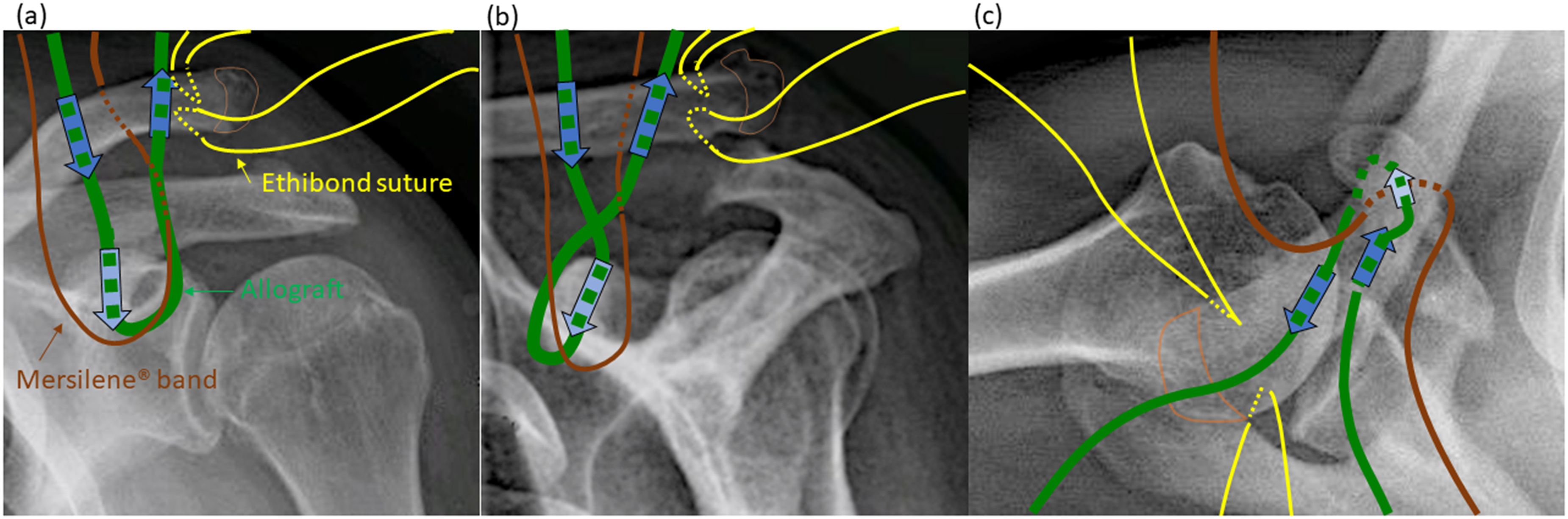
Preliminary laying of the semitendinosus allograft, the Mersilene® band and the ethibond sutures: preparation of the allograft, band and sutures at the coracoid base and in the coracoclavicular interval as well as at the distal clavicle in (a) craniocaudal, (b) anteroposterior and (c) axial view: (a)-(c): semitendinosus allograft (green): passage through coracoid bone tunnel and passage through the clavicle bone tunnels; Mersilene® band (brown): passage around coracoid base and proximally subdeltoidal anterior and posterior to the clavicle; ethibond sutures (yellow): preparation of dorsal and ventral ‘scarred AC joint capsule’ with positioning of two ethibond sutures; orange lined half round shape: part of the clavicle resected for cortico-cancellous bone chips generation.
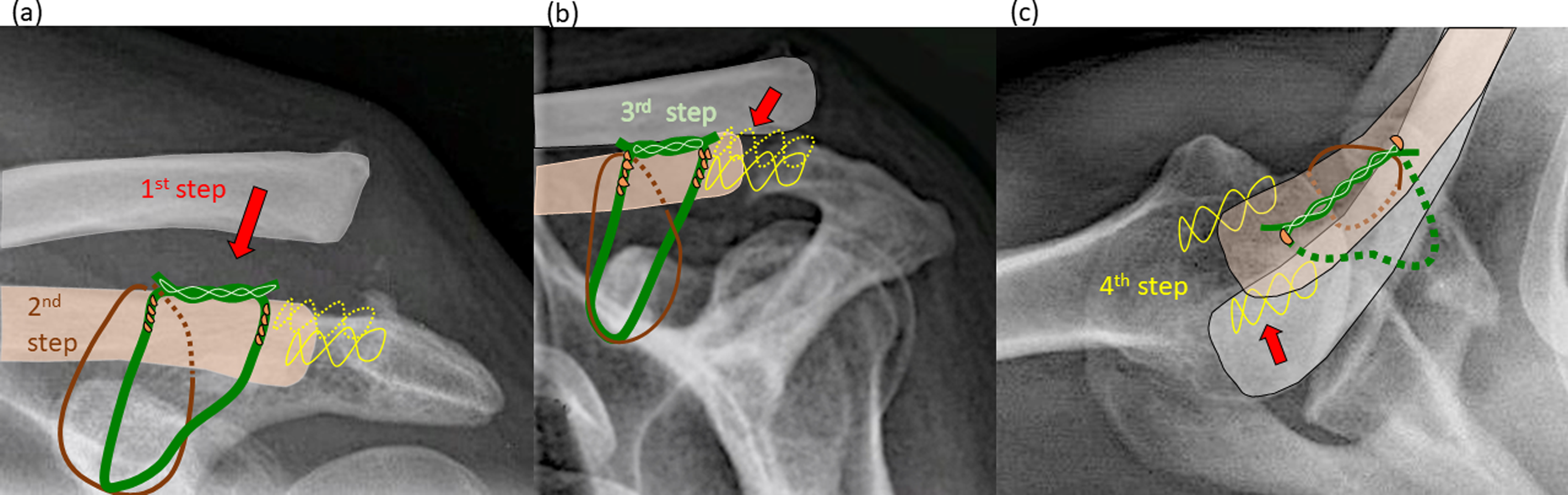
Tying the allograft and the threads: repositioning (red arrow) of the clavicle in (a) craniocaudal, (b) anteroposterior and (c) axial view: (a)-(c): first step: reduction (red arrow) of AC joint (craniocaudal and anterosuperior) into normal position (beige bone color); red arrows: direction of repositioning; second step: tying the Mersilene®-band (brown loop) (positioning of the knob dorsal from the clavicle); third step: tightening of semitendinosus allograft (green loop) and fixation using a tendon interlacing stich (clear green) with Vicryl Nr. 1; Forth step: Interlacing Ethibond sutures (yellow) with trans-osseous refixation of the neo-capsule of the AC joint for additional ventral and dorsal stabilization. Orange drops: cortico-cancellous bone chips harvested from the clavicle (Figure 2).
Supplementary soft tissue measure, fascia closure: trapezoid-deltoid fascia (pink) suture in (a) craniocaudal, (b) anteroposterior and (c) axial view: (a)-(c): continuous adaptation suture (clear pink) of the trapezoid-deltoid fascia (pink).
Post-surgery treatment
In Germany, this surgery is done as an in-patient procedure and on average patients remained in the hospital for 3.7 days. The operated shoulder/arm is immobilized with a Medi-arm-fix ® (Medi GmbH & Co.KG, Bayreuth, Germany) bandage for two weeks, day and night and for a further two weeks only at night. In week 3 and 4, an arm-carrying strap was allowed during the day. The movement was restricted to only lifting the arm to face level for six weeks. Starting from the 7th week, free mobilization was scheduled and after nine weeks strength development occurs. The remaining craniocaudal dislocation, horizontal stability and pain after surgery was evaluated and the remaining Rockwood classification post-surgery was recorded. Loss of correction was recorded and is dependent on the shaft size of the patient. Half a shaft width can be between 3 and 6 mm, which refer to a good result. Post-surgery stability was classified due to shaft width, with very good (<3 mm), good (3–6 mm), acceptable (6–9 mm) and failed (>9 mm). Elongation of the graft was measured using MRI technology, and elongations over 3 mm were considered a failed reconstruction. Return to work/sport was recorded as a measure of acromioclavicular joint stability under physical work.
Calculations and statistics
Values are given as mean ± SD, with range, or median values and are calculated with GraphPad Prism for Mac OSX (version 7.0e, GraphPad Software Inc., San Diego, CA, USA). In this retrospective observational study, there is only one patient group. To measure the parameters: abduction, extension, adduction, flexion internal and external rotation, the Neutral-0-method 33 was used. To calculate statistical differences for different time points (the routine visits post-surgery) and for the comparison of the time of surgery with and without associated injuries, non-parametric Mann–Whitney U tests were performed for two-group comparisons due to the non-Gaussian distribution of the values. Kruskal–Wallis tests were performed for the comparison of three or more groups combined with Dunn's multiple comparisons test. There are no missing data. A p-value < 0.05 was defined as significant.
Results
Patient data
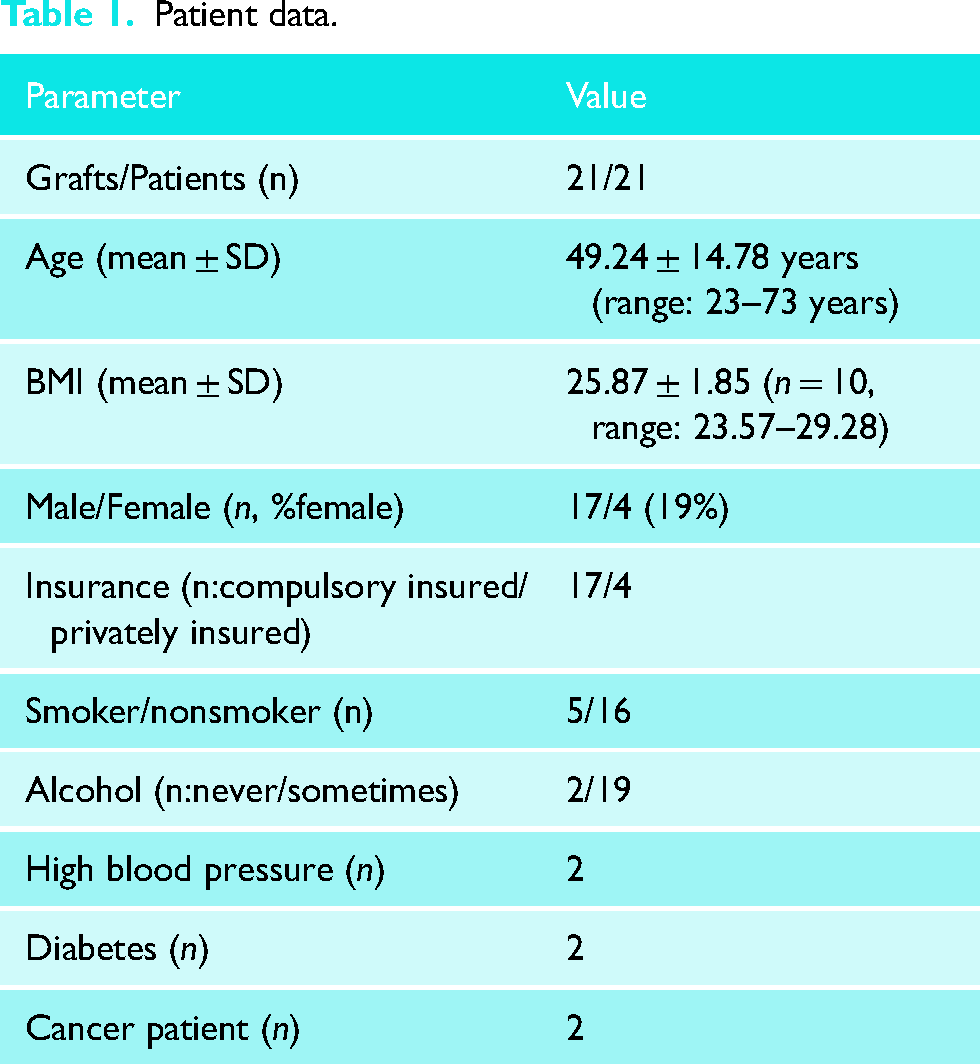
Due to the retrospective nature of the study, a control group was not available. Twenty-one patients were treated with 21 tendon allografts (Table 1). One patient was excluded due to acute surgical treatment even though the patient was treated with the same procedure; 21 patients were sub-acute or chronic. More than half of the chronic patients were revisions and for the remaining patients the diagnosis took longer than a week, thus they were grouped into sub-acute. Mean age, body mass index and co-morbidities are presented in Table 1. Non-related drug treatment, including anticoagulants, was recorded for 30% of the patients, while 70% did not take any medication before surgery. Patients with chronic pain were not part of the patient cohort. Male patients were the majority in this cohort (81%).
Patient data.
Clinical data
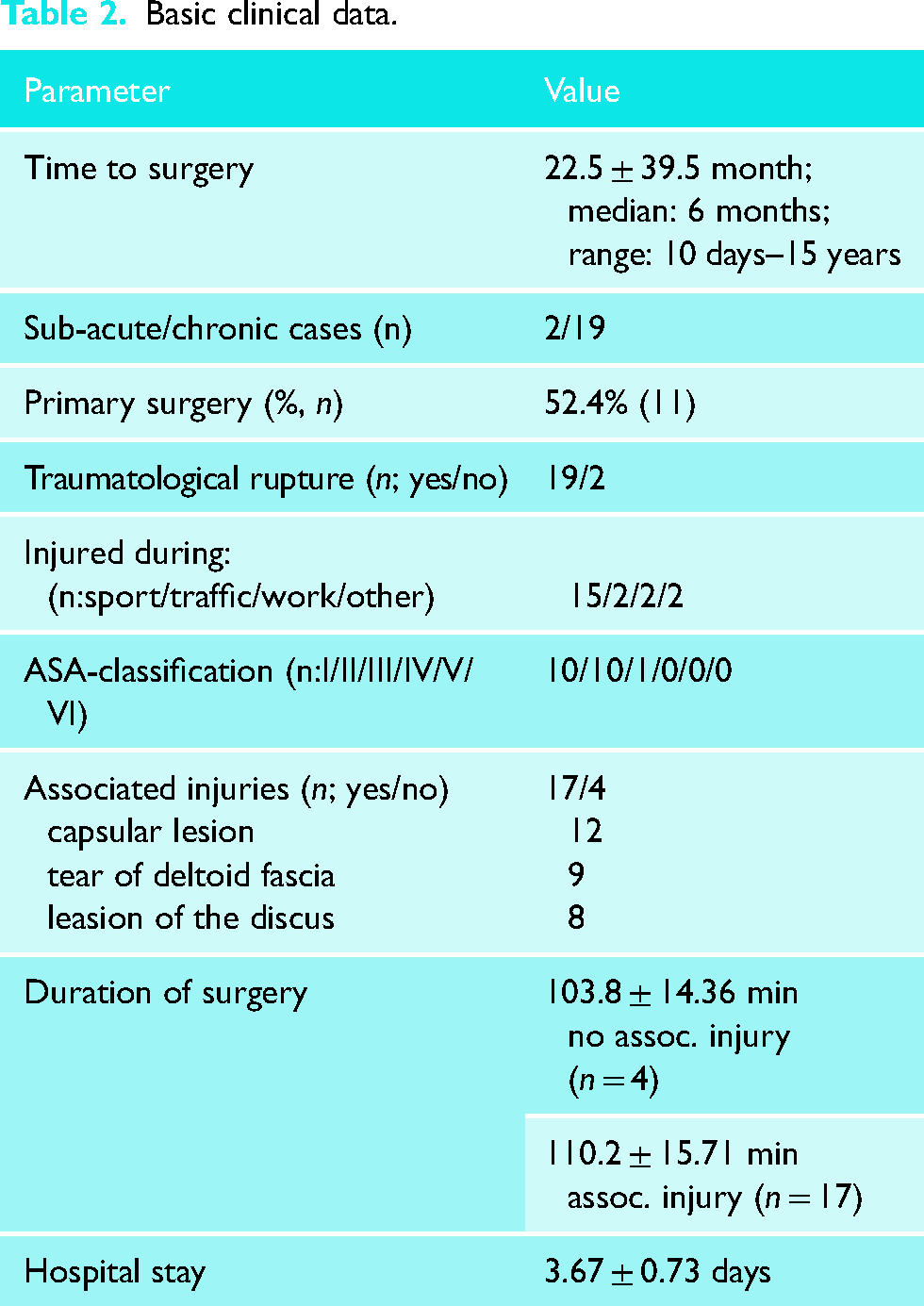
The average time between injury and surgery was 22 months (median 6 months) with a range of 10 days to 15 years (Table 2). Only sub-acute and chronic cases were included. Primary reconstruction was performed in 52% of the patients while 48% had at least 1 previous surgery on the same shoulder at another clinic (Table 2). The right shoulder was involved in 43% of the patients. In the present analysis, 90.5% of the ruptures that preceded the described surgery with the allograft were caused by trauma. In two patients, the reason for surgery was due to remaining symptoms of earlier operations or chronic insufficiencies. Out of the 21 patients, 9.5% were injured in traffic, 9.5% were at work and 71.5% of the patient cohort were injured during sports. Patients classified as ASA (American Society of Anesthesiologists, physical status classification System) I accounted for 47.6% of patients, 47.6% as ASA II and 4.8% as ASA III. Pre-surgery clinical examination, ultrasound and MRI diagnostic, was performed in all patients for detailed diagnostics and to exclude associated relevant glenohumeral lesions. Associated injuries such as impingement syndrome, partial rotator cuff tear and typical for AC joint injuries: rupture of AC-joint capsule, discus lesion and rupture of the trapezio-deltoidale fascia were recorded in 81% of the patients. One patient had a previously known functional impingement syndrome. In accordance with the patient, it was decided not to treat it simultaneously. The presence or absence of associated injuries led to a similar duration of surgery (Table 2). All patients received anti-coagulation therapy for two days after surgery and rehabilitation treatment, mainly comprising of isometric and free muscle mobilization.
Basic clinical data.
Scores and return to work/sport
The Literature is controversial when deciding if Rockwood III should be operated. In our patient, series 2 symptomatic (pain and instability) Rockwood III were operated. There is no controversy in the literature regarding that Rockwood IV (n = 14) and Rockwood V (n = 5) have to be treated with surgery, thus presenting the majority of the described patients. Partial weight load was allowed after a mean of 49 days ± 0 days (seven weeks) and full weight load after a mean of 120 days ± 0 days (four months). After surgery, only two patients (Table 3) had slight instabilities (half shaft width, less than 6 mm loss of correction), which were partly due to none-compliance of the patient to the advice of the surgeon. The use of MRI showed only slight elongation (less than 3 mm) and graft continuity was proved. Graft rupture and elongation >3 mm would be the criteria for failure. For the remaining patients, normal AC-joint position was radiologically recorded in craniocaudal and anterior-posterior direction with less than 3 mm (1/4) shaft width, at last follow up (at least 12 months after surgery, Figure 6). Pain levels during rest and heavy workload act as a good indicator for the healing process. The pain level was classified as severe, moderate, light pain, very light or no pain. At the last follow-up, only one patient experienced very light pain during rest. Three patients experienced light pain and two very light pain during heavy work or overhead work (Table 3). No patient reported moderate or severe pain. Information regarding the profession and the work model (e.g., full-time/part-time) was available before and after surgery (Table 3). After surgery, the distribution was the same as before except that, the single unemployed patient returned to full-time work. The average time taken for patients to return to part-time and full-time work was 3.0 months and 4.7 months, respectively (Table 3). The two professional athletes returned to their previous level of sport nine months after surgery.
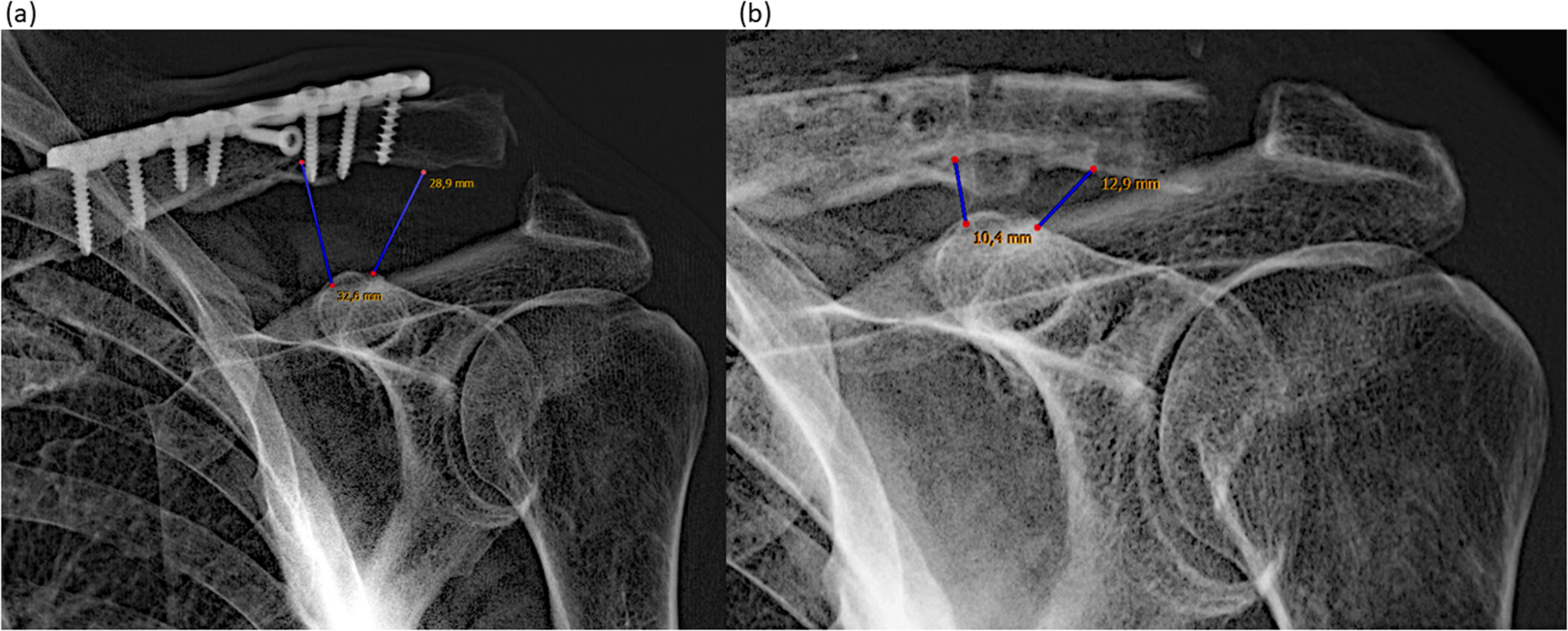
(a) X-ray showing the chronic AC-joint instability with a distance of 32.6 and 28.9 mm; (b) same patient after AC-joint stabilization with semitendinosus allograft and described surgical technique with a distance of 10.4 and 12.9 mm.
Pre- and post-surgery values.
Neutral-0-Method 33
After surgery, the movement of the shoulder was restricted for 42 days. Abduction to that of a healthy shoulder was obtained after 183 days and averaged to 173.3° (Figure 7A). After 79 days, adduction and extension were in the healthy range with 67.5° and 67.0°, respectively (Figure 7), flexion reached normal degrees after 183 days with 176.7° (Figure 7B). External and internal rotation in the neutral position as a healthy shoulder was recorded after 183 days with 74.3° and 87.6°, respectively (Figure 8A). In a 90° abduction position, it was recorded with 79.3° and 77.6°, respectively, after the same time period (Figure 8B).
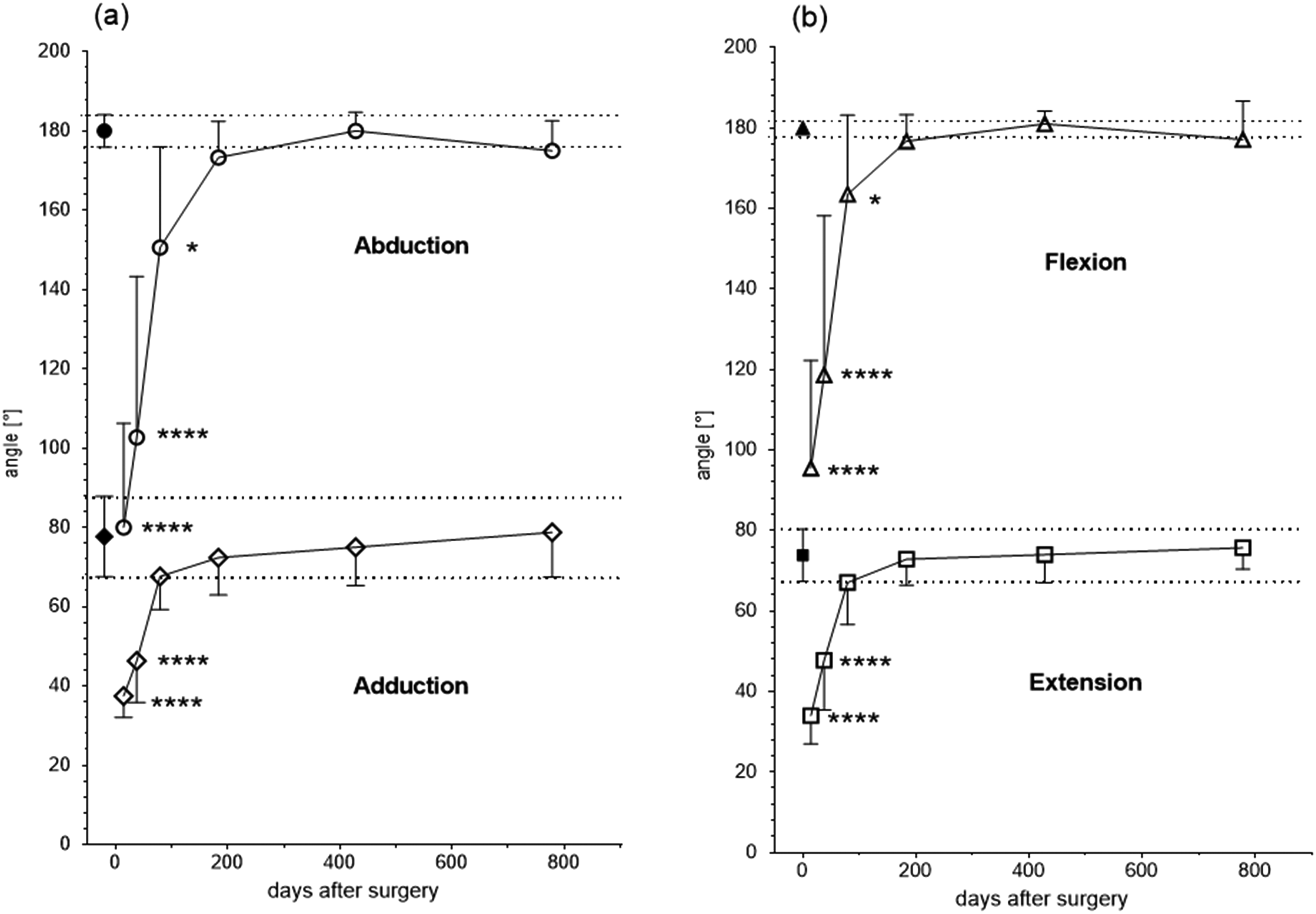
Neutral-0-method; closed symbols: healthy shoulders (a) abduction (open circles) and adduction (open diamond); (b) flexion (open squares) and extension (open triangles) for abduction and adduction 14/38/79/183/428/778 days after surgery, n = 10/22/17/21/10/7, *p < 0.05, ****p < 0.0001.
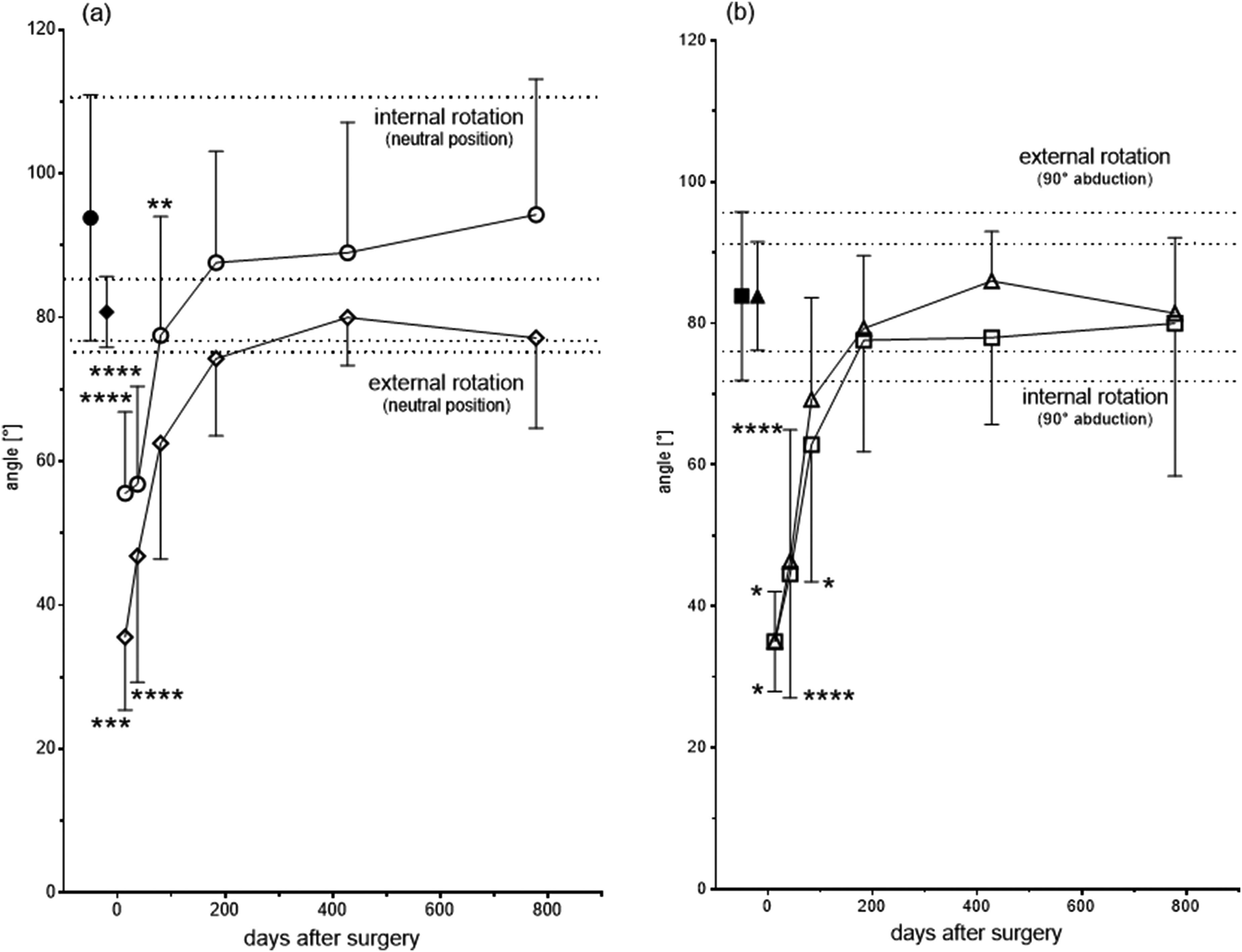
Neutral-0-method: closed symbols: healthy shoulders; (a) internal (open circle) and external (open diamond) rotation in neutral position after 14/42/83/183/428/778 days after surgery, n = 9/23/16/21/10/7, respectively, (b) external (open triangle) and internal (open square) rotation in 90° abduction position after 13/42/83/183/428/778 days after surgery, n = 2/10/14/21/10/7; *p < 0.05, **p < 0.01 ***p < 0.001, ****p < 0.0001.
Follow up and survival data
The mean follow-up was 33 months (981.3 ± 406.5 days) with a range of 12.8 months (391 days) to 5.6 years (2037 days) (Table 3). Patients had at least three follow ups. A follow-up of more than two years was recorded for 90.5% of the patients. Due to the rural area, the first author is practicing in, patients return to the doctor for other orthopaedic health issues. At these appointments, the performance of the shoulder was checked. Thus, later causes of loss of reduction or failures would have been detected. Directly after surgery, there were no complications. Three weeks to six months after surgery, 13.6% of patients (three grafts) described complications. Two patients were suspected of subcutaneous infections, without proof of bacteria presence or reaction to intracutaneous skin suture material (no association with the graft). They were successfully treated by skin/scar care with additional oral antibiotics (sulbactam–ampicillin 750 mg every 8 h) for 10 days. One patient was diagnosed with a temporary nervous suprascapularis lesion. All these complications were resolved without additional surgery. The overall graft survival rate was 100% (Table 3).
Graft data
Overall, 21 grafts were used, and all of them were semitendinosus tendons (<26 cm). The average donor age was 52.7 years (range 21–64 years), and the folded diameter was 7.24 mm ± 0.95 mm (range 5.5–9.5 mm).
Discussion
The most important finding of this study is that chemically sterilized tendon allografts used for primary and revision surgery achieved similar results with respect to re-rupture and complication rate as reported in the literature. A significant improvement in shoulder AC joint stability and a low (9%) loss of reduction were observed. The novelty of this reconstruction is that it is an anatomical reconstruction with chemically sterilized allografts, and it is nearly implant free. There was no re-rupture in the treated patient cohort. The first author, who did all the surgery, practices in a small city and would be notified when a re-rupture occurred after the follow-up for this treatment was finished. Anatomical CC-ligament reconstruction with chemically sterilized ST-allograft combined with periarticular procedures provides several potential advantages over non-anatomical techniques. This includes better replication of the native CC-ligaments strength and stiffness, increased joint stability, decreased subluxation and superior clinical outcomes scores. 1 Using allografts instead of autografts avoids donor site morbidity and provides a bigger selection of available grafts. Additionally, the sterilization of allografts with methods such as gamma irradiation has shown increased failure rates compared to non-irradiated grafts. 25 Thus, using chemically sterilized allografts is an attractive alternative to irradiated grafts.
Biomechanical studies also demonstrated, that free graft CC-ligament reconstruction more closely recreates native anterior–posterior and superior–inferior translational stability of the native joint. 34
The use of semitendinosus allograft for anatomical reconstruction of CC-ligaments in chronic AC-joint dislocation provides stability similar to that provided by the intact ligaments.13,32,35 The presented data show that sterilized semitendinosus allograft used for anatomical AC-joint stabilization is equivalent to the use of other allografts.1,2,13,17,29,30
The use of free tendon grafts (ST) together with non-biological support is widely used for better healing and remodelling times.7,12,20,22 An artificial band is used to avoid elongation in the first weeks after surgery, but cannot be used alone, because high re-rupture rates are reported with artificial grafts alone.36,37 Additionally to the high re-rupture rate, there is poor biological integration of the artificial graft in bone tunnels and articular cavity. 38 Yeranosian et al. 22 described the benefit of a non-biological support of the allograft in reducing creep and graft elongation, which can occur, even after preconditioning the allograft. The technique described in this study, which uses chemically sterilized (non-irradiated) allograft tendon (ST), shows that anatomical reconstruction of the AC joint can be performed with this kind of graft successfully. In our study, only two patients (9.5%) had a loss of reduction over 3 mm (less than 6 mm) at the last follow-up (12 months at least after surgery) but still showed a markedly improved stability. These patients had recurrent chronic instability; several previously failed surgeries and decreased healing capacity, additionally to low compliance and a too early return to strength exercises. The described craniocaudal AC-joint reduction and stability after surgery was comparable to results previously described.11,15 A mean loss of reduction with 4.1 ± 3.9 mm was described by Cerciello et al., 11 and Pill et al. described loss of reduction in 21% of the patients. 23 Choi et al. 39 described that the elongation of the autograft was the main reason for reoperation and in 47% of the patients a loss of reduction was recorded when a semitendinosus autograft was used. 39 Loss of reduction was found to be significantly higher with autografts (24.5%) in comparison to allografts (9.8%). 23 The observed percentage of instability is below the range of reported observations (12–41%).20,40,41 This is in line with the results described here. The high stability rate may be partly attributed to the fact that all associated injuries, such as the capsule and discus lesions and fascial tears, were addressed during surgery.
In our cohort, the operated shoulder recovered to a normal range of motion. Abduction was the same as in the healthy shoulder after 183 days with 173.3°, and extension was normal after 183 days with 177° (176°–179° and 177°–179°, respectively, as confirmed by others).9,35,42 External rotation was better in our described patient cohort with 74° after 183 days, which was confirmed by Nicholas et al. (73°), 35 compared to other studies, (63°) 42 and (66°) 9 after a two-year follow up. The mean follow-up of patients was 33 months with a range of 12–68 months, similar to others (26–49 months).10,11,15,17,18,22,40,43
Complications after AC-joint stabilization vary and may be unique to the implant and fixation method used during the index procedure. 3 Here, complications resolved without surgery and were as observed by others (8.5–40%).3,7,9,11,17,23,27,43,44 Moatshe et al. 44 described that free graft reconstruction provided the highest subjective scores and fewest complications, whereas using the hook plate resulted in high complication rates (26.3%) and an additional operation to remove the hardware.
The re-rupture rate in the current patient cohort was 0% (0 grafts), which was confirmed for allografts elsewhere.10,35 The Wang and Nicholas groups10,35 claim that the use of allogeneic tendon for the reconstruction of the coracoclavicular and acromioclavicular ligaments displays excellent outcomes as hardware removal is not required. Spencer et al. 45 reported different survival rates depending on the technique used with a low failure rate for the group where a combined allograft loop and a synthetic cortical button fixation were used. Martetschlager et al. 46 described an 86.2% and 83.2% successful surgery rate after 12 and 24 months, respectively, when tendon allografts were used. Failure rates using tendon allografts are reported to be 8%–18%.7,13,20,23
The chips used to fill the tunnel in the presented data collection, avoided the ‘windshield’ effect at the level of the clavicular tunnels as previously described. 29 The drilling holes may fail 3 but did not fail in any case for our reported data. This may be due to the impacted chips or due to the optimal position in regard to bone density. 15 Another reason could be due to the smaller diameter of the drill holes described herein and as described by others. 16
Return to sport usually occurs after six months13,14 but it generally requires nine months to a year for patients to regain peak strength.13,14 In our study, the two professional athletes returned to professional sports after nine months. Boileau et al. 47 described that nine of ten patients returned to their previous level of sport.
In the literature, sick leave after AC-joint stabilization is described between six weeks and six months.15,29,48,49 In the presented study, all patients returned to their previous work and one unemployed patient was able to start working again, similar to other studies.10,15,50 The described patient cohort returned to work after an average of 4.7 months, what is more than a month earlier than Parnes et al. described. 15 The economic value of the choice of surgical procedure is very high. Additionally, the average re-rupture rate in the literature is between 10% and 20%. In the described procedure, no re-rupture occurred. When reducing the re-rupture rate by 10% with an incidence in Germany of 3–4 per 100.000 inhabitants 51 and sick leave money of 68 Euro per day, 2.8 million € would be saved just in sick leave money in case of re-operation, excluding treatment costs.
In conclusion, chemically sterilized biological allografts are a reliable alternative to autografts for anatomic reconstruction of the CC-ligaments and stabilization of AC joint.11,13,28
Limitations
A potential limitation is the retrospective nature of the data collection. This is also the reason for the lack of scores and a control group. The treatment conducted here was the usual practice of the surgeon and not due to a study protocol. Due to only one acute patient being excluded, it is believed that no adverse impact is produced by the limitations mentioned. Therefore, further studies have to be performed to compare this method directly with others, but this could raise an ethical issue as this technique does not present any failures.
Conclusion
The data presented here reports that chemically sterilized allograft use, in combination with the described surgical technique, does not correlate with high re-rupture rates as described in the literature. 23 The stability of the AC joint can be restored anatomically and is reproducible and reliable when using chemically sterilized semitendinosus allograft tendons with an initial internal splint via a Mersilene® band. Overall, a low complication rate and no donor site morbidity are displayed.
Footnotes
Acknowledgements
The first author would like to thank Sylvia Müller for her enthusiasm to perform this analysis.
Author's Note
Gudrun H Borchert, Dr. Borchert Medical Information Management, Langen, Germany.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GB was employed and, NA and JB are employed by the DIZG. This paper is free of Institutional Review Board or Ethic Committee approval due to the letter of the Ethic Commission of the Bavarian ‘Landesärztekammer’ with sign 2020–1025.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.