
Abstract
Healthy eating is influenced by a myriad factors ranging from individual to societal. Healthcare organizations have recently adopted healthy eating policies to improve food environments; however, how such policies shape practice is still unknown. This qualitative study explores perspectives on continuous quality improvement (CQI) among healthcare staff and managers working in hospital foodservices post-implementation of a healthy eating policy aimed at improving food environments. We conducted semi-structured interviews with 12 foodservices staff at Nova Scotia Health. Participants varied in role (administrative, point-of-sale) and location (rural/urban). We analyzed findings using directed content analysis. Participants’ approach to quality revealed a range of definitions of healthy eating, from health promotion efforts directed towards individual behavior change management to a broader emphasis on supportive food environments. This research also highlighted the complexity of the healthcare food environment in which health promotion was being implemented, a ‘setting’ as per the ‘settings approach’ to health promotion, but also revealing a ‘setting within a setting’: food environments within healthcare environments. These nested environments are alternatively more business or healthcare service-centric, within the larger healthcare environment. Healthcare practitioners’ views on effective implementation of the policy also spanned many scales of healthy eating, informed by concepts within their core healthcare practice (dietetics: nutrients), the organization (historical nutrition contexts) and broader food culture (food trends and choice). This study has demonstrated that CQI for a healthier food environment within healthcare needs a broader focus to advance benchmarks for health promotion.
Keywords
Background
According to the 2019 Global Burden of Disease study, suboptimal diets contribute to 14.6% of male (4.47 million) and 13.5% of female deaths (3.09 million) worldwide (1), making nutrition a critical component of health promotion and disease prevention (2,3). The meaning of the term healthy eating, however, has expanded over the years, coinciding with our understanding of the factors influencing health.
Traditionally, healthcare practice viewed diet and many other health behaviors as a direct result of behavior and willpower (4). The adoption of the Ottawa Charter for Health Promotion shifted focus to upstream social and structural determinants of health (5). Recently, an emphasis on ‘food environments’ as settings where people purchase and access food has become central to health promotion efforts, where interventions altering the price, promotion and placement of food and beverages have been developed to influence diets (6).
Healthcare settings have been suggested as optimal organizations for health promotion since they are valued by the community, open to the public and well-resourced (7). They also have mission statements centered around healthy communities (8). Yet, incorporating upstream efforts to promote health within healthcare has been recognized as challenging (9). Recent literature suggests, for example, that the international Health Promoting Hospitals network comprises over 600 hospitals from 24 countries with some adoption of self-assessment tools and benchmarks, but what constitutes a model health promotion standard for healthcare and how to implement it effectively remains poorly understood (10). Researchers have observed that health promotion standards and benchmarks are lacking within healthcare to ascertain whether interventions or policies are efficacious (11).
In recent years, healthcare organizations have adopted health promotion policies that promote healthier eating environments (12). Scholars have also suggested strengthening health promotion’s ties to continuous quality improvement (CQI) to better incorporate health promotion into the fabric of healthcare (7). CQI is an iterative approach to practice that engages people at all levels of organizations (e.g. leadership, frontline) to try small tests of change, measure outcomes and adjust practices as needed (13). The purpose of this qualitative study is to explore perspectives on quality improvement among healthcare staff working in hospital foodservices and nutrition post-implementation of a healthy eating policy integrative of food environments. This research aimed to uncover how healthcare ideas around quality improvement may have informed implementing a healthy eating policy.
As a conceptual framework, we used the Inside out model by Golden et al. (14) (Figure 1). This model inverts the concentric circles of the traditional socio-ecological model (15) and places policies at the center to highlight the larger organizational conditions and individual and interpersonal factors contributing actively to policy ‘success’ and support (14). The following factors from the Inside out model were examined in this study: Communities, including decision-making groups, champions or advocates; Organizations, groups of people united around a common goal involved in policy monitoring and evaluation; Interpersonal connections, partnerships and coalitions between people; and Individuals, practitioners who exercise autonomy and can exert power.
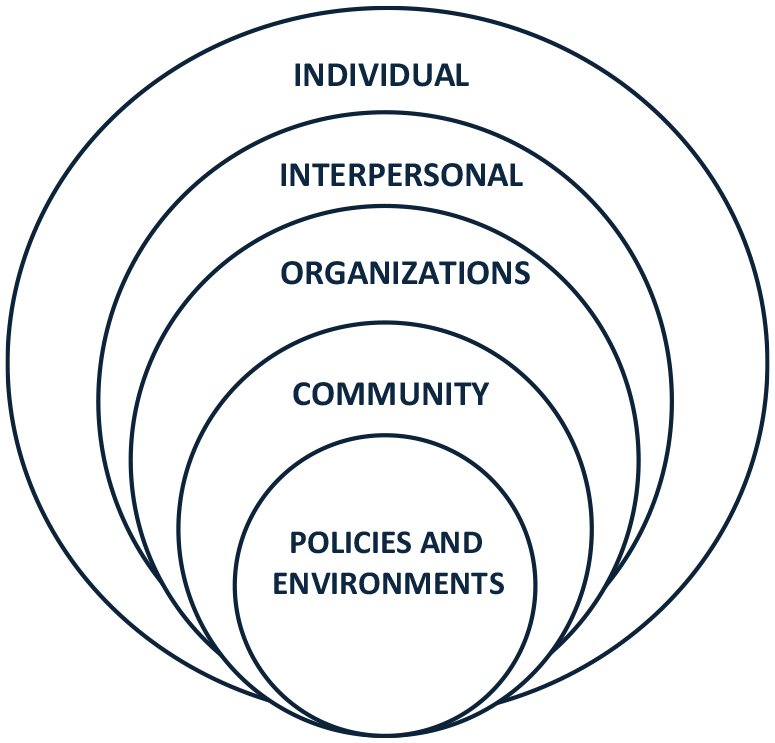
Inside out model derived from Golden et al. (14).
Methods
This paper used a qualitative study design to explore the perspectives of quality improvement. We interpreted our findings using the Inside out model.
Setting and policy context
This research was conducted in the Maritime Canadian city of Halifax, NS. In 2018, the provincial health authority, Nova Scotia Health (NSH), implemented an organizational Healthy Eating Policy. Novel to the policy, compared with earlier efforts, was its comprehensive emphasis on a whole-of-organization role in supporting healthy food environments. The policy presents ‘food as medicine’, with supportive food environments as essential to the patient’s overall treatment (16). The Healthy Eating Policy references a supplemental document, the Nova Scotia Food and Beverage Nutrient Criteria – a ‘traffic light’ style system with three tiers: maximum, moderate, and minimum nutrition (17) – but, unlike previous versions, covers a wide range of food provisioning across the entity of the organization (e.g. cafes, cafeterias), encompassing broad areas of affordability, access, advertising, fundraising and catering. Policy implementation is intended to be organization-wide but coordinated by Nutrition and Food Services and the Healthy Eating Policy Steering Committee (HEPSC) with representation from across diverse healthcare services. The policy has limited areas it does not cover (e.g. food brought from home by staff and intended for personal consumption).
Data collection
This qualitative study used a phenomenological approach, defined as the ‘design of inquiry from philosophy and psychology in which the researcher describes the lived experiences of individuals about a phenomenon as described by participants’ (18).
Participants were recruited using a snowball technique, starting from the HEPSC, to recruit a diverse group from a variety of organizational roles (e.g. point-of-sale to senior managerial) (19). In particular, this was done because CQI is a science that involves people at all levels of the organization; therefore, it was important to our understanding of CQI for health promotion to capture the views of various practitioners at different levels of the organization. Data collection occurred until data saturation was achieved (20).
Twelve participants were interviewed from Nutrition and Food Services. An initial interview guide was pilot-tested with a peer researcher for coherence and clarity. Interview questions focused on the daily activities of the participants (phenomenology) and were grouped by levels of the Inside out model (e.g. questions about individual practices or organizational practices). Participant inclusion criteria included participants who had been employed for at least three years; they varied in career stage, geographic region of service (n=3 urban; n=9 rural) and organizational roles: point-of-sale staff (n=3), supervisors (n=2), managers (n=3) and directors (n=4). Eleven participants identified as women and one participant identified as a man.
Interviews were conducted by the lead author LJK from January to June 2023 and lasted between 45 and 75 min. Consent forms were provided in advance in writing and then reviewed with participants to obtain written informed consent before completing the interviews. Interviews were audio recorded with consent. Interviews took place in person (n=1), over the phone (n=2) and virtually (n=9). A study by Johnson et al. (21) found no significant differences in data quality between interview approaches. This research received institutional ethics approval from Nova Scotia Health (REB# 1028236).
Data analysis
Interviews were transcribed verbatim by LJK and coded using NVivo Software (Release 1.7.1). Directed content analysis (DCA) was used to uncover the meaning of the data based on participants’ experiences (22). DCA uses deductive and inductive coding and theming processes, drawing from preexisting literature and participant lived experiences. An initial codebook was created based on theory and literature (deductive aspect). The codebook was revised after reading the transcripts and further examining emerging concepts (inductive aspect). Codes and emerging concepts were discussed through peer debriefing among the remaining authors and analyzed using the Inside out model as a conceptual framework (14). HW independently examined a random sample of 10% of interview transcripts to discuss the meaning and interpretation of the data. It is noteworthy for analysis considerations that LJK was an insider to the organization.
Findings
Reframing healthy eating in practice: ‘Do I care if it’s real bacon or turkey bacon’?
Across the participants, a range of perceptions and interpretations of quality health promotion practice as informed by the Healthy Eating Policy was detected. Participants spoke about how they aimed to address healthy eating in various ways and indicated what ideas within the policy resonated most closely with them in practice. Some participants described health promotion as the broadest environmental aspects of healthy eating, such as access and affordability, while others focused on specific nutrients. For example, one participant described healthy options as lower in sodium, sugar and processing. Another participant who was working as point-of-sale staff highlighted their actions towards reducing the availability of less healthy options:
Unhealthy food and pop like a lot of soda pops and like even some of the iced teas were so high in the sugar content. (Participant #11, point-of-sale)
Frequent examples of less healthy foods were mentioned, such as hot dogs, and pop and iced teas, as examples of drinks high in sugar. Less healthy options were also described as larger portion sizes, with one participant describing large, sugary muffins as bucket muffins when recalling a former food item offering from a third-party vendor before adopting the policy. In contrast, the same participant described healthy food options as ‘better’:
Muffins were massive … when the health authority took it over, they have a very standard smaller size made homemade not bucket muffins … with whole wheat flour like those things are much better than what we had before … (Participant #11, point-of-sale)
In contrast, some participants expressed concerns about being solely nutrient-focused, noting the dependency it could create for Nutrition and Food Services to interpret the policy on a case-by-case basis during implementation. One participant, a dietitian, presented an alternative approach, moving towards a holistic view of foods and beverages:
Our dietetics profession has moved toward… the holistic view of food and less about… the nutrient criteria… (Participant #3, manager)
Several participants commented that one vital component of implementing the policy was their new capacity to combine different approaches within the same intervention to promote health, such as altering prices for more nutrient-dense foods to make that same food more affordable. This goes further than offering a healthy option; it provides an affordable healthy option. Another participant mentioned affordability as essential to their definition of healthy eating.
There is a financial component, of course, making sure that we are not giving things away, but we are also looking at making sure that healthy choice is the easier choice. So, for example… our bottles of water are $1.00, whereas our cans of pop or diet pop … $2.79 … (Participant #9, director)
In other words, for several participants, healthy eating meant creating an environment that supports healthier options without abandoning a focus on nutrients. Noted one manager:
My values are measuring the healthy eating environment right now, not whether there’s real bacon or turkey bacon like offered as an option on the grill, but our measures are really based on nutrient criteria. (Participant #3, manager)
Participants identified past issues with previous healthy eating policies and expressed interest in improving its approach to healthy eating by focusing on food environments. The organization monitors aspects of the policy, such as the healthy eating audits completed by the team, aiming for no more than 30% of options to be minimum in nutrient criteria, suggesting that measuring progress and success of policy implementation within food environments remains at least to some practical extent nutrient-focused.
Not everything in our cafeterias reflects the Healthy Eating Policy in terms of maximum or moderate. Some items are obviously minimum, but we’re aiming for that 70–80%. (Participant #9, director)
Despite this, participants indicated their openness to benchmarks beyond nutrients. One participant discussed future benchmarks that might be used to measure food environments and commented on the difficulty of ‘benchmarking’ health promotion.
I think the benchmark of 70/30 is a starting place, and it certainly not our end all be all…, it’s only measuring availability of items like there is no benchmark for placement… product…. promotion…. (Participant #3, manager)
Participants expressed interest in developing future benchmarks for other aspects of the food environment (e.g. advertising) outlined in the policy.
Navigating culture: let them eat (birthday) cake
The Healthy Eating Policy focuses on building supportive environments. The Nova Scotia Health policy is particularly comprehensive relative to other Canadian examples in how it applies to food environments across the entire healthcare organization, from breakrooms to vending machines; however, it does not apply to food brought in for personal use by staff. Yet, in discussing this policy feature, participants explained that it also raised tensions in terms of their approach to policy implementation. Here, participants mentioned various events that shed light on how broader aspects of food culture had informed their interpretation within the policy and the nuanced exceptions to it: among them, birthday cake. The participant noted:
Food shouldn’t be used as a fundraising event… but there are times when, yes, it probably does need to be because we have traditions, so like birthday cake – that’s tradition. Are we going to interfere with anyone having a birthday cake? No. Right? (Participant #4, manager)
This response highlighted how certain traditions, like celebrating a coworker’s birthday, require adaptation in practice when the policy does not align. These tensions between traditions and nutrients speak to the intersection between healthcare organization culture and food culture more broadly. Another participant further expanded on this idea when discussing birthday cakes, which were presented in contrast to fruit.
I know there’s a healthy eating policy at this organization; it’s my coworker’s birthday, and I’m really wondering what I can do… I’m going to bring the cake, but I’m also going to bring fruit… that is such… a win… that says I’m creating an environment where I can make a healthy choice… (Participant #3, manager)
Here, the participant mentions existing interpersonal relationships between coworkers. Participants valued these connections and did not want the policy to alter interpersonal relationships:
My goal is to not be the restrictive team. My goal is to make the healthier option, the easier option, and the more accessible option. (Participant #9, director)
This was also evident regarding participants’ views on ‘policing’ the policy. Several participants tied the concept of enforcement during policy implementation to an action of ‘policing’. As one director-level participant noted,
We didn’t want to be the food police. (Participant #2, director).
‘Policing’ policy was discussed negatively by all participants and spoke to how participants believed that policing implies punishment for non-compliance. Like policing, monitoring people’s choices was also viewed negatively. One participant described this view using the example of a candy dish:
I’m not going around to people’s desks and removing their candy dishes (Participant #9, director).
On the other hand, monitoring was described positively when discussing the healthy eating audits used within the retail environment to monitor nutrient criteria within the foods sold.
Fish and chips ‘fills’ the cafeteria: the appeal of selling less healthy food
Our study revealed several paradoxes of principles guiding policy implementation for different sub-environments. Participants mentioned that offering certain options, like fish and chips, ‘fills the room’ of the cafeteria, optimizing revenue and appeasing customers, as one participant stated:
…how do we ensure that we’re successful not only with what the policy’s aiming to do but also… break[ing] even… how do you balance that when we typically know if you put fish and chips on, people are going to buy. Right? (Participant #4, director)
The focus of the Healthy Eating Policy is to create supportive food environments and to support healthier choices, but it is not to eliminate all less healthy choices. This was a policy design feature of interest to participants, who expressed the appeal of offering less healthier options and the issues of previous approaches of selling healthy foods only. Participants reflected on how they wanted healthcare retail spaces to be sought after by staff, patients and visitors.
Several participants described ‘food as medicine’ and contrasted conventional or policy-informed approaches to healthcare outpatient and inpatient environments. For instance, food may be provided in healthcare as a component of treatment for an inpatient, who turns customer if they or their families then shop in the cafeteria or vending machine. Participants in this study, therefore, saw hospital-based food retail spaces as part of a patient’s treatment pathway, noting inadequate nutrition as a risk factor for adverse health outcomes experienced by the larger population of Nova Scotia. One participant highlighted the paradox of retail services selling less healthy food options:
There is something terrible about our patients coming and getting a stent put in place for their heart disease and buying a doughnut on the way out. (Participant #1, dietitian)
Other participants went on to compare the selling of less healthy food to an earlier era when smoking was allowed in hospitals. As hospitals banned smoking within facilities, they became involved in a broader cultural shift denormalizing smoking in healthcare settings. It was evident that participants in the study had internalized the idea that building a health-promoting setting is an active process of challenging the status quo over time and reflecting on the organization’s mission and values. Participants were also keenly aware of the potential for pushback to health promotion activities. One participant stated,
…it might take time, sort of like when cigarettes… people grumbled because they couldn’t smoke in public… if you smoked in public, you would be ostracized… (Participant #11, point-of-sale).
This pushback required champions and coalitions to continue promoting the policy even when it was unpopular. This suggests that participants were committed to moving beyond a simplistic understanding of food towards a more complex one requiring a culture shift.
Discussion
This qualitative phenomenological study explored healthcare perspectives on CQI for health promotion in light of a healthy eating policy. Our findings showed a complex array of interpretations of healthy eating. Overall, our findings revealed various settings (e.g. physical and social) within healthcare, thus revealing the healthcare retail food environment as a setting within a setting.
Consistent with the Inside out model, health promotion policies within healthcare are situated within nested or multi-level organizational contexts. Research on CQI has suggested that policies targeting multiple contexts (macro, meso, micro) are needed to effectively support CQI (23). As Epping-Jordan et al. (23) explored in a study evaluating a CQI healthcare policy for chronic disease management, policies targeting multiple levels influenced patients, staff, organizations and macro-levels, such as accreditation, standards and monitoring. Similarly, the Healthy Eating Policy addressed multiple contexts for the hospital environment, including physical (e.g. promotions, price, placement) and social (e.g. staff lunchrooms, catering, fundraising), as well as individual (e.g. nutrient criteria). A review by Coles et al. (24) explored contextual factors influencing clinical CQI studies and identified that in addition to policies, CQI required strong leadership, strategic application and ‘point-of-sale’ or frontline engagement as possible mechanisms for effective CQI management across policy and organizational contexts. These findings and ours suggest synergies working across policy and organizational contexts, contributing to CQI advancement, meaning that policies work in a dynamic interrelationship with organizational support to evoke CQI practices (25).
Individuals influenced the implementation of the policy. Most of our participants identified as women, who tend to have higher-quality diets than men, which may have influenced their support and maintenance of policy (26). Additionally, participants with dietetics training approached food more holistically, which could be explained by the relationships between education, health literacy and nutrition (3). These findings align with the Inside out model, highlighting that individuals with control over resources may be more likely to influence policy change.
Monitoring centered around nutrient criteria. This is consistent with a healthy eating policy analysis reviewing Australian healthcare policies (13). This is also similar to CQI health promotion studies, including diet-related health education (27) and fruit and vegetable screening tools (28). However, there was interest among the practitioners in our study in monitoring other food environment benchmarks (e.g. price and promotion). Based on a CQI policy study by Gardner et al. (29) evaluating a chronic disease program in Indigenous community-based primary healthcare settings, such a shift in monitoring a range of practice outcomes and using this information to incorporate and adapt new practices, could reflect the organization’s absorptive capacity, the ability to absorb new knowledge and adjust practices based on data.
However, monitoring has been raised as a potentially unpopular aspect of CQI. During the study by Gardner et al. (29), monitoring was viewed by some health practitioners negatively as ‘policing’. Monitoring can be done in a way that maintains interpersonal relationships and allows for individual autonomy (e.g. birthday cake). CQI monitoring tools may need to be further studied for their acceptability, as Shaikh et al. (30) used iterative rounds of benchmarking to improve the adoption of primary care dietary tools. Benchmarks can allow for input across disciplines, meaning people across positions and power provide input. Additionally, CQI tools may need to be adapted. Bloomquist et al. (31) conducted a study of CQI addressing population health promotion in a regional health authority in Saskatchewan. They found that CQI tools to improve health promotion partnerships had ironically jeopardized these partnerships. Considering the monitoring impacts could improve CQI implementation and shift conversations from individual responsibilities toward power, inequities and environments (15).
The community discourses about healthy eating varied in our study. They unveiled tensions where culture had not entirely adapted to the policy (e.g. fish and chips). This could be explained by the lack of community readiness, as described by Agron et al. (32) and also identified by McIsaac et al. (33) in their study of school healthy eating policies, where the community response was described, at times, as obstructive. To increase acceptability, support from leaders across multiple levels of the organization is necessary (34).
Finally, resistance to health-promoting changes to environments could also reflect the nature of upstream health promotion and how it differs from traditional treatment and diagnostic programs within hospitals (10). For example, a CQI retail intervention by Tinney et al. (35) found that customers were hesitant about restrictions for sugar-sweetened beverages, and some expressed concerns about eliminating choice. Healthy eating discourses are still focused on downstream behavior change, and practitioners may need discretion as they implement the policy (e.g. candy dish). Practitioners who can exercise discretion and power within organizations are more engaged in CQI efforts (36).
Strengths and limitations
This qualitative study used data from semi-structured in-depth interviews, allowing for a rich analysis of perspectives. Data analysis used both iterative, as well as inductive and deductive coding, and a peer researcher independently examined a random sample of 10% of interview transcripts to discuss the meaning of the data.
LJK was an insider, allowing trust to be built throughout the interview process. Alternatively, this could have introduced bias. The codebook and themes were discussed extensively with the primary author’s committee, supervisor and research lab to mitigate bias. The snowballing technique may have introduced sampling bias (response bias). Participants’ responses may have reflected answers they believed the interviewer wanted to hear (social desirability bias).
A novel contribution of this study is that it used the Inside out model to further our understanding of policies and CQI within nested contexts. These findings add to the usefulness of this model to understand how policies are reinforced and maintained through reciprocal relations with individuals tasked with implementing them. However, as cited by other scholars, the Inside out model does not speak to political influences or other external factors (37), a potential limitation of its use in this study. Also, it has been suggested by scholars implementing the Inside out model that the levels of the model may overlap, which suggests our effort to distinguish between the effects at different levels may not have been accurate (e.g. interpersonal connections that foster collective action may have overlapped with individual resources and power) (38).
While our findings are not generalizable, they may be transferable to other healthcare organizations and other settings, such as schools and recreational centers, especially those operating under a healthy eating policy or guideline (e.g. Canada’s Food Guide). It is important to note that hospitals contain distinctive food environments compared to schools, with hospital sites operating during atypical hours and offering food to the general public.
Conclusion
Health promotion interventions within retail settings are complex, partly due to the shift in healthy eating from nutrients to environments, and require evidence and precision when altering aspects of the food environment, such as promotions, price, placement and convenience. The Healthy Eating Policy acted as a guide for decision-making within the healthcare food environment. Researchers and practitioners must consider a range of context-specific factors when implementing policies and interventions, which include food culture, traditions (e.g. birthday cake), past policies, and revenue. Organizations could also consider benchmarking environmental aspects of the food environment, in addition to nutrients, since the policy’s value in practice appears to have already exceeded what is currently monitored.
Footnotes
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LJK received support from a Nova Scotia Graduate Scholarship; JPL from the Killam Memorial Chairs program at Dalhousie University; HW, a Vanier Canada Graduate Scholarship; and CLM, the Canada Research Chairs program.