
Abstract
The pressing global health crises highlight the need for professional health promotion (HP). Debates on the professionalization of HP are still overlaid by questions regarding the conceptualization of HP, yet literature is scarce regarding this point. Therefore, this article aims to (a) provide an overview of the current state of professionalism in HP with a focus on the Swiss context, and (b) identify facilitators, gaps and barriers of professionalism in HP. By investigating these aims, we contribute to specifying the conceptualization of the specialist HP professional profile. To analyse professionalism in HP, we examined individual and institutional aspects of sociological theories on professions. We selected seven aspects as a theoretical foundation for the analysis: (1) specific knowledge base, (2) specific field of action, (3) specific education, (4) professional association, (5) specific competencies, (6) professional identity, and (7) professional practice. Analysing each aspect of professionalism in HP, we see a clear progression within the last decades internationally as well as in Switzerland. The development of a Core Competency Framework – the CompHP – is a milestone in the professionalization of HP. Some major gaps and barriers are identifiable, which should be proactively faced by the specialist HP professionals. To further flourish as HP professionals, a unity regarding contents and levels of education needs to be discussed. Therefore, an investment in professional identity formation of the specialist HP workforce is likely to promote their engagement, competencies and shared values, which are essential promotors of professionalism in HP.
Keywords
Introduction
Global health crises, including the emergence of expensive non-communicable diseases (NCDs), mental health issues and growing health disparities, highlight the inadequacy of relying solely on individual-focused curative and preventive healthcare services for achieving population health. This concern has been amplified in recent times, notably during the COVID-19 pandemic (1).
The concept of ‘new public health’, as defined in the Ottawa Charter, introduced health promotion (HP) as an approach to address population health more comprehensively. The HP movement aimed to expand the scope of traditional public health (PH), which often remains centred around biomedical perspectives and epidemiological research (2–4). The Ottawa Charter articulated new dimensions for HP, including (5):
• Emphasizing resources and promoting health-protective factors (salutogenesis) (6,7);
• Fostering community orientation and reducing hierarchical structures through participation and empowerment (8);
• Acknowledging the influence of social determinants of health within living, working, and ecological contexts (socio-ecological health model) and prioritizing health equity (9,10).
From these dimensions two key implementation strategies for HP emerged: first, the ‘health in all policies’ approach that calls for intersectoral collaboration (11) and recognizes that health is a product of various facets of life that necessitate the involvement of multiple professions and policy domains. Second, the settings approach, which favours a relational understanding of health where health behaviour intertwines with setting structures (12) and calls for integrative interventions that involve the communities within the settings in order to create healthy environments (13,14).
The intended paradigm shift of the Ottawa Charter led to several initiatives in health promotion promoting to extend traditional PH interventions. To mention just a few: 1) regular world conferences held by the World Health Organization (WHO) (15); 2) scientific journals, textbooks and specific working groups by the International Union for Health Education and Promotion (IUHPE) to promote capacity building 1 ; 3) diverse international networks to implement the settings approach, for example, healthy cities or health promoting schools; 4) educational programmes to build workforce capacity.
Despite these advancements, the ‘health in all policies’ and settings approaches have not fully reached their potential. Many HP interventions, both in practice and within the health sector, still overly concentrate on individual behaviour change and neglect the connection to structural elements (14,16). Moreover, the lack of clarity regarding roles and required competencies of HP professionals limits the effective implementation of the Ottawa Charter.
Improving clarification of competencies and roles necessitates recognizing that the procedural and systemic approach of HP calls for specific competencies, training and, ultimately, professional identity (17,18). Within this context, mainstream HP and specialist HP are differentiated as two ways to foster clarity of competencies and roles (17,19). Mainstream HP integrates HP values and methods into other professions to facilitate the ‘health in all policies’ approach. Specialist HP focuses on advancing HP practice and knowledge, leading the charge in realizing the Ottawa Charter’s ideas.
To advance professional HP practice, the specialist HP professional’s profile needs to be investigated and further developed. In today’s knowledge-driven society, demonstrating the quality and evidence of professional practice is essential for garnering support from donors, policymakers and society (20). A specialized HP workforce with a strong professional identity is crucial for advocating for the Ottawa Charter’s ideas and driving change in HP practice and policy (18,21). A recent review of empirical studies on the state and progression of research on profession, ethics, education/training, competencies and quality suggests a lack of research on HP professionalism, particularly in the German-speaking region (22).
Thereby, the varying conceptualization of HP influences the perceptions of professionalization. Some authors describe HP as a rising discipline (17,19), where a professional identity is being formed during studies (21). Other authors conclude that HP cannot be viewed as a profession, because: (a) HP professionals’ identity refers to their former educational background (23), (b) PH as a whole does not fulfil a societal function in the sense of Luhmann’s systems theory and can therefore not be seen as a profession (24), and (c) HP lacks the necessary institutional structures (25–27). Given these differences, a theoretical foundation for analysing and advancing professionalism within the field is needed.
The theoretical background of professionalism
As a relevant theoretical discourse, sociological theories on professions have addressed professionalism for nearly a century but did not come to a consensus regarding the understanding of a profession or the associated theories (28,29). Most commonly, professionalization is understood as the process of pursuing, developing and maintaining the unity of an occupational group (29). However, whereas older theories tended to focus on the institutional level of professionalization, newer theories emphasize the individual level, for example, professional practice, competencies or professional identity, which is summarized as professionalism (29,30).
In this article, the term ‘professionalism’ is defined as the current state of the professionalization process. We draw on Pfadenhauer and Sander (28), who synthesized theories on professions within the last century that focus on the institutional level. On the individual level we refer to Mieg (30), who introduced specific dimensions of professionalism. These combined theories yield seven aspects of professionalism, forming the foundation of our analysis (see Table 1).
Seven aspects of professionalism and their definition.

References: aPfadenhauer and Sander (28); bMieg (30).
Applying these seven aspects, this article aims to a) provide an overview of the current state of professionalism in HP with a focus on the Swiss context, and b) identify facilitators, gaps and barriers of professionalism in HP to inform further research and practice.
Method
For the analysis of the current state of professionalism in HP with a focus on the Swiss context, as well as the identification of facilitators, gaps and barriers, we draw on different data sources:
• International and German speaking literature on HP professionalization, which was identified in a scoping review conducted in 2020 (22);
• Additional literature identified beyond the scoping review’s inclusion criteria: before 2012 and after 2020 as well as theoretical papers, which were excluded in the scoping review;
• Reference books on the historical development of PH and HP in Switzerland (31–33).
For analytical reasons we describe each of the seven aspects of professionalism separately (see Table 1), while in practice all aspects are closely related. To validate the description of professionalism in HP in the Swiss context, feedback was obtained by experts in the field.
Analyses
(1) The specific knowledge base
The evolving knowledge base of HP is driven by dedicated journals (e.g. ‘Health Promotion International’, ‘Global Health Promotion’), reference handbooks (7,34–36) and national and global HP conferences. These conferences, such as the pioneering Ottawa Charter in 1986, the Bangkok Charter in 2005 and the recent Geneva Charter in 2021 (5,37,38), showcase current HP developments. Therefore, the conference charters are important to transfer recent theory into HP policy and practice and spread a shared vision of HP.
Whereas the conferences have a clear focus on HP, the research around HP diversifies across topics and professional viewpoints, making it challenging to distil a coherent and comprehensive knowledge base (39). Thereby, three knowledge dimensions for best practice in HP have been differentiated (40): values, context, and knowledge. Thus HP is supposed to reflect its values and principles, to analyse its contextual factors (sociocultural, political) and to delve into evidence-based and experiential HP knowledge from practice and policy (40–42).
Due to the intersectoral approach of HP, its theory base refers to health sciences (e.g. epidemiology), social sciences (e.g. psychology, sociology) and humanities (e.g. ethics) (36). The theoretical foundation spans individual health behaviour, communication, organizational change theories, community development and policy theories (43). In particular, HP’s relational perspective, linking health behaviour and structures, prompts exploration of dynamic structure–agency interplay (12). Research projects delve into these relationships (44,45,47,48). (See Supplementary material online for references 47–97.) Moreover, literature calls for a more fundamental integration of social theories of health inequalities, for example, posthuman theory into HP (18). The integration of these diverse perspectives contributes to cultivating a robust knowledge base of HP for advancing professional HP practice.
In Switzerland, HP knowledge is informed by international standards. A main pillar of the knowledge production of HP is the Swiss School of Public Health (SSPH+). It is an inter-university faculty assembling PH scholars from 12 Swiss universities and universities of applied sciences. Serving as the central coordinating entity, SSPH+ is dedicated to advancing postgraduate education and research in PH disciplines across Switzerland. HP knowledge production is focused among others by the Center of Salutogenesis at the University of Zurich, the Institute of Public Health at the ZHAW Zurich University of Applied Sciences, and the Département promotion de la santé et préventions at the University of Lausanne. Furthermore, also the broader PH science at the University of Basel, Geneva or Fribourg and all of the 12 affiliated universities at the SSPH+ are essential for the transition into HP theory and practice. Outside of the SSPH+, further research institutes are also relevant for the HP knowledge production, for instance, the Institute of Social and Preventive Medicine at the University of Berne, Institute for Social Work and Health at the University of Applied Sciences and Arts Northwestern Switzerland, or the Centre for Prevention and Health at the Lucerne University of Applied Sciences and Arts.
The specific HP knowledge is summarized and distributed by the national foundation ‘Health Promotion Switzerland’ and the Federal Office of Public Health. Moreover, these institutions disseminate project funds, conduct national and regional conferences, and publish reports and material to support quality assurance of HP practice in Switzerland, for example, on fundamental values of HP or specific themes (e.g. mental health). However, the project funds and conferences are more focused on transfering knowledge into practice than on the development of the scientific knowledge base of HP.
In addition to these facilitators, some gaps are seen in research regarding the professionalism of HP including a shared understanding of the specialist HP professional role. Further empirical investigations on HP’s specific methods and interventions and further outcome evaluation are necessary. Moreover, in Switzerland there is no scientific journal in HP which specifically focuses on these mentioned research gaps and therefore the development of the knowledge base of HP. This is also due to a lack of financing of HP research.
(2) The specific field of action
The socio-ecological and salutogenetic perspectives of HP, reflected in the ‘health in all policies’ and the settings approach, constitute an infinite field of action of HP. Both whole-of-society approaches are applicable to all political sectors at regional, national and international levels as well as in governmental and non-governmental institutions. Still the ‘health in all policies’ approach is not well established in many countries, even though some best practice examples exist in the UK, the Netherlands, Canada, et cetera (49). Comparatively, the settings approach grasps the specific fields of action of HP more easily. It includes change to the physical and social environment, to the organizational structure, administration and management within specific settings in co-creation with the citizens (50). Major developments are obvious within different settings, for example, healthy cities, health promoting schools, healthy workplaces, or health promoting hospitals (50). The WHO and others have developed specific guidelines and charters to spread the knowledge of the HP settings approach for different fields of action. Specialist HP professionals are responsible for developing policies and advocating for the establishment of the settings approach, potentially using labels like ‘Friendly Workspace’ or ‘Healthy Community’. Yet, the settings approach is underdeveloped and not implemented sufficiently. Also, it is often misunderstood as mere ‘HP within a setting’, leading to HP interventions without a systemic approach, focusing solely on behaviour change (14,51).
In Switzerland, the settings approach is mainly implemented in the school and workplace setting and facilitates the specification of the respective field of action of HP. Health promoting schools are fairly established and successful although a recent report on the activities of health promoting schools showed that more than 50% of interventions are not based on a settings approach but solely focus on individual behaviour change (51). Also, the development of HP at the workplace is successful in Switzerland. The foundation ‘Health Promotion Switzerland’ supports companies in creating supportive environments for their employees. The ‘Friendly Workspace Label’ tool was developed to implement healthy structures at the workplace. It has become well known and established (52,53) and the evaluation showed that the label helps to implement systematic HP at the workplace, especially if the label has been established over years and the companies get a re-certification (54).
Regarding other settings, however, the implementation of the WHO Healthy Cities Program was not successful and was only adopted in Geneva, and the network of health promoting hospitals was terminated due to a lack of interested hospitals (55).
(3) The specific education
The Ottawa Charter announced a paradigm shift within traditional PH, emphasizing capacity building to foster a skilled, motivated workforce. This entails training and educating the workforce (56,57) to cultivate specific competencies and form a professional identity. The Bologna Process, launched in 1999, opened the chance to establish a great variety of undergraduate and postgraduate programmes related to HP. At the international level, EU legislation facilitated initiatives like the European master’s in HP (EUMAHP: 1997–2004). Further developments of this project (PHETICE, CEPHAL, TEP) led to the successful implementation of educational programmes of HP at the international level (4,58,59). Today, doctoral degree programmes have also been established (60). At the national level academic programmes at various levels and continuing education options have emerged (19,61).
However, while HP, health sciences, health communication and health management all intend to educate for HP, the programme names and content differ substantially (24,61). Therefore, some initiatives sought standardized curricula structures and content through sharing international best practices (59,62,63). As a milestone in the professionalization of HP, a common competency framework for HP (Core Competencies for Health Promotion (CompHP)) was elaborated by the IUHPE (64). Based on the CompHP, the IUHPE established an accreditation framework to enhance professional capacity by ensuring transparent competencies in accredited HP professionals and accredited programmes (65). The ‘International Handbook of Teaching and Learning in Health Promotion’ (35) provides an overview of HP’s pedagogical landscape.
The training and education in PH in Switzerland started late in the early 1990s. Diverse undergraduate and graduate programmes in specific fields of PH have been established over the last years, for example, health sciences and epidemiology (66). Most of these programmes are affiliated with the SSPH+, the inter-university faculty for PH sciences, which is described under heading 1 of this analysis section. Professional education in HP started in the 1990s by establishing continuing education programmes mainly in departments of social work at applied sciences universities. The workload of these programmes varied between 10 and 60 European Credit Transfer System (ECTS) (i.e. around 300 to 1800 hours of workload). As a main facilitator for specific education in HP, the first undergraduate programme in HP and prevention started in 2016 at the ZHAW Zurich University of Applied Sciences in Winterthur (67). But there are still no consecutive master’s degrees in HP available in Switzerland and no programmes in the French or Italian speaking part of Switzerland.
(4) The professional association
The most important global professional association of HP is the IUHPE, which has taken action to further professionalize HP in collaboration with WHO and other global institutions since 1951 (19). This global representation supports capacity building of HP at regional or national levels, exemplified by initiatives like the CompHP, the accreditation system for HP practitioners, the organization of international conferences or the publication of scientific HP journals and text books (68,69).
At the national levels, professional associations are sparse, notably in Ireland and Australia (65,70). Yet many regions lack these crucial associations, despite their fundamental role in professionalizing HP and supporting capacity building (70,71).
As an alternative, some countries like Austria or Switzerland have established national HP foundations by law to strengthen and coordinate HP activities (21,72). These national institutions are also important to increase the visibility of the HP professionals (19,73). Despite their importance, a decrease of HP institutions on governmental levels (e.g. in the UK or Canada) has been observed (19,74). This underscores the importance of establishing national professional associations to advocate for the HP workforce’s interests.
In Switzerland, there is an active professional association for PH (Swiss Society for Public Health), with a HP working group which addresses aspects of professionalism in HP in Switzerland (75). Furthermore, diverse multi-professional associations dealing with HP and prevention do exist (e.g. addiction prevention, mental health, HP at the workplace setting, nutrition, physical activity, or health literacy). While they all aim to promote health in their specific fields of action and their specific topics, these institutions are not engaged in capacity building of HP or representing interests of the HP workforce.
Moreover, there are three governmental facilitators that promote the visibility and identity of the HP workforce. 1) The foundation ‘Health Promotion Switzerland’ was established in the late 1980s by the cantons and is now financed by every insured person in Switzerland with CHF4.80 per year. It is now a national representative of HP advocating for HP, initiating, financing, coordinating and evaluating programmes (53). Unfortunately, the strategic goal regarding capacity building of HP as well as regarding international collaborations has been cancelled within the last decade. 2) The national ‘Consortium of Cantonal Delegates of Health Promotion’ coordinates HP activities at the regional level in every canton. Since 2000, every canton has been represented in this consortium and has therefore an important role for the (political) visibility of HP in Switzerland (76). 3) The Federal Office of Public Health is the central institution for health policy and an important regulator for HP interventions in the areas of nutrition, physical activity, addiction prevention, and prevention of infectious diseases or NCDs. Taken together, these governmental institutions increase the visibility of HP in Switzerland, but do not assume leadership for capacity building of HP as a professional association might do. A specific professional association does not yet exist in Switzerland.
(5) The specific competencies
Since the Ottawa Charter in 1986 laid the foundation for a paradigm shift from traditional to new PH, it has become obvious that new competencies and methods, and new forms of collaboration are needed. Since then, diverse professions have entered the field of HP with different methods, values and research interests, which hinder an efficient implementation of HP’s core strategies. Therefore, specialist HP professionals emerged as a necessity to drive this transformative process. In response, the HP workforce made an effort to define and spread specific competencies, which are the basis for a shared understanding and standard as specialist HP professional (63,77). The IUHPE set a milestone by elaborating and publishing the CompHP, whose competencies are based on the Ottawa Charter (64). This framework sets common competencies for HP practice, education and training, encompassing the theoretical knowledge base, ethical values and nine standards with core competencies (64).
Efforts continue to globally implement and disseminate CompHP (69,71). Also, ongoing adaptations of the CompHP consider regional contexts, as seen in New Zealand (78). Besides serving as a standard for a shared understanding of common competencies in HP, the CompHP is used as a basis for an accreditation system for institutions and for individual HP practitioners, which is being promoted and slowly implemented around the globe (65).
In Switzerland, the need for standardized, specific competencies of HP professionals has not yet been discussed or studied in a broader context, although some initiatives and facilitators for specific competency development in HP can be identified. The HP working group within the Swiss Society of Public Health is advocating for the specific competencies of HP professionals (79). Furthermore, in November 2023, a symposium was conducted in Lausanne addressing the professional competencies of HP and prevention, which stimulated the discussion. A continuous debate of the professional competencies of HP practitioners is led by the Institute of Public Health at the ZHAW, who also implemented the undergraduate programme in HP and prevention in 2016. This programme is based on the CompHP (67) and got accredited by the IUHPE recently. Together, the Institute of Public Health at the ZHAW advocates for the professional competencies of HP practitioners within its network of practice partners and further regional and national cooperation partners, but continued efforts are needed to further advance HP competencies.
(6) The professional identity
Professional identity goes along with high engagement, commitment, quality awareness and competencies among professionals (80). It is a central construct of professionalism in HP, which is built on a personal and a social level. Literature asserts the existence of professional identity in the HP workforce (17,19,21,72,81), yet empirical studies on its formation are scarce (22).
Forming professional identity on the personal level involves embracing professional values and roles. This necessitates integrating HP’s knowledge base, ethical values and competency standards, such as those in the CompHP in one’s self-concept. Thereby, professional ethical values that are usually explicated in a shared code of conduct within the professional group are particularly important for professional identity formation in HP (20,82,83). A short list of central ethical values in HP is summarized in the CompHP: 1) belief in equity and social justice, 2) respect of individual autonomy, 3) collaborative and consultative ways of working (62). The ethical values in HP are subject to societal change as the discussion of planetary health as an increasing ethical value in HP exemplifies (20,84). Yet a commonly elaborated code of conduct does not exist in HP.
On the social level, professional identity is shaped by institutional structures, professional associations and societal recognition. In this regard, a professional association such as the IUHPE, the presence of national and governmental institutions of HP, specific laws on HP, specific journals, conferences, or research are important for professional identity formation of HP professionals. However, their implementation varies internationally (85).
In Switzerland, the situation regarding professional identity of the HP workforce is comparable to the international context, thus, the efforts in specific investigations and debates on this topic are rather sparse. Regarding the personal level of professional identity formation, again, the undergraduate programme in HP and prevention at the ZHAW is mentioned as a facilitator here. It aims to build capacity of the HP workforce with a specific professional identity of the graduates to further professionalize HP practice in Switzerland (86) and investigates factors that influence the professional identity formation of their students empirically (21). Regarding ethical values in HP, recent debates in Switzerland (87,88) indicate the importance of the reflection of ethical values within professional HP practice.
The situation in Switzerland regarding the social level of professional identity was mentioned in the previous sections. Of the national governmental institutions, the foundation ‘Health Promotion Switzerland’ organizes an annual national conference in HP and enables networking and a professional exchange of the HP professionals, which promotes professional identity formation. However, as barriers for professional identity formation on the social level in Switzerland, there is still a lack of 1) a legal basis for HP, 2) specific journals and 3) a professional association to promote visibility and capacity building of HP professionals.
(7) Professional practice
Professional practice stands out by dedication, engagement in the profession, the appreciation of quality assurance (89) and application of specific competencies (90). Evidence-based practice is crucial in HP (91,92), necessitating consistent models and tools for effective application, especially given the complexity within a socio-ecological and salutogenetic health framework. This poses a great challenge to structuring the implementation of HP practice and measuring the impact of interventions. Some models and tools already exist, which certainly need specifications and constant development for the use in HP. Such an established framework is the Public Health Action Cycle (PHAC). It serves as a model for conducting population-based interventions, as pursued by the ‘health in all policies’ and settings approaches. The PHAC was developed in 1988 in the US to lay out the governmental PH interventions and was adapted as a suitable model for health politics and quality assurance of HP interventions on regional, national and also international levels (93,94). The PHAC’s four phases – Assessment, Policy-development, Assurance and Evaluation – ensure transparent processes, and emphasize the continuing processual character of HP practice. Figure 1 explicates a simplified model of the professional practice of the specialist HP professionals within the community setting while adding the importance of critical reflection within HP practice.
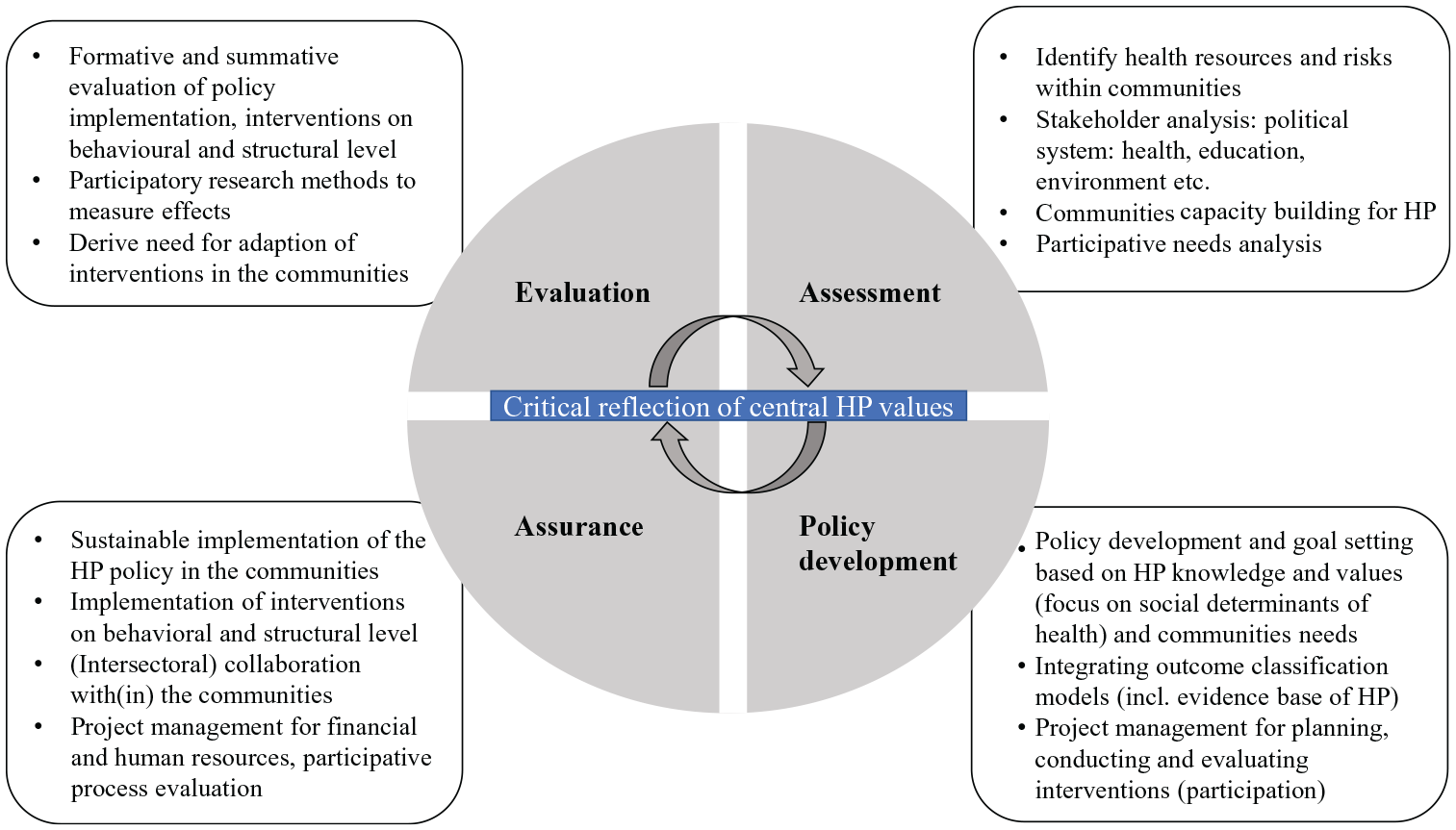
Shortened listing of the professional practice of health promotion (HP) at the community level structured with the Public Health Action Cycle.
From the PHAC, specific tasks and competencies for HP interventions and training contents can be derived, aligning with the CompHP (64). However, applying the PHAC necessitates specific tools such as ‘quint-essenz’ (95) or the ‘QATCHEPP’ (92), for quality assurance and measuring the intended effect. These models and tools support an evidence-based and reflective HP practice and facilitate the investigation of its effectiveness, which is fundamental to policymakers and the public.
In Switzerland, structures and institutions exist that promote and enable professional practice of the HP workforce by strengthening the knowledge base, especially the foundation ‘Health Promotion Switzerland’. Also, HP practice in the cantons is being further professionalized within the Consortium of Cantonal Delegates of HP (76). The funding structures of HP interventions in Switzerland mostly have set certain standards for quality assurance including an orientation on the PHAC. Therefore, the PHAC is well known and established in HP’s professional practice in Switzerland.
Additionally, in Switzerland some further tools were developed to facilitate quality assurance of HP practice, which have been promoted by the foundation ‘Health Promotion Switzerland’: 1) ‘quint-essenz’ (42), which is now administered as ‘www.good-practice.ch’ (95), 2) the Swiss Model for Outcome Classification in Health Promotion and Prevention (96) and 3) a guide for best practice in HP (41). These instruments are well-known and form the basis for long-term quality assurance of HP practice in Switzerland (41,42,96).
In Switzerland, the state of professional HP practice that is implemented cannot be fully evaluated owing to the incomplete availability of specific monitoring reports of HP interventions (the only exceptions are the funded projects by ‘Health Promotion Switzerland’ or voluntary project reports on www.good-practice.ch). Yet, research on HP’s professional practice, including the further development of specific tools and methods, has to be expanded.
Conclusion
Professionalism in HP is definitively progressing regarding the seven analysed aspects, which can be traced back to facilitators such as the strong support by the WHO or the CompHP development by the IUHPE. Even so, major gaps and barriers are seen in Switzerland and internationally, for example, in the lack of a) common standards for education in HP, b) professional associations and c) national legislation for HP. A competent workforce with a strong professional identity must proactively face these barriers and advance the development of the knowledge base and professional practice. To make better use of synergies, the growing HP workforce should collaborate and advocate for HP within professional associations at (inter)national levels. In conclusion, the specialist HP workforce must further promote and implement their standards regarding the analysed professionalism aspects, as only a well-equipped HP workforce with an effective, evidenced-based practice can fulfill its potential to contribute to solving the ongoing health crises in a sustainable way.
Supplemental Material
sj-docx-1-ped-10.1177_17579759241246777 – Supplemental material for A theoretical analysis of professionalism in health promotion with a focus on the Swiss context
Supplemental material, sj-docx-1-ped-10.1177_17579759241246777 for A theoretical analysis of professionalism in health promotion with a focus on the Swiss context by Verena Biehl, Brigitte Ruckstuhl and Frank Wieber in Global Health Promotion
Footnotes
Acknowledgements
We kindly wish to thank Andreas Pfister, Julia Dratva and Karin Nordström for their valuable feedback on the description of the professionalization of health promotion in Switzerland. Furthermore, we are very grateful to David Stamm for proofreading and editing the manuscript.
Author contribution
Each author made contributions to the conceptualization of the article. V.B. started the draft, while B.R. and F.W. constantly provided feedback and reviewed the draft. All authors approved the final version of the article before submission. To assure accuracy, the authors decided to engage further experts for critical feedback, who are mentioned in the Acknowledgements.
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The authors referred to the Committee on Publication Ethics’ International Standards for Authors (97). In accordance with the Declaration of Helsinki (2013), no consent was necessary from the ethics committee for this research. The scholarly paper is an analysis of professionalism in health promotion and no personalized data was used.
Supplementary material
References 47–97 are supplied as Supplementary material online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.