
Abstract
Sustainable development goals (SDGs) and public health are often considered as separate policy fields, whereas there is a considerable potential in better coordinating their objectives and measures. Using an analytical grid (S2D grid) linking SDGs and public health objectives and comprising 6 thematic issues and 56 categories, the research team conducted an assessment of health promotion programs in the city of Lausanne, Switzerland. Their objective was to determine whether SDGs and public health concerns can translate into complementary policy objectives, and what was the level of achievement of Lausanne in terms of implementation, intersectoral collaboration and avoidance of redundancy, regarding the vast array of measures potentially dealing with SDGs and health promotion. Results show that measures implemented by Lausanne deal with 80% of categories included in the S2D grid, with a high level of intersectorality and a low level of redundancy. These results also emphasize the fact that linkages between SDGs and health promotion go well beyond the SDG 3 dedicated to ‘good health and well-being’, and that the S2D grid could be used as a tool in favor of organizational change, promoting the collaboration between stakeholders often reluctant to engage in public health policies.
Introduction
During the 23rd World Conference on Health Promotion, which took place in April 2019 in New Zealand, a sub-plenary session was dedicated to ‘Implementing the Sustainable Development Goals at the Local Level: The Example of Francophone Healthy Cities’. Based on an analytical framework developed from a selection of sustainable development goals (SDGs), S2D grid, which was discussed during the sub-plenary session, this article aims to present and analyze the results of applying the S2D grid to the city of Lausanne, Switzerland. The objective is twofold: first, from a conceptual perspective, discussing how the apparent tension between the achievement of SDGs and health promotion policies can be addressed at the city level through the use of an adequate framework; second, from an empirical perspective, assessing the degree to which a municipality can implement measures in line with the SDGs’ targets and local health strategies, taking into account relevant target groups, promoting intersectorality and avoiding redundancy.
The Swiss health system
Switzerland is a federal state whose public health system is based on three different levels of competencies: communal (municipal), cantonal, and federal. The principle of subsidiarity implies that the vast majority of public health financing and provision, including health prevention and promotion, is a cantonal task. However, since the 1990s, and following legislative changes, a growing entanglement of competencies has progressively blurred the distinction between federal and cantonal levels (1). Furthermore, the health insurance system is largely privatized but regulated by the state, meaning for instance that the public/private mix changes between in- and outpatient care financing. In consequence, and from an institutional perspective, cities in Switzerland (communal level) do not usually play a key role in shaping public health policies.
Connecting sustainable development and health promotion
The idea of linking health promotion and sustainable development is not new and can be traced at least to the Ottawa Charter adopted in 1986 following the first International Conference on Health Promotion held by the World Health Organization (WHO). The document insists on a series of prerequisites for health, including peace, shelter, education, food, income, a stable ecosystem, sustainable resources, and social justice and equity, which all sound very similar to the SDGs (2). This call for a comprehensive approach to health promotion was continuously reaffirmed during the following international conferences (Adelaide in 1988, Sundsvall in 1991, Jakarta in 1997, etc.) (3) leading in 2010 to the Adelaide Statement on ‘Health in All Policies’ (HiAP), acknowledging the fact that health issues should be considered and dealt with according to an intersectoral approach, not confined to health ministers, and a multilevel governance, gathering national, regional, and local levels (4). More recently, the WHO has established a ‘New Urban Agenda’ and developed the concept of health in urban and territorial planning (UTP), in an attempt to explicitly link the HiAP approach with the SDG framework and emphasizing the role played by a broader array of actors, notably at the city level (5,6). Indeed, the local level, in the face of complex interrelated health issues, appears to address more easily ‘spatial and cognitive conditions’ necessary to successfully achieve a collaboration between several stakeholders (7).
In Switzerland, it is interesting to note that, in the field of environmental and sustainable development policies, the key player is the Confederation (federal state), not the cantons, leading to an even greater complexity in the design of policies linking health and sustainable development issues. This is notably illustrated by the case of the Swiss National Environmental Health Action Plan (NEHAP), a strategic plan aiming at implementing policies in the field of environmental health and developed in relation to the National Strategy of Sustainable Development (NSSD). The Swiss NEHAP was abandoned in 2007 partly due to the strong subsidiarity preventing the federal section in charge of the NEHAP from effectively collaborating with cantons (8). To this day, Switzerland remains without a NEHAP, an exception in Western Europe.
The relationship between SDGs, and more generally sustainable development policies, and health promotion has often been characterized by a tension between two antagonist views. On the one hand, health has generally been envisioned as a subcategory of the social dimension in many sustainable development representations (along with environmental and economic dimensions), notably within United Nations (UN) organizations (8,9). In that sense, the fact that SDG 3 specifically addresses health and well-being, ‘Ensure healthy lives and promote well-being for all at all ages’, comes as no surprise. The Swiss NSSD (2016–2019) retained this approach and dedicated one of its nine chapters to health, combining objectives for instance related to the burden of disease of non-communicable diseases, the provision of medical staff or the level of physical activity among the population, without any explicit overarching framework other than the reference to SDG 3 (10). On the other hand, and following systemic approaches to health, for instance inspired by the concept of environmental health, several scholars have acknowledged the necessity to use a multidimensional, cross-disciplinary, and cross-sectoral approach to correctly assess the intrinsic complexity of health determinants (11 –13). According to that perspective, connections between SDGs and health determinants are everywhere (14). In the same vein, it can be observed that the 11 qualities of healthy cities 1 are compatible with the 17 SDGs (15). Evidently, the added value of the SDG framework for public health policies lies in its institutional pervasiveness, most organizations and administrations, from the local to the international level, referring to it.
In summary, there are several factors that tend to explain the disconnect between sustainable development and public health policies. First, from an institutional perspective, levels of policymaking might simply not be aligned. This is typically the case in Switzerland with communal, cantonal, and federal levels overseeing different policy domains. Belgium is another example of such a discrepancy, health and environmental policies relying on different governance levels (respectively communities and regions) (16). Second, from an actors’ perspective, national ministers and local administrations can be reluctant to share their competencies or prerogatives, especially in the absence of strong incentives. Again, this has often been the case in Switzerland, between policy actors at the cantonal level (siloed approach), and between actors at the federal and cantonal levels (strong subsidiarity principle). Third, from a conceptual perspective, the disconnect between sustainable development and public health policies arises from the notion that sustainable development policies somehow encompass (environmental) health policies, thus contributing to the development of health policies limited in their scope and far from corresponding to their systemic nature.
Methodology
The epistemological approach followed here is largely pragmatic (17) and responds to stakeholders’ needs (health practitioners and decision-makers in municipalities) to have a practical instrument allowing them to take the SDGs into account, while implementing health promotion policies at the local level. It is therefore an ad hoc tool, tested iteratively in order to meet the expectations of those in the field. The research team first developed an analytical framework of health promotion measures, based on a grid designed by S2D, the Association Internationale pour la Santé et le Développement Durable (International Association for Health and Sustainable Development), which they then applied to Lausanne, a city of approximately 140,000 inhabitants located in the French-speaking area of Switzerland and notably known to host the International Olympic Committee. The parliament of the municipality is composed of 100 deputies representing six political parties, whereas the government, whose seven members are elected by the people, represents four political parties, with a strong left-wing majority (2016–2021). The city does not have any legal obligation to implement health promotion or sustainable development policies, nor does it receive any significant incentive from the cantonal or federal authorities to do so. It is therefore following the municipal political ambition that Lausanne has established itself as a pioneer in that field, serving as a role model for surrounding communes and cities across Switzerland. The analysis was conducted in 2018–2019 by the Institute of Global Health at the University of Geneva, following a mandate from the municipal authorities, and financially supported by the national foundation ‘Swiss Health Promotion’ with the aim of offering the city’s example to the ‘Union of Swiss Cities’, the main association in the country defending political interests of cities, notably at the federal level. The municipality’s objective was to produce an initial diagnosis of the city’s health promotion policies in relation to the SDGs, and to identify potential areas of improvement, given their focus on three main objectives: healthy diet, physical activity, and social cohesion. This focus reflected a political decision taken before any discussion was engaged with the University of Geneva and before considering the integration of health promotion and sustainable development policies.
Design of the S2D grid
The first step was to define which of the 169 SDG targets were relevant at the local level (municipality) and clearly related to health determinants (Table 1). An example of target not retained would be 2.b: ‘Correct and prevent trade restrictions and distortions in world agricultural markets, including through the parallel elimination of all forms of agricultural export subsidies and all export measures with equivalent effect, in accordance with the mandate of the Doha Development Round’. Indeed, its relationship to health determinants is not clear. Another example would be target 1.b: ‘Create sound policy frameworks at the national, regional and international levels, based on pro-poor and gender-sensitive development strategies, to support accelerated investment in poverty eradication actions’. This time, it is the relationship to a local level of implementation which is absent.
SDG targets related to health and relevant at the local level (represented by shaded cells).
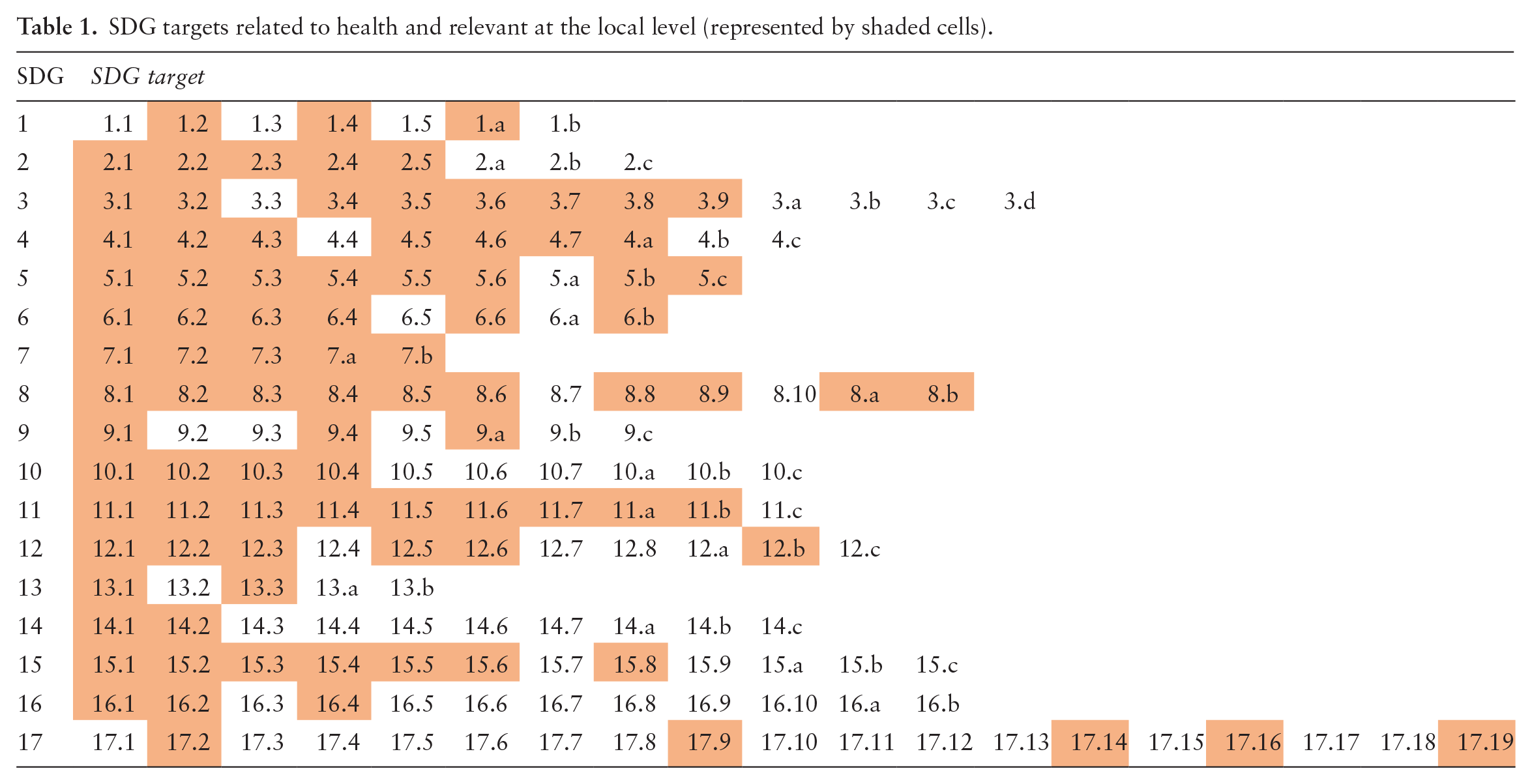
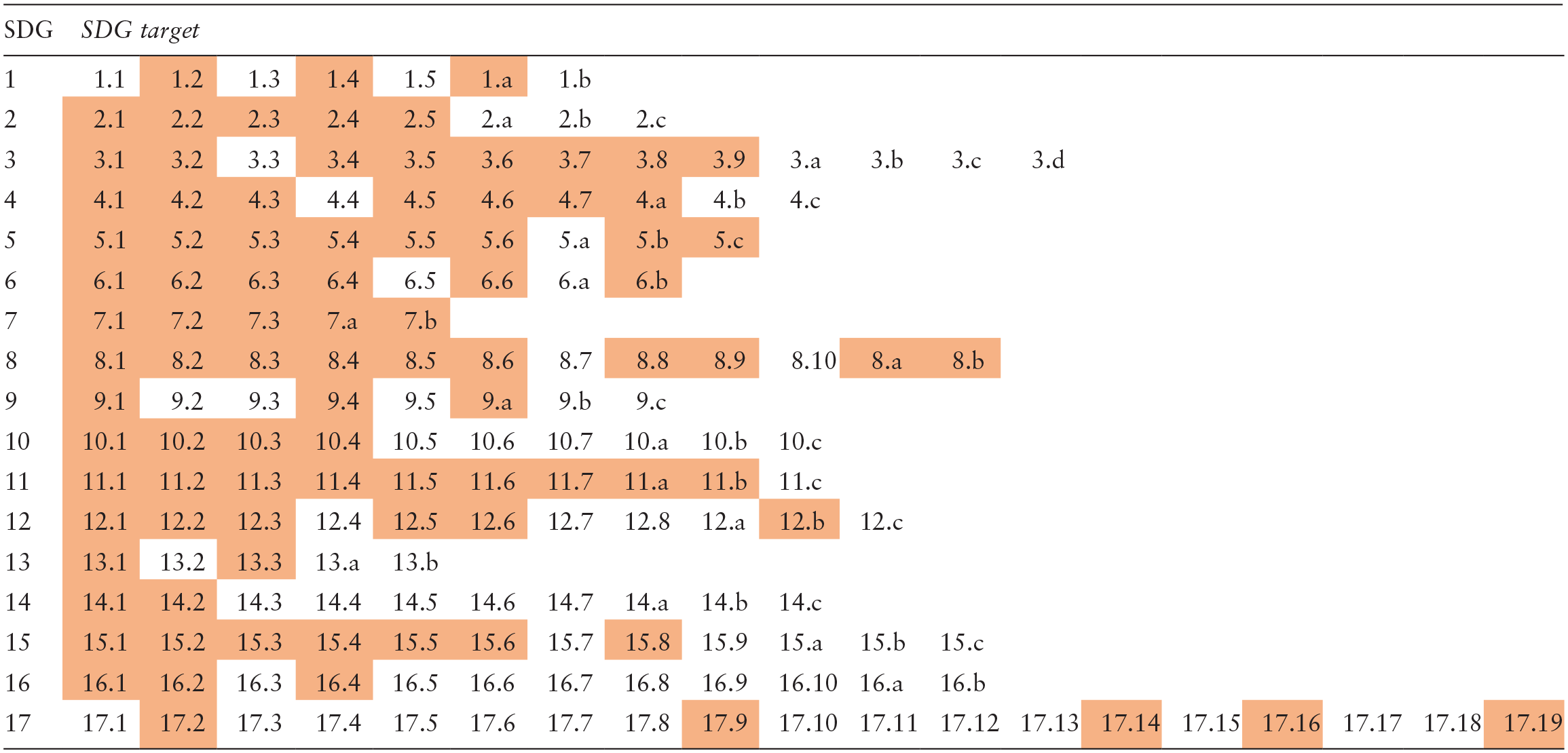
Second, these targets were then classified into 56 categories according to the 6 following thematic issues: (i) environment with 13 categories, (ii) production and economy with 13 categories, (iii) social cohesion and equity with 10 categories, (iv) prevention and promotion of individual health with 5 categories, (v) urban governance with 10 categories, and (vi) development aid and international cooperation with 5 categories. Urban noise (thematic issue 1) and local projects in social cohesion (thematic issue 3) were not part of the SDG framework and were added. The objective was to sort SDG targets in a more meaningful way, that is likely to correspond to concrete measures implemented at the local level. This was done following the grid created by the École Nationale Supérieure des Mines to analyze European Agendas 21 (18).
Application to the city of Lausanne
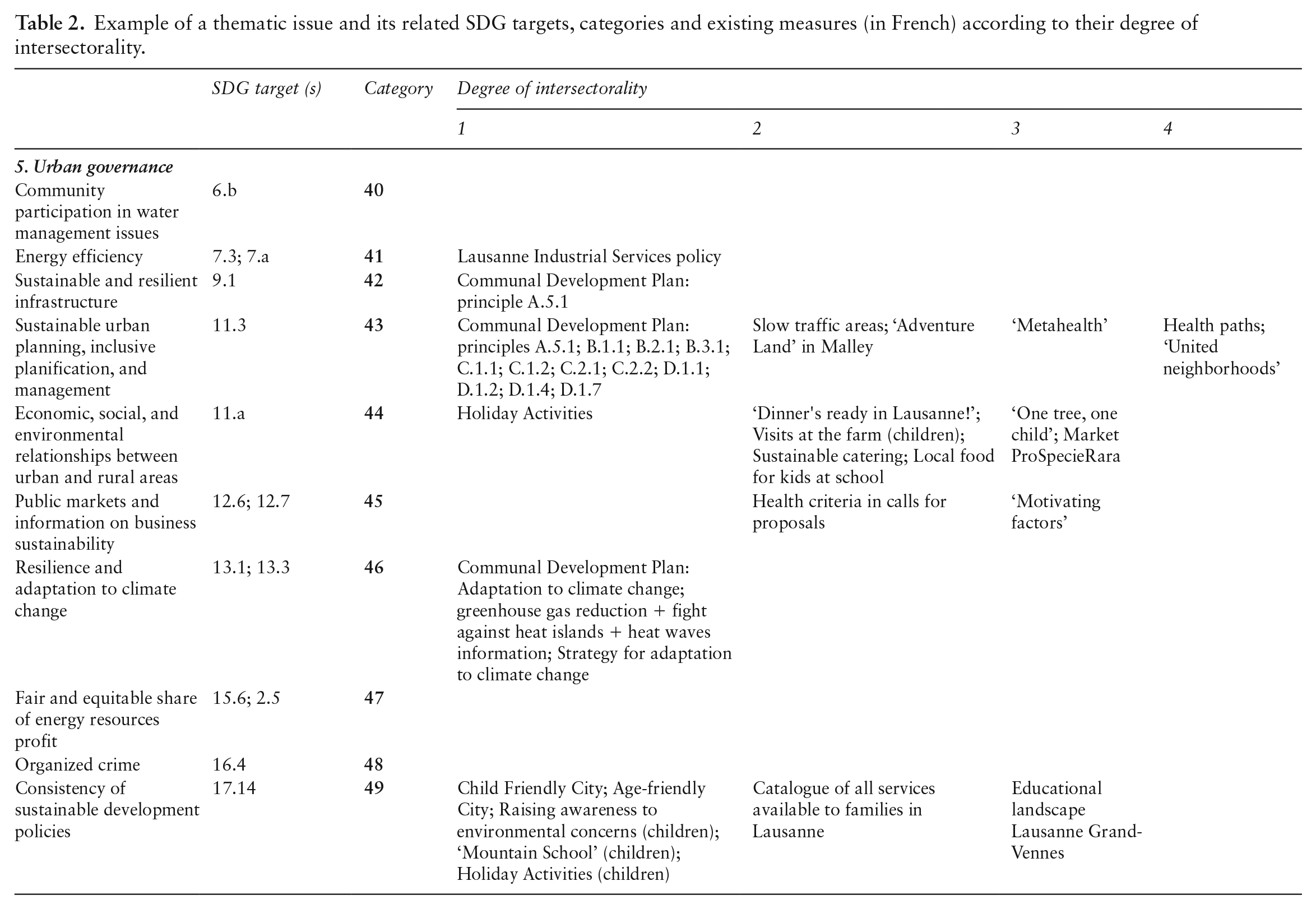
Third, data were collected from the three main health programs conducted at the city level in Lausanne. ‘Global Active City’, an international network aimed at promoting physical activity and tackling non-communicable disabilities and supported by the International Olympic Committee. ‘Commune en santé’ (Healthy municipalities), a Swiss network of French-speaking municipalities whose aim is notably to assess existing health promotion measures in six domains (municipality policies, leisure activities, family, school, occupational health, and public spaces) and identify corresponding needs. A successful process of assessment is awarded a label for a three-year period. ‘Healthy Cities’, a network established by the WHO and based on the concept of Health For All, on the Ottawa Charter, and on Agenda 21. Its aim is to promote a socioecological approach to health anchored at the local level and reward cities following a process of continuous improvement, rather than the achievement of specific targets. Approximately 1600 cities across the world are part of the network. Based on this collection, an exhaustive list of close to 250 health promotion measures was established, reflecting the content of the SDG targets mentioned previously. In addition, the following 10 target groups were considered: (i) feminine gender, (ii) vulnerable people (including migrants), (iii) poor people, (iv) disabled people, (v) pregnant women, (vi) infants, (vii) children, (viii) adolescents, (ix) young adults, and (x) the elderly. Finally, five degrees of intersectorality were also taken into account: (i) measure based on an integrated approach, (ii) measure based on a sectoral approach, (iii) temporary and sectoral measures, (iv) declaration of intent, and (v) not dealt with. Table 2 lists part of this process regarding the fifth thematic issue, ‘Urban governance’.
Example of a thematic issue and its related SDG targets, categories and existing measures (in French) according to their degree of intersectorality.
Analysis of results in Lausanne
A total of 92 SDG targets (approximately 54% of the 169 SDG targets) have been identified as potentially corresponding to measures taking place at the local level and related to health promotion. It is interesting to note that, as far back as the 1990s, the vast majority of measures proposed in the framework of Agenda 21 were considered to be best implemented at the local level, hence the considerable success, at least in terms of strategy production, of Local Agenda 21 (19). However, not all SDGs are equally represented. Whereas SDGs 5 (‘Achieve gender equality and empower all women and girls’), 7 (‘Ensure access to affordable, reliable, sustainable and modern energy for all’), 8 (‘Promote inclusive and sustainable economic growth, employment and decent work for all’), and 11 (‘Make cities inclusive, safe, resilient and sustainable’) have more than 80% of their targets related to a local health promotion perspective, this ratio is less than 30% for SDGs 14 (‘Conserve and sustainably use the oceans, seas and marine resources’), 16 (‘Promote just, peaceful and inclusive societies’), and 17 (‘Revitalize the global partnership for sustainable development’).
Looking at the measures actually implemented by the city of Lausanne in relation to the analytic grid presented previously (which uses 6 thematic issues and 56 categories), it appears that their distribution is extremely heterogeneous (see Figure 1), ranging from zero existing measure (for instance, regarding the category ‘terrestrial and freshwater ecosystems’) to more than 35 measures in the case of the category ‘access to green spaces and safe public spaces’. Overall, two thematic issues, social cohesion and equity and prevention and promotion of individual health, account for almost 60% of all measures implemented. The thematic issue ‘development aid and and international cooperation’ is quasi-inexistent with less than 2% of existing measures.
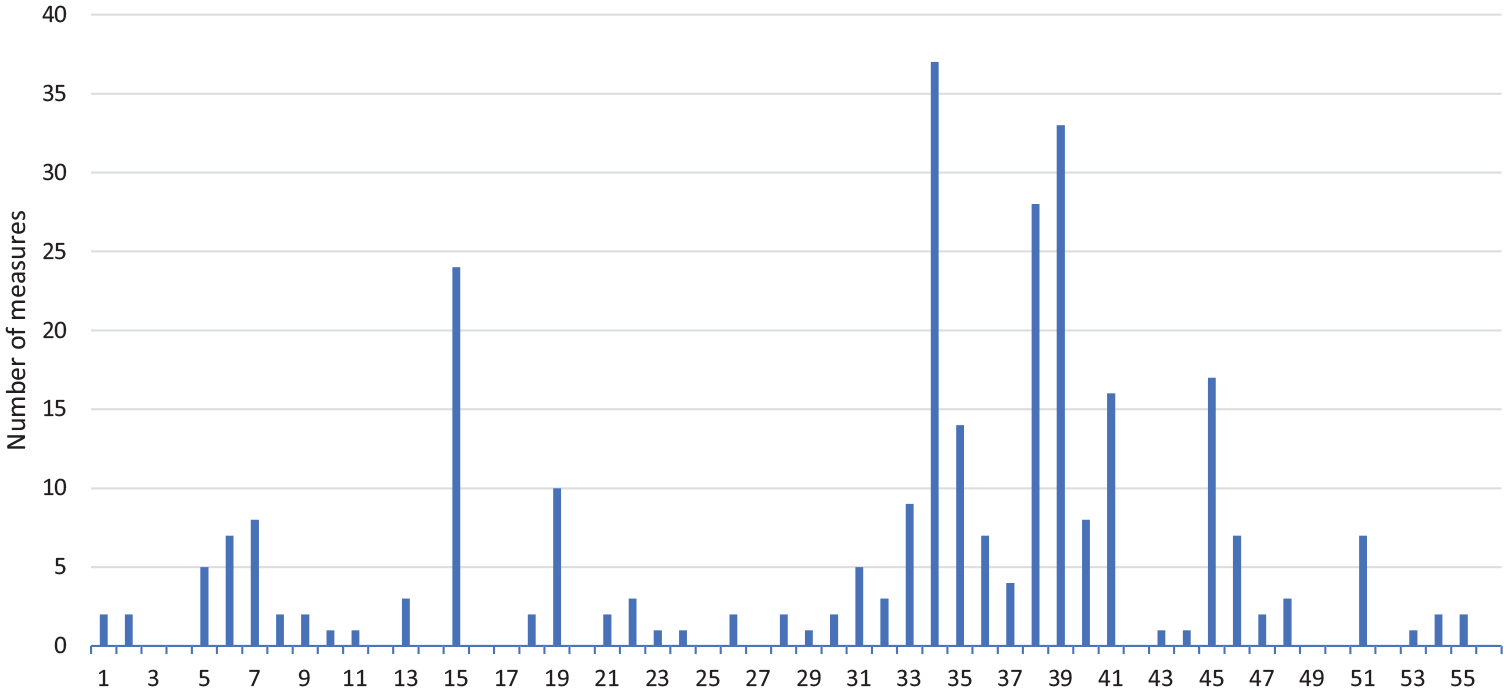
Number of measures for each of the 56 categories.
Furthermore, the significance of those measures largely varies, depending notably on the degree of intersectorality. For instance, the program ‘One tree, one child’, which has taken place on an annual basis since 2001 and aims at raising awareness on the importance of green spaces in urban settings by planting one tree for each newborn, does not have the same impact as the protection of forest areas inscribed in the municipal development plan. In order to account for that diversity, each of the 56 categories has been analyzed and ranked according to the scope and impact of the measures it encompasses. Six levels of implementation have then been identified (from the highest level to the lowest): (i) category is well covered, (ii) category is covered but there is room for improvement, (iii) category is not well covered or not enough information is available to determine the level of implementation, (iv) category is not well covered or not enough information is available to determine the level of implementation, however this category does not affect the main health promotion objectives of the city, (v) category is probably not relevant for the city (not enough information available to determine it), and (vi) category is not relevant for the city.
Based on this classification, three main findings can be highlighted. First, 33 of the 56 categories (59%) are either covered or well covered by measures implemented at the city level. This leaves only 8 categories insufficiently covered (14%) and 15 categories which are deemed at least partially irrelevant (27%). Second, some thematic issues are better covered by measures than others. In line with previous results, social cohesion and equity, and prevention and promotion of individual health are the two thematic issues with the highest level of implementation, at 70% and 100%, respectively. In contrast, production and economy only reaches 23% of categories (well) covered by measures implemented by the city. In consequence, this assessment reflects a promising situation with the vast majority of relevant SDG targets being dealt with by the city of Lausanne.
Nevertheless, several aspects of the city health promotion policy should be addressed. To begin with, 16 categories are covered by measures but could be improved and 5 others are insufficiently covered. This is primarily the case of the categories dealing with air quality, urban noise, biodiversity, sustainable food production, sustainable housing, access to green space and safe public spaces, and sustainable urban planning. Related health issues have indeed been sensitive, municipal representatives as well as the local population having expressed their concerns, notably regarding unsatisfactory levels of compliance with federal health standards.
Second, the listing of all health-promotion-related measures based on the three main health programs implemented by Lausanne shows their complementarity (most SDG targets are covered). However, it is hard to determine whether it reflects a strong synergy between health promotion programs or rather a lucky siloed process avoiding too much redundancy. Indeed, ‘Global Active City’ is focusing on measures related to physical activity, ‘Commune en santé’ has served as the basis for the city health promotion assessment, and ‘Healthy Cities’ is supposed to ensure the overall coherence of health-related measures with the SDG framework. A qualitative analysis of key stakeholders should then be conducted to evaluate their level of collaboration. The present analytical framework could be used to support such an endeavor.
Third, the relationship between the degree of intersectorality of existing measures and the overall level of implementation seems to clearly support the fact that more intersectorality leads to better results, i.e., categories with the highest levels of coverage (well covered). However, a closer look at data also shows that a few categories with the highest degree of intersectorality do not achieve the equivalent level in terms of implementation (this is, for instance, the case of measures related to categories ‘soil quality’ and ‘biodiversity’). In addition, a couple of categories with lower degrees of intersectorality do achieve the highest level of implementation (‘fair and universal access to water’ and ‘public markets and sustainable companies’). This observation calls for a more qualitative assessment of existing measures that could be based on interviews with municipal representatives, in order to better understand these few ‘outliers’. Furthermore, the identified intersectoral measures will be subject to in-depth discussion with Lausanne’s administrative authorities, so that their full potential can be acknowledged from a policy perspective.
Discussion
On the one hand, these preliminary results seem to indicate that measures implemented represent a systemic and relatively intersectoral effort developed by local authorities. On the other hand, they also point to a significant potential regarding the consideration of so far marginalized categories of measures, and an increased collaborative work during initial phases of policy development to notably avoid redundancy. It should also be pointed out that, in light of the general disconnect between sustainable development and public health policies, which seems to prevail in many countries, including Switzerland, the results obtained by the municipality of Lausanne indicate that, even in the presence of institutional barriers (e.g., conflicting levels of governance), policymaking at the local level has a lot of potential in circumventing these barriers. It can also be considered that the efforts made by Lausanne largely respond to the WHO’s repeated call, made for instance explicit in the HiAP or UTP programs, for a better integration of local stakeholders and cities in health promotion policymaking. However, it should also be emphasized that these results were obtained by a municipality whose political leaders decided to play a proactive role, 2 in contrast to many situations where actors’ interests tend to preserve a form of status quo (e.g., defense of ministers’ prerogatives). Furthermore, it could be argued that the ‘spatial and cognitive conditions’ necessary to achieve this level of policy integration are indeed easier to obtain at the local level, where the number of measures concerned, though considerable (approximately 250), remains manageable and relatable for actors involved. Following our initial argument stating the city level might be better suited to dealing with the complex array of factors impacting health and sustainability issues, the relative success of Lausanne could partly explain the renewed interest in the role of cities in tackling those issues. Indeed, over the last 30 years, the number of ‘theme cities networks’ (20) has grown considerably, from Healthy Cities to Sustainable Cities or Age-Friendly Cities, acknowledging the capacity of municipalities to bring about positive policy change.
Conclusion
This article aimed at presenting an analytical grid developed to assess health promotion measures implemented at the local level in relation to the SDG targets. The city of Lausanne served to illustrate the potential of such an analytical tool in providing a comprehensive perspective on current, potential, and missing measures. From a conceptual perspective, it has been shown that linkages between SDG targets and health promotion policies are manifold, and that health considerations go largely beyond the limited SDG 3 dedicated to ‘good health and well-being’. In that sense, the S2D grid can be seen as a tool in favor of organizational change, if stakeholders having an influence on health promotion but traditionally reluctant to collaborate, acknowledge their role in light of this new ‘theory-in-use’ (21). Increased inter-organizational governance could indeed be achieved thanks to the governing belief that health promotion and SDGs are deeply interrelated. From an empirical perspective, results obtained by Lausanne, and based on the analytical grid comprising 6 thematic issues and 56 categories explicitly comparable to the 169 SDG targets, tend to emphasize the global achievement of policies relevant both in terms of health promotion and sustainable development. It should also be noted that the analytical grid presented here is characterized by its versatility and potential usefulness in other local contexts. Furthermore, it could serve to measure the gap between an ideal situation, where all relevant categories identified are dealt with, there is no redundancy among measures taken and the degree of intersectorality is highest, and the current situation experienced by a municipality. In the case of Lausanne, this gap appears to be relatively limited: 80% of relevant categories are taken into account by existing measures, redundancy is very limited, and the degree of intersectorality is high. Finally, it should be noted that the S2D grid is designed to be applied in other municipalities and to achieve several goals: assessment of a particular health promotion program, communication between cities or departments, to be a benchmarking tool, and providing information for the public.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
1.
According to Hancock and Duhl (22), these 11 qualities are: (1) a clean, safe, high-quality physical environment; (2) an ecosystem which is stable now and sustainable in the long term; (3) a strong, mutually supportive, and non-exploitive community; (4) a high degree of public participation in and control over the decisions affecting one’s life, health, and well-being; (5) the meeting of basic needs for all the city’s people; (6) access to a wide variety of experiences and resources with the possibility of multiple contacts, interaction, and communication; (7) a diverse, vital, and innovative city economy; (8) encouragement of connectedness with the past, with cultural and biological heritage, and with other groups and individuals; (9) a city form that is compatible with and enhances the above parameters and behaviors; (10) an optimum level of appropriate public-health and sick-care services accessible to all; and (![]() ) high health status.
) high health status.