
Abstract
Most people in need of mental health services in Mexico do not seek formal support or professional services to address their mental health needs. Understanding help-seeking behaviors is crucial to addressing underutilized mental health services and to leverage health promotion efforts. Data were collected as part of a larger research project on stigma and help-seeking for mental-health-related concerns in Mexico. A convenience sample of 469 adults residing in Mexico City participated in the study using an experimental vignette methodology assessing stigma toward individuals with mental health conditions, along with characteristics and demographic correlates of help-seeking. All survey measures were administered in Spanish. A structural regression was conducted for the outcome ‘openness to professional help seeking for mental health problems’ as a latent variable. Compared with males, females were more open to professional help seeking (b = 0.09, p = 0.038), as were people who endorsed higher spirituality (b = 0.01, p = 0.006); while people who experienced self-stigma were less open to professional help-seeking for mental health concerns (b = −0.15, p = 0.005). Self-stigma was a major driver of low service utilization. Contrary to previous studies, spirituality was a significant positive predictor of professional help-seeking. A more nuanced understanding of mental health help-seeking in Mexico can be useful for outreach efforts to increase service utilization both in Mexico and among Latinos in the United States (US). Given historical, geographic, and cultural ties with the US, it is important to understand mental health help-seeking in Mexico, which may relate directly to help-seeking behaviors in many US Latinos who have immigrated to the US. Directions for future research and practice implications are discussed, including a roadmap for health promotion activities.
Introduction
Despite recent advancements in acknowledging mental health as a public health concern, Mexico continues to face significant challenges in promoting mental wellbeing and providing accessible mental health services. Mental health promotion is essential for overall population wellbeing, but it is lacking in Mexico, a country grappling with a mental health crisis marked by high prevalence rates of mental disorders, limited resources allocated to mental health services, and low mental health services utilization (1). Lifetime prevalence of any mental health disorder in Mexico is 26.1%, with the most prevalent diagnoses being alcohol use disorder (AUD) and major depressive disorder (MDD), affecting 7.6% and 7.2% of the adults, respectively, at any given time (2). Yet, only 24% of those in need of psychiatric care utilize any mental health services (3). Most people with severe mental health diagnoses (76.2%), such as schizophrenia or bipolar disorder, 77.9% of those with more moderate mental health disorders, and 87.4% of those with mild disorders, receive no mental health treatment (4). These grave mental health challenges do not exist in isolation; rather, they exist against a backdrop of significant health disparities and barriers to effective health promotion exacerbated by the unequal distribution of healthcare resources and limited health education in general, and especially in marginalized communities.
Access to mental health care is an international public health challenge and an important consi-deration when discussing help-seeking behaviors (5,6). Without treatment, mental health problems can have staggering implications for individuals and society, with consequences including unnecessary disability resulting in diminished quality of life, poverty, lost productivity, impact to the local economy, and increased healthcare costs (7).
Seeking help for a mental health disorder is a critical first step to accessing and receiving mental health care (5). A variety of sociodemographic factors, including age, gender, level of education, geographic location, religiosity, socioeconomic status (SES), and stigma, have been found to predict help-seeking behavior, including seeking professional help for mental health concerns (5,8). In addition, for Mexican adults, economic barriers, logistical barriers such as lack of transportation or limited availability of services in one’s neighborhood, the belief that mental health disorders are associated with personal weakness, and lack of faith in the system due to failed previous healthcare experiences, are commonly endorsed barriers to seeking help (9,10). Mexicans with high levels of religiosity often turn to faith-based healing as a form of alternative treatment and are less likely to seek professional mental health treatment (11). Further, Mexican men have been found to be less likely to engage in professional help-seeking behaviors, in part due to conformity of masculine roles in the culture (12,13). Many of these factors could be addressed through increased health promotion efforts, as presented later in this paper.
Once a decision is made to seek help, individuals with mental health disorders are required to overcome additional, non-logistical barriers to access mental health care, including social stigma, discrimination, comorbidity of mental health disorders and non-communicable diseases, and the presence of additional mental health disorders (4,14). Mental health stigma is widely present in Mexico (15,16). Even with increased knowledge of mental health disorders, negative attitudes towards mental health and help-seeking may prevent individuals from getting the necessary care. This results in those affected becoming more likely to hide their symptoms and to seek help only after years of suffering or if symptom progression gets so severe that they can no longer function (17). Many of these factors are addressable through increased health promotion efforts.
Untreated mental health conditions are a significant burden to society, communities, families, and the individuals managing them. This research seeks to better understand the factors contributing to mental health help-seeking in Mexico. More specifically, the study investigated the following questions:
What are the attitudes toward professional help-seeking for mental health concerns among Mexican individuals?
What sociodemographic characteristics are associated with Mexican individuals’ help-seeking attitudes?
Materials and methods
Data for this paper were collected as part of a larger research project on stigma and help-seeking in Mexico City — the most populous and well-resourced metropolitan area in Mexico. A convenience sample of 469 adults residing in Mexico City participated in the study, which used an experimental vignette methodology to assess various domains of stigma toward individuals with mental health conditions. Before data collection, this study received ethics approval from University in Mexico and approval from the Institutional Review Board (IRB) of American University. A bilingual English/Spanish-speaking research team, recruited from University in Mexico and trained jointly by faculty from Mexico and the US, street-recruited a convenience sample of participants from various public spaces in Mexico City (e.g., shopping malls, markets, churches, social service agencies, etc.).
To participate in the study, interested participants had to be at least 18 years of age at the time of data collection and reside permanently in Mexico City. Eligible participants were given verbal information, in Spanish, concerning eligibility criteria, purpose of the study, time of participation, and potential risks and benefits. To ensure the privacy and anonymity of participants, as well as to reduce potential response bias, the research team received a waiver of documented written consent from the IRB. After eligibility was established, if the individual agreed to participate, verbal consent was obtained, and a research assistant read the survey questions aloud to the participant and recorded their responses verbatim, in written form. All survey measures were administered in Spanish. Measures not originally available in Spanish were back translated from English before survey administration by a professional translation team with input from faculty at the Mexico University, to capture the linguistic nuances of the local community. The entire instrument took approximately 45 min to complete, and participants were given a backpack with the logo of the Mexico university (approximate value $15 USD) to compensate them for their time (the backpack was used to allay concerns from the Mexico team about cash incentives, including security, logistics, and any potential concerns of being associated with efforts to sway voters).
Measures
Demographics and familiarity with mental health conditions
Demographic variables included: age, gender, marital status, parental status (i.e., with/without children), highest level of education, employment status, and subjective financial circumstances. Participants were asked three questions to assess their previous exposure to someone with mental health issues: whether they, any of their friends, or any of their family members had mental health problems. If they replied yes to any of these questions, they were classified as having some familiarity with mental health issues.
Spirituality
Spirituality was measured with six items extracted from the Daily Spiritual Experiences Scale (DSES) (18). Items were rated on a 6-point Likert-type scale ranging from 1 = never or almost never to 6 = most of the day every day. The total score of the six items was summed, with higher scores indicating higher levels of spirituality.
Stigma
Public stigma was measured with the Devaluation of Consumer Families Scale (DCFS) (19,20) which consists of seven items measured on a four-point Likert scale from 1 = strongly disagree to 4 = strongly agree. Negatively worded items are reverse coded before summing all items, so that a higher score indicates a higher level of public stigma.
Self-stigma was measured using the Stigma Concerns about Mental Health Care Scale (SCMHC) (21). The three items measure self-stigma using the following prompts: I would not want to receive treatment for depression because. . . followed by ‘embarrassed to talk about personal matters with others,’ ‘afraid of what others might think,’ and ‘family members might not approve.’ Possible responses were agree, disagree, and I don’t know. If a person answered agree or I don’t know to any of the three questions, they were categorized as showing signs of self-stigma; participants who answered disagree to all the three questions were categorized as showing no signs of self-stigma.
Attitudes and beliefs about help-seeking
Openness to seeking help for mental health issues was measured using the Attitudes Toward Seeking Professional Psychological Help, Short Form (ATSPPH-SF) (22). The ATSPPH-SF is a 10-item scale that measures responses to questions related to people’s beliefs about help seeking on a 4-point Likert scale where 0 = disagree, 1 = probably disagree, 2 = probably agree, and 3 = agree. Negatively worded items are reverse scored and items are then summed, with higher scores indicating more positive attitudes toward seeking professional psychological help and lower levels of stigma about mental illness.
Statistical analysis
Data analyses were completed using SPSS 28 and Mplus 8.4 (23). Data were checked for normality. Maximum likelihood estimation was used, along with robust standard errors and model fit statistics to account for departures from normality and to account for missing data. Cases with missing values were less than 5% (n = 21, 3.5%). Counts and percentages were calculated for categorical variables and means and standard deviations were calculated for scale variables. Before fitting full structural equation models, a measurement model was checked using a confirmatory factor analysis (CFA) framework to determine whether measures for constructs of interest had performed as expected in this sample.
Results
Psychometric evaluation of performance of study measures
ATSPPH–SF
Among the 10 items, the five reverse-worded items were dropped because they had low factor loadings — an approach employed in previous studies. The five positively worded items were used to represent the attitudes towards seeking professional psychological health. The model fit for this measure was adequate:
DCFS
Similar to ATSPPH-SF, only the four positively worded items were used due to low factor loadings for the reverse scored items. CFA showed an adequate model fit:
DSES
For the spirituality measure, a scree plot was first checked to verify the scale was unidimensional. A one-factor CFA was then fitted with the data. The model had an adequate fit:
Univariate and bivariate results
Sample sociodemographic characteristics and descriptive information of the outcome variable are summarized in Table 1. The mean age of participants was 37 years old (Mean = 37.28, SD = 14.31). The sample was almost evenly split on gender, with 293 (49.2%) identifying as female and 302 (50.8%) as male. Just over half of the sample (n = 308, 51.8%) said they were not married. Two-thirds (n = 399, 67.3%) were employed at least part time at the time of data collection. In terms of subjective financial circumstances, just over a third (n = 216, 36.2%) indicated that they ‘did not have enough money’ to meet their expenses. Almost half of the participants (n = 267, 46.1%) indicated that they did not know anyone with a mental health problem. Seven in 10 (n = 425, 71.3%) reported no self-stigma towards mental health concerns. On the DSES, the sample mean of 14.58 (SD = 8.27) on a scale of 0 to 30 indicates a moderate level of spirituality in this study sample. On the DCFS, the average sample mean of 2.38 (SD = 0.65) on a scale of 1 to 4 indicates a moderate level of public stigma towards mental health issues in this study sample. Lastly, on the key outcome variable — attitudes towards seeking professional mental health services — the average sample mean of 3.29 (SD = 0.60) on a scale of 1 to 4 indicates a high level of openness to professional help with mental health problems.
Sociodemographic characteristics of participants.
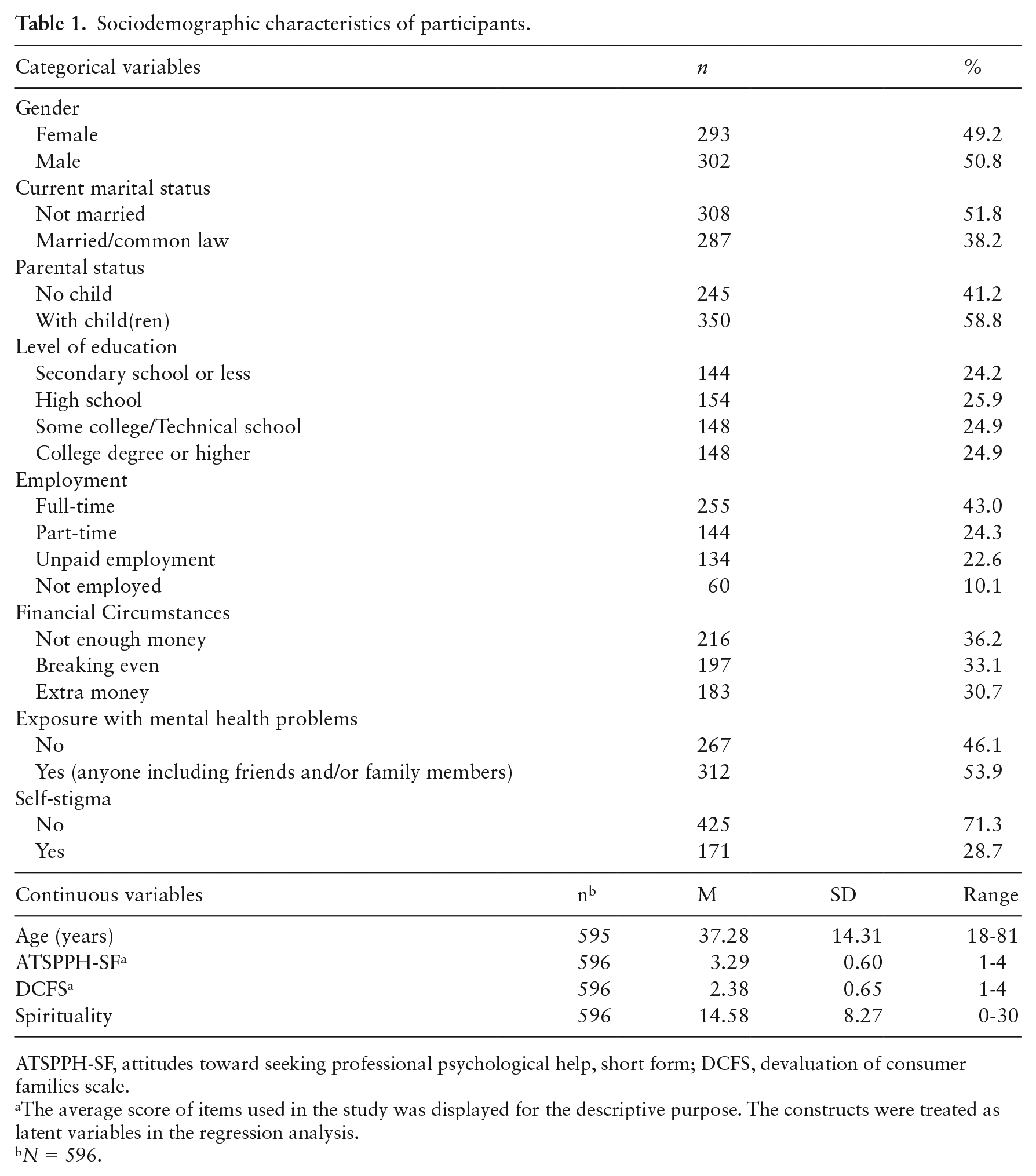
ATSPPH-SF, attitudes toward seeking professional psychological help, short form; DCFS, devaluation of consumer families scale.
The average score of items used in the study was displayed for the descriptive purpose. The constructs were treated as latent variables in the regression analysis.
N = 596.
Structural regression
After an adequate measurement model was established, a structural regression was conducted with the outcome openness to professional help seeking for mental health problems treated as a latent variable. The predictors of the model include age, marital status, gender, parental status, financial status, education, employment, exposure to mental health problems, spirituality, public stigma, and self-stigma; public stigma was treated as a latent exogenous variable. Detailed in Table 2, the model explained 10.3% (p = 0.001) of the variance in openness to help-seeking. Among the 11 predictors, gender, spirituality, and self-stigma significantly predicted openness to professional help-seeking for mental health concerns. Compared with male participants, female participants were more open to professional help-seeking (b = 0.09, p = 0.038), as were people who endorsed higher spirituality (b = 0.01, p = 0.006); people who reported self-stigma were less open to professional help-seeking for mental health concerns (b = −0.15, p = 0.005).
Regression of associations between openness to help seeking and sociodemographic characteristics of respondents.
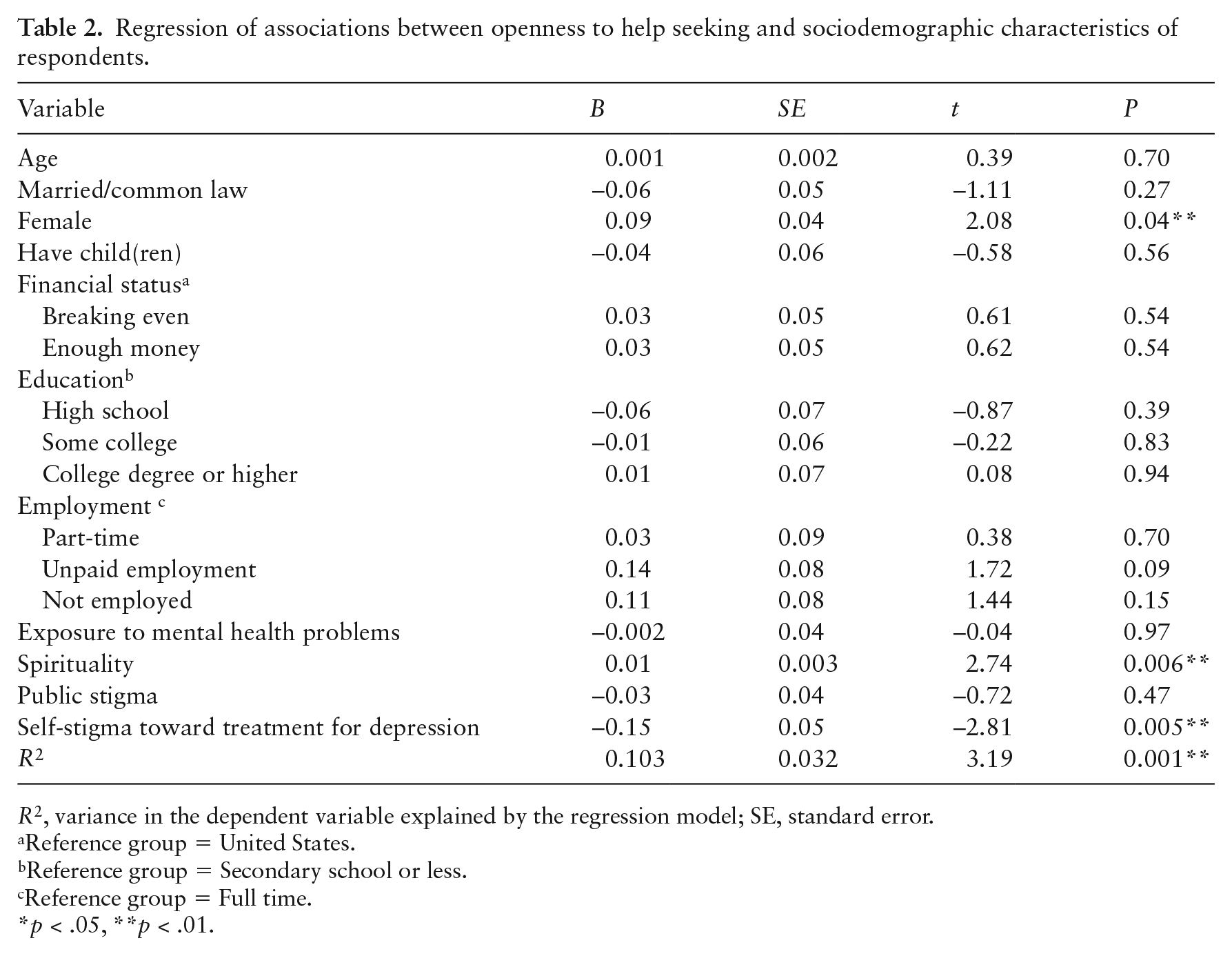
R2, variance in the dependent variable explained by the regression model; SE, standard error.
Reference group = United States.
Reference group = Secondary school or less.
Reference group = Full time.
p < .05, **p < .01.
Discussion
Individuals in Mexico continue to have low levels of mental health service utilization despite high prevalence of mental health disorders (1). Moreover, there is a lack of current research that explores predictors of mental health help-seeking behaviors in Mexican adults. To understand this area more in depth, this study examined predictors of attitudes towards mental health and professional help-seeking in a homogenous sample of adults in Mexico City.
Several predictors of attitudes toward mental health help-seeking commonly found in the literature were not found to be significant in this study. For example, SES is frequently correlated with help-seeking, especially in those reporting higher levels of income. Two proxy measures of SES were included in this study, education, and financial circumstances (i.e., ‘not having enough money to meet their needs’), and neither were found to be a significant predictor of attitudes toward help seeking, which is consistent with Zimmerman (24) but inconsistent with work by Lorenzo-Blanco and Delva (25), which found that individuals with higher incomes and with at least 16 years of education (i.e., higher SES) found formal services more helpful compared with individuals with lower incomes and less education. Both articles are more than 10 years old and the relationship between income and help-seeking may have changed over time. It is also worth considering that Mexico City is a large (>25 million people), multicultural, and very progressive metropolis where openness might be more common, as compared with smaller cities and more rural areas. Moreover, given its size and status as Mexico’s capital, it is also much better-resourced than many other regions in terms of health and mental health services, and health promotion efforts are perhaps more concentrated in a city the size of Mexico City. The relationship between SES and help-seeking is complex and warrants further study, especially in populations with lower income and lower formal education, like those in this study, who reside in Mexican communities distinct from Mexico City in their size, resources, and health promotion efforts.
Recent research on the relationship between exposure to mental health problems (i.e., knowing anyone with a mental health problem, including friends and/or family members) and attitudes toward help-seeking behaviors tends to be positive, such that those with greater familiarity will engage in less stigmatizing behaviors and have a greater openness to mental health help-seeking (6). However, in this study respondents’ exposure to mental health problems was not significantly related to mental health help-seeking. This may be due, in part, to an unexpectedly high percentage of respondents in this study (46.1%) endorsing having no familiarity with someone experiencing a mental health concern. The high percentage of individuals indicating no previous exposure to someone with a mental health condition speaks to the potential for those with mental health concerns to hide their symptoms and potentially not seek help due to perceived public stigma toward mental health conditions. Also, ours was a community-recruited sample, not a clinical sample and, as such, many respondents could have been wary of disclosing any connection with individuals struggling with mental health concerns. Further research into which groups of individuals in Mexico have low, moderate, or high exposure to those with mental health concerns is warranted, given the significant mismatch between the high diagnostic and symptom prevalence cited in the literature and self-report of previous exposure to those with mental health concerns in our study.
Just over a quarter (28.7%) of participants in this study indicated self-stigma about mental health, with these participants also endorsing less openness to seeking professional help for mental health concerns. This means that, if all other factors are held constant, those endorsing self-stigma will have 0.15 points lower (on a 4-point scale) openness to seeking professional help for mental health concerns. This finding is consistent with previous research in this area suggesting that self-stigma is often negatively associated with seeking help for mental health conditions (14). Thus, interventions designed to address self-stigma toward mental illness within the Mexican context are currently warranted. Health promotion efforts, including raising awa-reness through targeted campaigns, expanding access, attending to cultural considerations, dev-eloping school-based mental health programs where conversations about mental health start early, and policy advocacy, have been found to combat stigma. These are important areas for practice and policy efforts in Mexico.
Also congruous with previous research, female respondents were more likely to seek help for mental health concerns than men (5,26,27). This finding has been hypothesized in studies with similar results as being influenced by gendered cultural norms around the role of masculinity (13) within Mexican culture. Often, men are expected to be self-sufficient, and admitting that they have a problem and seeking external assistance for it may be perceived as weakness. Health promotion efforts that seek to weaken the connection between mental health or asking for help and ‘weakness’ might be useful to address this gender disparity in help-seeking.
Finally, spirituality was found to be a significant predictor of help-seeking, with individuals endorsing higher spirituality being slightly more open to seeking help. This is a factor that is often considered to be a major predictor of help-seeking attitudes among Latinos (28). However, in previous studies conducted in Mexico and with Latinos in the US, higher levels of spirituality/religiosity were associated with less positive attitudes toward professional help seeking (29,30). This inconsistency could be explained, at least partially, by the characteristics of Mexico City and its residents, as described earlier. More research in other Mexico communities could help us better understand this relationship. The finding also speaks to the ongoing need for more research concerning the complex interplay between religiosity and help seeking, which may change based on one’s religious tradition, or may evolve as faith, spirituality, or religious beliefs and practices change over time. It also highlights opportunities for religious leaders to assist their congregants with seeking professional mental health treatment when needed (31). There were examples of this during the early days of COVID vaccination efforts, when religious leaders were being publicly vaccinated in their congregations and many members of their communities followed suit. Religious leaders speaking openly about mental health concerns and the need to seek treatment could be an important health promotion effort.
Limitations
These data were drawn from a community-based convenience sample of respondents from Mexico City. Caution should be exercised as results may not be generalizable to residents of other areas of Mexico, particularly those residing in more rural and less well-resourced areas. Similarly, social desirability bias may have impacted participant responses, as the survey was administered orally by the research associates, and participants also offered an oral response to the questions. Although this allowed for participation of those with limited levels of literacy, this method of survey administration may have potentially impacted the results. Also, this was a cross-sectional study measuring help-seeking attitudes at one point in time. Future longitudinal research examining willingness and openness to help-seeking across time may be warranted to further explore how help-seeking attitudes and behaviors may change or evolve.
Implications and conclusions
Despite the limitations, this research addresses a critical gap in the literature on the limited knowledge on attitudes of Mexican residents concerning seeking professional help for mental health concerns and identifies important areas for health promotion efforts. Just over a quarter of participants in our study endorsed self-stigma toward mental health concerns, and they are certainly not alone. Self-stigma is a phenomenon that has been reported in many countries, represents a barrier to seeking treatment, and also has negative psychological sequelae in people (9,32). Low levels of psychological help-seeking in Mexico and Latin America are often tied to the negative views about mental health problems (33). These negative views may be perpetuated by cultural beliefs about self-reliance, not having enough willpower, or keeping secrets in the family (33).
Stigma, however, has been shown to be ameliorated by health promotion efforts, and it can be addressed. Yet, Mexico currently has no identified publicly funded health programs focused on promoting mental health treatment seeking, and no large, organized, health promotion efforts designed to eradicate the social stigma associated with these conditions and their care (34). Mental health professionals often labor in isolation as they try to combat stigma and shift people’s beliefs so that communities can have increased knowledge and confidence in treatment and, thus, become more receptive to seeking and accepting help. Providers cannot do this alone, and must partner with government and non-government organizations, academics, K-12 (kindergarten to 12th grade) schools, faith leaders, media, and grass roots organizations, to disseminate accurate information about mental health and the symptoms of common mental health concerns, and to reduce stigma, enhance services, and promote acceptability and access. This is of particular importance in relation to men, who are, in general, more reluctant to engage with formal treatment providers. By leveraging expanded health promotion efforts to change the narrative of ‘help seeking as a sign of weakness’ to ‘help seeking as a way to take care of one’s responsibilities and one’s family,’ treatment providers can encourage those in need of formal services to seek them out when needed. Moreover, the ongoing development of mental health service infrastructure and implementation of evidence-based treatment approaches are essential to increasing access to treatment and quality of care, thus supporting increased and ongoing engagement with formal systems of care.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded in part by the University of Houston Center for Mexican American Studies (CMAS) Grant, R.E.G. (PI).