
Abstract
Studies evaluating the influence of health literacy on patient behavior and outcomes suggest a positive relationship between health literacy and health knowledge, health behaviors, and health status. In Latin American countries, studies assessing health literacy are few, regional, and demonstrate considerable variation, with reported rates of adequate health literacy ranging from 5.0% to 73.3%. In this paper, we examine and explore the state of health literacy and efforts to promote it in Latin America. Key challenges to those efforts include socioeconomic inequality, social/geographic isolation, and cultural-, language-, and policy-related barriers, many of which disproportionately affect indigenous populations and others living in rural areas. Greater use of infographics, videos, and mobile apps may enhance health literacy and patient empowerment, especially when language barriers exist. This paper provides strategies and tools for tailored programming, examples of successful health literacy interventions, and policy recommendations to improve health literacy in Latin America, intending to spur additional discussion and action. Centrally organized collaboration across multiple sectors of society, with community involvement, will enhance health literacy and improve health and well-being across Latin America.
Keywords
Introduction
There is a critical need for health literacy initiatives across Latin America to improve navigation of healthcare systems and empower individuals to make informed decisions regarding lifestyle and health. Health systems in Latin America are often uncoordinated and segmented, which can adversely impact the people they serve. This is especially true for the aging population, individuals with comorbid chronic conditions, and those experiencing epidemics (e.g. chikungunya, Zika, coronavirus disease 2019 [COVID-19]) (1,2).
Health literacy embodies the skills and motivation needed to find, understand, evaluate, and use health information (3). Health literacy influences knowledge, attitudes, and behaviors, including disease prevention and self-management. Low health literacy impacts health outcomes and health-related costs, leading to inefficient healthcare utilization and delivery (4,5). Improving health literacy increases the ability to obtain and understand health information, facilitates informed decision-making, and improves the ability to manage and cope with health disparities. This allows for greater autonomy and empowerment (4).
At the population level, promoting health literacy may lead to improved equity and sustainability in public health. As a modifiable social determinant of health, it is considered an outcome of education and health promotion (6) and is closely linked to general literacy (4). Hence, improving primary education, expanding adult education, reducing health system complexity, and expanding conceptions of health beyond medicine to include social, economic, and environmental (built and natural) factors are all parallel policy goals that must be promoted to enhance health literacy (1).
In this paper, we examine the current state of health literacy in Latin America, including challenges and barriers, and explore initiatives to promote health literacy and health in the region. We also suggest strategies to address disparities, with the intent of spurring future discussion among healthcare workers, governments, patient groups, industry, and academia. The 33 countries that make up Latin America have diverse cultures, resources, and healthcare systems. Integrating health literacy principles into healthcare, disease prevention, and health promotion initiatives is one way to improve the health of individuals, their families, and society as a whole.
Current state of health literacy in Latin America
We found no studies that evaluated national levels of health literacy in Latin American countries. Table 1 shows considerable variation of measurement approaches in regional studies, with adequate health literacy ranging from 5.0% to 73.3%, although assessments did not always use the same scale, and definitions of adequate health literacy were inconsistent (7–14). Condition-specific assessments have also been evaluated. For example, a Brazilian study demonstrated the validity and reliability of a health literacy assessment scale for drug treatment adherence among patients with diabetes (15).
Health literacy levels in Latin America.
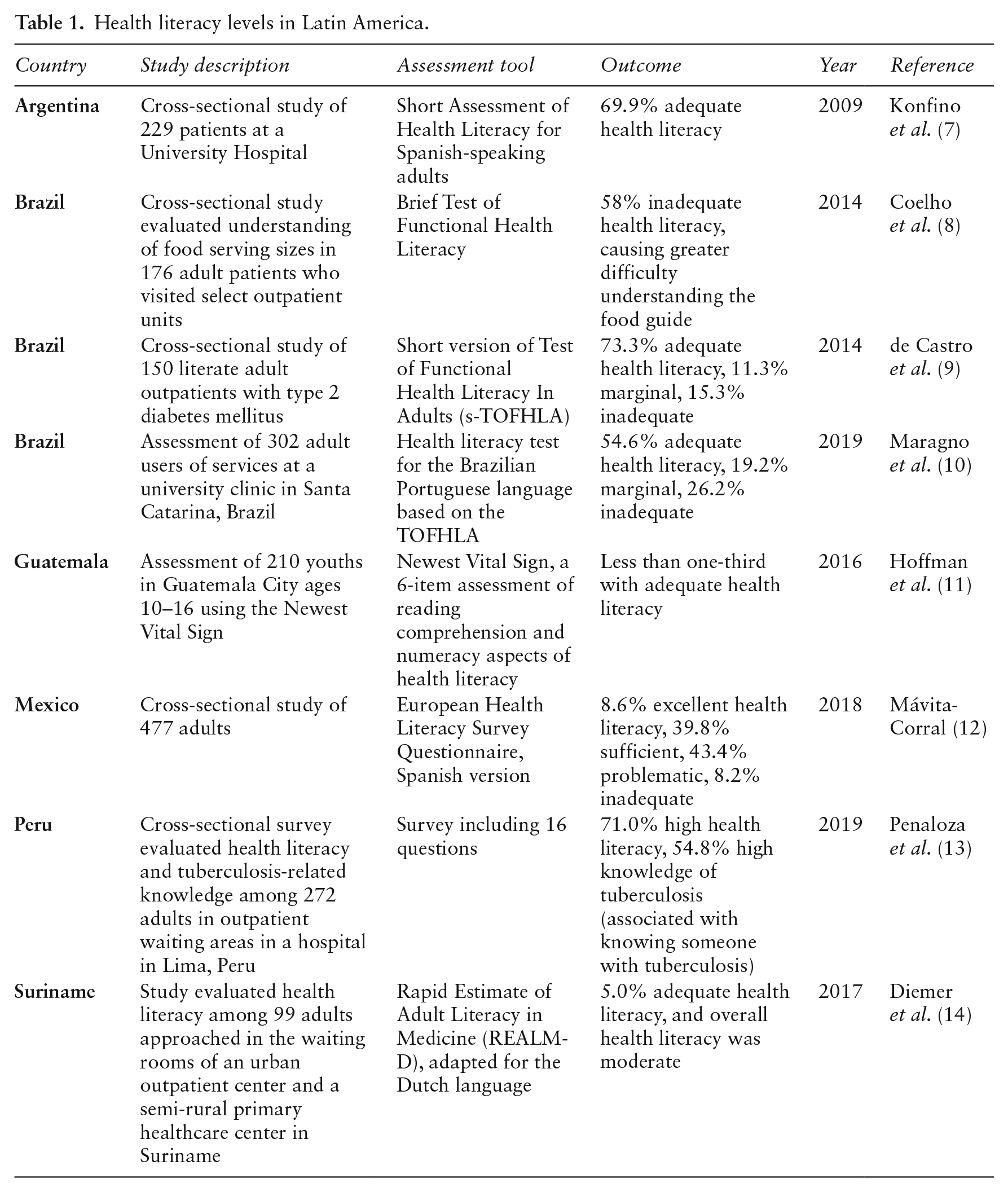
Studies evaluating health literacy often did so in association with concerns about prevalent diseases that cause high morbidity and mortality, like cardiovascular disease in Suriname, diabetes in Brazil, and tuberculosis in Peru (9,13,14). This is important, as adequate health literacy may enable people to engage in positive behaviors related to modifiable risk factors for non-communicable diseases and help people recognize and slow the transmission and progression of communicable diseases.
Studies evaluating the impact of health literacy on health behaviors and outcomes demonstrate a positive relationship with knowledge of health, health behaviors, and health status (16–18). For example, among 156 patients with diabetes in Argentina, glycated hemoglobin (an indicator of management of diabetes, with a generally recommended goal of <7% (19)) was 8.15% among those with inadequate health literacy versus 7.15% among patients with adequate health literacy (P = 0.0001) (16). In another example, two overlapping surveys of 651 adult patients in La Paz, Bolivia (all with at least one chronic disease) showed that people with low health literacy were 37% more likely to have poor adherence to medication compared to people with higher health literacy (17). In a third example, a cross-sectional study of 248 adults in Piracicaba, São Paulo, Brazil showed an association between low oral health literacy and the presence of dental plaque, use of dental services for emergency treatment only, use of dental services due to pain, and a ‘not good’ dental service evaluation (18).
Barriers to improved health literacy in Latin America
While limited health literacy is common across all backgrounds, certain sociodemographic groups (e.g. older adults, those with low socioeconomic status or less education, people who speak a language other than the national/majority language at home) are more likely to have limited health literacy (4,9,13). Given the language diversity in the region — over 270 languages are spoken in Brazil alone (20) — limited fluency in the national language can be a significant barrier to health literacy. To help navigate this obstacle, some organizations have integrated indigenous languages into health education. During the COVID-19 pandemic in 2020, the Tekove Katu School of Health (Gutiérrez, Bolivia) and the Pan American Health Organization/World Health Organization (PAHO/WHO) developed a training and communication program in Bolivia’s Chaco region to help prevent the spread of COVID-19 among indigenous communities. Working with the local community and community health workers, they created leaflets, folders, radio broadcasts, and infographics in both Spanish and Guaraní, the primary language for most Chaco residents (21). In another regional initiative, the United Nations High Commissioner for Refugees developed a training program to improve healthcare for Venezuelan migrants who moved to Brazil. To facilitate communications between Brazilian health professionals and Venezuelan citizens, training and educational materials were developed in several indigenous languages, like Warao and Panare (22). Still, bridging culture and language barriers remains a significant hurdle in Latin America. Inadequate proficiency in the national language puts people at a marked disadvantage, as language comprehension and communication are essential to advocate for oneself, to understand and act on health information, and to navigate complex healthcare systems (4).
Another barrier to health literacy in Latin America is poverty. Social inequities, like poverty, have had a profound effect on health in Latin America. Member states in PAHO have been working to reduce inequalities as a key aspect of their ‘Strategy for Universal Access to Health and Universal Health Coverage,’ and the region has experienced commendable economic growth. Yet, despite these advances, Latin America remains one of the most economically challenged regions globally, with almost one-third of people living below the poverty line and the poorest 40% receiving less than 15% of the overall income (1). Although 49% of indigenous people in Latin America live in urban areas, they are 2.7× more likely to live in extreme poverty compared to nonindigenous urban residents (23). The widening economic divide that separates indigenous and nonindigenous communities also contributes to health disparities. Improving health literacy is one way to improve well-being and boost regional economies. While no comparable statistics are available in Latin America, a 2020 analysis conducted by UnitedHealth Group suggests that improving health literacy in the United States could save the US Medicare program up to $25.4 billion (24).
Marginalization has been associated with lower educational attainment and socioeconomic status, which in turn are associated with lower health literacy. Among indigenous populations in Latin America living in urban areas, primary education completion is 1.6× higher, secondary education 3.6× higher, and tertiary education 7.7× higher than those living in rural areas (23), indicating that social marginalization may be associated with less education opportunities among indigenous populations. Opportunities are also limited for nonindigenous populations in rural areas of Brazil, Argentina, Uruguay, and Paraguay (25). Further, both indigenous and nonindigenous people in rural areas are more likely to be poor (23). Disparities associated with social/geographic isolation — especially combined with the fact that healthcare budgets are often inequitably distributed nationwide (1) — have important implications regarding the potential impact on health literacy and health outcomes.
When addressing health literacy in vulnerable groups, it is important to consider historical experiences, gender, cultural differences (e.g. language), and the political climate. In Mexico, historical experiences (like mass sterilization under false pretenses) have led to distrust among indigenous populations, contributing to fears that government-sponsored healthcare programs will not respect them. Gender discrimination often prevents women from making the healthiest decisions and can reduce their feelings of engagement and empowerment (26). Language barriers disproportionately affect vulnerable populations. Indigenous Latin American populations do not always speak Spanish or Portuguese; many communicate primarily in native languages. While not all countries officially recognize these languages in government communications, some do. For example, in Paraguay, both Spanish and Guaraní are official languages (23). Finally, political systems and views affecting public health policy pose challenges to improving health literacy, and incoming governments should prioritize continuity in initiatives across Latin America.
Initiatives to improve health literacy in Latin America
Culture, civics, and science should be equally addressed in health literacy initiatives and policies to address key challenges in Latin America. Programs should address socioeconomic inequality, social/geographic isolation, cultural/language barriers, and policy-related barriers. Patient organizations, healthcare organizations, governments, foundations, and community leaders have taken various approaches to address these challenges, mostly within the realm of preventive healthcare.
Patient organizations in Latin America focus on increasing patient-centered care and patient empowerment (27). As part of the patient advocacy postgraduate program at the Biomedical Faculty of Austral University in Argentina (28), leaders from different countries representing patients’ organizations can learn to implement health literacy strategies in their countries.
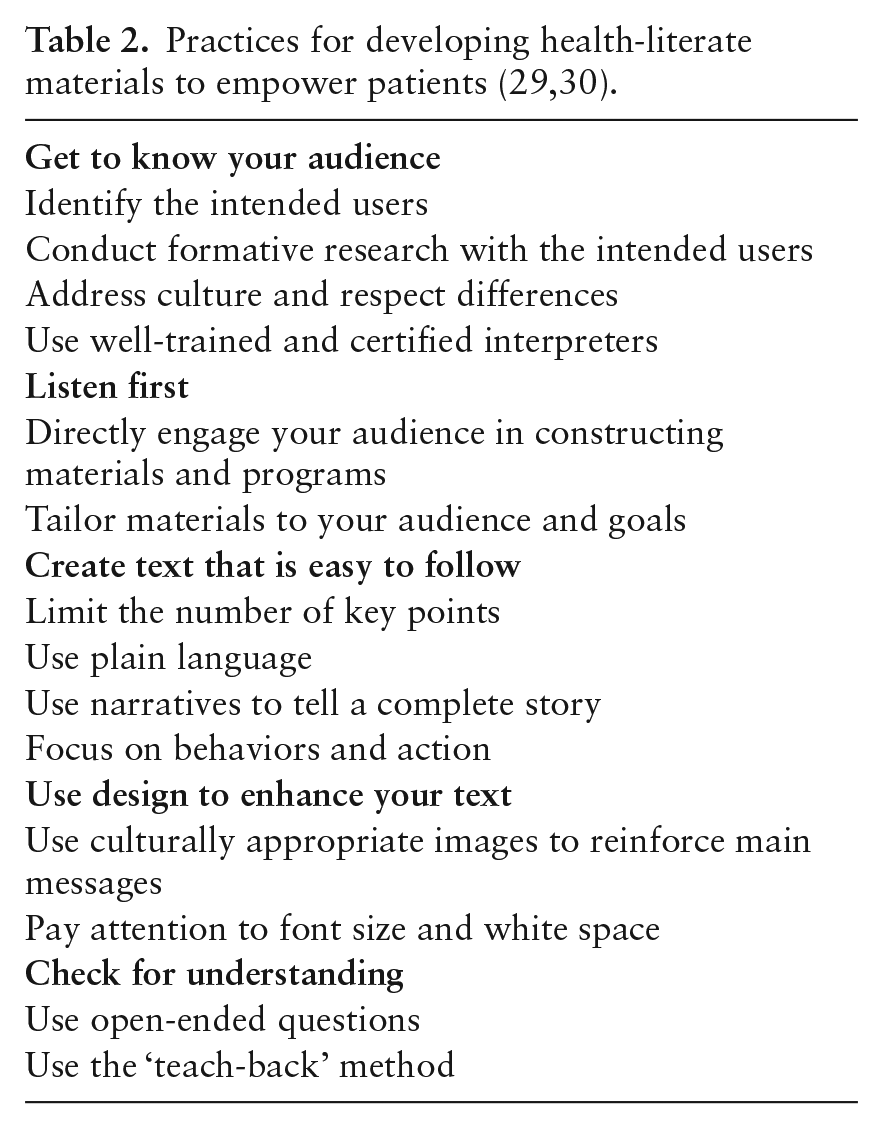
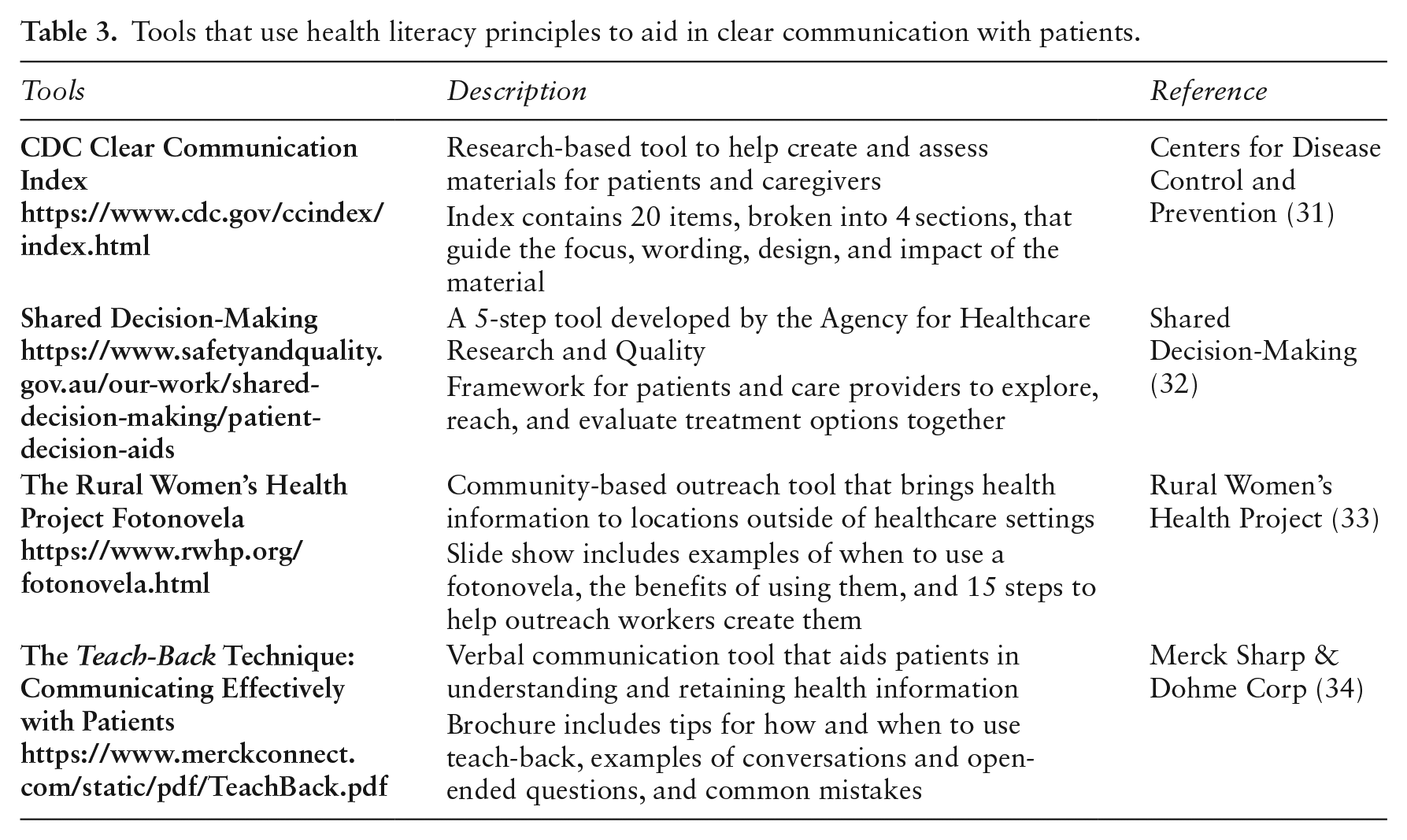
Healthcare organizations can empower the people they serve — as well as their doctors, nurses, and other care team members — to actively engage in making collaborative decisions about their health. To help in this effort, Table 2 provides tips for developing written materials, and Table 3 provides links to communication tools. These approaches can enhance the partnership between healthcare providers and patients to empower patients and engage them in the decision-making process (32). However, there remains a significant need for health literacy materials to be translated into and developed in Spanish, Portuguese, and local languages.
Tools that use health literacy principles to aid in clear communication with patients.
Mexico
Government-led vaccination campaigns headed by the Ministry of Health in Mexico successfully increased awareness and encouraged immunization (35). In another example from Mexico, PrevinIMMS, an integrated health program of the Mexican Institute of Social Security, focuses on promoting preventive healthcare through education (35). One aspect of this program is the development of an online portal to improve health literacy with modules on cancer, hypertension, heart health, addiction, diabetes, and influenza.
Colombia
In Colombia, government efforts aim to improve sources of health information, standardize health information and services, generate evidence (e.g. national health observatories in conjunction with analytic strategies), and share data through searchable databases. Mobile apps and interactive data tools were provided to increase access to health information and national health observatories were established to monitor health outcomes with the aim to help individuals access and apply information in self-care (36).
In 2017, recognizing a need to address antimicrobial resistance and the appropriate use of antibiotics, the Colombian Minister of Health, the Colombian Association of Infectious Diseases, and MSD Colombia agreed to promote the appropriate use of antibiotics through a health literacy campaign named ‘Twelve Commandments for Avoiding Antimicrobial Resistance’ (37). The campaign included a set of educational materials (video, infographics) that generated nationwide media attention and reached an audience of approximately 10,500,000 people. Phase II of the campaign focused on creating an alliance with the Colombian Hospitals and Clinics Association to expand outreach by sharing content on social media.
Peru
The Arts for Behavior Change Program, implemented in two shantytowns in Peru, combined music, dance, theater (Theater for Health), and visual arts with best practices of health literacy to reduce disease risk by improving personal and household hygiene (38). This program involved medical experts and team members with expertise in the arts, public health, health literacy, and communication. Participants learned about healthy practices at home and in the community to prevent disease and foster a healthier environment. Through direct testing in homes, statistically significant reductions in disease-causing microorganisms were seen in areas targeted by the performance messages.
Paraguay
Structured interviews in rural Paraguay examined factors influencing pregnant women’s maternal health literacy in a community-based prenatal care program (39). The program was taught in a common local dialect, and it measured maternal health literacy. Improvements in knowledge and health literacy were significantly greater for women who received services by personnel with formal healthcare training than from healthcare volunteers with less or no training. Improvements were also greater for those in housing with adequate water supply and lavatories. The study found that wider implementation of the community-based prenatal care program to people who have shown to be functionally illiterate in the standard national languages would increase maternal health literacy. They also concluded that maternal health literacy could be enhanced by additional training for healthcare personnel and improved social networking capabilities and resources for the community.
Chile
Patient-focused programs have been shown to be beneficial. Motivational interviewing is a patient-focused strategy that can support and assist people with examining and resolving opposing attitudes, ideas, and emotions (40). Uncovering a person’s motivation to change can increase awareness of potential problems, risks, and consequences. A motivational interviewing approach to improving oral health literacy is currently under evaluation among preschoolers and their caregivers in two disadvantaged urban areas in Concepción, Chile (40).
Brazil
Communication and health education on new media (e.g. infographics, videos, apps) can enhance health literacy. Infographics can be especially useful when language is a barrier. In Brazil, educational materials on chronic kidney disease incorporating infographics (41) and mobile health technology for prevention and control of obesity are under development, using the principles of health literacy (42).
Community leaders are important champions of health literacy and social mobilization. At the 9th Global Conference on Health Promotion held in Shanghai, China in 2016, many health literacy projects were presented. One project represented three indigenous communities in Brazil. In a collaborative effort between the Special Indigenous Sanitary District Cuiabá and the School of Public Health of the State of Mato Grosso, 20 students from villages in Chapada dos Guimarães, Poconé, and Cuiabá were trained in oral health, helping to reduce periodontal disease and cavities in their communities (43).
Health literacy policy recommendations
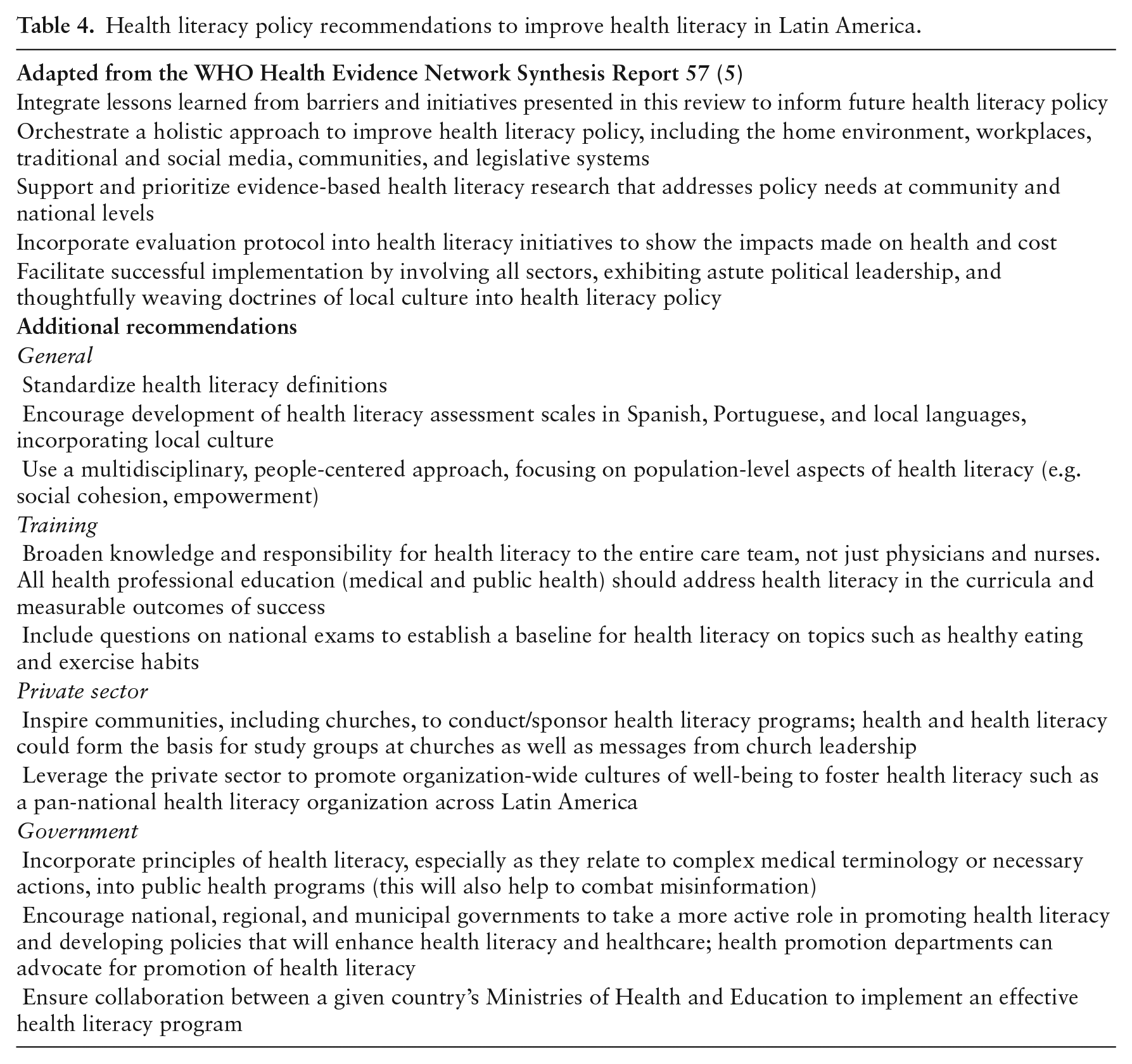
Latin America requires a comprehensive and integrative approach to improve health literacy. The aforementioned initiatives may serve as stepping-stones for future programs. Global organizations, such as PAHO, the International Health Literacy Association, the International Union for Health Promotion and Education, and the United Nations Educational, Scientific, and Cultural Organization, call for actions to improve health literacy in Latin America (6,44,45). In this regard, several policy recommendations pertaining to health literacy have been proposed: (see Table 4) (5).
Ensure that health literacy materials are available in common local languages and dialects
Combine health literacy assessment in resource-poor communities with initiatives to improve health and well-being
Challenge local communities and regional governments to identify individuals who can set an example and champion local health literacy initiatives (5)
Start education on health literacy as early as preschool and continue through university studies and beyond (5)
Motivate employers to make health literacy training available to their employees, as a healthier and happier employee is also a more productive employee
Assimilate health-literate messages through the media in print, radio, TV, and the internet to help improve community health
Include health literacy training in educational curricula and professional development
Health literacy policy recommendations to improve health literacy in Latin America.
Conclusions
Given the wide range of disparities and the burdens of communicable and non-communicable diseases in Latin America, improving health literacy has never been more important. Although there have been substantial advances in health resulting in part from economic and social development, poverty remains a significant barrier to health literacy, education, and health outcomes (1). Clinicians, educators, patients, patient advocates, caregivers, health authorities, churches, the private sector, and governments need to collaborate and take action to improve health literacy, enhance health, and lower costs. There is awareness of this need among former and current government officials, but it is not widely discussed or adequately addressed. While there is a desire to enhance health literacy, there is less awareness about how to do so.
Understanding the state of health literacy across Latin America and initiating the proposed recommendations are first steps toward improving health literacy and health. Additional research on health literacy’s impact on health outcomes in Latin America is warranted. While a variety of assessment tools have been employed (46), an overall assessment of health literacy in Latin America, similar to the health literacy survey in Europe conducted by the WHO Action Network on Measuring Population and Organizational Health Literacy, is recommended (47).
We are optimistic that these recommendations will increase awareness about health literacy, improve patient care, improve health, and lead to the development of health-literate policies that enhance well-being in Latin America.
Footnotes
Author contribution statement
All authors made substantial contributions to the conception/design of this work, drafting/revision of the work, have approved the final version, and agree to be accountable for the submitted work.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C. Gunther, R. Lopez, L. Myers, J. G. Quijada, and M. Vichnin are employees of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA and may hold stock/stock options in Merck & Co., Inc., Kenilworth, NJ, USA. K. Sørensen reports personal fees from Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA, outside the submitted work. A. Pleasant is an employee of Health Literacy Media based in St. Louis, MO, which is contracted for work by Merck & Co., Inc., Kenilworth, NJ, USA, Novartis International AG, Basel, Switzerland, and other pharmaceutical and health care organizations that are unrelated to this work. E. Arrighi, E. M. Ruiz de Castilla, F. Peres, and R. Mejía have no conflicts to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Medical writing and editorial assistance was provided by Churchill Communications (Maplewood, New Jersey). This assistance was funded by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, New Jersey.