
Abstract
Introduction:
Facilitating processes for coordinated action in the field of health promotion is a challenge. Poorthuis and Bijl’s (2006) Participatory Network Mapping Tool (PNMT) uses visualization and discussion to map the positions and roles of network actors, stimulate learning processes, and elicit actionable knowledge. This article describes the results from the application of the PNMT in networks of two Dutch health promotion programmes (Health Race and BeweegKuur) with the aim of determining the value of the PNMT to partners in health promotions networks.
Methods:
A qualitative secondary analysis (QSA) was conducted to clarify positions and roles, learning processes, and actionable knowledge of network actors in existing data sets including five group interviews of the Health Race programme and 16 individual interviews and 15 group interviews of the BeweegKuur programme.
Results:
The PNMT maps both positions and roles of (missing) actors and makes successes (e.g. knowing each other) and challenges (e.g. implementing new activities) visible. Thus, the PNMT provides a starting point for discussion and reflection and eliciting actionable knowledge such as involving new actors and target populations in the programme.
Conclusion:
The PNMT contributes to the facilitation of coordinated action in health promotion networks by making positions and roles of network partners visible. In combination with dialogue and reflection the PNMT helps to elucidate factors influencing coordinated action and outcomes. The PNMT is valuable in grasping intangible aspects between actors by stimulating collective learning. These insights can be used by researchers and network actors to achieve more successful coordinated action for health promotion.
Introduction
In health promotion, the increased need for coordinated action, or building and strengthening networks within the healthcare sectors (care, cure, and prevention) and between health and other societal sectors (e.g. welfare, social work, landscape and spatial planning), is more and more recognized (1). Coordinated action enables stakeholders to address main concurrent challenges in public health, such as non-communicable chronic diseases and ageing (1–3), and is defined by Nutbeam (4:14) as ‘a recognized relationship between (parts of) different sectors of society which has been formed to take action on an issue to achieve health outcomes in a way that is more effective, efficient or sustainable than might be achieved by the health sector acting alone.’
To initiate coordinated action, several preconditions have to be met, such as engaging network actors, nurturing relationships, and time to reach consensus on aims and roles (1). Moreover, in coordinated action, information sharing and collaborative learning processes (2) are involved. These are vital in realizing social change processes and other effects such as behavioural change or population health outcomes (1,3,5). To initiate and sustain networks, regular evaluation and feedback contribute to the visibility of achievements; this consequently contributes to collective learning processes and stakeholder enthusiasm (1,2,6). Evaluation methods and instruments facilitating reflection and learning processes that result in knowledge directly usable by stakeholders to tackle challenges (7) are helpful in coordinated action networks. Such so-called actionable knowledge is defined as propositions that make explicit causal processes, and that can be used by actors to implement effectively their intentions (8) and to achieve a better understanding of the factors influencing coordinated action and outcomes (9).
Several methods can be used to engage stakeholders in a network and to elicit (actionable) knowledge. In particular, there are methods that are used in group model building, known as a system dynamic process in which a researcher or expert gathers stakeholders together to elicit a model or system (10). Engaging stakeholders is crucial for capturing the required knowledge, increasing implementation changes from the results, and enhancing stakeholders’ learning processes (10,11).
An example of a method that fulfils this description is Poorthuis and Bijl’s network analysis tool (12), which has been further developed by Wielinga et al. (13) in the field of animal husbandry. Because this tool does not analyse a social network in the traditional way (14,15) but primarily facilitates and evaluates coordinated action by mapping positions and roles in the network performed by network actors themselves, usually facilitated by a professional or a researcher, we have renamed this tool as the Participatory Network Mapping Tool (PNMT). The tool is based on the free actors in networks approach, in which network actors focus on energy and connections to manage their networks (13). The tool enables network actors, by visualizing and discussing, to understand and explore their different positions and roles, such as partners, linkers (or brokers), suppliers, and users, thereby stimulating learning processes and eliciting actionable knowledge. Visualization of actors’ perceptions guides the discussion and analysis of roles. In the field of animal husbandry, use of the tool has resulted in flourishing networks (13).
Given its successes in animal husbandry, the PNMT (12) has been used to facilitate and evaluate coordinated action in health promotion networks in two Dutch health promotion programmes, the Health Race programme (Gezondheidsrace) and the BeweegKuur programme (or Exercise Therapy). In both programmes, local networks were developed, but they differ in aims and scale of implementation. The aim of this article is to study the value of applying the PNMT in health promotion networks and programmes.
Methods
To gain a comprehensive insight into the value of the PNMT (12), we conducted a qualitative secondary analysis (QSA). QSA is a technique for extending social work knowledge by using qualitative datasets that contain information hitherto untapped (16–18). We used existing datasets, originally collected for the purposes of two prior evaluation studies, the ‘parent studies’ (6,19). In our analysis, a new conceptual focus (18) was applied, meaning that concepts were re-examined to answer a new research question that emerges from, and fits with, the original data (20): what was the value of the PNMT to partners in health promotion networks in terms of clarifying positions and roles, stimulating learning and eliciting actionable knowledge?
Parent study I: Health Race
Health Race is a community programme implemented in the Dutch municipality Laarbeek (21,803 inhabitants), consisting of four villages in the south of the Netherlands. The aim of the programme was to raise awareness and encourage a healthy lifestyle among inhabitants. Health Race was initiated by two inhabitants in collaboration with Laarbeek municipality and the Municipal Health Service. In each of the four villages, a so-called Health Race team, consisting of 12 inhabitants (team partners), was established. Over a 9-month period, the four teams competed for the title of Laarbeek’s healthiest village.
The PNMT (12) was used to study positions and roles of actors in the Health Race network as part of the broader evaluation study carried out in 2012 (19). First, the two initiators of Health Race were interviewed, followed by four group interviews with each Health Race team, in total 15 team partners.
On the basis of the interview with the initiators, the researcher (EW) made a general visual map of the teams and their networks, describing all actors, their linkages, and their roles in terms of partners, linkers, suppliers, and users. The map was used in the four group interviews as a basis to discuss in-depth the composition and functioning of the team and the viability of the network. The researcher stimulated this by asking questions such as, ‘Are the right actors involved?’, ‘What roles do actors take?’, ‘Which roles are not represented?’, and ‘How does this work?’ The team partners adapted and completed the visual map and told the story behind the network.
Parent study II: BeweegKuur
BeweegKuur is a national lifestyle programme, launched in 2007 by the Dutch government and developed and coordinated by the Netherlands Institute for Sport and Physical Activity (NISB). The aim of the programme is to guide participants to achieve a healthy lifestyle and to transfer participants from primary care to local sports facilities to enhance and sustain physical activity behaviour. In 2010, NISB initiated the Building BeweegKuur Alliances project to better facilitate nationwide implementation of BeweegKuur (6).
The PNMT was used as part of an evaluation to study factors for building and sustaining BeweegKuur alliances, carried out between 2011 and 2013 (6). In the evaluation study, among other things, a phone interview was conducted with coordinators of 16 local alliances to obtain insight into alliance composition and to prepare for group interviews. Next, 15 group interviews were held with the partners of the same alliances, including the coordinators. One local alliance was not able to organize the focus group. From the interview with the coordinator, the researcher (MK) made a visual map of the alliance and its network. Next, this visual map was used and completed in the group interviews (in total, 69 alliance partners) to extensively discuss the composition and roles of the alliance actors. Questions asked were similar to the questions asked in the parent Health Race study.
Qualitative secondary analysis (QSA)
In the parent studies the interviews and group interviews were – with the interviewees’ permission – audiotaped and completely transcribed (intelligent verbatim style).
Visual maps of the Health Race networks were completed by EW and maps of the BeweegKuur networks were finalized by MK. The maps were compared for actors involved, actors’ roles, and linkages between actors. Based on discussion among the researchers, general visual maps representing both the Health Race teams’ networks and the BeweegKuur alliances’ networks were composed.
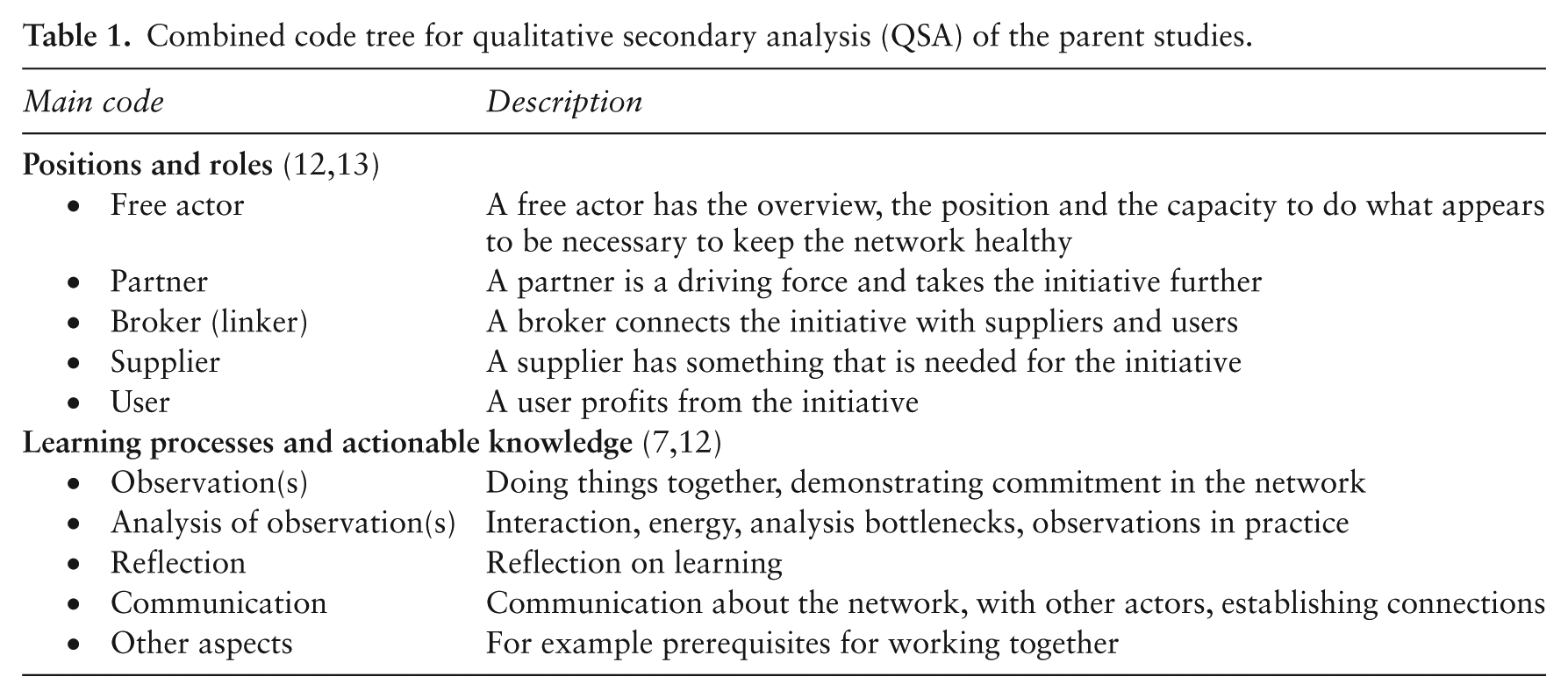
For the QSA, the data and analyses were re-examined by EW, AW and MH: EW was the main researcher of Health Race, AW was involved in both studies in the role of supervisor, and MH – not involved as a researcher in the parent studies – contributed to coding the data. Validity and objectivity could therefore be ensured (21) from both an insider and an outsider perspective. First, the code trees used in the parent studies were combined and merged by EW, AW and MH into one comprehensive code tree. Second, from this tree, codes were selected for this study and further operationalized and described, based on the promising features of the PNMT: positions and roles (12,13), and learning processes and actionable knowledge (7,12). Third, transcripts were re-examined to refine codes. This resulted in a code tree (Table 1). Codes of positions and roles overlapped to a great extent and therefore were merged. The same applies to codes of learning processes and actionable knowledge; these concepts follow on each other and are intertwined. EW recoded the Health Race data and MH the BeweegKuur data, using ATLAS.ti (version 6.2) for transparency. Findings were cross-checked and discussed with AW to reach consensus. Fourth, EW and AW summarized the results in line with the positions, roles, and aspects related to learning processes and actionable knowledge. Finally, the results and the value of the PNMT were formulated and reformulated until consensus was reached by all researchers. In the results, quotes are used to illustrate interviewees’ views.
Combined code tree for qualitative secondary analysis (QSA) of the parent studies.
Results
Positions and roles
The visual maps of the four Health Race teams’ networks were quite similar, as the teams were composed of 12 inhabitants including the initiators. Network actors represented the municipality and other organizations, such as sports organizations, schools, and local business associations (Figure 1). The visual maps of the BeweegKuur networks revealed two network types: the network chain, smaller networks in which mainly primary care professionals were represented, and the network strategy, broader networks in which other sectors were also represented (Figure 1).
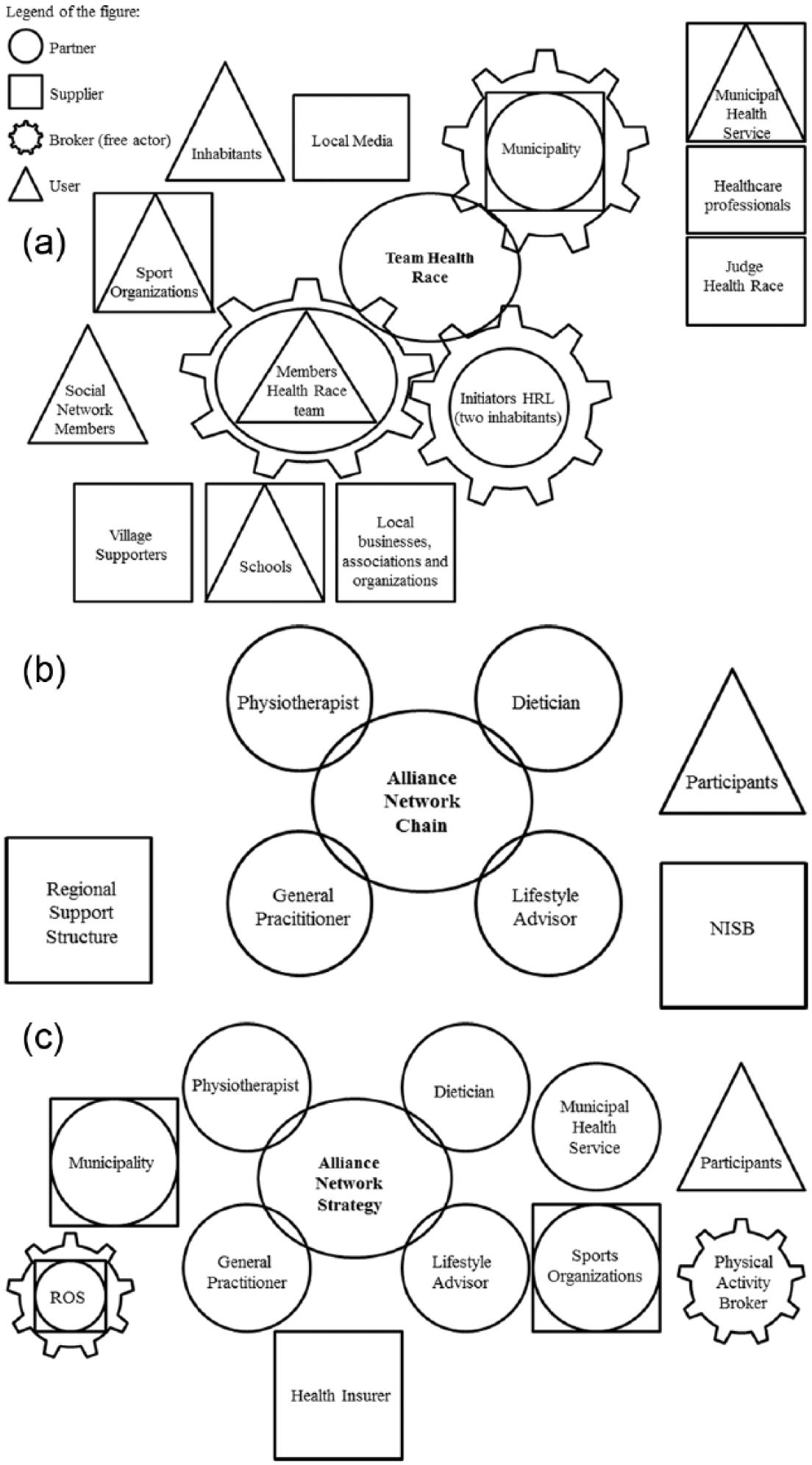
Visual maps of the Health Race network and the BeweegKuur networks: network chain and network strategy.
Actors often fulfilled multiple roles: partner and supplier or partner, supplier, and broker. An example was the municipality, having the role of both initiator and broker in the Health Race networks and the role of both partner and supplier in the BeweegKuur networks. At the same time, multiple organizations had similar roles. For example, in the Health Race networks, several grassroots organizations, local businesses, and local media fulfilled the supplier role; and schools, childcare, and sport organizations all fulfilled the user role. In the BeweegKuur networks, suppliers were mostly found in the field of health, for example healthcare insurers and the Regional Support Structure (ROS), and users were the enrolled patients.
In the Health Race networks, the initiators acted as brokers and ‘free actors’. Team partners viewed the initiators as ‘very important key-players’, a statement confirmed by the initiators.
We are brokers between the municipality and all the other organizations and Health Race teams. (Initiator, Health Race)
In the BeweegKuur networks, the broker role was often absent. In a few cases, the ROS fulfilled the broker role. In one network, a physical activity broker was appointed by the municipality, with the task of connecting different network partners.
The PNMT helped partners to discover that certain actors were missing from the network. In the Health Race networks, primary care professionals were often missing; in the BeweegKuur networks, several organizations were often not represented.
There are a number of organizations that we think need to be involved – the homecare organization, the municipal health service, and the welfare organization. Thus, actually, organizations that already function in the neighbourhood, but that have another focus. And we would like to link that more. (Municipal officer sports, BeweegKuur)
Learning processes and actionable knowledge
Reflection in the Health Race teams on the visual maps resulted in thinking about alternative ways to involve missing actors.
We are not able to motivate General Practitioners to collaborate with us in the Health Race (…). In order to improve something in the Health Race, maybe we should give the General Practitioners a certain role (…). They could fulfil a role in providing information and education to patients we don’t reach with our activities. (Initiator, Health Race)
Based on this (actionable) knowledge, partners agreed to undertake action by contacting these missing partners. For example in the BeweegKuur, the PNMT resulted in the intention to engage these missing partners in the alliance.
Also, partners realized that certain sub-populations were not reached and therefore new activities were being implemented.
With the ‘Dining and Walking’ activity we tried to reach as many people as possible. This was really difficult…but well…we have tried through schools and through advertisements. We did reach a lot of people, who participated in the activity, except teenagers. Teenagers were under-represented. Therefore we approached [name organization]. And we intend to organize activities with this organization. (Partner, Team 4, Health Race)
Dialogue and reflection helped partners to recognize factors that positively influenced coordinated action, such as getting to know one another and being open to people from different backgrounds.
Actually we are all put together, like well you all do your own thing and find some way and there’ll be something nice when you work together. I didn’t expect all this [successful coordinated action]. I think that’s very nice. BeweegKuur evoked something like ‘let go of your own background.’ You meet new people who are also doing something, all have joint problems, and I think that’s also the recognition that we all have. (Partner, Alliance 4, BeweegKuur)
Dialogue and reflection also helped partners to elicit what works and why, and also what does not work.
How do we establish connections between different actors? I think by bringing people in contact with each other and keeping them informed about things that are important for them. There has to be some kind of shared interest among actors in order to connect them. (Partner, Alliance 11, BeweegKuur) At first we thought we should put everything pretty strictly on paper, but that interferes with other people getting over the threshold. (Partner, Alliance 3, BeweegKuur)
Partners preferred face-to-face communication within the team or network and with new actors or organizations. A more personal approach helped to achieve coordinated action, because ‘it is more effective’. When contacts had been established, phone and email were often used.
Although the PNMT stimulated the network partners to reflect upon their learning processes, this learning process itself was described vaguely. Partners recognized that the network is an organic whole and that learning takes place by trial and error.
It’s just growing and developing, there is no one who says how to do it, which I think everyone also likes very much. It is just doing and experimenting and occasionally launching ideas that ultimately do not seem to work. (Partner, Alliance 3, BeweegKuur)
Overall, partners appreciated using the PNMT to stimulate dialogue about the network and stimulate learning processes.
Indeed, there are learning points. When I started with those questions, like when did the alliance start? What is the aim of the alliance? I think those are questions you need to discuss again, and also the role and task division (…). We really should do this more. (Partner, Alliance 8, BeweegKuur)
Discussion
In this paper, we described the value of the PNMT to partners in health promotion networks in terms of clarifying positions and roles, stimulating learning, and eliciting actionable knowledge. We presented results based on QSA of data from two health promotion programmes.
Using the PNMT revealed qualitative data about the positions and roles of actors in the networks. This in turn helped partners to recognize actors missing from the network and target groups not being reached, as well as factors important for coordinated action such as knowing each other well and personal communication.
Valuable characteristics of (applying) the PNMT to partners in the Health Race and BeweegKuur programmes are: (i) its visual presentation, (ii) its ability to make successes of coordinated action visible, and (iii) its value when used in combination with other methods.
The visual representation of the network was helpful for both partners and researchers in gaining insight into positions and roles of network partners. Our results match the study of Vennix (10) who reports that mapping or qualitative modelling, among other things, helps to keep track of complex structures, increases the group’s information capacity, and aids reflection and dialogue (10). This contributed to partners’ understanding of actors’ positions and roles. This in turn made upcoming challenges explicit, such as engaging new actors and implementing new activities. The literature confirms that the use of visual instruments in combination with the encouragement of network partners’ active participation has the potential to reframe the problems being investigated and encourage mutual learning on the part of researched and researcher alike (2,22–25). Evidence from social network analysis also indicates that network-informed programmes are more effective than non-networked ones (26).
The use of the PNMT in the two Dutch programmes made successes of coordinated action visible by enabling partners to generate insights that are difficult to capture, such as the fact that the partners liked the programme, the partners got to know one another better, and they learned as a network during the programme. Lorenz and Kolb (22) and Guillemin (27) suggest that grasping these intangible aspects and bringing out information that otherwise would remain hidden (e.g. positive emotions) can contribute to a better understanding of the wider context of the network and facilitate knowledge integration among network actors (22,27). Thus, the results of our study show that the PNMT contributes to communication and reaching agreement between actors, and supports individual and coordinated action in the network, as is also underlined by others (28–30).
The PNMT, when used in combination with other methods such as interviews and focus groups, is valuable for researchers and network actors in gaining a rich understanding of the strengths (e.g. successes) and weaknesses (points to improve) of aspects of coordinated action (e.g. communication strategies) in the network. The PNMT supported the partners by facilitating dialogue, reflection, and evaluation based upon in-depth questions (e.g. actors’ roles and ways of collaborating) (18). The integration of the different network partners’ understandings was thereby stimulated and resulted in a shared body of knowledge on the network. Consequently, network actors were stimulated to take action. Experience from other projects (28) also stressed the value of actors using tools in combination with other methods to interpret data and take action, because the methods complement and reinforce one another. Although actionable knowledge was elicited in this study, it is not known what further actions have been undertaken by the partners and whether this contributed to the improvement of coordinated action. To study this, coordinated action in networks needs to be monitored for a longer period of time, which was not part of this study and neither of the parent studies.
The deep involvement of the actors justifies presenting the PNMT as a group model building method, rather than a network analysis, as suggested by its original name (12). Nevertheless, in the field of social network analysis also, (quantitative) network measures can be used to facilitate coordinated action by collecting and analysing data during the implementation stage (26). In our parent studies, we used the PNMT as part of an evaluation study. Stimulating learning processes was not the primary focus of these studies. Therefore, in order to benefit most from the PNMT as a group model building method, it is recommended to integrate guiding principles and facilitating tips, as provided by Vennix (10) and Hovmand (11), more comprehensively.
Strengths and limitations
We used QSA in a systematic way to describe valuable characteristics of (using) the PNMT to analyse data from two Dutch programmes. The reliability of the data interpretation was enhanced by several researchers analysing Health Race data and BeweegKuur data in a similar way and checking interpretations. Nevertheless, three issues, which were out of our control for this study, could possibly have influenced our original data: (i) social desirability, (ii) other developments in the network, and (iii) the way in which the PNMT is used in teams or alliances. First, in the parent studies (6,19), the network partners may have been influenced by the research context and/or other actors, and given socially desirable answers. Second, other developments (e.g. changes in collaboration between healthcare, cure, and health promotion) outside the network were not taken into account and could have influenced the collaboration between the network actors. Third, we chose two different health promotion programmes that both used the PNMT in a similar way. In both programmes, Health Race and BeweegKuur, the PNMT was (only) conducted with partners: teams in Health Race and alliances in BeweegKuur. In both programmes, the entire network was much greater and involved also other actors such as the municipality, healthcare professionals, and sport organizations (see Figure 1). The fact that these actors’ perspectives were not included might have impaired the completeness and accuracy of the entire networks’ structure and functioning. This point relates to the questions posed in group model building: ‘who should be involved?’ and ‘how many people should be involved?’ (11).
A last remark about our study is that the PNMT was performed only once. In order to assess the use of actionable knowledge and social change processes over time, it is recommended to use the PNMT multiple times. More generally, there is scope for studying the impact of the PNMT in comparison with other (group model building) methods, in order to understand when each method is most appropriate (30). As such, the PNMT might also be useful as an evaluation tool to assess coordinated action over time.
Conclusions
The PNMT is relevant for the facilitation of coordinated action in health promotion networks by making positions and roles of network partners visible. This, in combination with dialogue and reflection, helps to elucidate factors influencing coordinated action and outcomes. The PNMT is valuable in grasping intangible aspects between actors by stimulating collective learning. These insights can be used by researchers and network actors to achieve more successful coordinated action for health promotion.
Footnotes
Declaration of Conflicting Interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.