
Abstract
A non-profit organization was formed in 2009 by lay citizens of Nagahama, Japan in response to a community-based genome-epidemiologic study, the ‘Nagahama Zero(0)-ji Prevention Cohort Project (N0PCP)’. This organization aims to promote health by taking advantage of citizens’ social networks. The Ottawa Charter for Health Promotion affirms the importance of creating supportive environments and coordinating social relationships. Supportive environments (infrastructure) and social relationships (resources) work together as aspects of social capital. This study sought to examine the association between self-rated health and social capital, at both individual and neighborhood levels, and to discuss suitable health promotion strategies for local circumstances.
A cross-sectional survey was conducted in 2011, using a self-administered postal questionnaire. Social capital indicators included aspects of support in the environment (social support, neighborhood connectedness, informal social controls, neighborhood trust, general trust, and attachment to place) and social relationships (number of activities; participation in neighborhood activities; participation in recreational activities; and social leverage regarding physical health, mental health, and acquisition of health information). Neighborhood-level social capital was calculated as the percentage of individuals in a neighborhood in the ‘high social capital’ category. At the individual level, participation in recreational activities, high general trust, and discussion regarding mental health problems with family members were associated with self-rated health positively, whereas discussion of mental health problems with acquaintances had a negative correlation. At the neighborhood level, a highly supportive environment did not contribute to good health, whereas aggregated attachment to place had a positive correlation. There were no significant inter-regional health differences.
The results of this study suggest that health promotion activities should aim at promoting the formation of empathetic friendships through individual networks, based on bringing individuals who need support to compatible places. Attachment to place should be incorporated into activities as an important and effective tool.
Keywords
Background
In his book Bowling Alone, Robert Putnam writes, ‘Americans have had a growing sense at some visceral level of disintegrating social bonds’ (1). Many Japanese citizens might agree with Putnam’s description of a sense ‘that something bad has been happening in their community and in their country’ (1). In Japan, 42.9% of people aged 60 years or older regard ‘an unattended death’ as ‘a familiar problem’ (2). In addition, 29.8% of 15-year-olds in Japan report feeling ‘lonely’, which was the highest percentage in the world (3).
According to Putnam, the importance of social connectedness is more prominent in the context of health and well-being than in other domains. In his book, Putnam quotes an article by Kawachi et al. (4), reporting the results of a survey of approximately 17,000 people in 39 states in the US. According to the results of this study, states in which more residents assessed their self-rated health as medium or bad also had more residents who indicated that they could ‘generally not trust others’. The latter is one of the commonly used indexes of social capital. Kawachi et al. also found that people in regions characterized by a generally lower atmosphere of trust had significantly worse views on health than those in areas characterized by a greater sense of trust. These differences were statistically significant, even after adjusting for variables at the individual level. Since the article was published, the association between social capital and health has attracted the attention of researchers, and additional evidence has accumulated recently (5).
According to Kawachi et al. (6), two distinct conceptions of the term ‘social capital’ appear in public health research. The social cohesion school typified by Putnam defines social capital as a contextual effect on individuals, conceptualized as the resources available to members of a social group (e.g. trust, norms, and the exercise of sanctions). In contrast, network analysts define social capital as the resources embedded within individuals’ networks that people can access through those networks (e.g. social support, information channels, and social credentials). Kawachi et al. (6) tentatively conclude that social capital should be conceptualized in terms of social cohesion and resources embedded in networks. Moore et al. (7) examine this conclusion further in a citation-network path analysis of public health articles on the topic of social capital. They argued that, at the time that Kawach et al. (4) published their study, discussions of social capital in public health research had been placing disproportionate weight on the social cohesion interpretation, thereby marginalizing network approaches to social capital. Moore et al. (7) suggest that, because social capital is a composite of psychosocial and material elements, social network approaches are likely to provide many tools that could be used to encourage the development of public health research.
Few empirical studies have used concepts from both the social cohesion school and network analysts. Carpiano (8) provides a brief review of the social capital conceptualizations of the network analyst Pierre Bourdieu, alongside those of Putnam and the social cohesion school. In his review, Carpiano (8) explicitly draws upon Bourdieu’s social capital theory to consider neighborhood effects on health. He further proposes a conceptual model of social capital, based on Bourdieu’s concept, consisting of four aspects: social support – the form of social capital upon which individuals can draw in order to cope with daily problems; social leverage – the form of social capital that helps residents access information and advance socioeconomically; informal social control – the ability of residents collectively to maintain social order and keep the neighborhood safe from criminal and delinquent activity; and neighborhood organization participation (9). Social cohesion (from Putnam’s concept) consists of two aspects: connectedness and value. Carpiano’s term social cohesion refers to the same concept that the social cohesion school defines as social capital, and Carpiano terms the underlying causes structural antecedents. Ziersch (10) conceptualizes social capital as ‘the social infrastructure, such as networks and values, that facilitates the exchange of social resources between individuals (SCI), and the sum of resources available to those individuals through this infrastructure (SCR).’ Ziersch further explores the relationship between the elements of SCI and SCR, and physical or mental health.
The Ottawa Charter for Health Promotion (11) affirms the importance of coordinated action by all concerned, as well as the importance of mediation between differing interests within society, for the pursuit of good health. To accomplish these goals, building social relationships is necessary within diverse communities to help citizens meet their needs. The Ottawa Charter also emphasizes the creation of supportive environments, in which people take care of each other and their natural environment, thereby empowering the community. Citizens’ ownership and control of their own endeavors thus lies at the heart of the health promotion process. It could be argued that social relationships closely resemble Ziersch’s concept of SCR (or even those of the network analysts), and that supportive environments resemble Ziersch’s concept of SCI (or even those of the social cohesion school).
In 2005, the Kyoto University Graduate School of Medicine established an agreement with the city of Nagahama in Shiga prefecture to initiate the Nagahama Zero(0)-ji Prevention Cohort Project (N0PCP), for promoting the health of citizens and developing community-based genome-epidemiology studies. Nagahama, which has a population of about 125,000, is located about 60 km northwest of Kyoto, the ancient capital of Japan, and it faces Biwa-ko, the largest lake in Japan. Owing to its long history and rich natural environment, Nagahama thrives on tourism. Between 2008 and 2010, 10,084 citizens (14% of eligible people aged 30–74 years) participated in the N0PCP program. A non-profit organization (NPO) of lay citizens, the Health Promotion Zero-ji Club (hereafter, the Zero-ji Club), was inspired by the N0PCP program. The Zero-ji Club’s mission is to ‘bridge people by taking advantage of their connections, and promoting the physical and mental health of citizens’ (12). We can therefore examine the extent to which the Zero-ji Club applies the philosophies of the Ottawa Charter.
As observed by Moore et al. (7), almost all Japanese studies of the relationship between social capital and health (13 –20) apply the definition conceptualized by the social cohesion school. As scale items of social capital, many scholars have examined neighborhood trust (16,19,20) or general trust (15,17), and participation in various types of local activities, classified according to whether the group is homogeneous or diversified and whether it is egalitarian or hierarchical (13,15,16,18 –20). Few, if any, studies refer to resources embedded in social networks, thus limiting our ability to examine their evidence in the context of health promotion activities.
According to the Ottawa Charter, both aspects of social capital are necessary for health promotion. The purpose of our research is therefore to examine which items of supportive environment, social relationships, and structural antecedents are associated with residents’ perceived health and how these items can be made suitable for inclusion in strategic health promotion plans on the basis of local circumstances.
Methods
Participants and setting
A cross-sectional survey was conducted in November 2011 using a self-administered postal questionnaire. The sample consisted of 3448 Nagahama residents who had participated in the N0PCP and who had expressed agreement with the Zero-ji Club mission. All participants were registered members of the Zero-ji Club, and their names and addresses were available. A linkable anonymization method was adopted to contact members who had expressed their intention to participate in the activities of the Zero-ji Club in the future. More specifically, the researcher had ID numbers and data, with no names or addresses, and the Zero-ji Club had directory-ID pairs, with no other data. The questionnaire packet included a briefing paper about the study and instructions for completing the questionnaire. The return of the questionnaire was viewed as implied consent. Participants were asked to provide their postal codes, which were classified into 28 school districts, considered as neighborhood units. In Japan, political or historical areas are customarily classified according to school districts, and some Japanese studies of the relationship between social capital and health have used school districts as units (8,12,13,15). In Nagahama, the Citizen Autonomy Act in 2006 provided for the establishment of Community Renovation Conferences in each local community hall (about one per school district). The duties of these facilities include health promotion. In the future, it might be possible to share information and collaborate with them to develop activities. The study protocol was reviewed and approved by the Ethics Committee of the Kyoto University Graduate School and Faculty of Medicine (E-1044).
Measures
Social capital
Based on Carpiano’s model (6,7) and according to a previous study (21), the members of the Zero-ji Club, staff members of the Nagahama City Health Promotion section, and researchers, adopted six items as indicators for supportive environment (social support, neighborhood connectedness, social control, neighborhood trust, general trust, and attachment to place) and six items as indicators for social relationship (number of activities, participation in neighborhood activities, participation in recreational activities, social leverage about physical health, social leverage about mental health, and social leverage for acquisition of health information). All items were dichotomized as either ‘high social capital’ or ‘low social capital’. The items used to create these measures are displayed in Table 1. Neighborhood-level social capital was calculated as the percentage of individuals in a neighborhood who were categorized as ‘high social capital’.
Measurement items and scale coding for social capital variable.
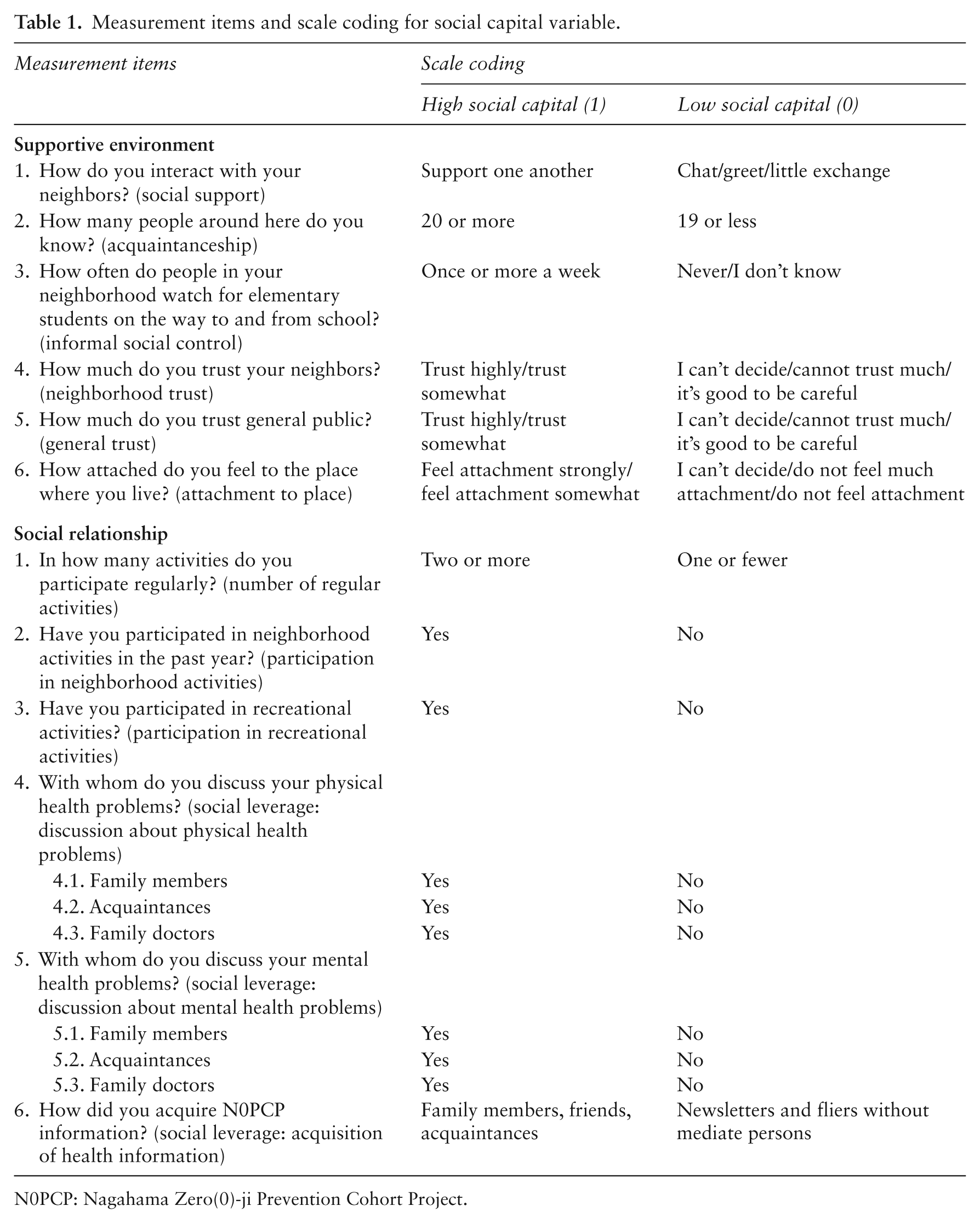
N0PCP: Nagahama Zero(0)-ji Prevention Cohort Project.
Self-rated health
The following question was used to measure the dependent variable of self-rated health: ‘How do you rate your current physical health status?’ Respondents answered along a four-point Likert scale (1 = very poor, 2 = poor, 3 = good, and 4 = very good). The variable was dichotomized as ‘poor self-rated health’ (response of 1 or 2) or ‘good self-rated health’ (response of 3 or 4).
Individual factors
Respondents were asked to provide information concerning their age, sex, employment status, family structure, and whether they had ancestors from Nagahama. Employment status was dichotomized as ‘employed’ and ‘unemployed’. Family structure was divided into four categories: ‘three or more generations living together in the family home’, ‘two-generation family’, ‘one-generation family’, and ‘living alone’.
Neighborhood structural antecedent factors
The structural antecedents considered in this study consisted of population density, population increase over 30 years, proportion of people over 65, homeownership rate, household unemployment rate, proportion of people having completed more than 12 years of formal education, and proportion of people who had not relocated since birth. These data were compiled for every school district using the Japan National Census 2010, subregion block (22). For reference, we counted average income in areas larger than school districts, supplementing missing data with information from the Municipality Economic Account, as the average income of subregions is not announced officially in Japan.
Analyses
To identify individual factors associated with health, we analyzed the data using SPSS Version 19.0. Chi-square tests were used to examine associations between items. Logistic regression analyses were used for items with significant effects on self-rated health. To identify neighborhood factors associated with health, we examined correlation coefficients between items at the neighborhood level. We applied structural equation modeling using Amos version 20.0 to generate a model of the relationships between neighborhood factors and health. We assessed significant differences in health among neighborhoods using the one-way analysis of variance.
Results
Of the 3448 questionnaires distributed, 15 were returned unopened because of unknown addresses, and 2124 were returned (response rate: 61.9%). We excluded 33 questionnaires that did not mention postal codes. Because our study aims to research relationships between health and regional characteristics, answers without postal codes were unusable. Missing data for most other items were negligible (≤2.0% for all variables). Our analyses are thus based on data from 2091 questionnaires.
The demographic and social capital characteristics of all participants in the study are shown in Table 2. Females constituted 64.9% of the participants, almost exactly reflecting the rate of females’ participation in the N0PCP program (66.9%). People in their 30s (5.6%) and 40s (7.6%) were underrepresented, relative to the participants of the N0PCP, and people in their 60s (46.3%) and 70s (21.1%) were overrepresented. More than 25% of the participants were living in families consisting of three or more generations, thus constituting more than twice the national average (10.9%). Almost 80% of the participants had ancestors from Nagahama.
Individual characteristics of respondents (n = 2091), Japan, 2011.
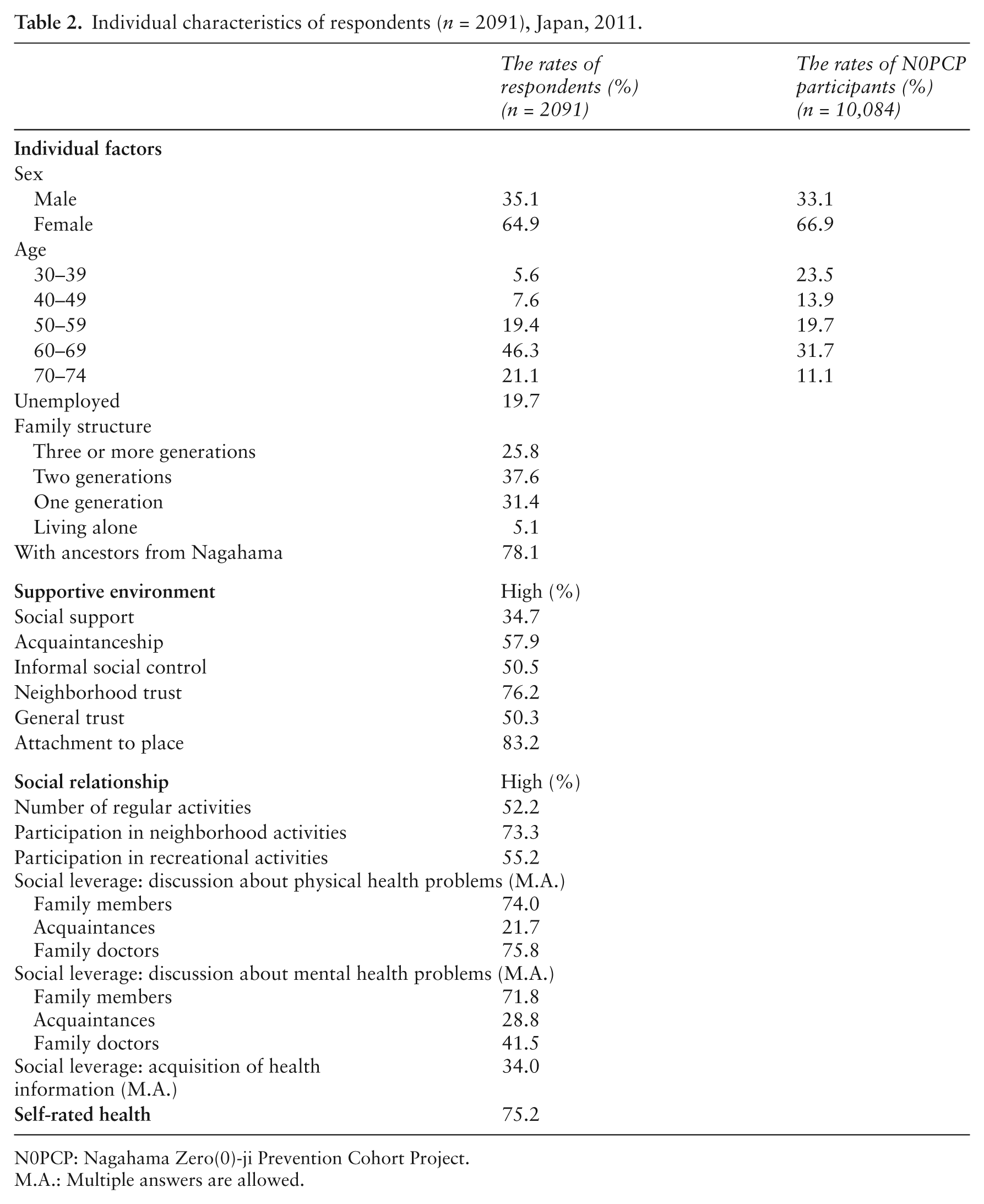
N0PCP: Nagahama Zero(0)-ji Prevention Cohort Project.
M.A.: Multiple answers are allowed.
With regard to social capital aspects relating to supportive environment, one-third of the respondents indicated that they support each other in various aspects of life, and more than 50% reported having more than 20 acquaintances in their neighborhoods. The majority of respondents (76%) expressed trust in their neighbors, and 53% expressed trust in the general public.
With regard to aspects related to social relationships, more than 50% reported participating in more than one voluntary activity, 73% participated in neighborhood activities, and 55% participated in recreational activities. The majority of the respondents (74%) reported discussing their physical health problems with their family members, 22% with their acquaintances, and 76% with their primary-care doctors. With regard to mental health problems, 72% discussed these problems with their family members, 29% with their acquaintances, and 42% with their primary-care doctors. More than one-third of all respondents had acquired information on the N0PCP program from their family members, friends, or acquaintances.
As stated above, we dichotomized self-rated health into ‘good health’ (combining ‘very good’ [20.5%] and ‘good’ [54.7%]) and ‘poor health’ (combining ‘poor’ [22.0%] and ‘very poor’ [2.8%]). We conducted chi-square tests to examine relationships between social capital factors and self-rated health at the individual level. We found no significant associations between self-rated health and any of the individual background factors (age, sex, family structure, employment status, and having ancestors from Nagahama).
The factors having significant associations (p < 0.05) with self-rated health are displayed in Table 3. We used these factors to conduct multivariate logistic regression. Three of the factors (trust in the general public, participation in recreational activities, and discussion with family members about mental health problems) had positive associations with individual health. Discussion with acquaintances about mental health problems was negatively correlated with individual health.
The relationship between self-rated health and social capital factors, at the individual level.
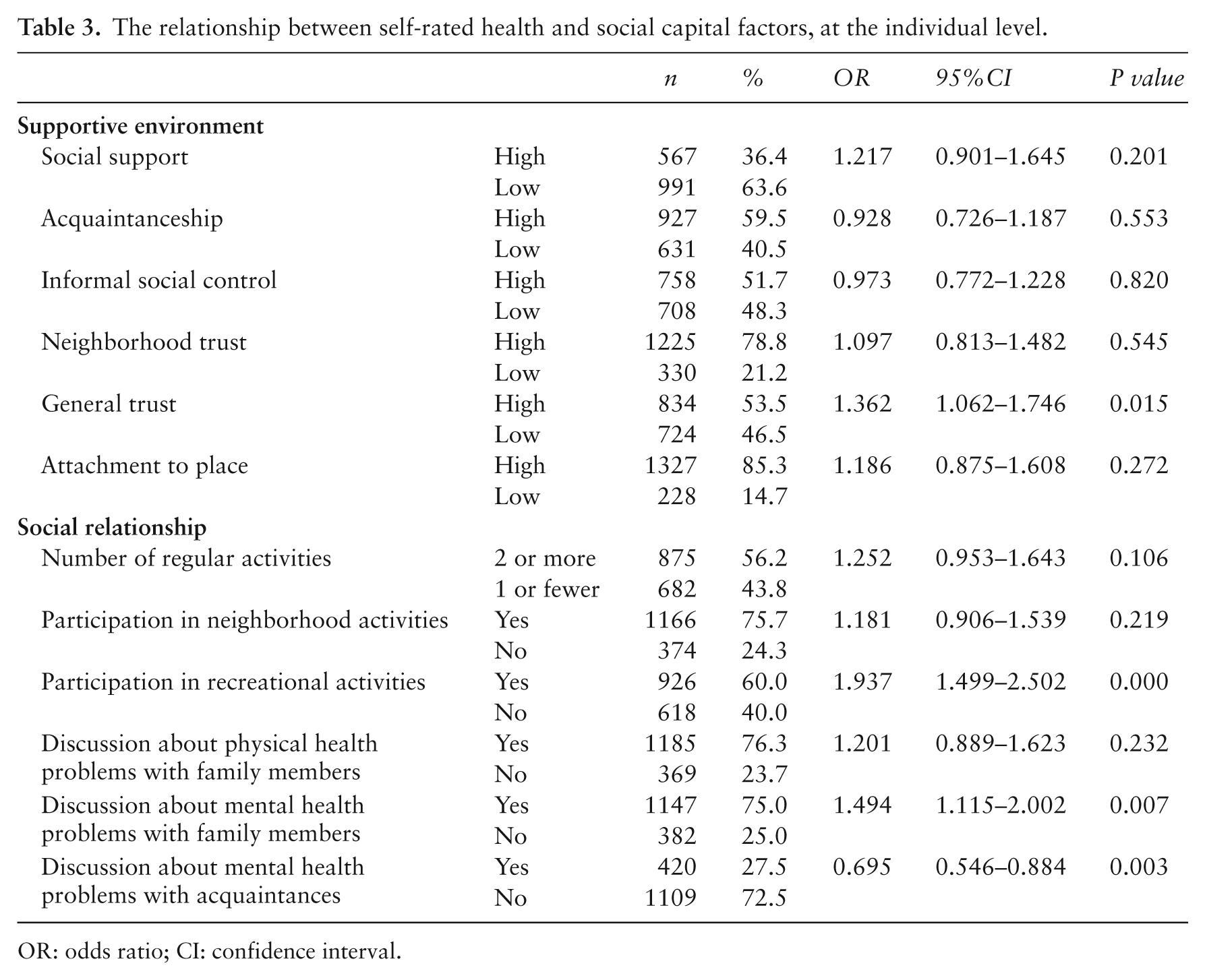
OR: odds ratio; CI: confidence interval.
Neighborhood characteristics are displayed in Table 4. Two groups of three items exhibited high mutual correlations. The first group consisted of the proportion of people over 65, homeownership rate, and proportion of people who had not relocated since birth. The second consisted of population density, population increase over 30 years, and proportion of people having completed more than 12 years of formal education.
Neighborhood characteristics (n = 28).
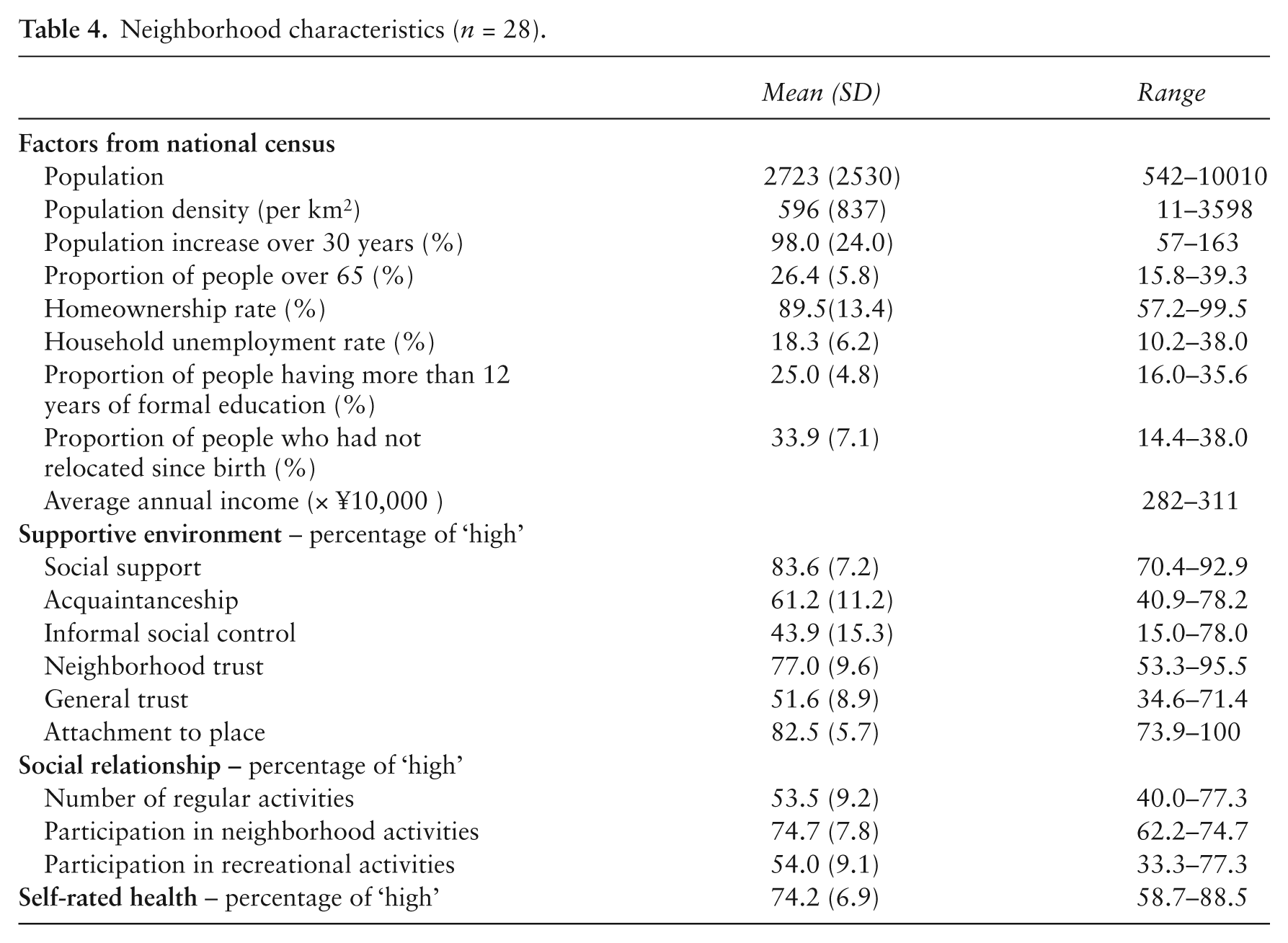
Neighborhood characteristics (n = 28). The first group of items was used to create a traditional-region index (Cronbach’s alpha = 0.88), and the second group was used to create an urban-region index (Cronbach’s alpha = 0.80). Correlation coefficients between social capital factors and self-rated health at the neighborhood level are displayed in Table 5. The traditional-region index exhibited a high correlation with social support, neighborhood connectedness, and neighborhood trust (aspects of supportive environment), as well as with neighborhood activities (an aspect of social relationships). The urban-region index exhibited a low correlation with social support, neighborhood connectedness, and neighborhood trust. Good self-rated health was highly correlated only with attachment to place, which exhibited no correlation with any other factors.
Bivariate correlations at the neighborhood level (n = 28).
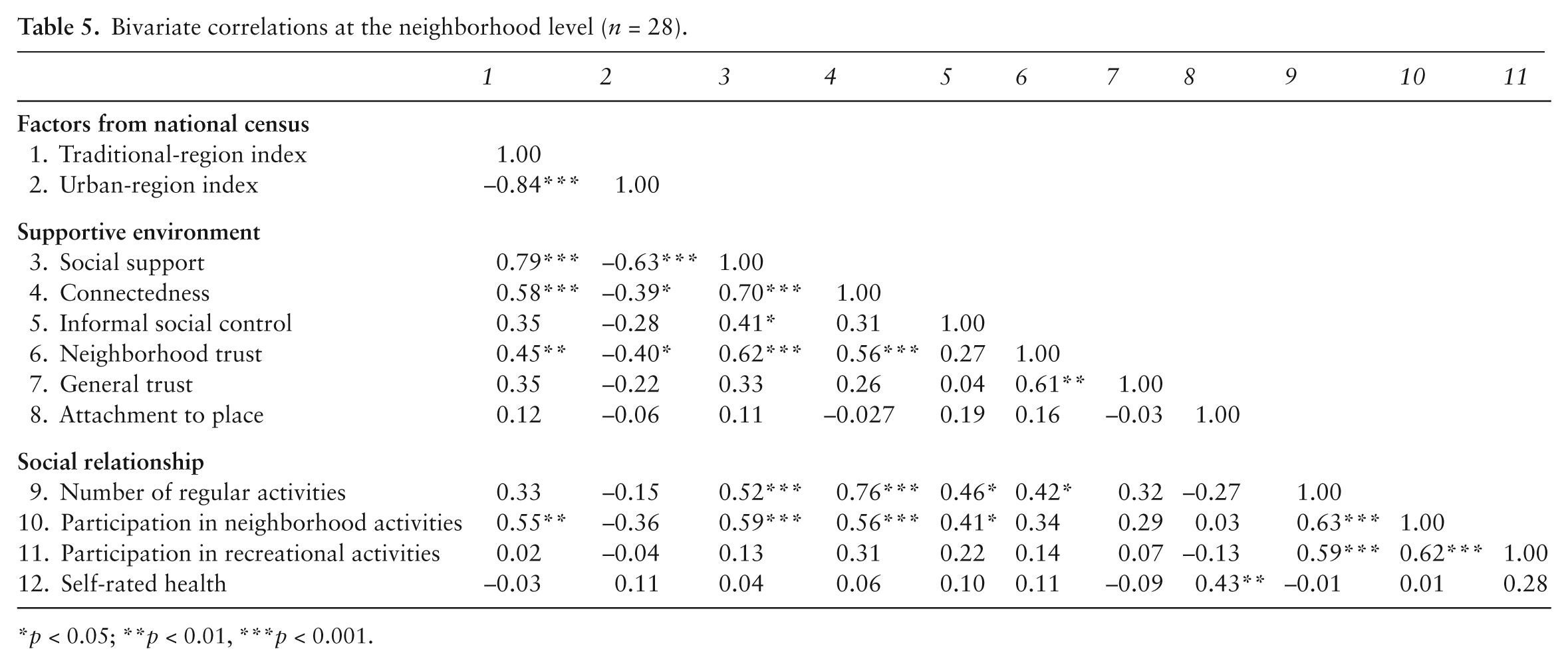
p < 0.05; **p < 0.01, ***p < 0.001.
We used structural equation modeling to examine the relationship between social capital and self-rated health at the neighborhood level. The model had a good to acceptable fit (GFI > 0.9), as shown in Figure 1. High levels of social support, neighborhood connectedness, and neighborhood trust (aspects of supportive environment) correlated with neighborhood structural antecedent factors, but they did not affect self-rated health. High levels of participation in neighborhood activities (an aspect of social relationships) were negatively correlated with self-rated health. Attachment to place and recreational activities did not correlate with any of the neighborhood structural antecedent factors, although they were positively correlated with self-rated health. One-way analysis of variance revealed no significant differences among neighborhoods with regard to neighborhood health. The intra-neighborhood correlation coefficient (ICC) of self-rated health was 0.00%.
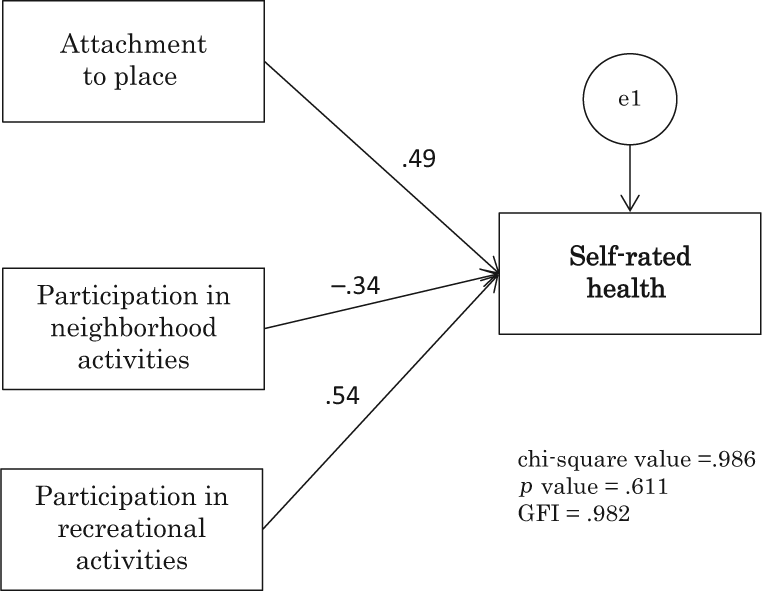
Measurement model for self-rated health and social capital at the neighborhood level. All paths are statistically significant at p < 0.05.
Discussion
In this study, we examined the relationship between self-rated health and social capital, which consists of supportive environment (as social infrastructure) and social relationships (as resources embedded within individual networks). The goal is to provide lay citizens with strategies for health promotion activities suitable to their own individual cases.
According to our results, participation in recreational activities, general trust, and discussion about mental health problems with family members are positively correlated with individual self-rated health, whereas discussion about mental health problems with acquaintances is negatively correlated with health. In traditional regions, people support each other, have many acquaintances, and share mutual trust in the neighborhood, although these factors are not correlated with good health. Greater participation in the neighborhood community is associated with poorer health at the neighborhood level, whereas greater attachment to place is associated with better neighborhood-level health. Owing to large intra-regional variances, we found no significant inter-regional health differences.
The very competence of family members who provide an infrastructure for discussing mental health but not physical health might contribute to good individual self-rated health. This is consistent with the network analysts’ view of resources ‘embedded within an individual’s social networks’ (23). In a study conducted in Norway, Gele and Harsløf (24) report that having someone to talk to when an individual is distressed is the best predictor of good health. The authors further suggest that the quality of the network that provides necessary support is more important than the frequency of contact (consistent with ‘bonding social capital’, which is characterized by strong relationships between people with equal social standing). There are no significant differences in self-assessed health between people with and without bridging social capital as characterized by complex contacts between people from different social environments. Nevertheless, ‘counting one’s medical doctor as one’s friend’ is an important factor for good health (consistent with ‘linking social capital’, which is characterized by contacts between people from different social positions of formal authority) (25). It is actually more important for useful resources to be embedded within connections than it is for these resources to take specific forms.
It would seem logical for people to try to maintain their health by talking to others about their mental health. According to our results, discussing mental health with family members is positively correlated with individual health and discussing mental health with acquaintances is negatively correlated with individual health. As reported by Melchior et al. (25), the functional aspects of social relationships are more important to health compared with structural aspects, and a lack of social support serves as a stressor, thus contributing to poor health on its own. Japan has very few psychological counselors, and there is only one psychological counseling facility in Nagahama. Therefore, very few people use counseling on a regular basis. They are more likely to discuss their mental health situations with people who are close to them. One possible explanation is that the lack of family support for mental health problems contributes to poor health, and that unhealthy people may discuss their problems with acquaintances as substitutes for family members, who are usually expected to be more empathetic. We further found no significant differences in self-rated health between those who opt to consult with physicians and those who do not. The situation might be affected by the fact that because of Japan’s universal health insurance coverage everyone has access to doctors.
Harpham recommends measuring social capital according to cognitive aspects, which relate to how people feel (e.g. trust, values), and according to structural aspects, which relate to what people do (e.g. participation, associational links), as the two types of factors are likely to influence health through different mechanisms (6). According to our findings, individual health is associated with trust in the general public, but not with trust in the neighborhood (cognitive aspects), as well as with participation in recreational activities, but not with participation in neighborhood activities (structural aspects). We found no significant differences between neighborhoods with regard to either general trust or participation in recreational activities, and the presence of a supportive environment within a school district was not associated with self-rated health.
In an ethnographic study of social connection based on Bourdieu’s social theory, Stephens (26) clarifies that the neighborhood is neither the main source of social connections nor the basis of social capital. Stephens (26) further suggests that competition for resources is an activity shared by all citizens across the range of communities. These observations are supported by our finding that there are no significant differences in terms of self-rated health between traditional regions, which maintain supportive environments, and urban regions, which do not. In fact, neighborhoods may be no longer the basis of resources. If resources are lacking within the community, people can easily seek them outside the community. Moreover, they are likely to be connected with people around the world through the Internet.
At the individual level, having family members with whom to talk during periods of distress is associated with good health. At the neighborhood level, heart-warming neighborhoods are not sufficient to make someone healthy, although relatively exclusive communities outside neighborhoods (e.g. recreational activities in which people with the same interests and values participate) can promote health. In a study of the relationship between social capital and health in a Japanese suburban area, higher district-level mistrust in neighbors was associated with higher self-rated health (19). As viewed from the perspective of network theory, regions in which many residents participate in communities other than the actual neighborhood may be resourceful and vigorous. If resources require effort to obtain, rather than being distributed automatically, this might make people uneasy and cause them to feel ‘that something bad has been happening in their community’ (1).
In many reports of the association between social capital and health, social capital has been suggested to provide a buffer for social divisions (27). Islam et al. conclude tentatively that neighborhood characteristics do not play a significant role in explaining health disparities in egalitarian countries (e.g. Scandinavian countries, the Netherlands). As areas become less egalitarian, however, social capital plays a more important role as a buffer. Japan is a moderately egalitarian country, with a Gini coefficient of about 0.3. The tentative conclusion of Islam et al. (27) is supported by the results of a nationwide survey of Japan (ICC: 5.8), which reveal a weak association between social capital and health (14). In our results, income disparities are unclear, as we did not ask about participants’ income. Moreover, the Japanese government does not officially announce Gini coefficients by subregions. Nevertheless, in Japan, the gap in assets exceeds the gap in income (28), and people over the age of 70 with low average incomes have 5.9 times more household assets than people under 30 (29). According to data on areas larger than school districts in Nagahama, a rural region with a high rate of homeownership (96%) has a low average annual income (2.82 million yen), whereas an urban area with a low rate of homeownership (63%) has a high average annual income (3.09 million yen). In addition, regionally specific statuses (e.g. family history) might be due to the presence of historic areas, and the social status of females remains controversial (30). The criteria for social disparities are hence unclear. The insignificance of health differences among neighborhoods may be due to undetected complex disparities rather than egalitarianism.
Another factor that might explain the absence of health disparities between neighborhoods with high and low levels of social capital could be that excessive cohesion compensates for the beneficial effects of social capital. As suggested by Kawachi et al. (6), strong bonding social capital within disadvantaged communities might promote poor health. According to the results of the aforementioned Japanese suburban study, people consider it bothersome to develop new cooperative relationships based on trust, and this causes poor health at the neighborhood level (19). As noted in another Japanese study of the association between social capital and mental health, people who belonged to a neighborhood association perceive their membership as a great obligation with a small return (16). As suggested by Hamano et al., this might feel bothersome. In this context, they refer to a study by Kondo et al. (31), which demonstrates that non-cohesive bonding networks may harm the health of their members.
In traditional regions, even with high homeownership rates, neighborhood activities can be harmful to health because of the burdens involved. Cohesion might also decline in neighborhoods in which people know and mutually support each other. According to Wakefield and Poland (32), marginalized people become increasingly excluded when connection and cohesion are emphasized without addressing fundamental inequities in access to resources. They suggest that recognizing the ambiguity of social capital could help community organizers build healthy communities (32).
Although our results cannot verify any regional inequities, we did observe that individuals who have no family members with whom to discuss mental health problems and who mistrust the general public tend to report being in poor health. The success of any health promotion activity will depend on the ability to involve such people. Giordano et al. (33) use ICC to examine associations between social capital indicators and self-rated health at the individual, household, and small-area levels. According to their results, household contexts account for total variance in individual health, whereas only 2.4% of total variance in individual health could be attributed to small-area contexts. The authors suggest that social capital interventions targeting health are unlikely to be cost-effective if directed solely at the neighborhood level, given that only small variations in health can be attributed to this context (33).
Attachment to place affects health at the neighborhood level. Hidalgo and Hernández (34) defined this concept as ‘a positive affective bond between an individual and a specific place’, examining it according to three spatial ranges (house, neighborhood, and city) and two dimensions (physical environment and social relationships). According to their results, neighborhood attachment is the weakest of the three spatial ranges, and social attachment is more important than physical attachments, although both are important (34). Our results indicate that neighborhood social relationships did not affect attachment to place. Nagahama has many features that evoke attachment to place, e.g. Buddhist arts (including national treasures) and the largest lake in Japan. The processes through which attachment to place is formed call for further examination, as this aspect could be used as a powerful tool in health promotion activities.
Our study is subject to several limitations. First, regarding selection biases, all the respondents had participated in community-based genome-epidemiology studies, and all had agreed to participate in collective health promotion activities. The vast majority of our sample (54%) thus consisted of females between the age of 50 and 74 years, who were cooperative and well-informed about local circumstances. Any conclusions drawn from this survey are thus of limited relevance to people in their 30s and 40s. It is nevertheless imperative to understand the attitudes of the groups represented to our respondents for promoting NPO activities with them. Females from these generations constitute a diverse population, including those who drive cars, use the Internet effectively, and work in other cities, as well as those who do none of these things. Sharp divides are likely to exist between those who have resources from outside the neighborhoods and those who do not. Younger generations are likely to become less and less associated with their neighborhoods. The selection bias inherent in this case might be useful for anticipating the future roles of social capital.
A second limitation to our study is that we did not ask participants about their income. As mentioned in the methodology section, we adopted a linkable anonymization method for recruiting motivated people for future activities. We therefore avoided questions about their income or educational status out of a concern that such inquiries might prevent people from volunteering. The correlations between self-rated health and general trust, participation in recreational activities, and family problems might have been partly due to economic factors. Even if economic disparities are responsible for poor health, health promotion activities by lay citizens are unlikely to be able to correct such disparities. Such activities should focus instead on affordable goals (e.g. making empathetic friends) and the accumulation of solutions to small problems, thereby helping to maintain people’s motivations (35). Moreover, income cannot be confidently regarded as an appropriate moderator variable in this study, as the study region includes areas with low income and high rates of homeownership. Furthermore, the social status of females between the ages of 50 and 74 years (who are overrepresented in this study) affects not only themselves, their husbands, and cohabitating in-laws, but also their own parents and children living in other locations. The relationship between income and social status is not clear.
Third, the cross-sectional design of this survey research prevents us from establishing the causality. According to our results, people in areas in which a higher proportion participate in community activities have lower self-rated health. Although this result might suggest that participation in neighborhood activities has a negative effect on self-rated health, it could also mean that people with poor physical health are more likely to want to engage in neighborhood activities. This could be attributed to a desire to compensate for their poor health, or it could be because they were unable to work or engage in activities outside the neighborhood, thus leaving them with more time for neighborhood activities, in contrast to their healthier counterparts. Additionally, we identified a correlation between general distrust and self-rated poor health. Poor health might lead people to harbor general distrust.
Fourth, the primary outcome variable of this study was self-rated physical health, but we did not measure mental health. As explained above, we employed a linkable anonymization method, thus intentionally avoiding the measurement of mental health status, which might be perceived as carrying a social stigma. According to our findings, those with whom people discuss their mental health problems are associated with their self-rated physical health. The result might have been different if mental health had been the primary outcome variable. Finally, located near the ancient capital of Kyoto, Nagahama has a long history. One-third of its residents have never lived outside the city (more than five times the national average of 6.3%), and the fluid population is low. Our results might therefore not be applicable to places with high fluid population.
Long city histories have the potential to foster unique and complex social statuses. Additional qualitative study is needed to determine why general mistrust is associated with poor health, whereas neighborhood mistrust is not, as well as why discussing mental health problems with acquaintances is associated with poor health. Further insight into the range and dimensions of attachment of place is required as well.
Conclusion
With regard to health at the neighborhood level, we found no significant differences between traditional areas characterized by highly supportive environments and high levels of neighborhood trust and urban areas that lack these characteristics. Our findings associate poor individual health with not participating in recreational activities, not having general trust, and not discussing mental health with family members. These results suggest that health promotion activities should aim to help people develop empathetic friendships through individual networks and take individuals who need support to compatible places. After examining the processes through which attachment to place is formed, this factor should be incorporated into activities.
Footnotes
Acknowledgements
We would like to thank the members of the Health Promotion Zero-ji Club for cooperating with this research. We are very grateful to two anonymous reviewers for detailed comments on the original manuscript.
Conflict of interest
None declared.
Funding
This project was supported in part by the ‘Nagahama Regional Open Genome Epidemiology Study’ of Ristex in the Japan Science and Technology Agency.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.