
Abstract
Aims:
Public health intervention research increasingly adopts a complex systems approach, viewing interventions as events in systems that must adapt to evolving circumstances for sustainability. This study examines how a process of self-evaluation guided by the Action Scales Model (ASM) can enhance adaptive capacity in intervention programmes.
Methods:
This study reports on the experiences from the Child Life in Healthy Balance (CLHB) programme. Data sources include participant observations, interviews, meeting minutes, and implementation logs from programme developers, project leaders, and local practitioners collected between 2020 and 2024. Observations examined engagement with the ASM during workshops and implementation activities, while interviews illustrated practitioners’ understanding of programme goals and implementation. Meeting minutes documented programme planning and self-evaluation discussions, and implementation logs showed progress and signs of change derived from the programme.
Results:
Through practice examples from the CLHB, we demonstrate how the ASM was used as a self-evaluative tool among programme developers and project leaders, as well as a framework for participatory evaluation and communication of programme goals to local practitioners. We highlight signs of capacity building and system change. The ASM facilitated structured discussions on implementation progress and helped align and adjust actions with programme goals. Although practitioners were not always explicitly aware of the ASM, interviews revealed that their understanding of programme goals was aligned with the terminology of the ASM and the overall principles of a systems approach. Some inconsistencies in interpreting the model created uncertainties, yet ASM proved valuable for communicating programme strategies and engaging local practitioners.
Conclusion:
The ASM helped align actions with CLHB programme goals, fostering adaptive capacity by reframing and aligning perspectives. These positive experiences suggest that the ASM can be a useful tool for self-evaluation to enhance capacity-building efforts in systems-oriented community health interventions.
Plain Language Summary
Why was the study done? This study aimed to understand how the Action Scales Model (ASM) can help community health programmes adapt to changing needs. It focused on the ‘Child Life in Healthy Balance’ programme, which promotes healthy lifestyles for children, to see if this model could improve how the programme evaluates progress and to help communicate the programme’s goals to practitioners. What did the researchers do? Researchers collected data from observations, interviews, meeting notes, and implementation records. They examined how the ASM was used during workshops and daily activities, examined local practitioners’ understanding of the programme’s goals, and tracked how the programme developers and project leaders used the model to evaluate the programme’s progress and changes over time. What did the researchers find? The ASM proved useful in two main ways. First, it helped those running the programme review activities and tracking progress. Second, it facilitated clear communication with local practitioners about the programme’s goals. While not all practitioners were fully aware of the model, their actions generally aligned with its principles. Some misunderstandings of the model caused occasional confusion, but overall, it kept the programme focused and engaged. What do the findings mean? The findings suggest that the ASM can be a valuable tool for community health programmes, enhancing their ability to adapt strategies and align actions with goals. Using this model, health programmes like Child Life in Healthy Balance can make positive changes in their communities by responding effectively to challenges. This study shows the model’s potential to strengthen community health initiatives.
Introduction
Public health intervention research is increasingly embracing a complex systems approach. 1 This approach moves away from a reductionist perspective, which addresses health issues and interventions in isolation, towards recognizing the intricate interactions among various factors across different levels (such as individual, community, and societal).2,3 Moreover, it involves viewing interventions as events in systems that can only be sustainable if they adjust to evolving circumstances. 1 Sawyer et al. 4 characterizes a complex systems intervention approach as multilevel action (e.g. at several levels of government at the same time), cross-sectoral working (i.e. including a diverse set of actors), and responsive adaptation. The latter necessitates the ongoing adaptation of intervention content, of implementation strategies, and even of targets in response to systems change. Thus, the question arises: How can the capacity for responsive adaptation be built within public health programmes and their sustainability ensured over time?
Van den Broucke has proposed that working with ‘capacity building shifts the focus from directly trying to influence the health of the population towards enabling systems and networks to promote health in a self-determined and sustainable manner, thus enhancing, prolonging and multiplying the health effects of actions undertaken. 5 ’
According to the ‘parallel track theory’, capacity building should run concurrently with specific intervention goals, recognizing its role as a complementary effort that contributes to broader objectives. The parallel track theory and capacity-building literature in general highlight the interconnectedness of capacity-building efforts and public health interventions, striving for comprehensive and sustainable improvements in outcomes, such as community health.5–8 An essential facet of capacity building is its reliance on existing structures, aiming to enhance what already exists. 9
The literature on capacity building presents several types of capacities, each targeted at specific goals or capabilities or situated in specific disciplines, for example, public health capacity, 10 health promotion capacity,11,12 and mental health promotion capacity.13,14 Another type is adaptive capacity which, in general, describes ‘the capacity of systems, institutions, humans, and other entities to adjust to potential damage, take advantage of opportunities, or respond to consequences’. 8 Adaptive capacity is, thus, not situated in a specific discipline or field but focuses on the ability to navigate ever-changing complex systems.
In this article, we report on the experiences from a Danish systems-oriented and community-based health promotion programme, Child Life in Healthy Balance (CLHB). 15 Specifically, we describe a process of self-evaluation, conducted by project leaders and programme developers, and we discuss the extent to which this process may have served to build adaptive capacity.
The CLHB programme was developed based on parallel track theory by Local Government Denmark, the national interest organization for Danish municipalities, in collaboration with municipal representatives, and was designed to improve the wellbeing and healthy weight of children in low-income communities in Denmark, as well as the adaptive capacity of the communities. The programme was developed and tested in ten communities across three municipalities during a 5-year period, 2020 to 2024. The purpose of the CLHB programme was to bring municipal and local actors in the communities together to engage in interventions to enhance the everyday life environments for children with regard to play and movement, healthy food, and drinks, as well as local experiences. The programme involved local project leaders from each participating municipality in the collaborative development, implementation, and evaluation of evidence-based intervention strategies. 15 Specific interventions and implementation strategies were developed in collaboration with local practitioners and included actions such as the development of a proactive breastfeeding approach in family healthcare and new models for collaboration between daycare centres and local sports clubs. Implementation was supported by meetings and workshops both within and across communities and groups of practitioners, contributing with knowledge and sharing of experiences.
The CLHB programme was embedded in a Danish welfare context characterized by a high degree of municipal autonomy, universal access to health and social services and an encouragement for intersectoral collaboration in local health promotion.16–19 These structural conditions allow municipalities to design and implement context-sensitive interventions tailored to local needs and resources. While the CLHB programme is context-specific, it shares core characteristics with international programmes such as the Amsterdam Healthy Weight Programme.4,20 Both initiatives take a whole-systems and community-based approach to childhood overweight, aiming to address structural determinants of health through long-term, cross-sectoral collaboration. For example, like the CLHB programme, the Amsterdam programme engages stakeholders across domains – including education, health, social care, and urban planning – to promote healthy food and drink, physical activity, and supportive everyday environments for children. Both programmes work with the understanding that child health is a shared responsibility that requires coordinated action across multiple levels of society.4,21
During the implementation phase of the CLHB programme, the programme developers introduced the Action Scales Model (ASM) 2 to facilitate an ongoing self-evaluation process with the purpose of tracking the CLHB programme’s contributions to systems change and adaptive capacity within the communities.
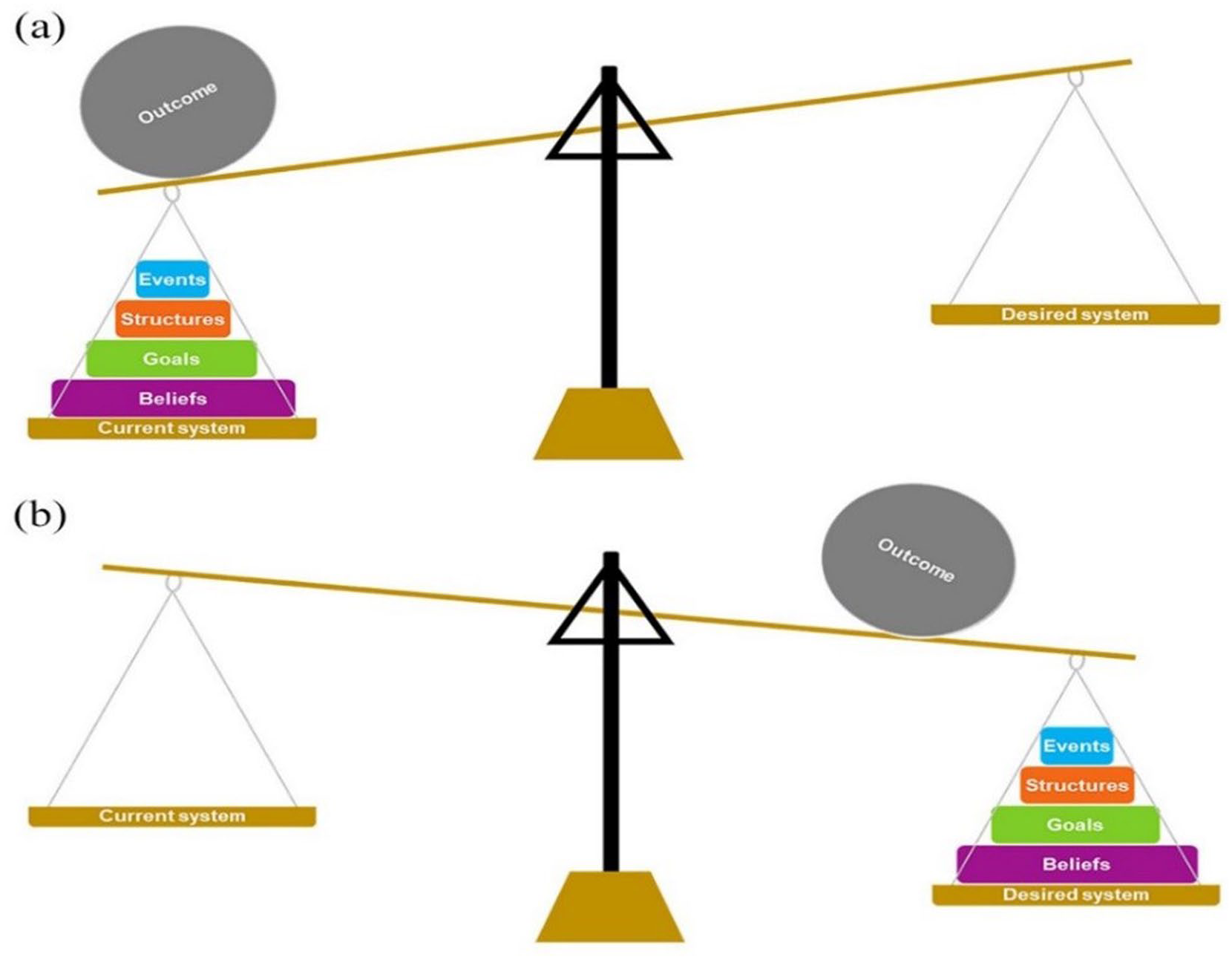
The ASM
The ASM is designed to help users understand the complexity of their respective systems and to identify opportunities to change how these systems work. The ASM is depicted as a set of ‘weights’, with certain weights holding greater leverage for systems change (Events, Structures, Goals, and Beliefs). The idea being that if we can tip the scales from one side to the other, then sustainable and transformational systems change may occur. This nuanced understanding allows intervention developers and evaluators to grasp the systemic impact of interventions and tailor strategies that align with the overarching health goals. 2 In addition, the model’s design is underpinned by Meadows’ 12 places to intervene 22 to provide theoretical rigour. The simplicity of the ASM (as opposed to Meadow’s work) is intended to broaden the model’s applicability, making it not only accessible to researchers but also a tool for practitioners and organizations without specialized knowledge of complex systems theory or intervention development and evaluation.
The aim of this article is therefore to understand how the ASM was used to guide the self-evaluation process undertaken within the CLHB programme and to critically assess its utility in enhancing adaptive capacity within the communities.
Methodology
Study design
This study employed a qualitative, multisource approach to examine the use of the ASM as a self-evaluation tool during the implementation of the CLHB programme. Data were collected throughout the entire implementation process across three municipalities, covering 10 distinct local areas. The study integrated a variety of data sources, including participant observations, interviews, meeting minutes, and implementation logs. This comprehensive data collection strategy was chosen to facilitate an in-depth exploration of the ASM’s role in self-evaluation among programme developers and project leaders, as well as its influence on fostering adaptive capacity and systemic change within the communities involved.
Data sources
A variety of data sources were drawn upon to provide practice-oriented examples of utilizing the ASM during the self-evaluation process. All data were collected between 2020 and 2024. The data sources were selected to capture diverse perspectives and gather comprehensive information about the experiences of programme developers, project leaders, practitioners, and other local agents when implementing the CLHB programme.
Participant observations
Participant observations were conducted by authors C.L. and D.D. to examine how programme developers and project leaders facilitated the self-evaluation process. Observations took place during implementation activities, such as workshops and themed evaluation days with practitioners. This ethnographic approach 23 provided insights into how the use of the ASM influenced the communication, delivery, and implementation of intervention strategies. An ethnographic approach situates the researcher within the practices of interest, thus allowing for a close engagement with the perspectives of various actors in the field. 23
Interviews
Semi-structured interviews 24 with 46 stakeholders, such as programme developers, project leaders, and local practitioners (e.g. child home nurses, pedagogues and teachers), were conducted between 2020 and 2024 to examine the implementation of the CLHB programme. The interviews were based on a guide specifying the overall themes and questions of interest, while maintaining flexibility to follow topics that were raised by the participants. 24 Through the interviews we gained insights into how the ASM was used in the project communication to form practitioner perspectives on the programme’s intervention strategies and overall goals.
Meeting minutes
Access to meeting minutes of sessions involving programme developers, project leaders, practitioners, and other local agents, such as schools and sports clubs, was provided by programme developers. These minutes documented discussion points related to programme planning, implementation, and self-evaluation. They served as a record of stakeholder engagement and collaboration throughout the self-evaluation process, providing insights into the experiences of all involved parties with utilizing the ASM for self-evaluation.
Implementation logs
Project leaders utilized implementation logs to collect data and reflections on programme implementation. These logs were completed based on dialogue with and observation of practitioners from primarily child home nursing, kindergartens, and schools at various stages of the programme. The logs facilitated tracking of adaptive capacity, implementation of programme components, and signs of change across the four levels described in the ASM.
Data analysis
By drawing on multiple data sources, the documentation and exploration of the self-evaluation process aimed to develop a rich, multidimensional understanding. This approach facilitated the comprehensive assessment of the model’s usage and its efforts in cultivating adaptive capacity within both the programme and its associated communities. All data were carefully read and analysed by CL using thematic analysis 25 to extract relevant practice examples of the ASM’s application. This method enabled a systematic identification of recurring patterns and variations in how the model was understood and enacted across contexts. The examples were discussed with all co-authors to ensure consensus on the interpretation of the findings.
Findings
The ASM as a self-evaluation tool
During the implementation of the CLHB programme, the ASM was integrated into an ongoing self-evaluation process, which included weekly meetings between programme developers and project leaders from each participating community. In addition, the programme group met at biannual seminars to have in-depth discussions on implementation progress, challenges, and potential drivers. Self-evaluation tools included, in addition to the ASM, a simple visual analogue scale to assess the status of implementation in the participating 37 daycare centres and 10 schools, and network models to record the development of new relationships and collaboration in each community.
One dedicated session during these seminars focused on evaluating the application of the ASM in the programme’s implementation. During the initial seminar, where the ASM was introduced, project leaders brainstormed observed signs of change and capacity building at each level, developing matrices for intervention areas (Figure 1 and Table 2). Approximately 1.5 years into implementation, the focus shifted to identifying new strategies for areas lacking sustainable change. For instance, while the CLHB programme had been integrated into curriculum themes and annual plans in many daycare centres, it was not as deeply ingrained in school culture. Around 2.5 years into implementation, matrices for all major intervention areas and project goals were developed and discussed by the group, providing insights into implementation strategies to support efforts at all levels and promote sustainable change. Examples of these matrices are presented below.
Action scales model by Nobles et al. 2
Healthy food and drinks
One of the programme’s goals was to foster an environment with healthy food and drinks, with involvement from stakeholders, such as parents, daycares, schools and local sports clubs, as well as businesses sharing responsibility for a healthier environment for children in the community. 2 During project seminars, signs of change related to this goal and capacity building were identified across all four levels of the ASM, indicating positive shifts in children’s food habits and lunchtime experiences (see Table 1).
Matrix of signs of change and capacity building across the levels in the ASM: healthy food and drinks in kindergarten and schools
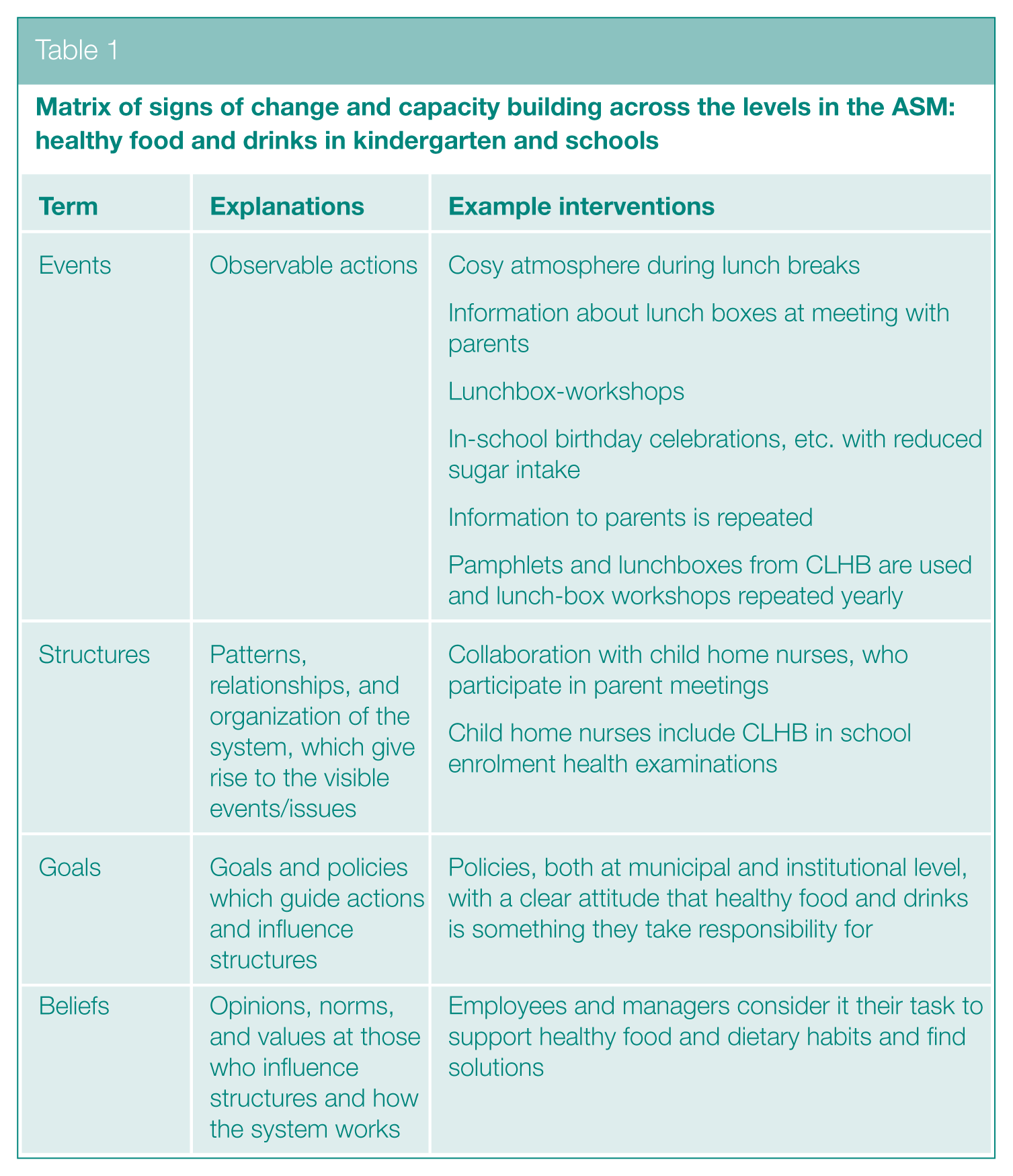
Table 1 illustrates examples of identified signs of change and capacity building at all four levels from the model: Events, structures, goals, and beliefs.
Promoting collaboration for healthy activities and environments in the community
Another objective of the programme was to increase physical activity and health-related engagements through community collaboration. 2 Matrices were created to assess signs of change and capacity building regarding children’s activity levels and community health promotion efforts (see Table 2).
Matrix of signs of change and capacity building across the levels in the ASM: the local communities collaborate to promote healthy activities and environments
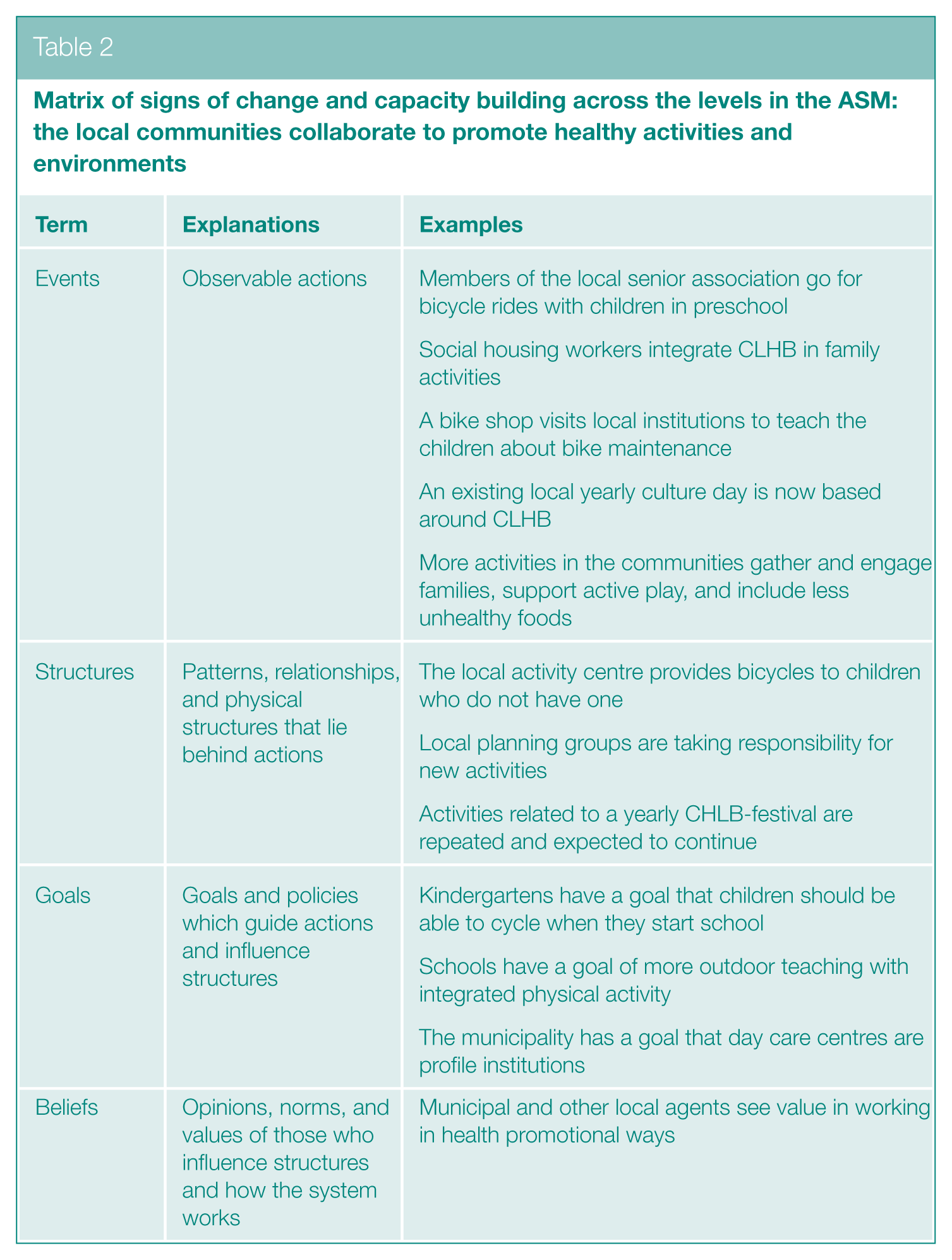
Table 2 illustrates the examples of collaborative community efforts to promote healthy activities and environments for children.
The ASM as a tool for participatory evaluation
The ASM served effectively as a framework for participatory evaluation. Project leaders and programme developers utilized the ASM to convey programme objectives and anticipated impacts to practitioners. It was instrumental in illustrating the programme’s goals, the implementation process, intermediate outcomes, and the capacity-building components embedded within the programme.
Participatory evaluation
Annual or biannual themed project days were organized for practitioner groups, including child home nurses, pedagogues, teachers, and consultants from cultural and leisure sectors. These sessions focused on evaluating implementation achievements and challenges. While the ASM was not introduced to all practitioners from the outset, project leaders and programme developers implicitly applied its logic in their communication of programme principles. This contributed to practitioners’ growing awareness of the programme’s system-oriented goals.
In the third year of implementation, the ASM was explicitly introduced during themed project days for child home nurses through a presentation, followed by a structured exercise where participants were asked to assess their own actions according to the model. Practitioners were encouraged to categorize observed or intended changes under the model’s four levels – events, structures, goals, and beliefs – to support discussions on how and on which levels new practices affected children and families and contributed to systemic change (see Picture 1). The ASM thereby functioned both as an analytical tool for participatory evaluation and as a framework for fostering reflection on sustainable changes in everyday practices.
Photo from a workshop with child home nurses
Experiences with this approach varied. In one workshop, the ASM was highly valued, helping child home nurses identify and discuss changes in their practices. In another, it was perceived as overly theoretical and too abstract, with some participants struggling to connect the model to their daily work. One nurse noted, ‘No, I don’t think I can identify any changes. We do as we always have. But I also implement what we do in CLHB for the other families I visit’. However, this comment suggests that, despite not perceiving changes, nurses may still be implementing CLHB practices during other family visits, indicating a shift in practice.
While some practitioner groups quickly grasped the model and used it actively to structure discussions, others found it less accessible. This variation reflects a lack of full consistency in how the ASM was understood and applied. Nonetheless, across contexts, the model functioned as a catalyst for reflection and discussion, even where it was not explicitly referenced. Practitioners’ descriptions of new routines, structural changes, and evolving professional goals often aligned with the ASM’s four levels, indicating a tacit internalization of its principles. For some, particularly those who had contributed to the programme’s development, the model reaffirmed existing intentions; for others, it provided a new lens through which to understand the broader aims of their practice.
Communicating the systems approach
Not all practitioners attended the ASM evaluation workshops, but the communication of project principles by project leaders – and in some cases by local leaders from child home care and daycare institutions – reflected the systems approach underlying the ASM. This contributed to practitioners’ understanding of the programme’s goals and seemed to enhance their motivation for implementing the intervention strategies.
Several practitioners expressed that the programme’s purpose was to systematize their activities. For instance, a pedagogue from a daycare institution remarked, It makes so much sense because there are so many things we need to focus on health-wise (. . .). So, yes, we’re already doing them, but it’s nice to have a framework around what exactly we need to remember is important for children’s health.
A child home nurse commented, ‘It becomes more explicit that there are certain areas we need to ask about in particular, and we have some guide questions for that. And I think it’s become more systematic in that way’. Although not directly referencing the ASM’s design, practitioners often highlighted the programme’s goal to integrate specific activities into improved structures within their respective institutions.
Some practitioners also noted changes in goals and policies, when asked about the implementation of the programme. A pedagogue from a daycare institution said that she observed a shift in attitudes towards healthy food among parents and children, representing a sign of implementation to her, while an after-school care leader mentioned updating school policies to align with the programme’s health objectives. These examples reflect an understanding of the programme’s aim to induce change at multiple levels, not just within practitioner activities.
Several practitioners recognized the programme’s capacity-building aspect. Pedagogical leaders described it as strengthening existing institutional structures. One leader explained, ‘We always approach [the implementation] deductively: What are we already doing? How does it fit with what’s coming from the outside? Does it give us a perspective on something we might be missing?’ Similarly, another leader stated, ‘It’s about creating some good routines that fit into the daily life we already have’. A child home nurse also noted, ‘It’s really an upskilling of what we’re already doing. Or at least, I think that’s the purpose, right? To strengthen the initiatives’.
Overall, these findings reflect that the systems approach of the programme was communicated successfully to the involved practitioners in a way that resonated with the terminology within the ASM (focusing on the levels of events, structures, goals, and beliefs). This contributed to increasing practitioners’ understanding of the programme’s objectives, including its impact at various levels and its focus on system-oriented and capacity-building aspects.
Discussion
In this article, we demonstrate how the ASM facilitated a self-evaluation process among project leaders and programme developers, enabling them to discuss signs of change and drive implementation towards sustainable changes and capacity building. Furthermore, the model served as a framework for participatory evaluation with the involved practitioner groups and provided a useful terminology for communicating the programme’s objective and the overall systems approach.
This study is one of the first to apply the ASM in a real-world health promotion context, other than the one in which it was first developed. The ASM, developed relatively recently, has not been tested or explored in previous research. Its intended function, as described in the original framework, is to guide stakeholders in identifying points of intervention within a system to maximize the impact of their actions and foster systems change. 2
This study expands on that by demonstrating how the ASM can be used practically to support self-evaluation, facilitate communication, and promote adaptive capacity in health promotion programmes, particularly through its roles in knowledge enhancement and communication facilitation. Adaptive capacity in healthcare contexts refers to the ability to adapt services or practice, and a 2022 literature review found that adaptive capacity relies heavily on enabling factors such as knowledge and communication as drivers for adapting practices. 26 We argue that the ASM holds the potential (1) to strengthen the ability to integrate and combine different knowledge sources (i.e. knowledge as an enabler) and (2) to facilitate communication efforts (i.e. communication as an enabler).
In our study, the ASM was used as a participatory evaluation tool, allowing practitioners to gain valuable insights into the implementation and outcomes of new practices. One example is when child home nurses categorized signs of change during themed days, reflecting on their new practices and realizing how these aligned with broader programme objectives, thus enhancing their understanding of their own practice by integrating and combining different knowledge sources. Insights such as these can act as enablers for practitioners to adapt more effectively to the changing demands in their practice and their community. This corresponds to knowledge as an enabler for adaptive capacity as outlined by Lyng et al. 26
According to Lyng et al., 26 adaptive capacity has four main aspects to it: reframing, aligning, coping, and innovating. We argue that the use of the ASM in implementation may have enhanced adaptive capacity, particularly by promoting reframing. Reframing involves changing the way something is expressed, considered, or performed, thereby transforming perspectives and procedures. 26 The ASM was employed during themed days with practitioner groups and their leaders to visualize and reframe their daily efforts, enabling them to understand and communicate how their actions contributed to the programme’s overall goals at various levels. This approach also allowed practitioners to see how their past actions and strategies supported the programme’s objectives and how the new strategies fitted within the broader framework. In addition, the model appeared to foster an alignment of interest and goals. Alignment refers to converging views, meanings, and practices to achieve a shared outcome. 26 Adaptive capacity relies on aligning interests among different stakeholders with diverse perspectives and strategies. 26 In the CLHB programme, strategies were carried out by various practitioner groups, programme developers, and project leaders. The use of the ASM, illustrating the collaborative impact of the programme strategies across different levels, seemed to help align goals and views among all stakeholders involved.
However, inconsistencies in interpreting weights and efforts within the model led to uncertainties among practitioners when directly engaging with the ASM. This initial exploration suggests the need for diverse engagement and communication strategies tailored to the specific needs and perspectives of practitioner groups. The findings reveal that many practitioners understood and applied the model’s levels indirectly when framing the implementation of their efforts.
The experiences from the CLHB programme thus show that using the ASM as a framework to identify and discuss signs of changes and capacity building was beneficial for programme developers, project leaders, and practitioner groups. The model was particularly suitable for communicating the systems-oriented mission and purpose of interventions to the involved practitioners. By helping the involved practitioner groups visualize and understand the systemic impact of their actions, the ASM may have helped facilitate the integration of programme strategies into everyday practices and policies. This integration can promote the development of durable structures and relationships that support ongoing health promotion efforts. Furthermore, the model’s ability to align diverse interests and goals fostered a shared commitment to the programme’s objectives, enhancing the likelihood of long-term sustainability. Based on the experiences with the ASM in this context of CLHB, we argue that the model holds potential for use in the implementation of system-orientated interventions and should be tested in a broader range of contexts.
Implications for policy and practice
The findings from this study highlight the ASM as a valuable self-evaluation tool for community health promotion programmes, helping to identify signs of change and ensuring that diverse stakeholders share common goals and have a joint of understanding of the programme’s outcomes at different levels within a system. Our findings suggest that the model is particularly beneficial for practitioners, enabling them to clarify and visualize how their individual actions contribute to the broader programme goals and how health programmes can support systemic change. To maximize its potential, integrating the model during the early stages of programme design and development would be beneficial. Future research should investigate the model’s adaptability across different contexts and its long-term effects on adaptive capacity.
Conclusion
This article demonstrates that the ASM effectively facilitated a self-evaluation process among project leaders and programme developers, fostering discussions around change and contributing to sustainable outcomes and capacity building. The ASM served as a valuable tool for participatory evaluation, enhancing the integration of knowledge and communication, which are essential for increasing adaptive capacity within health promotion programmes. Based on the experiences from the CLHB programme, we recommend employing the ASM in future community-based interventions to ensure long-term sustainability and effective collaboration among stakeholders.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data collection for this study was funded by the Nordea-fonden. Centre for Childhood Health has funded the open access fee. The funder had no role in the analysis, interpretation of data, or the writing of the manuscript.
Ethical Considerations
This study complies with current Danish ethical guidelines and legislation of the Danish Data Protection Agency (Ref: 17/12006). Ethical approval was not required as per the National Committee on Health Research Ethics (Ref: 20182000–83) because our research did not fall under the scope of reportable research as outlined in the Committee Act [38].
Consent to Participate
Informed consent to participate in this study was obtained verbally from all participants.