
Abstract
Introduction:
Inflation and rising living costs are significant global issues impacting vulnerable groups, including informal caregivers. While it is known that informal caregiving may pose potential negative health effects, social inequalities associated with it are not well understood.
Aim:
This study aims to explore the material deprivation – specifically housing and food insecurity – faced by informal caregivers and the harmful effects this can have on health to inform future actions.
Methods:
We conducted a scoping review to explore the impact of material deprivation on informal caregivers’ health and well-being. We performed literature searches in databases including CINAHL, PubMed, SocINDEX, and Web of Science, along with hand searches, focusing on studies from the last 20 years.
Results:
The searches yielded 15 articles, mainly from the United States. The evidence shows that caregivers are more likely to report hunger, household food insecurity, and lower incomes than non-caregivers. They also experience household material, bill-paying, and healthcare hardships and have an increased risk of homelessness and child poverty. Some of these issues were further reported to affect their health.
Conclusions:
To tackle the social vulnerabilities caregivers face, robust national policies and healthcare practices that recognise and support informal caregivers and further in-depth research are needed.
Plain Language Summary
In recent years, the cost of housing and food has gone up around the world. This has made life harder for many people. When people cannot afford basic things like a safe place to live or enough healthy food, this is called material deprivation. We wanted to understand how this affects informal caregivers, those who care for or help a family member or friend without being paid. This review assesses previous studies and gathers evidence on whether these caregivers have what they need to live well and how not having these basics affects their health. We found that some caregivers do not have enough money for things like healthcare, safe housing, or regular meals, and some experience hunger. Young caregivers are especially affected. They may miss out on school or job opportunities, which can lead to long-term money problems and a higher risk of poverty. Not meeting basic needs like food and housing was harming the health of some caregivers, but we still need to learn more about this issue. To help caregivers who are not having their basic needs met, we need strong national policies, better support from the healthcare system, and more research to understand their needs.
Introduction
Informal caregivers provide unpaid care for their family members or other close ones with various health conditions. 1 Care provided by caregivers can be instrumental in supporting daily living, including help in bill paying and social activities, and concrete care duties, including giving medication, or around-the-clock care, which includes all the help and care the care recipient needs.2,3 The number of informal caregivers varies across Europe, from 2% to 38% of the population. 4 In addition, around 20% of the population provides family care in Canada, the United States (US), and the United Kingdom (UK), 5 and 12% in Australia. 6
Informal caregivers play a crucial role in supporting care recipients, helping to reduce the need for home healthcare and delaying institutionalisation, 1 reducing health and social care expenses, and limiting public spending. 7 For instance, informal caregivers provide 36 billion hours of care, valued at US$600 billion in the US. 8 While informal caregivers provide significant benefits at the individual and societal levels, their role may expose them to financial risks.1,9 The prior evidence suggests that some informal caregivers may suffer wage penalties, such as loss of earnings and employment opportunities, 9 opportunity costs, 10 poverty, 11 subjective experience of poverty, 12 and cumulative inequality in life, resulting in poverty in older age. 13 It is essential to recognize the vulnerability of some caregivers to economic hardships, particularly in light of the current global inflation trends.
Material Deprivation And Its Dimensions Of Housing And Food Insecurity
Material deprivation refers to economic hardship that limits access to basic necessities, such as the ability to pay unexpected expenses, maintain heating, or own essential items like a washing machine or car. It also involves facing payment debts on housing and utility bills. 14 Material deprivation can also be linked to the risk of poverty or social exclusion, and it influences living conditions. 14
Although the definition of material deprivation includes the elements of food insecurity, food insecurity is commonly described as the inability to obtain sufficient quality or quantity of food in socially acceptable ways, or the concern about doing so. 15 Food insecurity is the starkest indicator of social inequalities 16 and is strongly linked to human rights since everyone should have the right to affordable, nutritious food. 17
Inflation and increased living and food costs are two recent major global crises, along with the COVID-19 pandemic and the financial crisis of 2007–09. 18 Energy, housing, and cost-of-living crises, combined with rising inflation in the Western world, have further exposed national inequalities. 19 The current situation is alarming, as it may worsen material deprivation and deepen social and health inequalities. Housing and food insecurity significantly contribute to these disparities, 20 being the building blocks of inequitable societies and health.20,21 As history has shown, economic hardships and global crises affect food security22,23 and expand social inequalities.24,25 Material deprivation, 26 inappropriate housing, 27 insufficient living conditions, and food insecurity28–31 may also contribute to ill health.
Health Implications Of Caregiving And Material Deprivation
Caregiving has been described as a major public health issue. 32 Some caregivers are more vulnerable to low mental health, psychological well-being, and quality of life than non-caregivers.33–35 However, although the relationship between health and poverty 36 and social determinants of health37,38 have been widely investigated and identified, in general, informal caregivers’ social determinants of health have received less attention,39,40 although some prior evidence on the topic exists.41,42
Prior evidence shows that some caregivers experience subjective poverty and diet-related disparities, indicating their food insecurity risk. 12 Those experiencing food insecurity may consume less fruit, vegetables, and fish. 28 Healthy and nutritious food products might be more expensive than nutrient-poor and energy-dense foods. 43 Food insecurity often leads to the consumption of nutrient-poor, energy-dense foods, contributing to issues like obesity, infectious diseases, 44 and chronic conditions. 45
However, little is known about the health implications of caregiving related to material deprivation, although caregivers’ health and well-being have been extensively assessed. In addition, housing and food insecurity among informal caregivers have attracted limited attention. 12 Therefore, there is a need to bring together what is known about material deprivation and health implications among informal caregivers since little is known about their social determinants of health.39,46 This review will address this issue, build a knowledge base to inform social policy, and highlight areas for further research.
Aim
We aim to collect evidence from existing literature on informal caregivers’ material deprivation, focusing on housing and food insecurity. This will help inform future research and support needed actions, as little attention has been paid to the social challenges and inequalities caregivers face. To our knowledge, no literature review has been conducted on this topic.
Methods
We followed the steps for conducting a scoping review, including (1) identifying a research team for the review (i.e. sociologists and health scientists to have a comprehensive view around the issues of material deprivation and health), (2) the research questions, (3) relevant studies, (4) counting relevant studies in the review, and (5) extracting the data. 47 However, the review protocol or registration was not completed.
Review Objective
The objective is to present the existing evidence on informal caregivers’ material deprivation and the intersection of health and well-being outcomes. The following research questions guide this review:
What kind of material deprivation related to housing and food insecurity do informal caregivers experience?
What are the reported intersections of health and well-being outcomes related to informal caregivers’ material deprivation?
Search Strategy
Building on the earlier definition of material deprivation, we will examine the WHO Conceptual Framework on Social Determinants of Health. 20 In this context, we aim to evaluate the structural and intermediary determinants of health. Since material deprivation is classified as a social determinant of health, it emerges from structural determinants, influences intermediary determinants, and contributes to health inequalities and disparities in well-being. 20
We use a structured SPIDER method (Sample, Phenomenon of Interest, Design, Evaluation, Research type) for the search strategy. 48 The SPIDER method is an appropriate systematic search tool for this literature review, but it does not gather quantitative evidence for meta-analysis. We also follow the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 49 and reporting was conducted based on the PRISMA for scoping reviews (Supplementary material, Table 1).
Published literature was systematically searched in the following databases: Cumulative Index to Nursing and Allied Health Literature (CINAHL), PubMed, SocINDEX, and Web of Science. Moreover, to ensure strength, citation searches, searches by the web search engine Google, and hand searches in journals were added. Google search included similar search terms as the databases, including ‘informal caregiver’, ‘material deprivation’, and ‘housing/food insecurity’.
The search period for eligible articles was the last 20 years of publications to get an idea of the recent knowledge on the issue (2003–2023). This timeframe enables us to explore current research and perspectives that shape our existing knowledge. Search terms included but were not limited to the following keywords/MeSH terms: informal care/informal caregivers (i.e. Sample), material deprivation, food insecurity, and social and health inequality (i.e. Phenomenon of Interest). Terms were used alone and combined using Boolean Operators (and/or).
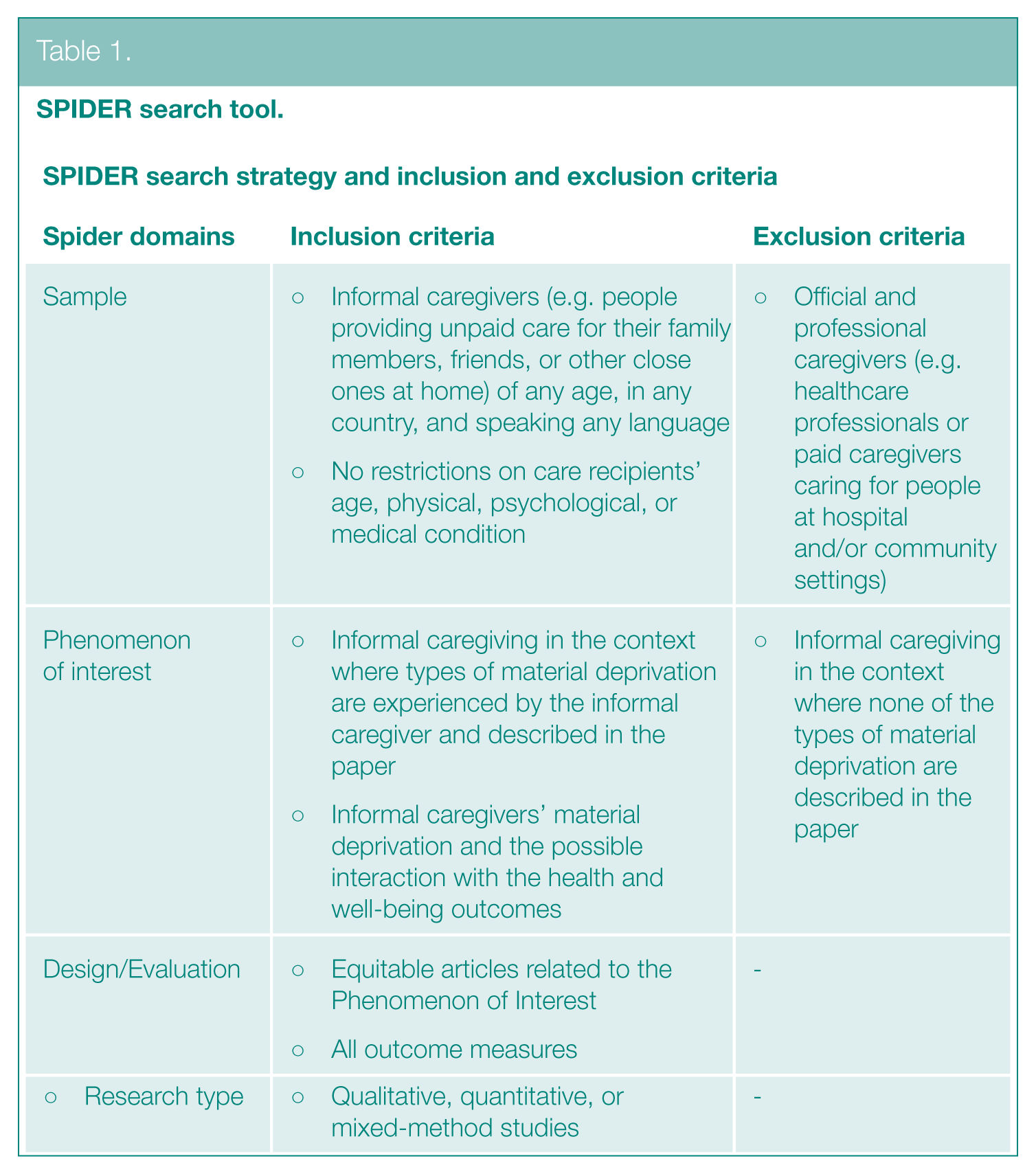
Eligibility Criteria
Table 1 shows the inclusion and exclusion criteria of articles. Moreover, along with the SPIDER domains, we included papers if they were (1) published in English and (2) peer-reviewed or gray literature. Those papers that did not meet the inclusion criteria were excluded. However, although the paper did not describe the connections between material deprivation and the health or well-being outcomes of informal caregivers, the paper was included. Thus, the focus is more on material deprivation. In addition, although the paper did not compare caregivers to non-caregivers, the paper was included.
SPIDER search tool.
Context of Caregiving in this Review
The included papers described informal caregivers using different terms, such as ‘informal caregivers’, ‘youth carers’, and ‘[people providing] unpaid care’. Therefore, we may use different terms for caregivers throughout the result section based on the terms used in the original source. Otherwise, we will discuss informal caregivers.
Moreover, due to the findings from the literature, the informal caregivers will be described as the context of the original study since many papers focused on specific groups of caregivers, such as older, younger, child, or youth caregivers, and highlighted their social issues or them in some social context. Therefore, informal caregiving will not be described by, for instance, the intensity of care, the conditions of the care recipient, or other factors familiar in the currently existing caregiving literature. We are more likely to describe informal caregivers by their demographic group, which will result from the literature included in this review.
Data Extraction, Synthesis, and Quality Appraisal
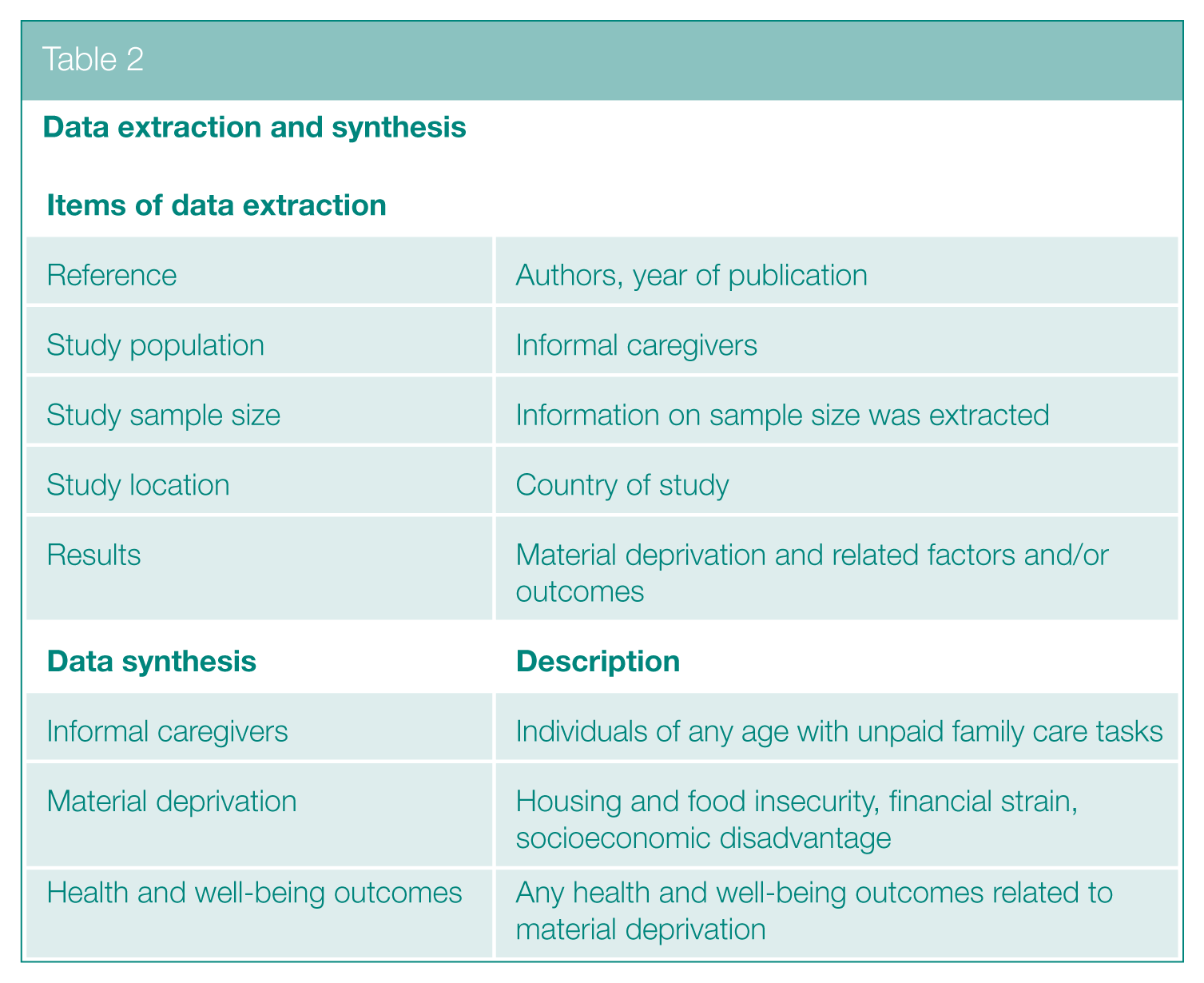
Data were extracted based on authors, publication year, methods, study population, sample size, study location, and results. The evidence focused on informal caregivers of any age who perform unpaid care tasks and experience material deprivation, along with related health and well-being outcomes. See Table 2 for details.
Data extraction and synthesis
Joanna Briggs Institute (JBI) appraisal tools were used for both qualitative and quantitative studies to assess methodological quality and potential biases in design, conduct, and analysis.50,51 The available options for answering the quality questions were ‘yes’, ‘no’, and ‘unclear’.
Two independent researchers screened the papers and conducted a quality appraisal, which involved resolving disagreements through discussion and collaborative decision-making on the selected articles.
Description of Included Papers
The PRISMA approach was used to review the process and report article selection. 49 The articles’ titles and abstracts were screened initially, followed by a detailed reading of the abstracts to eliminate irrelevant papers. The final step involved a full reading of the remaining eligible articles to select the qualified ones.
Of 1820 screened papers, 15 articles were included: 11 quantitative (73%) and 4 qualitative (27%) cross-sectional studies. These studies involved over 152,600 participants, mostly from the US (53%) and the UK (27%). Figure 1 shows the PRISMA flowchart of the selection process.
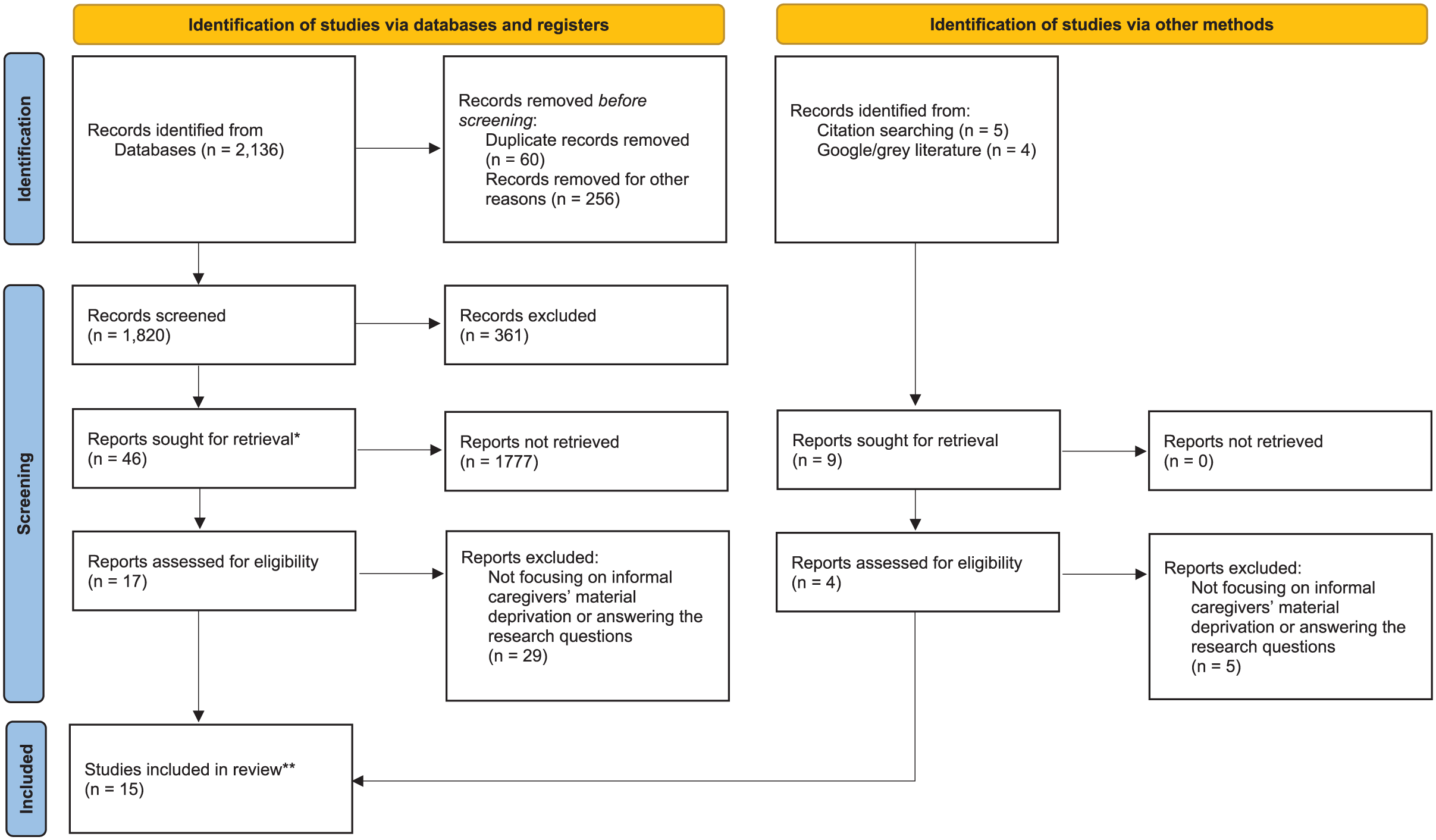
PRISMA flow chart
The included papers focused on caregivers of different age groups, from youth (underage) caregivers to older adults. In general, informal caregivers are defined as those who provide unpaid care for their family members or other close ones with various health conditions. 1 Young caregivers can be defined as ‘a child/young person under the age of 18 who provides care in, or outside of, the family home for someone who is physically or mentally ill, disabled or misusing drugs or alcohol. The care provided by children may be long or short term and, when they (and their families) have unmet needs, caring may have an adverse impact on children’s health, well-being, and transitions into adulthood’. 52
Methodological Quality of Included Papers
Table 3 includes an overview of the quality assessment. None of the articles were excluded due to the methodological quality. Some flaws of the included articles were related to (1) whether the influence of the researcher on the research and vice versa was addressed, (2) whether there is congruity between the stated philosophical perspective and the research methodology, and (3) whether the research is ethical according to current criteria or whether there is evidence of ethical approval by an appropriate body. In addition, there were rarely discussions regarding the influences of researchers’ background characteristics on interpreting the evidence. Similarly, ethical concerns were quite lacking. However, the overall quality of the articles based on the JBI was considered good.
Quality assessment
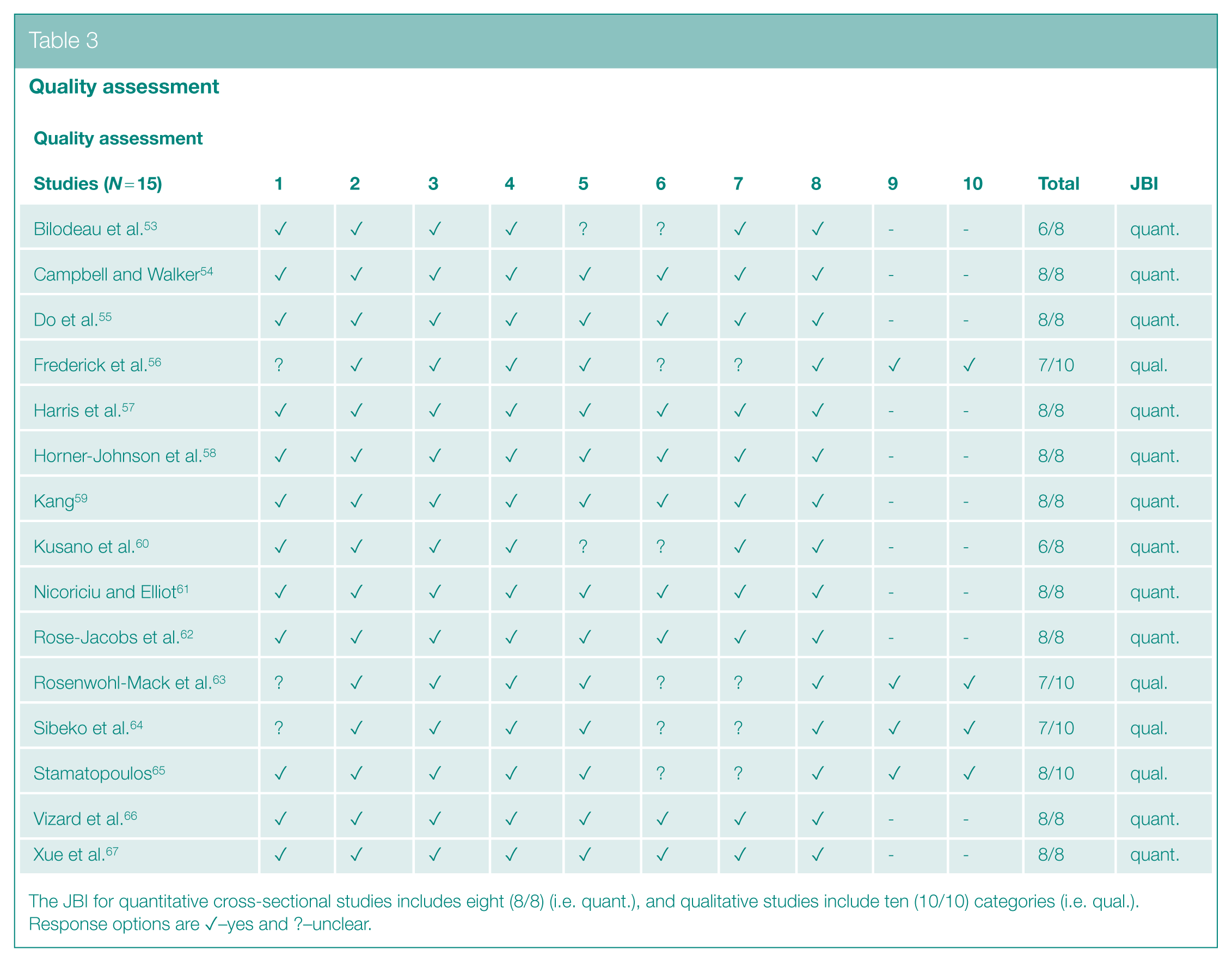
The JBI for quantitative cross-sectional studies includes eight (8/8) (i.e. quant.), and qualitative studies include ten (10/10) categories (i.e. qual.). Response options are ✓–yes and ?–unclear.
Results
The included literature primarily focuses on caregivers across different age groups, including youth (n = 5 of the included articles), adults of various ages (n = 5), and middle-aged or older adults (n = 5). Some of these definitions are derived from the original sources’ definitions of the age range.
Informal caregivers appear to be at an increased risk of material deprivation, such as housing and food insecurity. Young caregivers, in particular, encounter obstacles that can hinder their education and employment opportunities, further increasing their risk of poverty. The following sub-sections will provide a detailed assessment of material deprivation among informal caregivers and its relationship to housing and food insecurity, as well as the associated health consequences.
Informal Caregivers’ Material Deprivation And Its Relation To Housing And Food Insecurity
Table 2 in the Supplementary material includes the data extraction of the included articles. The evidence shows that caregivers are more likely to report personal hunger, household food insecurity, and obesity than non-caregivers. 58 Similarly, households with children with special healthcare needs and those receiving Supplemental Security Income were more likely to report household food insecurity. 62 Caregivers caring for a child with a disability were more likely to live in socially rented accommodation, be materially deprived, and not have a higher education. 61 In the study where the data were extracted, disability was defined as ‘disabled people have been identified as those who report any physical or mental health condition or illness that lasts or is expected to last 12 months or more, and which limits their ability to carry out day-to-day activities’. 61
Some caregivers caring for persons using mental health services reported that the households’ environment, including food insecurity, affected their ability to take care of the care recipient. 64 Moreover, the evidence showed that homeless older adults also engage in caregiving. They reported being caregivers to friends and family before and after becoming homeless. In addition, some older caregivers reported becoming homeless due to caregiving when the relationship with the care recipient ended. 63 Thus, some caregivers reported giving up jobs and apartments to care for their parents. Then, after the death of care recipients, the caregivers became homeless. The issue was considered to be related to the rising living costs; giving up a long-held lease can cause homelessness.63,68
Youth caregivers also experienced housing instability due to shared housing arrangements, or they had to use their own resources to support the family members they cared for. 56
Youth And Child Caregivers And Their Experienced Material Deprivation
Young caregivers (aged 15 to 19 years) experienced many severe outcomes from caregiving. These negative outcomes were described as the ‘young carer penalty’. 65 These penalties include personal (emotional, familial, and social) and professional (i.e. educational and employment-based) penalties, which are experienced by youth’s substantial and ongoing caregiving. 65
Young caregivers have also recognized the difficulty of negotiating working flexibility with large companies. They also experienced a lack of sleep, the time required for homework and studying, and concentration difficulties. 65 Moreover, young caregiving commonly included living in a lone-parent household, being from a non-professional socioeconomic group, and living in a household where no adults work. 66 Also, the evidence revealed some speculation on the ethnic diversity of young caregivers and themes about Indigeneity; 56 there might be a higher proportion of young caregivers in the areas with the greatest Indigenous population. 56
Trends in child poverty were stronger among young caregivers than among children without caregiving tasks, strengthening over time. 66 These young caregivers experienced relatively low income and had combined experiences of low income and material deprivation more than other children. 66 Young caregivers were also less likely to obtain a university degree and employment than young adults without caregiving responsibilities. 67 Young caregivers (ages 18-34) who lived with care recipients also had low incomes, were more likely to smoke, reported fair or poor health status, and were more likely to experience financial burdens. 60
Other Findings Related To Material Deprivation
Caregivers reported lower incomes than non-caregivers. 58 Similarly, having a lower educational status and being ‘Non-White’ increased the probability of material deprivation for those supporting children with disabilities. 61 Caregiving households were also more likely to experience bill-paying and healthcare hardships. 54 Based on data from the 2007 Behavioral Risk Factor Surveillance System collected in the US, some informal caregivers experienced financial burdens. In addition, around 15% of parents taking care of a child with cancer reported household material hardship, which increased to 33% after six months of the child’s chemotherapy. This trend stayed at the same percentage after one year of chemotherapy. 53 Around 36% reported losing more than 40% of annual household income due to treatment-related work disruptions. Similarly, 44% experienced financial hardship and reported ‘just getting by living paycheck to paycheck’. 53 Authors reported that this subcohort was socioeconomically advantaged middle-class families: White (81%), college-educated (83%), and employed (96%) with a median household income of US$101,012 (IQR US$72,690–US$182,500), which was above the median household income for families in Massachusetts (US$83,700), in the US. 53 Other evidence shows that caregivers were more likely to be unemployed or retired. 60 In addition, those working were less likely to work full-time.
Health And Well-Being Outcomes Related To Material Deprivation
Youth caregiving itself can be considered as material deprivation since it may make youths financially and socially vulnerable, as mentioned above. Due to their caregiving role, it was evident that they were exposed to potentially serious physical injuries, both short and long term, for which no health and safety workplace mechanisms exist to support them. 65 Similarly, homeless youths reported mental health burdens; they reported feeling guilt for not being able to do enough, being stressed and strained as they are trying to navigate services on behalf of their parent. The youths were also experiencing numerous disappointments and setbacks, which affected their mental health burden. 56 The burdens of young caregivers may also contribute to their housing instability and unmet personal needs. 56
Similarly, unmet needs were identified among older adults who were homeless and providing care. For example, an older adult taking care of his mother at the end of her life was occasionally homeless before caregiving. However, due to his caregiving role, he could not manage his medical conditions. 63 He then became homeless after his mother’s death again. Therefore, caregiving may reduce the ability to care for caregivers’ own health and lead to economic hardship for many.
Caregivers’ financial strain was also associated with self-rated health; a higher level of self-rated health predicted a lower financial strain among caregivers. 59 Similarly, those caregivers who reported fair or poor health were more likely to experience food insecurity, hunger, and obesity. 58 Caregivers’ financial burden was also associated with, for instance, smoking, having a stroke, lower incomes, and fair or poor health compared to those caregivers who did not report financial burden. 60
Finally, high-intensive caregiving might be common among those with greater levels of socioeconomic deprivation, affecting their health and employment. 57 The burden due to caregiving was also greatest among those with socioeconomically disadvantaged backgrounds. 57 In addition, the strongest association between poor health and caregiving was found among lower-income individuals, particularly ‘Non-Hispanic Whites’ with two or more children. 55
Discussion
Summary of the Results
The evidence is summarized in Table 4. The evidence shows a link between providing informal care to family and friends and experiencing material hardship. 54 Caregiving households were more prone to healthcare hardship, bill-paying hardship, and food insecurity than households not providing informal care. The literature also revealed young caregivers’ vulnerabilities in various financial, housing, and social issues. The evidence may align with the prior knowledge; young people without adequate support who are pushed into adult roles experience various risks. 56
Summary of the included articles
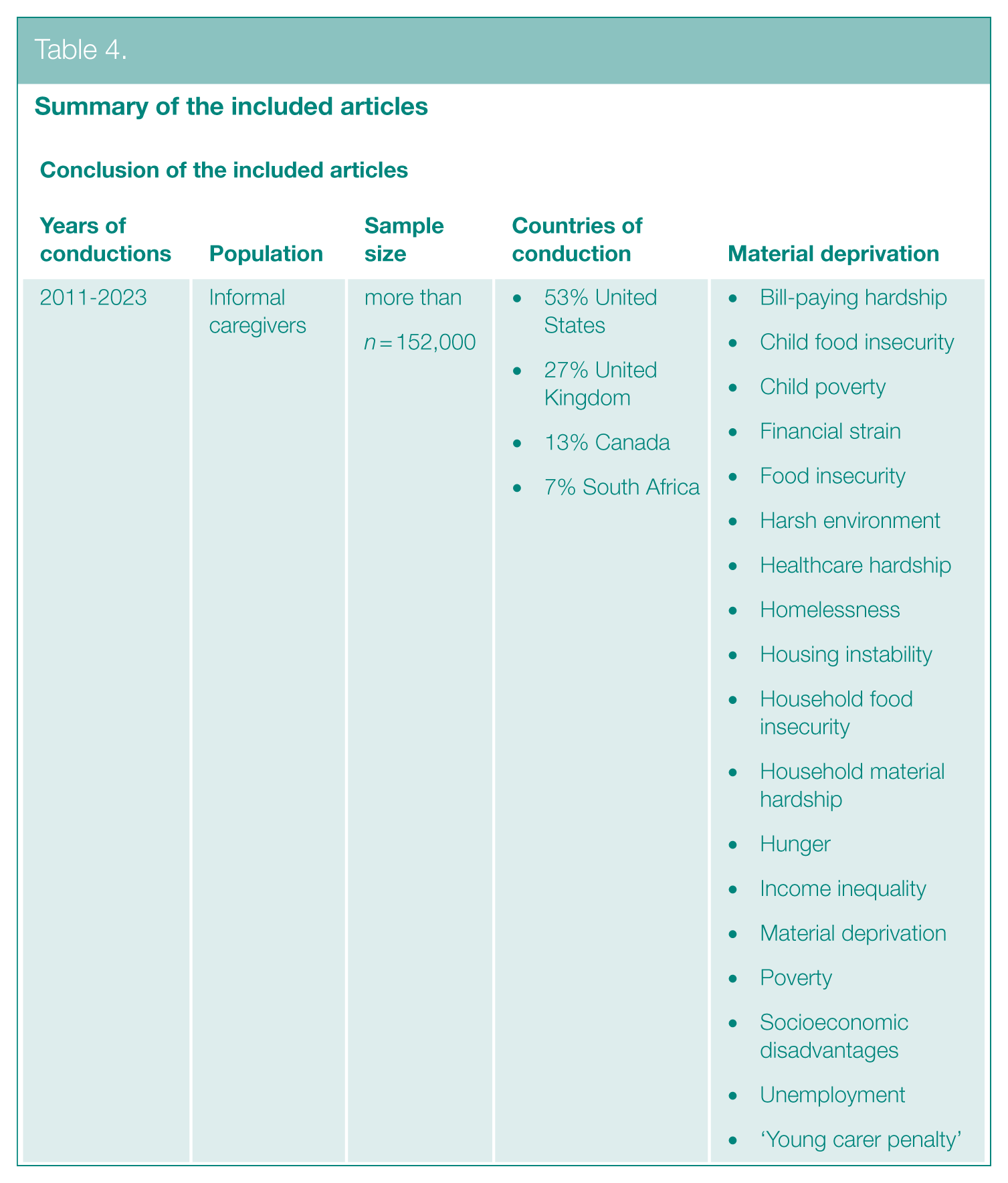
We may also draw lines between young and adult caregiving; both have similar issues. Hence, the evidence showed that adult caregivers were more likely to be unemployed or retired. 60 Those working were less likely to work full-time, which supports the findings related to the ‘youth carer penalties’; 65 these people are held back from pursuing educational and job-related opportunities. In addition, some young caregivers were at risk of child poverty, and there is a genuine concern about their health and well-being. In addition, caregivers caring for children with special healthcare needs and disabilities had socioeconomic vulnerabilities 61 and household food insecurity, 62 also indicating further health risks for these children with special needs.
Furthermore, the evidence indicated that there is speculation about the ethnic diversity of young caregivers, particularly about their connection to Indigenous communities. It appears that regions with higher Indigenous populations may have a greater proportion of young caregivers, suggesting a potential link between cultural background and caregiving roles. 56 This observation highlights the need for further research to understand the dynamics of caregiving within these communities and the unique challenges and experiences faced by young caregivers of diverse ethnic backgrounds. However, currently, the existing evidence is insufficient to draw any further conclusions.
Implications for Policy Development, Healthcare, and Future Research
The gathered evidence remains limited in its description of health outcomes related to caregivers’ housing and food insecurity. This is why the description persists superficially on a general level and assesses what the consequences could be among informal caregivers. Therefore, as inflation persists, there is a concern that health inequalities related to housing will escalate. Inflation encompasses a heightened risk of the cost of living, potentially resulting in homelessness, particularly among individuals in the privately rented sector. 69 This is considerable since homelessness, risk of homelessness, and housing instability were reported among both older 63 and youth caregivers. 56
The causes of health inequalities lie outside the healthcare sector. 70 Thus, reflecting on the WHO Conceptual Framework on Social Determinants of Health, material deprivation results from the structural determinants of health, including governance, social and public policies, socioeconomic position, social class, ethnicity, gender, education and culture, and social values. 20 These structural determinants affect intermediary determinants, including material circumstances (i.e. living conditions and food availability), the healthcare sector, and health and well-being outcomes. 20
Some countries, for instance, Scotland, may provide effective examples of how to tackle social and health inequalities, including housing and food insecurity, by seeking to address structural inequalities. 71 They have established three core principles through collaboration and public engagement, focusing on income, rights, and community empowerment. Guided by feedback from stakeholders during the pandemic, these principles address inequalities and uphold human rights: (1) ensuring everyone has adequate income through employment and social security, (2) advocating for access to essential goods and services, and (3) fostering community efforts to create a fairer society and empower individuals and frontline teams. 71
Moreover, social policies regarding caregivers vary globally. Some countries and areas of countries legally recognize caregivers,72–74 do needs assessments, and provide pension credits 4 and financial compensation for caregiving.4,75 At the same time, these are not applicable between or within all countries, and some caregivers may experience discrimination in labor markets 76 and a lack of support and social protection. 4 For example, only a few European countries have made arrangements for caregivers’ work-life balance. In addition, caregivers’ social inequalities are rarely the indicators selected to inform and assess public policies. 74
The current lack of equal policies may indicate the wide need for Western countries to evaluate whether the governments and their social and public policies are responsive to the issues related to material circumstances, including increased living and food costs. Improving housing and social policies across countries might be necessary. It should be evaluated if implementing various interventions to tackle poverty could assist households struggling. These interventions should focus on targeting, subsidizing, and customizing for various groups, ensuring fair access. 69
In addition, although the causes of inequalities lie outside the healthcare sector, healthcare plays a role in identifying an individual’s social determinants of ill health, including housing and food insecurity. However, the included studies did not have a view of healthcare or the role of, for instance, nurses in acknowledging or narrowing the inequalities. Nurses are on the frontline tackling health inequalities since they are the largest workforce in healthcare globally and have a necessary role in reaching the health-related targets of Sustainable Development Goals (SDGs) and Universal Health Coverage. 77 Nurses need (1) education on social determinants of health, (2) training on screening the social determinants of health, and (3) supportive working environments, which promote the importance of narrowing health inequalities.
Some governmental acts could be required. First, governments could (1) legally recognize caregivers and acknowledge their needed support and (2) provide necessary social protection. Then, it could be necessary to invest in policies that (1) improve housing security, (2) ensure affordable housing, (3) advance neighborhood quality and social support,69,78 (4) ensure adequate income and social security, and (5) guarantee rights and access to essential goods and services. 71
Second, we could consider whether there is a moral obligation to end the caregiving that children provide. SDG goal 1, ‘End poverty’, aims to end poverty in all forms. Currently, it seems that child/youth caregiving is deepening child poverty. However, we may first need to understand the broad issues leading to child/youth caregiving. Evaluating whether low-income families rely on children for caregiving, since they cannot receive help outside the household due to their lack of financial and social resources, would be necessary to investigate and provide solutions. Then, we could provide acts to end caregiving by children and protect these children from child poverty and poverty in later life. These children should also be protected from childhood food insecurity, which can have lifelong implications for mental and physical health, including infectious diseases, 44 and other chronic conditions. 45
Consequently, based on this review, we may conclude that some informal caregivers are vulnerable to material deprivation, including housing and food insecurity. However, little evidence exists on their housing and food insecurity and the consequences on health. Therefore, social inequalities among caregivers should be investigated further, including comparisons of diverse groups of informal caregivers in different countries to identify caregivers’ inequalities in health and evaluate policies. It would be necessary to, along with the aspects already mentioned in the discussion, investigate (1) whether informal caregivers have an increased risk for material deprivation, including housing and food insecurity, compared to those without caregiving tasks and (2) whether there are specific social determinants of health among informal caregivers, making some more vulnerable to material deprivation than other informal caregivers. In addition, less is known about whether informal caregivers have, in general, difficulties in grocery shopping and limitations in daily life that prevent them from preparing a hot meal, which could also affect their food insecurity. In addition, little might be known about whether caregivers lack access to other forms of capital, such as social capital.
Strengths And Limitations
We followed a systematic approach and screened and evaluated the included studies by two independent researchers. Nevertheless, we must also reflect on our own perspectives and beliefs on a topic and how this may shape our interpretation of the data extracted from the literature. Researchers of this review have expertise in caregiving research, social determinants of health, and food insecurity. The discovery of new literature and evidence indicates that our former experience did not prevent new literature from being discovered, and the methodology was sufficiently robust to capture literature outside the researchers’ range of expertise.
This review also has some limitations. For example, we included only studies that were written in English. Due to this limitation, we may have missed relevant evidence in other languages. In addition, the literature had some limitations; the main concepts and definitions of informal caregivers’ material deprivation vary in the literature, which may make it difficult to draw clear or consistent conclusions. Moreover, the evidence was mainly cross-sectional, a snapshot of the situation. Less is known about the causes and consequences of informal caregivers’ material deprivation and the further health and well-being outcomes. Therefore, clear conclusions cannot be drawn, and longitudinal studies are needed.
Also, the evidence was mainly from the US and the UK (80%); however, diverse evidence across, for instance, European Union countries would provide comparative evidence and an opportunity to assess caregivers’ material deprivation from the social policy perspective since there might be significant differences between different regimes, based on their political agendas. In addition, the gathered evidence lacks indication on aspects of material deprivation, for instance, caregivers’ inability to pay unexpected expenses, inability to adequately heat a dwelling (i.e. energy/fuel poverty), and inability to afford durable goods or being confronted with payment debts, which requires further evidence.
Conclusion
Informal caregivers are at a greater risk of experiencing material deprivation, including housing and food insecurity, which may negatively impact their health and well-being. Despite their challenges, the specific health outcomes related to their situation remain less explored. Young caregivers, in particular, face penalties that can hinder their education and employment, increasing their risk of poverty. To address these issues, governments must recognize the needs of informal caregivers, provide essential support and social protection, and implement policies to ensure adequate income and access to basic goods and services. Moreover, we must understand the factors contributing to child and youth caregiving; thereby, we can take measures to alleviate such responsibilities and prevent future social and health inequalities.
Supplemental Material
sj-docx-1-rsh-10.1177_17579139251371979 – Supplemental material for Material deprivation among informal caregivers: a literature review on housing, food insecurity, and harmful effects on health
Supplemental material, sj-docx-1-rsh-10.1177_17579139251371979 for Material deprivation among informal caregivers: a literature review on housing, food insecurity, and harmful effects on health by R-M Savela, O Kiljunen, T Välimäki, D Watts and J McKenzie in Perspectives in Public Health
Footnotes
Declaration Of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author received funding from the Jenny and Antti Wihurin Foundation and OLVI Foundation. INVEST Research Flagship Centre is funded by the Research Council of Finland (decision number: 345546).
Ethical Considerations
The approval from the Ethical Committee was not required because of the study design.
Availability Of Data
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.