
Abstract

Introduction and Context
The influence of the food environment on dietary behaviours and health outcomes has become critical in the population’s health. Food retail outlets (e.g. supermarkets, grocery, or convenience stores) influence the purchase of healthy and unhealthy foods, thereby impacting individual health. 1 Actively addressing food environments to create opportunities to achieve healthy, accessible, and affordable diets can improve the nutritional quality of food purchases and, subsequently, population health. 2 To effectively improve the food retail environment, transdisciplinary collaboration is critical, as food retail interacts with a wide variety of involved actors (e.g. government, the private sector and civil society), business models (e.g. supermarkets, café/restaurants or food chains), and diverse interests (e.g. economic, food supply or health advocacy). 3
Co-creation can nurture these interactions between retailers, researchers, consumers, and other interested parties to construct a shared goal.4,5 Co-creation facilitates collaboration and may provide a means to understand multiple aspects of stakeholder collaboration 6 required to create change. 5 To conceptualise co-creation as an approach, interactions between stakeholders and value propositions are essential. Value propositions are proposals that move stakeholders from passive to active players by motivating them to fulfil their needs through engaging in resource-sharing activities.5,6 The premise is that stakeholders’ experiences are shared when they interact and will help to attribute or propose value to something (e.g. revenue, health promotion). 6 Existing literature on the co-creation of health-enabling food retail environments has described the need to align strategies with the interests of all relevant parties (researchers and non-researchers), as non-researchers provide contextual knowledge of this emerging area of public health, and researchers’ skills may strengthen success in designing, implementing and evaluating initiatives.4,7
There is limited peer-reviewed literature in this rapidly emerging area of utilising co-creation approach to achieve mutually beneficial outcomes in food retail outlets.4,5,8 Academic researchers with experience in the co-creation of health-enabling food retail environments suggest that a collaboration based on trusting and respectful relationships, continual interactions and reciprocal acknowledgement between stakeholders is essential in the co-creation process. 7 However, views and perspectives of non-researcher stakeholders that may be using co-creation to improve the healthiness of food retail environments still need to be included as they are yet to be reported in peer-reviewed literature. This study aimed to identify practices and attitudes of a Healthy Supermarkets Community of Practice towards co-creation characteristics to develop or implement health-enabling initiatives in food retail environments.
Methods and Results
We applied a web-based survey (Supplemental Material Table S1) to the only Healthy Supermarkets Community of Practice in Australia to identify practices and attitudes regarding the co-creation of health-enabling initiatives in food retail environments. Figure 1 shows a summary of the main results.
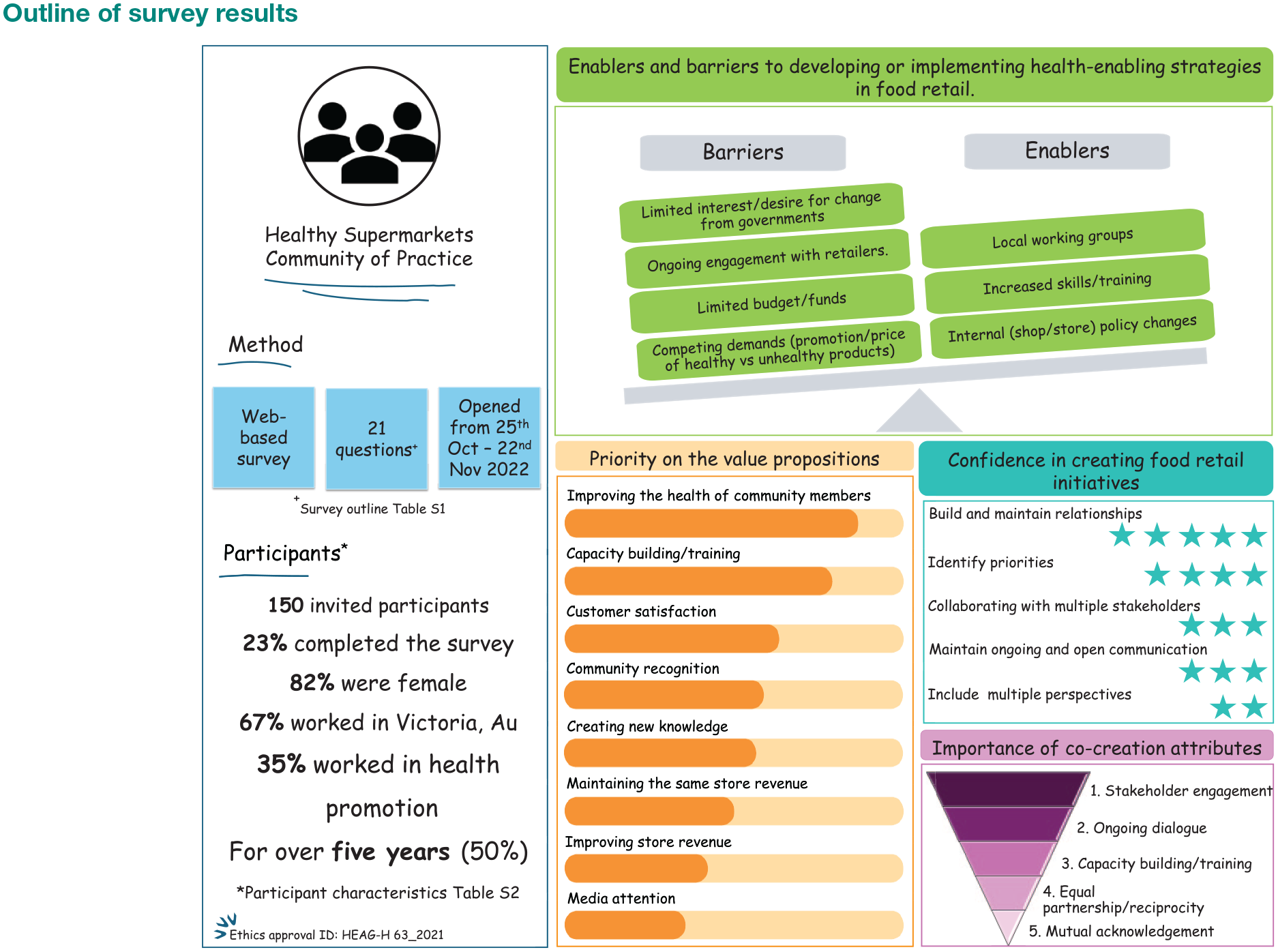
Outline of survey results
Discussion
Our results provided unique insights from practices and attitudes regarding the co-creation of health-enabling initiatives in food retail environments. While co-creation as an emerging approach to developing health-enabling strategies can achieve mutually beneficial outcomes in food retail outlets and sustain initiatives over time, our results highlight the complexity of embedding co-creation in current practice. However, building the capacity of the leading stakeholder group involved (i.e. health promotion) in healthy food retail outlets could help to progress the co-creation approach. Our findings highlighted the tension between health and business outcomes in the context of developing and maintaining health-enabling strategies in food retail outlets through ranking value propositions.
Our sample was represented by participants interested in improving the community’s health; therefore, it was expected that the ranking of the value propositions when collaborating with others related to benefits to the community or the workforce. With a lower value on maintaining or improving the revenue of the food retail outlet. When the value is centred on community benefits, the main motivation lies in promoting social change to benefit the population’s health. 8 Improving the community’s health as a main motivation can be the primary tension point when developing or maintaining health-enabling strategies in a setting that may have a primary interest for decision-making in improving sales, profits and competitiveness.3,8 Maintaining this interaction of value propositions (i.e. improving the community’s health and maintaining or improving the revenue of the food retail outlet) is essential to keep diverse stakeholders engaged in a different effort to influence the co-creation of health-enabling strategies in food retail outlets.3,4 It has been reported that the retailer’s perspective in encouraging healthy food retail to improve healthy food access is critical but poorly understood.8,9 Developing practical and longer-term healthy food retail policy approaches and interventions can be enabled by understanding factors that affect retailers’ in-store decision-making. 8
Co-creation, co-design and co-production have been used interchangeably in the literature to refer to some level of collaboration between stakeholders. 8 Our results show that there is still confusion about understanding the differences between these approaches, highlighting the need to establish precise and detailed applications or examples of these three approaches to advance theory and methodology to improve practice. Despite the variable understanding of the similarities and differences between these three approaches, participants mostly identified their practices as being co-design. They also considered co-design to be the most feasible approach in their workplaces. Co-design allows different levels of collaboration (from consultation to partnership) between different people to develop or improve a strategy. Research has proved the significance of co-design in developing health-enabling food retail strategies, yet implementing these strategies has only sometimes been sustained over the long term. 8 When different stakeholders develop partnerships and actively collaborate in designing, implementing and evaluating health-enabling strategies in food retail outlets, strategies are sustained over time, 8 being the main difference when using co-creation instead of co-design.
Our results showed that the less important co-creation attributes for participants were equal partnership/reciprocity and mutual acknowledgement. The challenge towards co-creation was also reflected in the participant’s low confidence in including multiple stakeholders’ perspectives in the final initiative. This result contradicts previous views from academic researchers, where these attributes were fundamental in the design and implementation of initiatives in food retail.7,8 In addition, research in multisectoral collaboration has shown that building a shared understanding and a clear sense of purpose, promoting accountability and supporting lateral or shared leadership, among others, are principles that can enable or impede successful nutrition-related strategies.9,10 Working successfully in a multisectoral way leads to sustaining momentum and stakeholder engagement that could be reflected in a more successful health-enabling food retail initiative.4,8,9 The most significant barrier for participants was the ongoing engagement with retailers. Some studies have demonstrated the impact of retailers’ buy-in on the project on successful implementation.4,8,9 In the co-creation approach, the ongoing collaboration between stakeholders will ensure stakeholder empowerment, project appropriation and the creation of value propositions. 9 Co-creation theory considers this possible when stakeholders enable and support individual ideas that satisfy specific needs (e.g. personal, social, business, civic or environments) in which the individuals interact. The lack of purposefully designed engagement platforms between stakeholders and co-creation frameworks in food retail environments for practitioners may be an issue in ensuring partnerships with retailers and advancing co-creation to develop health-enabling food retail initiatives. 9
While our results provide insights from, to our knowledge, the only healthy supermarket community of practice in Australia, these should be considered with caution as results from this convenience sample could not be representative of other communities of practice worldwide and may have introduced bias (e.g. availability, relevance and desirability to participate). In addition, the survey’s low response rate limits the representation and generalisation of our results. Further studies to test the hypothesis that co-creation, as an approach, can achieve mutually beneficial outcomes in food retail outlets and sustain health-enabling initiatives over time, would benefit from recruiting a larger and broader sample of key stakeholders. Understanding in-store stakeholders’ (e.g. retailers, suppliers and consumers) drivers for improving healthy food access and selection can help identify potential value propositions. Moreover, to advance co-creation research, we could explore ways to support health promotion practitioners in applying the co-creation approach and its attributes to their practice and supporting structures that foster collaboration.
Conclusion
The theoretical implications of co-creation make this approach relevant to developing health-enabling strategies in food retail outlets. However, academic evidence may not be guiding public health promotion practitioners to achieve these results. The essential attributes related to multistakeholder active collaboration and the creation of value propositions seemed challenging to apply in practice. One barrier associated with these issues is the ongoing engagement with retailers. To advance co-creation research, we could explore ways to support health promotion practitioners in applying the co-creation approach and its attributes to their practice.
Supplemental Material
sj-pdf-1-rsh-10.1177_17579139241308822 – Supplemental material for Health-enabling initiatives in food retail and co-creation attitudes from a community of practice in Australia
Supplemental material, sj-pdf-1-rsh-10.1177_17579139241308822 for Health-enabling initiatives in food retail and co-creation attitudes from a community of practice in Australia by C Vargas, J Whelan, J Brimblecombe and S Allender in Perspectives in Public Health
Footnotes
Acknowledgements
The authors acknowledge all participants who answered the survey, the Healthy Supermarkets CoP chairs, the Nourish Network and RE-FRESH for their ongoing support in disseminating the survey.
Author Contributions
Substantial contributions to the conception of the work (C.V., J.W., J.B. and S.A.); data collection (C.V.); data analysis (C.V. and J.W.) and interpretation of data for the work (C.V., J.W., J.B. and S.A.). Drafting the work (C.V.) and revising it critically for important intellectual content (C.V., J.W., J.B. and S.A.). Final approval of the version to be published (C.V., J.W., J.B. and S.A.). Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved (C.V., J.W., J.B. and S.A.).
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: C.V. and J.W. are supported by, and J.B. and S.A. are the members of, the National Health and Medical Research Council (NHMRC) funded Centre of Research Excellence in Food Retail Environments for Health (RE-FRESH) (APP1152968). The opinions, analysis and conclusions in this paper are those of the authors and should not be attributed to the NHMRC. J.W. is supported by a Deakin University Dean’s Postdoctoral Research Fellowship.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.