
Abstract

Background
Adolescents and young people, aged 10–24, experience critical developmental periods for physical, cognitive, behavioral, and social growth, which influence their lifelong health trajectory. 1 The Sub-Saharan African (SSA) population’s one-third comprises people aged 10–24 years, necessitating a public health approach to promote healthy nutrition. Adolescents and youth, who are particularly susceptible to undernutrition and diet-related obesity compared to other age groups, face increased risks for non-communicable diseases (NCDs), a major public health challenge that accounts for 70% of global deaths annually.2,3 In addition, between 1980 and 2015, the prevalence of overweight/obesity in adolescents increased in SSA, affecting 7.6% of boys and 15.4% of girls. 4 One driver of this increase in obesity is the increase in the consumption of sugar-sweetened beverages (SSBs) – a trend that was most pronounced in countries in SSA. 5
Despite the availability of cost-effective and evidence-based practices to address NCDs in low- and middle-income countries (LMICs), 6 implementing these interventions remains a significant challenge, particularly in promoting healthy behaviors among adolescents and youth. 7 In SSA, limited studies have focused on identifying the barriers and facilitators to implementing interventions and policies that promote healthy behaviors among adolescents and youth.2,7 Many of these efforts are concentrated on school-going adolescents and exclude those who are not in educational institutions and more vulnerable to unhealthy lifestyles. To be effective, new policies and programs need to consider the diverse profile of adolescents and youth, and involve multifaceted and multilevel efforts across education, health, food, social protection, and digital technology. In addition, various factors affect adolescent and youth diets and nutrition, physical activity, and healthy lifestyle behaviors. However, most intervention studies have focused on micronutrient supplementation. Finally, research is scarce on the long-term costs, effects, and impact of evidence-based interventions in this region.
Arise-Nutrint Initiative
To find solutions for these public health challenges, partners from SSA, Europe, and North America have established the multiactor, multidisciplinary, and population-representative ARISE-NUTRINT (The Africa Research, Implementation Science, and Education – Reducing NUTRition-related non-communicable diseases in adolescence and youth: INTerventions and policies to boost nutrition fluency and diet quality in Africa) initiative, which is funded by the European Commission Horizon 2022 and builds on previous successful collaborations of partners.8–10 The overall goal of ARISE-NUTRINT is to generate high-quality and actionable evidence on the (cost-) effectiveness, impact, and implementation aspects of community-based interventions and policies that promote healthy diets among adolescents in seven SSA countries: Ethiopia, Tanzania, Burkina Faso, Uganda, Nigeria, Ghana, and South Africa (Figure 1).
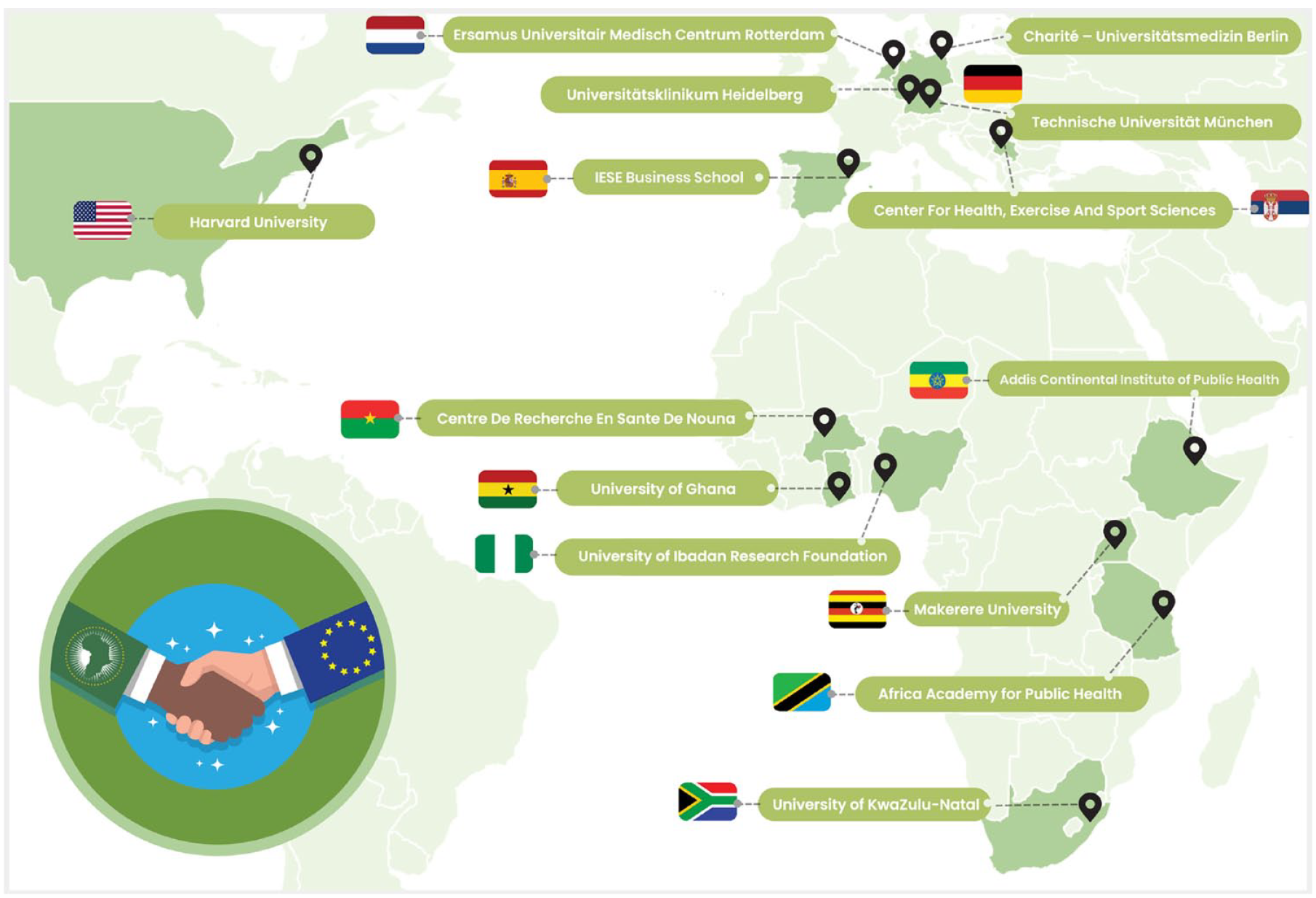
ARISE-NUTRINT consortium includes an experienced group of investigators working in population health and epidemiology, public health and intervention, sustainable nutrition, physical activities, mental health, health management and policy, health economics, mathematical modeling, and health systems from Europe, the US, and SSA. Most investigators have been involved in collaborative projects for many years within an established ARISE Network. The consortium members include partners in Central Europe (Germany, Netherlands), Eastern Europe (Serbia), Southern Europe (Spain), the US, as well as seven countries in SSA (Burkina Faso, Ethiopia, Ghana, Nigeria, South Africa, Tanzania, and Uganda)
ARISE-NUTRINT has several sub-aims (Figure 2). First, it aims to identify key nutrition-related health risk factors that contribute to long-term chronic disease burdens affecting adolescents and youth in Western, Eastern, and Southern Africa. For this, we will build a cohort of adolescents (three waves, 2024–2026) and efficiently collect data by piggybacking on endeavors of seven existing Health and Demographic Surveillance Systems (HDSS).9,10 Furthermore, ARISE-NUTRINT aims to design an effective intervention to enhance nutrition fluency, as well as literacy, practices, and nutritional status. To assure sustainability and appropriateness of the nutrition fluency intervention, which likely will comprise components of digital engagement such as educational videos and SMS/messaging through social media as well as educational material provided through pamphlets, pocket cards, and games will be co-created and piloted with adolescents following a human-centered design approach. This involves various stages, including literature reviews, qualitative investigation, co-creation workshops, drafting paper prototypes, testing the paper prototypes, and refining the prototypes for final implementation. The designed nutrition intervention will be implemented in four countries (Burkina Faso, Tanzania, Ethiopia, and Uganda) and will be evaluated through a randomized controlled trial (RCT) nested within the ARISE-NUTRINT cohort (intervention implementation in cohort wave 2, outcome assessment in wave 3). We will assess performance (processes, mechanisms, barriers, and facilitators), effectiveness, and cost-effectiveness to generate policy-relevant evidence. Finally, ARISE-NUTRINT aims to understand and assess the impact of the taxes imposed on SSBs in South Africa, Ghana, and Nigeria using mixed methods and quasi-experimental designs. Taxation of SSBs is recommended by the World Health Organization (WHO) as the best buy to reduce the consumption of SSBs and the burden of NCDs; however, its impact in SSA countries is unknown.
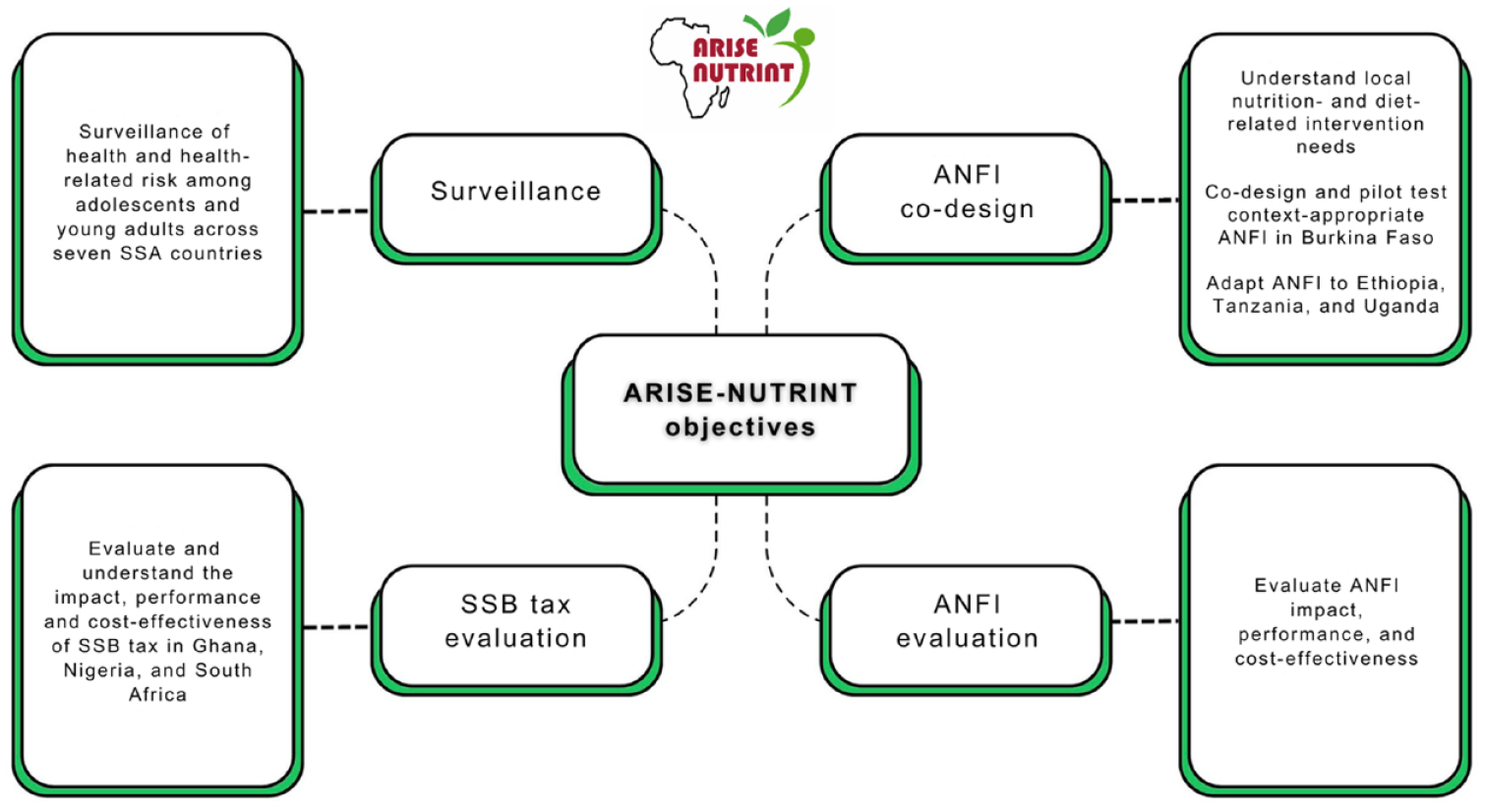
Summary of objectives of ARISE-NUTRINT initiative
Implications and Impacts
We anticipate several outcomes from ARISE-NUTRINT, including (1) an improved understanding of the risk of NCDs related to diet, nutrition, and physical activity among key stakeholders; (2) an improved understanding of the long-term costs, effects, and impacts of a co-developed nutrition fluency intervention and a WHO-recommended policy to reduce the NCD burden; and (3) insights into the factors that influence the adoption and sustainability of these evidence-based interventions and policy. A variety of groups are expected to derive benefits from the ARISE-NUTRINT initiative. Policymakers at various levels, from local to global, who aim to reduce the impact of NCDs, can use our results to inform their decision-making, policy adoption, and implementation. Adolescents and youth will benefit from the evidence-based implementation of interventions that aim to increase their nutrition literacy and promote healthier behaviors. Professionals responsible for implementing interventions to combat NCDs, including NCD policy implementers, public health workers, and other stakeholders, can leverage these findings to inform the formation and/or improvement of policy as well as integration strategies for practice. Early career research scientists in SSA and the Organisation for Economic Co-operation and Development (OECD) countries can find these results valuable for their research and career advancement. Finally, the scientific community across various disciplines in the broad field of NCDs can use these findings to further their understanding and research in this domain. ARISE-NUTRINT has the potential to contribute to improving health, economic prospects, and overall wellbeing in the SSA region. ARISE-NUTRINT’s findings and insights may also be applicable to other LMICs facing the increasing burden of nutrition-related NCDs among adolescents and youth.
Footnotes
Acknowledgements
ARISE-NUTRINT collaborators are Till Bärnighausen, Heidelberg Institute of Global Health, Heidelberg University Hospital, Germany; Wafaie W Fawzi, Department of Global Health and Population, Harvard T.H. Chan School of Public Health, USA; Jacob Burns, Professorship of Public Health and Prevention, Technical University of Munich, Germany; Mary Mwanyika Sando, Africa Academy for Public Health, Tanzania; Ayoade Oduola, University of Ibadan Research Foundation, Nigeria; Mosa Moshabela, University of KwaZulu-Natal, South Africa; Ali Sié, National Institute of Public Health, Nouna Health Research Center, Burkina Faso; Adom Manu, Department of Population, Family, and Reproductive Health, University of Ghana, Ghana; Jan AC Hontelez, Erasmus Universitair Medisch Centrum, The Netherlands; Magda Rosenmöller, Center for Research in Healthcare Innovation Management, IESE Business School, Spain; Ina Danquah, Heidelberg Institute of Global Health, Heidelberg University Hospital, Germany; Matthias Kern, Heidelberg Institute of Global Health, Heidelberg University Hospital, Germany; Joy Mauti, Heidelberg Institute of Global Health, Heidelberg University Hospital, Germany; Shannon McMahon, Heidelberg Institute of Global Health, Heidelberg University Hospital, Germany; Japhet Killewo, Muhimbili University of Health and Allied Sciences, Tanzania; Mashavu Yussuf, Africa Academy for Public Health, Tanzania; Innocent Yusufu, Africa Academy for Public Health, Tanzania.
Authors’ Note
I Brandt is also affiliated to Department of Psychiatry and Psychotherapy (CCM), Charité–Universitätsmedizin Berlin, Berlin, Germany. S Ostojic is also affiliated to Division of Public Health and Nutrition, Center for Health Sciences, Belgrade, Serbia.
Author Contributions
S.O. conceived the idea. A.L.K., S.O., and S.S. wrote the first draft of the manuscript. A.L.K. edited the manuscript. M.L., C.N., H.B., Y.B., C.H.H., S.L., I.B., D.G., N.B.M., U.P., A.T., and ARISE-NUTRINT collaborators reviewed the manuscript.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by the European Union Horizon 2022. Views and opinions expressed are however those of the author(s) only and do not necessarily reflect those of the European Union. Neither the European Union nor the granting authority can be held responsible for them. ‘For the publication fee, we acknowledge the financial support of the University of Heidelberg as part of an agreement with German academic institutions to cover Open Access Article Processing Charges (APCs)’.