
Abstract
Aims:
Unintentional injuries in the home contribute substantially to preschool child morbidity and mortality. Practitioners such as health visitors, family mentors and children’s centre staff are well-positioned to facilitate child injury prevention by providing home safety advice to families, and training may enhance their ability to do so. We aimed to assess the impact of child home safety training for these practitioners.
Methods:
An explanatory mixed-methods design was used. Practitioners completed questionnaires before, and up to 7 months after, receiving child home safety training and took part in interviews. Seventy-eight health visitors, 72 family mentors and 11 children’s centre staff members completed questionnaires. Items were used to calculate scores on home safety knowledge, confidence to provide home safety advice and belief that child home safety promotion is important. Thematic analysis of interviews with seven health visitors and nine family mentors, open-ended responses to the questionnaires and an additional evaluation form was conducted to explore attendees’ perceptions of the training and its impact. In addition, seven health visitors and six children’s centre staff who had received no training were interviewed.
Results:
Knowledge was greater post-training than pre-training across all participants (p < .001). When practitioner groups were analysed separately, there were significant increases in family mentors’ knowledge (p < .001) and belief (p = .016), and health visitors’ confidence (p = .0036). Qualitative findings indicated that most training session attendees valued the training, believed their practice relating to child home safety had improved as a result, and felt further similar training sessions would be beneficial. Those who had not attended the sessions described a need for more child home safety training.
Conclusions:
Delivering training to practitioners providing child home safety promotion to families with preschool children can enhance injury prevention knowledge, beliefs and confidence and positively impact on home safety promotion by practitioners.
Introduction
Unintentional injuries occurring in the home are a major contributor to morbidity and mortality experienced by children aged under 5 years,1–4 and many of these injuries are preventable.1,5,6 Such injuries are also much more likely to occur for families who are disadvantaged or who live in deprived areas.7–11 Practitioners who work with families with young children such as health visitors (public health nurses) and staff at children’s centres (family support centres) could play a key role in preventing child injuries by supporting families to make their homes safer for preschool children.12,13 Indeed, there is evidence that home visiting programmes aiming to reduce child injuries may be both effective and cost-effective. 14 Health visitors in England, however, tend to receive minimal child injury prevention training, and a recent survey indicated that many would be keen to undertake additional training to develop their practice. 15 Children’s centre staff also have the potential to play a greater role in promoting home safety for families with young children. Despite children’s centres often being positioned within communities at high risk for child injury, 16 home safety promotion does not appear to be provided consistently across centres. 13 Further evidence of a lack of a systematic approach to child home safety promotion in England and Wales comes from a recent survey which found only 43% of participating upper-tier local authorities and health boards provided child injury prevention training to practitioners. 17
Delivering injury prevention training to healthcare practitioners can increase knowledge18–22 and improve practices20–22 relating to child home safety, with even a single session potentially having a significantly beneficial impact. 20 After midwives and health visitors attended a session on risks associated with baby walkers, their knowledge of baby walker risks increased, midwives became more likely to discuss walkers at antenatal appointments, and health visitors’ attitudes became more negative towards walkers and more positive towards education on walkers. 20 Multisession programmes may also have beneficial effects upon knowledge and practice.21,22 A study in which physicians were randomly assigned to either receive standard training or training with two extra injury prevention sessions that focused on specific injury hazards found that parents seen by those who received the additional training received more extensive injury prevention counselling and were more satisfied with the safety-related advice they received. 22 In a further example, a 1-day multidisciplinary workshop led to health visitor attendees increasing their injury prevention knowledge, becoming more likely to identify and discuss risks to child safety in homes, and being more likely to visit families following an emergency department attendance due to child injury. 21
The present study describes our assessment of the effectiveness of child home safety training that was delivered to health visitors (this term includes all members of health visiting teams), family mentors (community members with experience of parenting who are trained to provide family support) and staff at children’s centres as part of the Stay One Step Ahead (SOSA) programme to improve child home safety. 23 SOSA was implemented in four electoral wards in Nottingham City between 2017 and 2020 as part of the Small Steps Big Changes (SSBC) programme, which works towards giving all children the best possible start in life. SOSA had multiple components including monthly safety messages, quarterly home safety educational activities delivered at children’s centres, checklists for use by health visitors at 9- to 12-month and 24- to 30-month child health reviews, and educational activities, guided by family mentors, for completion by parents of children aged 0–3 years. 23 The intervention led to families being more likely to store household poisons out of the reach of children, have a plan for fire escape, use a fireguard (or have no fire) and carry out more home safety practices. 24
The home safety training provided to practitioners was a key part of the intervention. We sought to determine practitioners’ views of the intervention training they received and the impact that it had upon their knowledge, beliefs, confidence and practice relating to home safety.
Methods
Design
An explanatory mixed-methods design was used, with quantitative data being assessed before qualitative data. Qualitative data explored attendees’ perceptions of the training and its impact. 25
Participants
Health visitors, family mentors and children’s centre staff working with children and families living in four electoral wards in Nottingham, United Kingdom.
Training sessions
The training was delivered between September 2017 and January 2020 by members of the research team with expertise in child home safety (E.O., M.H. and D.K.). It consisted of a single 2- to 3-h face-to-face session per person and was delivered by one or two presenters (the duration was 3 h for the first nine sessions, then 2 h for the remaining five sessions in response to practitioner feedback). Sessions were tailored according to the practitioner group in attendance; seven were delivered to health visitors, six to family mentors and one to children’s centre staff. Attendees per session numbered between 4 and 27. The aim was to instruct participants on how to deliver the SOSA home safety programme, increase their knowledge about how best to ensure child home safety, enhance their belief in the importance of promoting home safety and increase their confidence to deliver home safety advice. The sessions also included an explanation of the SOSA evaluation. See Supplementary File S1 for details of training session content.
Quantitative measures
Quantitative data were collected using questionnaires administered immediately prior to training (baseline) and post-training. Post-training questionnaires were provided at the end of the training sessions with a request to return them by post (freepost) within 2 weeks. An initial reminder was sent to non-responders by post or email (depending on stated contact preferences). A second non-respondent notification was posted to the participant’s manager, which requested they remind their employee to complete the questionnaire. See Table 1 for return date data for post-training questionnaires.
Return time (days) for post-training questionnaires
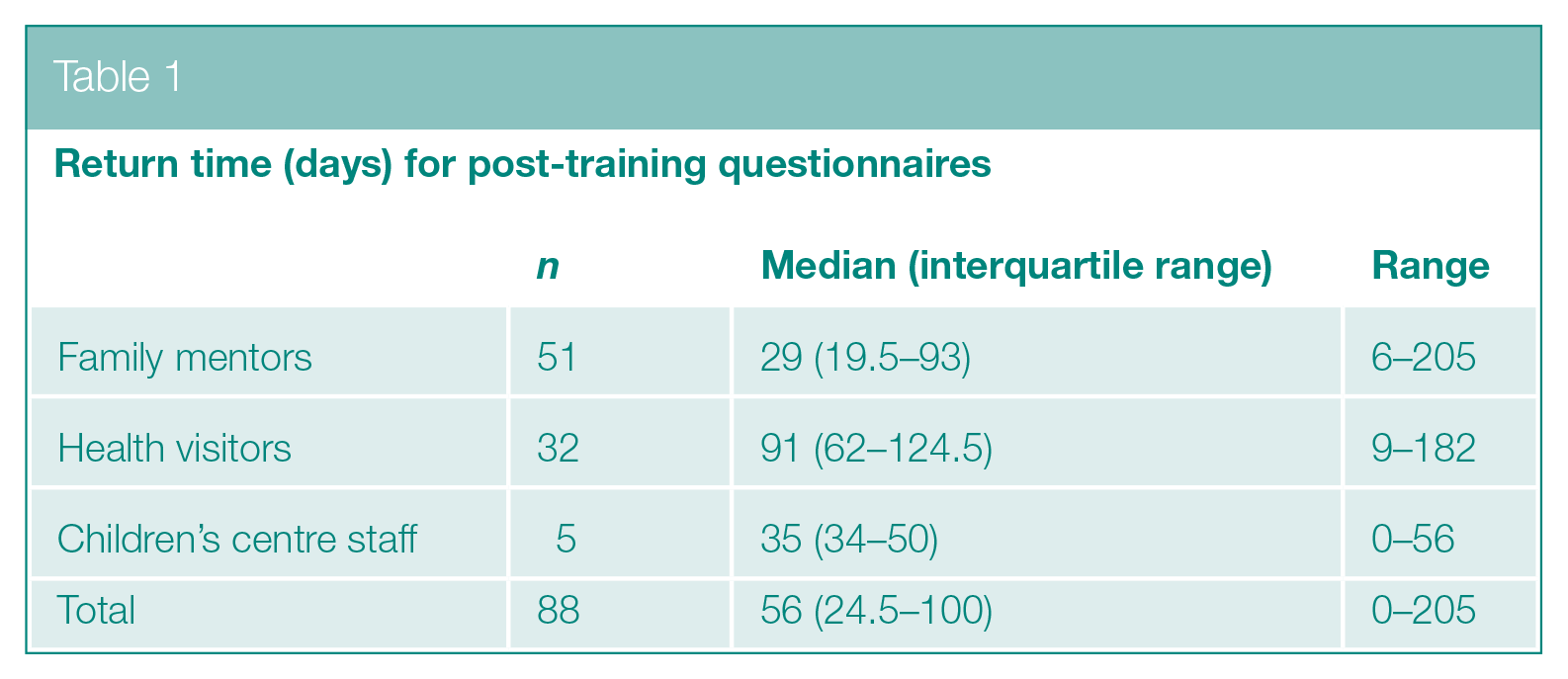
The questionnaires contained bespoke questions on home safety knowledge, confidence in being able to advise families about home safety and belief that child home safety promotion is important. These metrics were assessed using between 6 and 15 questionnaire items (see Supplementary Files S2–S4). Scores were calculated by assigning a point for each correct answer or for agreement (‘strongly agree’ or ‘agree’) on positively worded statements, or disagreement (‘disagree’ or ‘strongly disagree’) on negatively worded statements. Quantitative data were not normally distributed and were described using medians and interquartile ranges (IQRs). Pretraining and post-training scores were compared using Wilcoxon signed rank tests.
Qualitative measures
Qualitative data were collected from three sources: comments on the post-training questionnaires described above, open-ended feedback from SSBC-administered evaluation forms delivered in sessions held in SSBC premises that participants had the option of submitting at the end of the training sessions and interviews.
The post-training questionnaires contained the open-ended questions ‘How will the training change the home safety advice you provide to parents?’ ‘Are there any other home safety topics on which you would like training?’ and ‘Do you have any comments about the training?’
The SSBC evaluation forms were completed by attendees of the nine sessions held in September 2017 (the form was not distributed by SSBC staff at subsequent sessions because these were not held in SSBC premises). The questions, which were open-ended, were ‘What worked well for you?’ ‘What could be improved for the future sessions?’ and ‘What key messages/learning will you take away from the session?’
Semi-structured interviews were conducted by members of the research team with seven health visitors and nine family mentors who had received the training, and seven health visitors and six children’s centre staff who had not received it, due to working externally to the four electoral wards where the SOSA programme was delivered. Family mentors were only employed in the four SOSA programme wards, hence all received training. We were unable to interview any children’s centre staff who received training because of these participants being lost to follow-up, away on leave or having started working outside the SOSA programme areas. The interviews were conducted between 30 August 2018 and 29 April 2021 either by telephone or face-to-face, depending on interviewee preference. Interviews lasted between 25 and 91 min (median 39) and were conducted between 2.7 and 41.6 (median 33.6) months post training. At the time of data collection, children’s centres and Public Health Nursing Services, including health visiting, were undergoing restructuring and experiencing high rates of staff attrition. For some interviews, this led to delays which were sometimes further exacerbated by pressures associated with the COVID-19 pandemic. Interviews were digitally recorded and transcribed verbatim. Transcripts were analysed, along with open-ended questionnaire responses, using thematic analysis. 26 A researcher identified all quotes within the interviews that related to the training. Following this, two researchers, after familiarising themselves with the data by reading the transcripts multiple times, independently identified codes. These were developed into broader themes, which were subsequently refined, reviewed and named. Any inter-assessor coding discrepancies were resolved by consensus, and the codes were discussed with all members of the research team.
Results
Quantitative findings
Of the 161 participants who completed a pretraining questionnaire (72 family mentors, 78 health visitors and 11 children’s centre staff), 88 (54.7%) completed a post-training questionnaire: 51 family mentors, 32 health visitors and 5 children’s centre staff. For these participants, across all three practitioner groups, knowledge score distributions significantly increased following training (median 7 (IQR 6–7) to 7 (IQR 6–9) out of 14, p < .001) (see Supplementary File S5).
When the practitioner groups were assessed separately, significant increases between pre- and post-training were observed for family mentors’ knowledge (median 7 (IQR 6–7) to 8 (IQR 7–9) out of 14, p < .001) and belief (median 4 (IQR 4–5) to 5 (IQR 4–6) out of 6, p = .016) and health visitors’ confidence (median 12 (IQR 8–13) to 13 (IQR 11–14) out of 15, p = .0036). No other significant differences between pre- and post-training scores were observed.
Qualitative findings
Comments in response to open-ended questions were made on post-training questionnaires by 21 health visitors, 42 family mentors and 2 children’s centre staff. In addition, SSBC training session evaluation forms were returned by 72 health visitors, 31 family mentors and 3 children’s centre staff members. Results of the analysis of quotes from these forms and the interviews are described below. Quotes that were thought to illustrate themes particularly well are included in the main text, and further quotes are listed in Supplementary File S6.
Theme 1: Impact of home safety training
Subtheme 1.1: Perceptions of the training sessions
Attendees generally provided positive feedback about the session presenters, level of interaction, structure and content. The acquisition of new resources, such as written information to provide to parents, was often appreciated.
Enjoyed the visual aids and the opportunity to ask questions. Like the statistical facts as I feel families will respond to this. Love the information packs too, relevant for use in visits. (Family mentor evaluation form)
Health visitors often suggested that the level of interaction was appropriate (S6, quote H), while many family mentors suggested that more interaction would have been preferable (S6, quote I). Most comments relating to the resources that were provided were positive (S6, quote J), although some health visitors thought the volume of these to be excessive (S6, quote K).
Two health visitors did not remember the training sessions but appreciated the resources they had acquired (e.g. S6, quote L).
Subtheme 1.2: Impact upon knowledge
Many reported to have gained new knowledge from the sessions, and family mentors were particularly likely to state that their knowledge had increased.
Learning about home safety and accidents as I didn’t know everything but I do now. (Family mentor evaluation form in response to ‘what worked for you?’)
Attendees often reported the knowledge they had gained to be relevant to their role and that they appreciated learning about child injury incidence.
The statistics discussed during training is significant. My knowledge about the topic is now enhanced and I’m confident in signposting parents to resources and support in local area. (Health visitor post-training questionnaire)
Two health visitors and a family mentor suggested that the sessions had a minimal impact upon their knowledge level, because they already knew the information being taught (e.g. S6, quote M).
Subtheme 1.3: Impact upon attitudes or beliefs
The training appeared to enhance the belief of some family mentors and health visitors about the importance of home safety.
I really enjoyed that because it just makes us more aware how important it is to remind families about safety, not just only following the [ family mentors’] handbook because we can talk about these things at any time. (Family mentor interview)
The increased belief in the importance of home safety was linked by some to new knowledge of how one can contribute to the prevention of unintentional home injuries.
Will take it more seriously, as so many accidents occur in home each year and are mostly preventable. (Family mentor post-training questionnaire)
Subtheme 1.4: Impact upon confidence
Many attendees stated that their confidence in their ability to talk to parents had increased after attending training. This was reported on post-training questionnaires submitted by 11 family mentors, 3 health visitors and 1 children’s centre staff member.
I can confidently discuss safety with parents and feel able to advise them on safety equipment needed and storage locks for medicines and chemicals. (Children’s centre staff post-training questionnaire)
Improved confidence was frequently cited as being due to increased knowledge.
We had the training in the beginning which is good erm we had our first aid training so I feel confident to deal with things should we come across anything whilst we’re out and about. (Family mentor interview)
Some health visitors who reported increases in confidence suggested that this was partially due to the training sessions and resources resulting in their feeling better able to address a range of questions or challenges (see S6, quote X).
Subtheme 1.5: Impact upon practice
Family mentors frequently suggested that the knowledge they had gained from the training was helpful in informing discussions with families.
Having more knowledge and understanding it better to be able to reach out to the parents for them to get a better understanding around home safety. (Family mentor post-training questionnaire)
Some family mentor questionnaire responses indicated that their practice had improved due to increases in both knowledge and confidence after the training.
I now feel I have more knowledge to go into family homes to discuss home safety as before I didn’t know as much. I feel a lot more confident talking about it. (Family mentor post-training questionnaire)
Some cited specific home safety related advice they had learned, which they had since been able to pass on to families.
. . . because I wasn’t aware of that so now yes I keep saying to everyone about checking the erm changing the battery once a year, actually planning the exit away. (Family mentor interview)
Health visitors also often suggested (on both post-training questionnaires and evaluation forms) that knowledge from the training was useful for informing discussions with families about how to prevent child home injuries.
I think the training always prompts you, I think that is the good thing with any training that it prompts you to remind you to talk about certain things. (Health visitor interview) It gives me current ‘stats’ to a level and a tool that we use to open discussion and plan on. Provides a ‘tool’ for parents and myself to refer to in the future if needed. (Health visitor post-training questionnaire)
One health visitor reported on a post-training questionnaire that they would ‘be more vigilant’ and one said they would ‘Place more emphasis on home safety’. Some health visitors described the resources as being helpful in informing discussions with families.
Having a check sheet acts as a prompts during discussion. (Health visitor post-training questionnaire) More consistent as following the ‘stay one step ahead’ information and questionnaires. (Health visitor post-training questionnaire)
A few suggested that their practice had not changed following the training (e.g. S6, quote FF).
Theme 2: Potential further training
Some family mentors stated in interviews that it would be beneficial to receive regular training. It was recommended for this training to include recent information about local populations to make it more relevant.
It was a little while ago now. Erm but it was useful, in fact I think we could do with a refresher, certainly with regard to figures erm and trends if you like in accidents and stuff like that because I think there are trends erm yes people buying certain equipment. (Family mentor interview)
Those who had not attended training sessions frequently stated in interviews that receiving more child home safety training than already received during their occupational training would be beneficial. It was suggested that this could help to make home safety promotion conducted by practitioners more evidence-based and more relevant to local prevalence of injuries and safety hazards.
. . . it could be helpful to know what the accident rate is, the A&E rate due to accidents is, and erm that sort of thing to help us focus on the conversation. We don’t get any of that, I have been here for 12 years we get none of that, I can sit and rant about that and yes it would be helpful to have more of . . . to feel in touch with what is going on because if we sit on [sic] blurt out on our routine reviews, X, Y and Z things that we have to talk about and not know the impact of that, not know what is really going on in the city and what is going on with like the A&E attendances . . . (Health visitor interview)
Discussion
Our quantitative findings indicated that the training led to a significant overall increase in practitioner knowledge over a median period of 88 days. When each practitioner group was analysed separately, knowledge and belief significantly increased for family mentors, and confidence significantly increased for health visitors. We had not hypothesised that the scores would change by any particular amount, but we note that all significant increases were relatively small (maximum 1 point difference in medians). No other statistically significant changes were found. Although knowledge scores significantly increased, the median post-training score across all practitioner groups was 7 out of 14 (50%), indicating further potential for improvement. In contrast, family mentors’ significant improvements in belief led to a median score of 5 out of 6 (83.3%), and all practitioner groups’ post-training confidence median scores were high (at least 83.3% of the maximum), suggesting limited potential for further improvement.
The quantitative knowledge findings may be partially explained by qualitative evidence that many attendees, particularly family mentors, felt that the training increased their home safety knowledge and provided valuable information which was important and relevant to families living in the areas in which they worked. Quotes relating to the sessions themselves suggest that the training session structure, content, resources and level of interaction were usually appreciated. Some, especially family mentors, would have preferred more interaction during the sessions. Qualitative evidence also identified factors that may have limited quantitative knowledge score increases. A few felt that they already knew the information that was provided in the sessions, and a small number did not remember the training despite having attended and acquiring the resources that were distributed at the sessions.
For home safety beliefs, quantitative findings showed a significant increase in family mentors’ beliefs about the importance of home safety. Our qualitative evidence suggests that learning about the high incidence of accidents affecting children and that many of these could have been prevented helped to change family mentors’ beliefs. In terms of health visitors, qualitative data suggested that the significant increase in confidence scores may have been related to the training sessions and resources making them feel better prepared for a wider array of questions or challenges that might arise while advising families on home safety.
In terms of changes in practice described in our qualitative data, the training appears to have informed family mentor and health visitor discussions with parents. This came across particularly strongly among family mentors, of whom some also suggested that improvements in practice may be explained by increased confidence due to receiving the training. It would appear, therefore, based on the quantitative results, that even relatively small improvements in knowledge, confidence, and changes in attitudes and belief can lead to changes in practice.
Family mentors and children’s centre staff who attended the training stated that regular refresher training would be beneficial, and suggestions were made for this to include data, such as local information on child injury incidence. Health visitors and children’s centre staff interviewees who had not attended the training often stated that they perceived there to be substantial benefits to in-service home safety training. Reasons provided for this included that training that conveys up-to-date local child unintentional injury rates and effective prevention techniques may help to provide an enhanced link between practice and evidence that will help to inform discussions with families.
Our explanatory mixed-method design enabled us to present a qualitative exploration of potential reasons for the quantitative findings. To our knowledge, this is the first study assessing the impact of child home safety training upon family mentors. These practitioners being trained community members, rather than family support professionals, may have impacted upon their interest in, and benefit from, the training that was delivered. The increases in knowledge scores that we observed were relatively small, but previous studies have demonstrated relatively small knowledge increases following training to be associated with positive changes in injury prevention practice.20,21
A study limitation is that our quantitative sample contained considerably fewer children’s centre staff than health visitors or family mentors, and therefore the study had insufficient power for detecting statistically significant differences within this group. Furthermore, we were unable to interview children’s centre staff who attended training.
Our results may also have been affected by attrition bias. Despite multiple reminders, only 54.7% of those who completed a baseline questionnaire also completed a follow-up questionnaire. Although we did not find any statistical differences in pretraining scores between responders and non-responders, it is possible that non-responders held different views to responders. Follow-up questionnaires were administered at the end of the training sessions and were returned a median of 56 days later, hence our quantitative findings relate to short-to-medium term changes in knowledge, beliefs, confidence and practice. However, our interviews were conducted 2.7 to 41.6 months post training; hence, our qualitative findings do assess the longer-term impact of training (though a limitation of the interviews being conducted later is that some participants may have been less able to clearly remember the sessions).
A further limitation is that the proportion of the sample who completed a post-training questionnaire was smaller for health visitors than for family mentors, which affected statistical power to detect differences. The response rate for health visitors is likely to have been affected by a reorganisation of the health visiting service during the study period, with some participants changing roles or moving to teams who were not delivering the SOSA intervention.
Our findings are consistent with previous research that indicates practitioner training can be effective in enhancing knowledge,18–22 confidence 21 and practice,20–22 and changing attitudes and beliefs 20 relating to home safety. Like previous research has demonstrated, we found that providing information at a single session can lead to changes in practice, 20 indicating the potential positive impact upon community injury intervention that such training sessions may have. Our results are also in accordance with previous findings that practitioners working with families are often aware of the key role they can play in improving child home safety, are highly motivated to contribute to injury prevention and would like more related training. 12 In contrast to previous research, our mixed-methods design has enabled exploration of possible reasons for changes in knowledge, confidence, beliefs and practices.
Conclusion
Home safety training for practitioners working with families with preschool children enhanced practitioners’ belief that home safety is important, their child home safety knowledge and their confidence in being able to advise families about home safety. Home safety training also had a positive impact upon professional practice and ongoing similar training sessions would be beneficial. We suggest that a beneficial avenue of future work would be the implementation and evaluation of regular child home safety training for practitioners such as family mentors, health visitors and children’s centre staff. The present study indicates a substantial benefit of one-off training in the short-to-medium term, but also an unmet need for ongoing training, which may enable knowledge to be refreshed and learning to be contextualised according to local injury incidence and prevalence of risk factors relating to home injures. It would also be useful to explore the longer-term impact of training and how often training needs to be refreshed to maintain its impact.
Supplemental Material
sj-docx-1-rsh-10.1177_17579139231185999 – Supplemental material for Evaluating the effect of child home safety training upon three family support practitioner groups: a mixed-methods study
Supplemental material, sj-docx-1-rsh-10.1177_17579139231185999 for Evaluating the effect of child home safety training upon three family support practitioner groups: a mixed-methods study by MJ Taylor, T Patel, E Orton, MC Watson, M Hayes, R Clarke, S Stewart, C Timblin and D Kendrick in Perspectives in Public Health
Footnotes
Acknowledgements
We would like to thank the practitioners who participated in this project.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The University of Nottingham Faculty of Medicine and Health Sciences Research Ethics Committee granted ethical approval (46-1706).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This project was supported by funding from Small Steps Big Changes, part of The National Lottery Community Fund A Better Start Programme.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.