
Abstract
Aim:
Public health lifestyle databases at local authority level are currently poorly aligned across the UK. The integration of lifestyle databases at a regional level could provide a rich resource to support research and help inform public health leads and service commissioners in improving service delivery, facilitating decision-making and developing key public health policies. Prior to its implementation, the acceptability of an integrated lifestyle database should be explored. The aim of this study was to consult with public health stakeholders to explore the acceptability of developing and implementing a regional integrated lifestyle database across four key areas of public health: smoking cessation, diet, physical activity and alcohol consumption.
Method:
Qualitative interviews were conducted with public health stakeholders recruited from across the East Midlands region of England. All interviews were conducted using video conferencing software and recorded, transcribed, and analysed using the Framework approach. Sixteen public health stakeholders were purposively identified and invited to participate in interviews.
Results:
Stakeholders viewed the integrated database as having potential to support research, service development and commissioning decisions. Barriers such as providers’ reluctance to reveal their business strategies to rival organisations, cost of setting up and running the proposed database, complex information-sharing and governance were identified.
Conclusion:
An integrated lifestyle database has the potential to support research and service commissioning regionally. However, several barriers were identified that must be addressed prior to the development and implementation of an integrated database.
Keywords
Introduction
High-risk lifestyle behaviours including, smoking, poor diet, physical inactivity, and excessive alcohol consumption contribute to poor health and are widely acknowledged as prominent risk factors for the development of long-term conditions.1–6 There is a national drive within the UK towards preventing illness by tackling unhealthy behaviours and promoting health and well-being. The Health and Social Care Act 7 for England outlined specific duties for local government authorities to protect and promote health while reducing health inequalities. Local authorities therefore now provide interventions that reduce risks to health and the impact of disease, 8 in addition to exploring innovative ways of evaluating and improving their services, 9 such as data integration and sharing, and secondary analysis of existing data to identify risk factors and trends in patterns of behaviour.10,11
Electronic healthcare records from the UK are accessible to researchers via a number of platforms, but they tend to include data from a limited subset of health and care service providers, 11 or from separate geographical areas, unlinked across larger regions. Research in public health is now starting to explore the potential to transition away from siloed data systems to more accessible and integrated data resources.12,13 Several large integrated health databases, which involve the connection or linkage of multiple databases or datasets, now do exist within the UK, examples of which include the Clinical Practice Research Datalink (CPRD), 14 The Health Improvement Network (THIN) 15 and QResearch. 16 However, many of these contain mostly data from primary care records, with many local authorities in England lacking lifestyle data platforms that cover their whole population. 11 Existing lifestyle-related datasets such as ‘fingertips datasets’ 17 do collate local authority lifestyle datasets and can be useful in potentially informing service development and commissioning, but these are aggregated at population-level data and may not be suitable for research studies requiring individual-level data analysis across and between local authorities or regions.
While there remains an underwhelming lack of research concerning the development of integrated public health datasets across the UK, Lewer etal. 11 provide an excellent example of the potential usefulness of data integration through the development of the Kent Integrated Database (KID). The KID comprises individual-level linked Electronic Healthcare Records (EHRs) extracted from a wide range of services located across the Kent and Medway region including primary care providers, community health providers, mental health services and services commissioned outside of the National Health Service (NHS) including public health services, adult social care, and palliative care hospices 11 . Although focused primarily on healthcare utilisation, the KID provides data integration across the whole of Kent and Medway, providing a valuable resource for researchers who are investigating a broad range of public health questions while also supporting service commissioning based on patient needs. 11 There is great potential to learn from the KID in exploring how integrated systems can be achieved in different regions and with a focus on individual-level health behaviours.
This study has been designed to examine the potential for a fully integrated public health lifestyle dataset, using the East Midlands region of England as an initial pilot study area. We aim to explore the potential for the development of a model, which incorporates different individual-level lifestyle datasets across different geographical areas or local authorities across the East Midlands region and how lessons learned could be applicable elsewhere. This could help to inform public health policy, service delivery and commissioning decisions. It could also provide a rich data source for more in-depth analysis in future research studies, allowing for greater geographical comparisons of determinants and prevalence of lifestyle behaviours, alongside comparisons between and across lifestyle areas. Furthermore, building an integrated lifestyle database could help to inform regional and national efforts to promote health, support post-COVID recovery and return to business as usual. For example, aligning with the government’s recent obesity strategy promoting the nation’s health and to protect against COVID-19 18 or the new government white paper on improving healthcare and social care for all, 19 targeting improvements in the delivery of public health and social care interventions to support local systems to deliver high-quality care to their communities. Finally, lessons around data linkage and usage could also be learnt and applied across other local authorities within the UK and beyond.
Prior to development and implementation of such a model, it is important to explore views on the acceptability and potential demand of an integrated lifestyle database. Therefore, the aim of this research was to conduct in-depth qualitative interviews with key public heath stakeholders to explore the acceptability of developing and sharing an integrated lifestyle dataset to support service development, commissioning and research across the East Midlands region.
This study was informed by a feasibility framework, 20 which outlines eight key concepts (acceptability, demand, implementation, practicality, adaptation, integration, expansion, limited-efficacy testing). As the study aimed to explore participant perceptions of a proposed integrated lifestyle database, we focused on the acceptability, demand and practicality elements of this framework, which were adopted to inform the structuring of the topic guide for the consultations. The concepts of acceptability and demand more directly help to explain how practitioners perceived the benefits or usefulness of the proposed integrated database, while practicality helps to explain the potential barriers to the development and implementation of the database.
Methods
Study design
When conducting a research study, it is important for researchers to reflect on their philosophical perspective and position their research within a paradigm. 21 As the aim of this study was to use in-depth interviews to explore the perspectives of stakeholders and to understand issues around the acceptability of a proposed integrated database, the interpretivist approach was considered appropriate for this research.
The interpretive research paradigm is based on a subjective point of view as it seeks to gather understanding from the perspective of the participant rather than the objective observer (usually associated with the positivist paradigm) of an action. 22 Unlike a positivist approach, as well as understanding participant perspectives, the interpretivist paradigm seeks to establish trustworthiness through dependability, credibility, confirmability and transferability of the research.23–25 A positivist approach is typically associated with deductive reasoning; however, there are no fixed rules as some qualitative studies may have deductive elements, 26 and individual qualitative researchers may use both deductive and inductive approaches. 27 Therefore, this study adopted an interpretivist position with the flexibility of beginning with a deductive or theory-driven data collection (the topic guide structure and content being informed by a theoretical framework) and coding, and adding new codes inductively.28,29
Study participants
A range of public health professionals were purposively recruited from local authorities and local public health organisations from within the East Midlands region of the UK to participate in this study. To identify and recruit from local authorities, a key contact from each of the five County Council areas in the East Midlands region was identified and an invitation via email (with information about the research) was sent to them to facilitate the recruitment of eligible stakeholders to participate in the study. Stakeholders were recruited from within local authorities using the following inclusion criteria: currently engaged as a lifestyle service commissioner, public health consultant, public health manager, intelligence officer, service provider or user in any of the East Midlands local authorities, willing to participate in the study and consent to their data being used for the research. Relevant stakeholders were also identified from regional public health organisations and were invited to take part in this study through an invitational email.
Ten stakeholders from the five County Council responded and agreed to participate in the qualitative interviews. Six stakeholders working for Public Health England (now known as Office for Health Improvement and Disparities) and Population Health Management Implementation in the East Midlands region were also consulted, as they were identified as having the potential to provide relevant or expert information for the study.
Qualitative interviews
Working in collaboration with the National Institute of Health Research (NIHR)–Clinical Research Network (CRN) Public Health Speciality, the East Midlands Directors of Public Health and our Patient and Public Involvement (PPI) group, we conducted qualitative interviews with public health stakeholders across the East Midlands region of England, from September 2020 to February 2021.
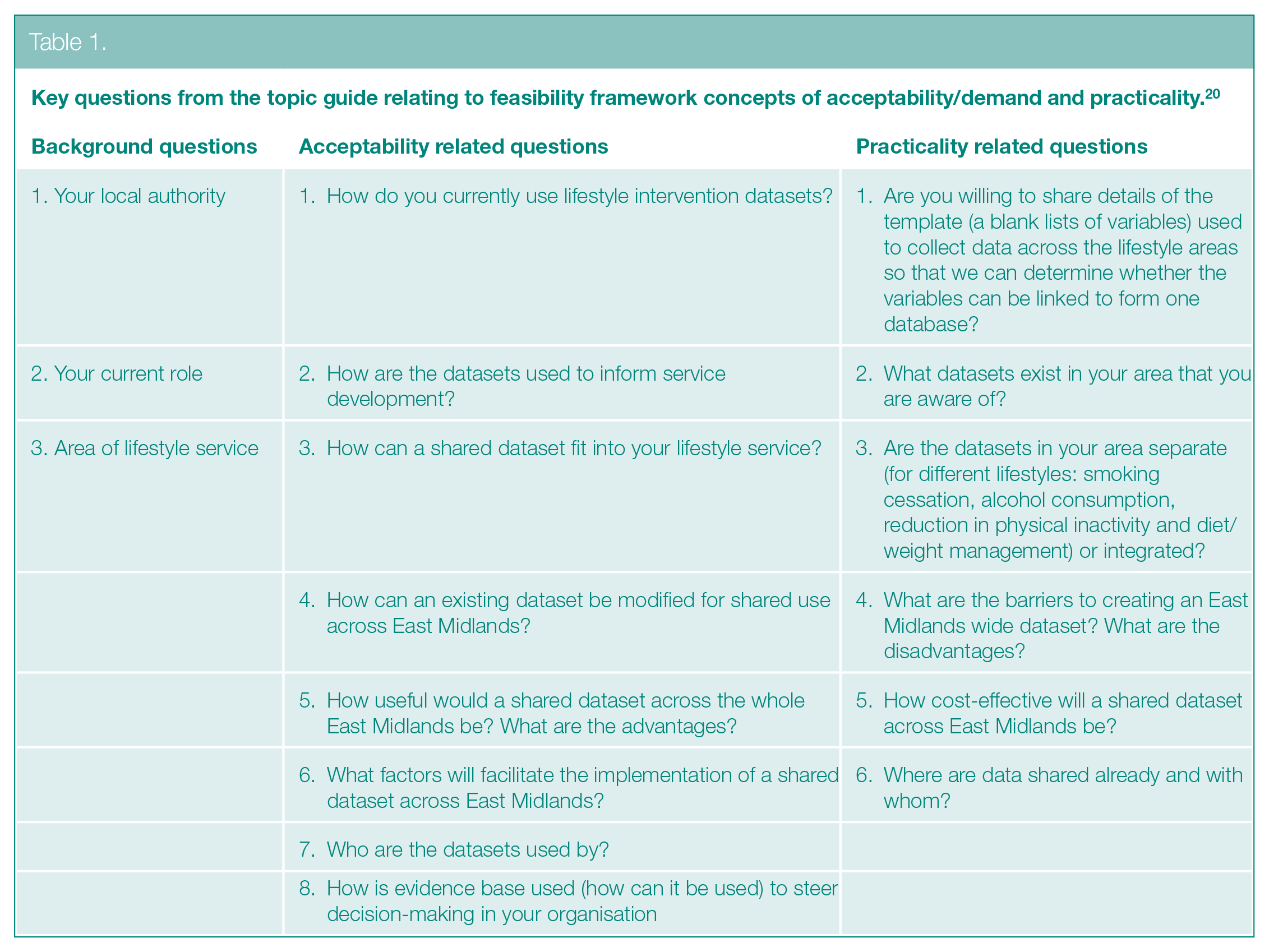
Qualitative interviews were conducted using an interview topic guide that was underpinned by the feasibility framework 20 in addition to discussion meetings with the study steering group and PPI. Key questions from the topic guide are outlined in Table 1. Qualitative interviews were conducted using video conferencing software and ranged from 30 to 60 min with an average time of 45 min. Stakeholders were informed that they could withdraw from the study up to the point of data anonymity and integration without having to give reason. Some stakeholders attended the interviews in groups, and there was one group of 2 and another group of 3. Other stakeholders opted to give extensive written feedback to questions on the interview guide, sent in advance, for discussion at the interviews. This written feedback was incorporated into the audio-recorded data for analysis.
Key questions from the topic guide relating to feasibility framework concepts of acceptability/demand and practicality. 20
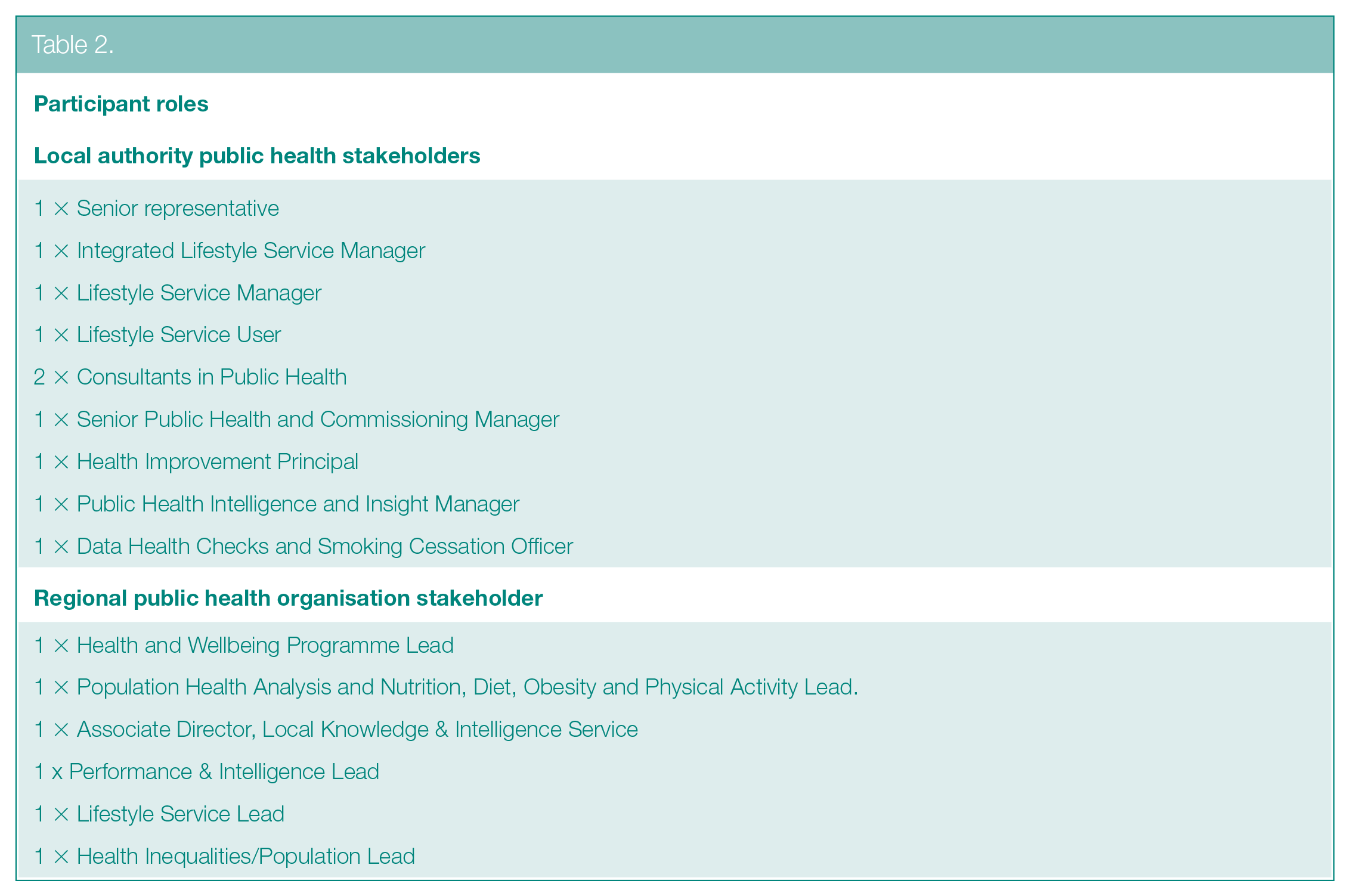
In total, 16 stakeholders responded and participated in the qualitative interviews which were arranged by email (including in some cases the provision of additional information and response to questions on the interview guide) and followed up by a virtual meeting via MS TEAMS. See Table 2 for participant details.
Participant roles
Strength, Weaknesses, Opportunities and Threats analysis
A Strengths, Weaknesses, Opportunities and Threats (SWOT) Analysis 30 was conducted using the identified qualitative themes to identify the factors that are either supportive or unfavourable to the implementation of an integrated lifestyle database. SWOT analysis is a common tool used in research as part of the strategic planning process and can be used to facilitate a better understanding of a situation and inform decision-making. 30
Data analysis
Audio data were transcribed verbatim and entered into NVivo 12 qualitative data analysis software system (QRS International Pty Ltd) to organise data and facilitate analysis. The collection of the data and analysis were undertaken until saturation had been reached. 31 In line with the philosophical position outlined above, a Framework analysis of the data32,33 was conducted, which allowed the researcher to explore deductive (a priori) and inductive (emergent) themes using the following stages: familiarisation, identifying a thematic framework, indexing, charting, mapping and interpretation.32,33 The feasibility framework concepts of acceptability, demand and practicality guided the deductive coding of the data, while ideas emerging from the data were coded inductively. The perceived benefits of the proposed database expressed by stakeholders were classified in the context of acceptability and demand, while concerns were classified as barriers in the context of practicality to the development and implementation of the database. This approach was deemed systematic and provided a clear audit trail from raw data to final themes, ensuring the trustworthiness of the results.34,35 In addition, an open, critical and reflexive approach was maintained to ensure a rigorous qualitative data analysis. 36 The Consolidated Criteria for Reporting Qualitative Studies 37 (see Supplemental Table S1) was also followed to add transparency and trustworthiness in reporting the research findings.
Results
The data were organised into two key themes: (1) benefits relating to the acceptability and demand for an integrated lifestyle database and (2) barriers relating to the practicality of constructing and implementing an integrated lifestyle database.
Benefits Relating to the Acceptability and Demand for an Integrated Lifestyle Database
Several subthemes concerning the benefits of the development and implementation of a regional integrated lifestyle database were identified, with evidence suggesting that it may be a useful resource for research development and informing service commissioning through ease of information access.
A rich resource for research
Many of the stakeholders expressed the view that an integrated lifestyle dataset would be a potentially rich resource for research:
. . . I think it is more of a potential research resource. (Stakeholder 1) Actually, if you’re relating all the provider datasets, that would be a bigger job and it would be potentially more useful for research purposes because it’s got those individual level variables. (Stakeholder 2)
Elaborating further on how an integrated database could support research, stakeholders also suggested that it could be useful for comparing service performance across geographical areas within the region:
. . . and looking at makeup of the community or the geographical sort of you know . . . and comparing similar areas to ourselves. And looking at performance in terms of what are they doing, what are they doing differently that we could perhaps adapt and use locally? (Stakeholder 3) It would give you the opportunity to compare how well things are doing in Lincolnshire compared to say Nottinghamshire because we would have both sets of information, yeah. (Stakeholder 4)
Ease of information access
Stakeholders expressed the view that a regional integrated dataset may have the potential to make it easier or quicker to access and search for lifestyle service information within a region:
. . . you’ve got five minutes and you want to know about smoking cessation services in Derbyshire. Where would you go to? You’ve got half an hour to do a bit deeper dive. Where would you go to? (Stakeholder 8)
Supporting service commissioning
Some stakeholders suggested that they would fully embrace the concept of having an integrated and shared dataset because it would be useful for service commissioning:
Having a national collection and reporting process like that of the Department of Health smoking reports would be useful. (Stakeholder 3) As a service provider we would embrace a shared dataset across the East Midlands – there are several considerations; however, I believe it would add value to service delivery and best practice. (Stakeholder 7)
Modification of existing datasets into an integrated database
Stakeholders supported the construction of a regional integrated dataset and suggested that some datasets already existed in each of the local authority areas across the East Midlands region and within each provider organisation, which could facilitate the data integration process:
For the commissioned lifestyle service two data sets exist, one which is used for smoking cessation and another which is used for lifestyle. (Stakeholder 5)
It was also noted that some standardisation in reporting mechanisms and the variables collected are already in place, particularly for smoking cessation, which could facilitate the dataset integration process:
But you know it’s quite sort of standardized that people actually think this has got potential. (Stakeholder 3)
Barriers Relating to the Practicality of Developing and Implementing an Integrated Database
Several subthemes emerged relating to the barriers or concerns of the practicality of developing and implementing an integrated lifestyle database: wide variety of commissioned services and unstandardised collection of variables, unaligned information technology (IT) systems and expense of initial setup, sensitivity of data and the need for service user consent, governance and data access issues, and reluctance of providers to share business strategies with competitors.
Wide variety of commissioned services and unstandardised collection of variables
Although some standardisation in reporting mechanisms and variables collected was already in place, particularly for smoking cessation data, some stakeholders suggested that a wide variety of commissioned services and unstandardised collection of variables existed in other areas:
Yeah, . . . it’s about the standardising of what people would commission, and another service which may be a private provider. Or it might be an NHS provider. So, provided you’ve got those two levels of understanding . . . (Stakeholder 6)
Reluctance of providers to share business strategies with competitors
Lifestyle service providers are often in competition for contracts and may not want to data share because of fear of revealing their service provision strategies to other service providers:
The data we collect and the way that we designed the processes are key in securing future business and are therefore not something that we want readily available to competitors in the public domain. (Stakeholder 7) That makes sense because yeah, I imagine some of them may have objections potentially, if they think they’re going to be compared with other areas of the effectiveness of other services. (Stakeholder 2)
Unaligned IT systems and expense of standardised software
Despite the benefits outlined by stakeholders, currently there are unaligned IT systems and expense of standardised software, in addition to the concerns that it would be costly to migrate from current datasets to a new integrated system and that the cost benefits may not emerge until the dataset is fully established:
I think you need to talk to providers . . . and Commissioners directly about it; I think there are insurmountable barriers that cost money. (Stakeholder 1) Time and capacity to support any implementation as well as any budgetary or procurement processes or other local arrangements. (Stakeholder 5)
Governance and data access issues
Stakeholders identified several concerns relating to data sharing and governance. Specifically, concerns were raised surrounding the difficulties in fully establishing data sharing agreements across all parties. There also remains unanswered questions about Information Governance and location and security of the dataset:
If you’re going to make it useful, then you have to have a way for us to access it whilst maintaining data protection and ensuring that we’re using it in a way that you agreed with providers that it will be used. Anyway, a whole lot of issues about holding it in data protection. (Stakeholder 2) . . . and especially with data sharing agreements that would need to be put in place between all the different providers. (Stakeholder 10)
Furthermore, a concern around the sensitive nature of some of the lifestyle data was expressed, with variation in the extent to which organisations are prepared to fully share their data:
Datasets and data collection methods vary greatly between services and there would be significant information governance issues with trying to combine them at a local level, let alone regional. (Stakeholder 11) Well, I would be a bit concerned because I know that all the names and addresses are attached to that information. (Stakeholder 4)
Need for user involvement and consent
In planning for the construction and implementation of a regional integrated database, some stakeholders believed that there was a need for service users to fully understand, be involved in and consent to the use of their personal (albeit anonymised) data for research or commissioning purposes:
. . . and you to have, I guess consent from the service users as well, it’s going to be shared in a different way. You know, it depends on how the providers want it shared, because many of them will likely have some agreement already. (Stakeholder 10) Data sharing would have to be done with client consent and how reasonable is it to ask clients to agree to their data being shared with numerous other stakeholders with no direct involvement in whatever intervention they’re receiving. (Stakeholder 11)
SWOT Analysis
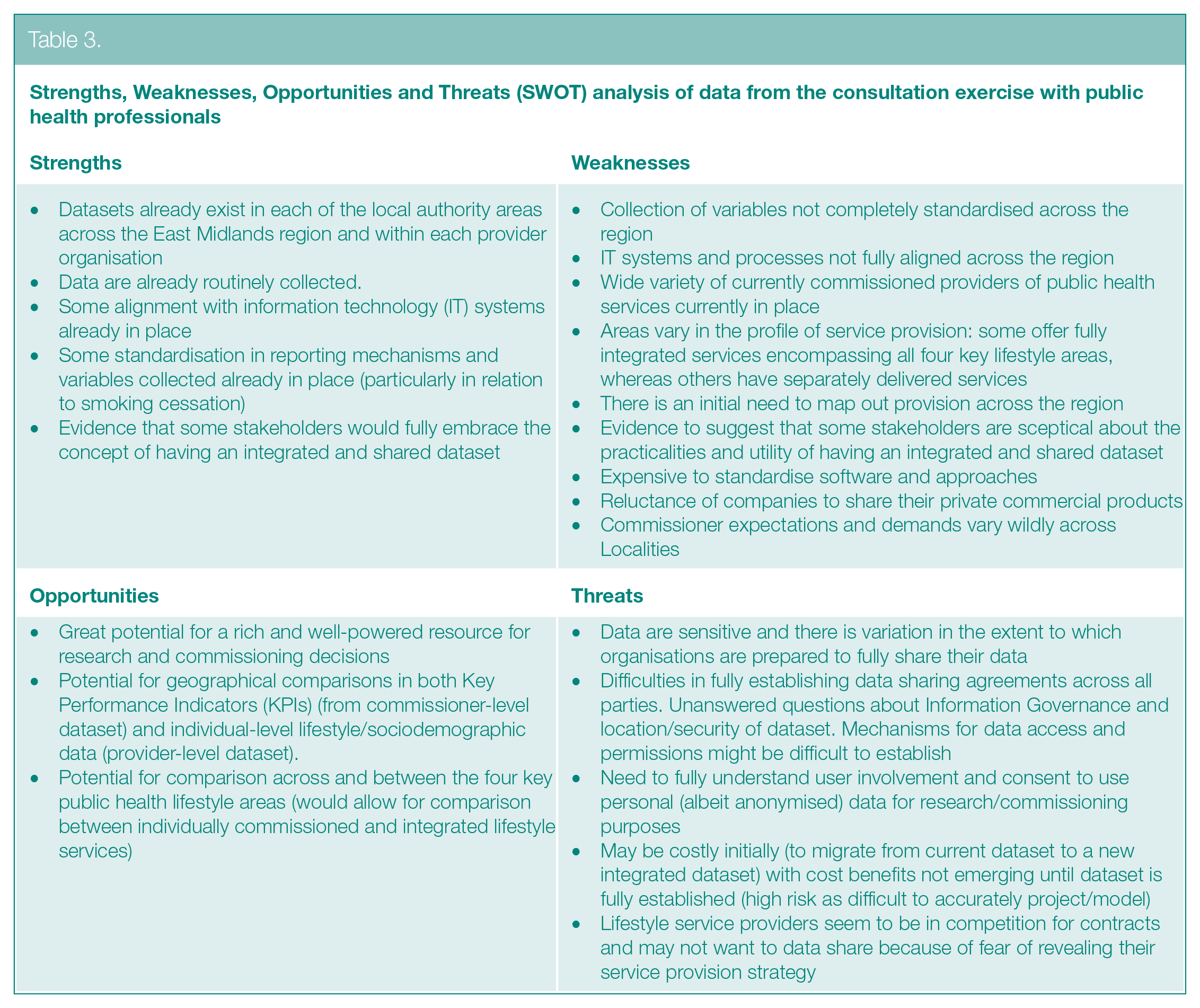
A SWOT Analysis 30 was completed using the qualitative data to organise the identified themes to outline the strength, weakness, opportunities and threats for the potential implementation of an integrated lifestyle database (see Table 3).
Strengths, Weaknesses, Opportunities and Threats (SWOT) analysis of data from the consultation exercise with public health professionals
Discussion
The aim of this study was to explore the views of public health stakeholders regarding the acceptability of developing and implementing an integrated lifestyle dataset to support services across the East Midlands region of England. There were clear benefits identified by stakeholders, including its potential for easing information access, supporting service commissioning and its potential as a rich resource for supporting research. Several barriers were identified, including reluctance to reveal business strategies to rival organisations, cost of setting up and running the proposed database, complex information-sharing and governance, which would need addressing prior to the development and implementation of a formal integrated database. The present study provides important insight into some of the perceived facilitators and barriers that could be used to guide and inform future researchers when considering the development and implementation of an integrated public health database.
Improved access to large-scale, multimodal data has previously been viewed as essential to creating an environment where research, healthcare delivery and population health are underpinned by data-driven approaches. 38 Previous evidence has shown that improving access to data can largely increase the quantity, quality and diversity of scientific research, 39 and the facilitation of a more efficient secondary use of data.40,41 Furthermore, the development of a regional integrated database has the potential to draw data from a wide range of providers and services allowing for a system-level insight into patient journeys and care utilisation while providing a unique epidemiological insight into key health determinants. 11 In addition to easing information access and its use as a rich resource for research, an integrated public health dataset was also viewed as useful in supporting and informing service commissioning. Evidence has previously highlighted the usefulness of integrated datasets in better assessing the magnitude of health problems, including identifying vulnerable populations, developing policy and evaluating interventions and initiatives. 42 A poignant example involves the recent COVID-19 pandemic where the development and maintenance of many integrated public health databases have been integral in informing rapid decision-making at a local, regional, national and international level.38,43
The potential benefit of easing information access is supported by evidence that combining data can enhance access to information at minimal cost. 13 The ease in accessing information can enhance other potential benefits of service commissioning and research. As a rich resource for research, the proposed integrated database could contain individual-level variables for more detailed and stratified data analysis, as previous integrated database-related studies found a research-related benefit of increased power for secondary data statistical analysis.10,11 Overall, these findings around benefits align with the views of experts and policymakers from a previous study, suggesting that Electronic Health Records offer significant benefits when they are used appropriately. 44 Hence, the proposed integrated lifestyle database could be useful not only within the East Midlands region but also in other regions of UK, and further afield, as it could be used to provide a snapshot of current situations and continually maintained to provide an ongoing source of data for researchers and local authorities. Specifically, like the Kent Integrated Database, 11 the proposed integrated database could be developed by linking individual-level lifestyle service data and updated regularly (e.g. monthly) for data to be available for research within a few months, easing access to information and allowing for rapid evaluation of service changes. 11
Despite the potential benefits surrounding the development of an integrated database, there are still important barriers to consider when integrating public health data, which need to be addressed and fully understood. In line with the views of public health stakeholders in the current study, both economic and technical barriers are widely considered major obstacles to data integration.45,46 The cost of both human and technical resources to prepare data, and annotate and communicate with recipients in addition to technical solutions to collect, integrate and share complex, heterogeneous data is often problematic within the public health sector.45,46 This is supported by previous evidence that show high acquisition and maintenance costs when implementing new electronic systems 44 in addition to restrictions of data harmonisation due the heterogeneity across outcomes. 10
An important concern is around the wide variety of commissioned services and unstandardised collection of variables, data collection methods and incompatible IT systems, which could make data linkage very challenging. Concerns around the initial cost of aligning IT systems and setting up standardised software have been expressed in this study and supported by evidence from a previous study concerning drawbacks associated with Electronic Health Records including high acquisition and maintenance costs. 44 Similar concerns were found in another previous study relating to variations in service commissioning and collection of variables alongside the need for a more standardised approach to data collection to maximise the potential for data integration. 10 While these concerns are important, it has been argued that the ultimate benefits of a fully integrated and functioning database could outweigh the initial cost of IT systems and standardised software. 44 Governance and data access concerns have also been expressed in the current study in terms of how best the proposed database can be housed and maintained. These findings support previous evidence on practical issues around how and where integrated data should be stored, controlled and accessed. 13 Data sharing could help to harmonise organisations, 47 but when sensitive information is involved, many lifestyle service providers within organisations like local authorities would be reluctant to share their data governed by privacy conditions. 48 As expressed by stakeholders in the current study, the concern here is about how service user privacy will be guaranteed. A related barrier is the need for service user involvement and consent, as service providers and users may refuse to share their data, as they may be worried about sharing business strategies with competitors and the risk of giving away person-identifying information. A reluctance to share data could slow research efforts to help reduce illness and prolong life, and taxpayers who contribute to research could be denied the benefits of such research efforts. 13 However, concerns around data sharing could be resolved if lifestyle service providers and users are reassured of protective measures such as anonymising the information collected into the integrated database. Drawing from the Kent Integrated Database, 11 this could be done by incorporating a unique reference number across all datasets, allowing individual lifestyle service users to be tracked across local authorities, leading to high-quality linkage with low risk of identifying personal and sensitive data of service providers and users. 11
The findings in the current study closely align with the feasibility framework concepts (Table 1). The benefits to the proposed integrated database found in this study, including ease of information access and potential to support research and lifestyle service commissioning, are aligned with the concepts of acceptability and demand 20 for the development and implementation of the proposed integrated database in the East Midlands region of England and lessons learned potentially applicable to other regions. On the other hand, barriers identified relate to the concept of practicality 20 which could oppose the development and implementation of the integrated database. However, evidence suggests that such barriers or local factors should be taken into consideration when planning the construction and implementation of an integrated database.10,11 Hence, one strength of this study is the identification of local factors, which are benefits and barriers, directly from stakeholders across the East Midlands region, which could be important for informing the development and implementation of the proposed integrated database. In addition, this study has provided relevant information from stakeholders that could contribute to the development and implementation of an individual-level integrated database, which currently does not exist particularly in the study region.
Limitations
An observed limitation of this study was that several stakeholders were willing, but unable to participate in the qualitative interviews due to the ongoing COVID-19 pandemic or workload. Public health consultants, practitioners, IT personnel, service providers and users who missed the qualitative interviews could have offered greater insight if they had participated. Furthermore, while this study may be used to inform the development of data integration across other regions of the UK, it is important to acknowledge that the views in the present study were specifically from stakeholders in the East Midlands region.
Implications for practice and further research
The barriers and benefits need to be addressed in planning for the construction and implementation of an integrated database. Further in-depth interviews with more stakeholders, particularly service users and providers, IT personnel, governance and data protection experts, is recommended to explore how barriers to the database construction and implementation can be overcome. Future research should seek to: examine under what conditions people would be willing to work collaboratively with a shared dataset across the East Midlands region; examine any potential benefits and barriers to data access or collation and sharing; and produce a toolkit, outlining the key factors to be considered (and how these could be addressed) in the construction of a regional integrated lifestyle database.
Conclusion
Based on findings from conducting qualitative interviews with public health stakeholders, an integrated lifestyle dataset has the potential to inform public health policy and practice in the East Midlands region of England and other local authorities across the UK in their approach to lifestyle data integration and usage at local authority level. It also has the potential to support in-depth statistical analysis, informing public health lifestyle interventions leading to prevention or reduction in long-term conditions and improvement in health outcomes. However, local factors such as the barriers and benefits identified should be considered.
Supplemental Material
sj-docx-1-rsh-10.1177_17579139221136726 – Supplemental material for Exploring the perceptions and acceptability of an integrated lifestyle database for public health research and service commissioning: a qualitative study
Supplemental material, sj-docx-1-rsh-10.1177_17579139221136726 for Exploring the perceptions and acceptability of an integrated lifestyle database for public health research and service commissioning: a qualitative study by JNA Akanuwe, S Cooke, H Henderson and R Kane in Perspectives in Public Health
Footnotes
Acknowledgements
Acknowledgements go to the Directors of Public Health in the East Midlands, particularly Professor Derek Ward, Director of Public Health, Lincolnshire and Chair of the East Midlands Directors of Public Health for his support throughout this project. Acknowledgements also go to the stakeholders who participated in the consultation exercise and willingly shared their views to inform this study. Thanks also go to Sally Bassett and David Clarke for their role as steering group members who guided the study to completion and to the Community and Health Research Unit Study Review team for reviewing the paper and offering advice.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This project was funded by the National Institute for Health Research East Midlands Clinical Research Network and the College of Social Science, University of Lincoln.
Ethical Approval
The project was formally logged with the University of Lincoln Ethics system on 16 September 2020 (Ethics review REF number: 2020_3761).
Availability of Data and Materials
The data used to support the findings of this study are available from the corresponding author upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.